Introduction & Epidemiology
The shoulder girdle represents a highly intricate anatomical and biomechanical construct, affording the upper extremity unparalleled mobility while demanding substantial stability. This balance is largely orchestrated by a complex interplay of muscles, originating from the axial skeleton and inserting onto the clavicle, scapula, and humerus. A comprehensive understanding of the origins, insertions, actions, and innervations of these muscles is paramount for the orthopedic surgeon, underpinning accurate diagnosis, effective surgical planning, and successful post-operative rehabilitation.
Pathologies affecting the shoulder girdle musculature are highly prevalent, contributing significantly to patient morbidity and healthcare burden. Rotator cuff tears, for instance, are among the most common diagnoses in orthopedic practice, with an estimated prevalence of 20-30% in individuals over 60 years of age, and symptomatic tears often necessitating surgical intervention. Deltoid injuries, pectoralis major ruptures, and scapular dyskinesis due to serratus anterior or trapezius dysfunction also represent substantial components of a shoulder surgeon's caseload. Moreover, these muscles are intimately involved in stabilization and movement during reconstructive procedures such as arthroplasty, instability repair, and fracture fixation. A detailed anatomical and functional grasp of each muscle is critical for precise surgical approaches, identification of internervous planes, protection of neurovascular structures, and optimizing functional outcomes.
Surgical Anatomy & Biomechanics
The muscles of the shoulder can be broadly categorized into those primarily acting on the scapula (scapulothoracic muscles) and those acting directly on the glenohumeral joint (glenohumeral muscles). A profound understanding of their individual roles and synergistic actions is essential.
Scapulothoracic Muscles
These muscles stabilize and move the scapula, providing a stable base for glenohumeral motion. Their coordinated action is crucial for the scapulothoracic rhythm.
-
Trapezius
- Origin: External occipital protuberance, nuchal ligament, spinous processes of C7–T12.
- Insertion: Lateral third of clavicle, acromion, spine of scapula.
-
Action:
- Superior fibers: Elevate scapula, upward rotation.
- Middle fibers: Retract scapula.
- Inferior fibers: Depress scapula, upward rotation.
- Innervation: Accessory nerve (Cranial nerve XI), C3, C4 spinal nerves (proprioception, pain).
- Surgical Relevance: The superior trapezius is often encountered in posterior approaches to the shoulder and scapula. Its integrity is vital for scapular stability. Accessory nerve palsy leads to trapezius dysfunction, resulting in shoulder droop, pain, and weakness in abduction and forward flexion, occasionally necessitating reconstructive procedures like modified Eden-Lange or pectoralis major transfers.
-
Latissimus Dorsi
- Origin: Spinous processes of T6–S5, thoracolumbar fascia, iliac crest, inferior three ribs.
- Insertion: Floor of the intertubercular groove of the humerus.
- Action: Extends, adducts, and internally rotates the humerus. Depresses the shoulder girdle.
- Innervation: Thoracodorsal nerve (C6–C8).
- Surgical Relevance: The latissimus dorsi is a powerful muscle frequently utilized in muscle transfer procedures, particularly for irreparable posterosuperior rotator cuff tears. Its broad origin and robust blood supply make it an excellent choice for pedicled or free flap coverage in complex shoulder wounds. The thoracodorsal nerve and vessels must be meticulously protected during its harvesting.
-
Rhomboid Major
- Origin: Spinous processes of T2–T5.
- Insertion: Medial border of the scapula (inferior to scapular spine).
- Action: Retracts and downwardly rotates the scapula, fixes scapula to thoracic wall.
- Innervation: Dorsal scapular nerve (C4–C5).
- Surgical Relevance: Deep to the trapezius, the rhomboids are important for scapular stabilization. They can be detached and repaired during approaches to the medial scapula. The dorsal scapular nerve typically pierces or runs along their deep surface.
-
Rhomboid Minor
- Origin: Spinous processes of C7–T1, nuchal ligament.
- Insertion: Medial border of the scapula (at the root of the scapular spine).
- Action: Retracts and downwardly rotates the scapula, fixes scapula to thoracic wall.
- Innervation: Dorsal scapular nerve (C4–C5).
- Surgical Relevance: Similar to rhomboid major, encountered in posterior scapular approaches.
-
Levator Scapulae
- Origin: Transverse processes of C1–C4.
- Insertion: Superior angle and superior part of medial border of the scapula.
- Action: Elevates and downwardly rotates the scapula.
- Innervation: Dorsal scapular nerve (C4–C5) and direct branches from C3–C4 spinal nerves.
- Surgical Relevance: Located deep to the sternocleidomastoid and trapezius, it is identified during superior medial scapular approaches. Injury to its innervation can impair scapular elevation.
-
Pectoralis Major
-
Origin:
- Clavicular head: Medial half of the clavicle.
- Sternocostal head: Sternum, costal cartilages 1–6.
- Abdominal head: Aponeurosis of the external oblique.
- Insertion: Lateral lip of the intertubercular groove of the humerus.
- Action: Adducts, internally rotates, and flexes the humerus (clavicular head assists in flexion).
- Innervation: Medial and lateral pectoral nerves (C5–T1).
- Surgical Relevance: This is the most superficial muscle in the anterior chest and shoulder. The deltopectoral interval, bounded laterally by the deltoid and medially by the pectoralis major, is a key internervous plane for anterior approaches to the glenohumeral joint and proximal humerus. Ruptures of the pectoralis major tendon, particularly at the humeral insertion, are common in athletes and typically require surgical repair.
-
Origin:
-
Pectoralis Minor
- Origin: Ribs 3–5.
- Insertion: Coracoid process of the scapula.
- Action: Protracts, depresses, and downwardly rotates the scapula. Stabilizes the scapula.
- Innervation: Medial pectoral nerve (C8–T1).
- Surgical Relevance: Located deep to the pectoralis major. Its attachment to the coracoid process is important in Latarjet procedures. Its tightness can contribute to neurogenic thoracic outlet syndrome.
-
Subclavius
- Origin: First rib and its costal cartilage.
- Insertion: Inferior surface of the middle third of the clavicle.
- Action: Depresses and protracts the clavicle, stabilizes the sternoclavicular joint.
- Innervation: Nerve to subclavius (C5–C6), from the upper trunk of the brachial plexus.
- Surgical Relevance: Protects the underlying brachial plexus and subclavian vessels from clavicular fractures.
-
Serratus Anterior
- Origin: Ribs 1–9.
- Insertion: Ventral surface of the medial border of the scapula.
- Action: Protracts and upwardly rotates the scapula. Holds the scapula against the thoracic wall.
- Innervation: Long thoracic nerve (C5–C7).
- Surgical Relevance: Paralysis of the serratus anterior due to long thoracic nerve injury (e.g., iatrogenic during thoracotomy, trauma, or viral neuritis) results in classic "winging" of the scapula, significantly impairing overhead function. Management may involve nerve grafting or muscle transfers (e.g., pectoralis major or rhomboid transfer).
Glenohumeral Muscles
These muscles directly act on the glenohumeral joint, providing both movement and dynamic stability.
-
Deltoid
- Origin: Lateral third of clavicle (anterior), acromion (middle), spine of scapula (posterior).
- Insertion: Deltoid tuberosity of the humerus.
- Action: Primary abductor of the humerus. Anterior fibers aid in flexion and internal rotation; posterior fibers aid in extension and external rotation.
- Innervation: Axillary nerve (C5–C6).
- Surgical Relevance: The deltoid is crucial for almost all surgical approaches to the glenohumeral joint. The deltoid-splitting approach (e.g., for rotator cuff repair) utilizes the internervous plane between the anterior and middle deltoid fibers, but care must be taken to protect the axillary nerve, which runs approximately 5-7 cm distal to the acromion. Deltoid dehiscence or avulsion after surgery is a serious complication leading to significant functional loss.
-
Teres Major
- Origin: Inferior angle and lower part of the lateral border of the scapula.
- Insertion: Medial lip of the intertubercular groove of the humerus.
- Action: Adducts, internally rotates, and extends the humerus.
- Innervation: Lower subscapular nerve (C5–C7).
- Surgical Relevance: Often considered a "latissimus dorsi's little helper" due to similar actions and contiguous insertion. It forms part of the posterior wall of the axilla and is encountered in posterior approaches.
Rotator Cuff Muscles
These four muscles are critical for dynamic stability and rotation of the glenohumeral joint. They form a musculotendinous cuff around the humeral head.
-
Supraspinatus
- Origin: Supraspinous fossa of the scapula.
- Insertion: Superior facet of the greater tuberosity of the humerus.
- Action: Initiates abduction of the humerus (first 15-20 degrees). Stabilizes the humeral head in the glenoid.
- Innervation: Suprascapular nerve (C5–C6).
- Surgical Relevance: Most commonly torn rotator cuff tendon. Repair is a cornerstone of shoulder surgery. The suprascapular nerve courses through the suprascapular notch and spinoglenoid notch, making it vulnerable during extensive dissection in these areas.
-
Infraspinatus
- Origin: Infraspinous fossa of the scapula.
- Insertion: Middle facet of the greater tuberosity of the humerus.
- Action: Primary external rotator of the humerus. Stabilizes the humeral head.
- Innervation: Suprascapular nerve (C5–C6).
- Surgical Relevance: Commonly involved in rotator cuff tears. Its function is crucial for activities requiring external rotation.
-
Teres Minor
- Origin: Middle part of the lateral border of the scapula.
- Insertion: Inferior facet of the greater tuberosity of the humerus.
- Action: External rotator of the humerus. Stabilizes the humeral head.
- Innervation: Axillary nerve (C5–C6).
- Surgical Relevance: Often co-injured with infraspinatus or axillary nerve. Its integrity is important for posterior stability and external rotation.
-
Subscapularis
- Origin: Subscapular fossa of the scapula.
- Insertion: Lesser tuberosity of the humerus.
- Action: Primary internal rotator of the humerus. Contributes to adduction. Stabilizes the humeral head anteriorly.
- Innervation: Upper and lower subscapular nerves (C5–C7).
- Surgical Relevance: Tears are less common than superior cuff tears but can lead to significant internal rotation weakness and anterior instability. Surgical repair often involves tenotomy or osteotomy of the lesser tuberosity for access during total shoulder arthroplasty, requiring meticulous repair for optimal post-operative function.

Figure 1: Superficial posterior shoulder musculature, illustrating the Trapezius and Deltoid.
Neurovascular Relationships
Key neurovascular structures traverse or lie in close proximity to the shoulder musculature:
*
Brachial Plexus:
Originates from C5-T1, supplying all major upper extremity muscles. Vulnerable in supraclavicular and infraclavicular regions.
*
Axillary Nerve:
Wraps around the surgical neck of the humerus, innervating the deltoid and teres minor. Highly vulnerable during shoulder dislocations, proximal humeral fractures, and deltoid-splitting approaches.
*
Suprascapular Nerve:
Courses through the suprascapular and spinoglenoid notches, innervating the supraspinatus and infraspinatus. Can be entrapped by cysts or impinged.
*
Long Thoracic Nerve:
Runs superficially on the serratus anterior, making it susceptible to iatrogenic injury during axillary dissection or trauma.
*
Thoracodorsal Nerve:
Accompanies the thoracodorsal artery, supplying the latissimus dorsi. Important to preserve unless performing a muscle transfer.
*
Pectoral Nerves:
Medial and lateral pectoral nerves supply the pectoralis major and minor.
*
Dorsal Scapular Nerve:
Supplies the rhomboids and levator scapulae.

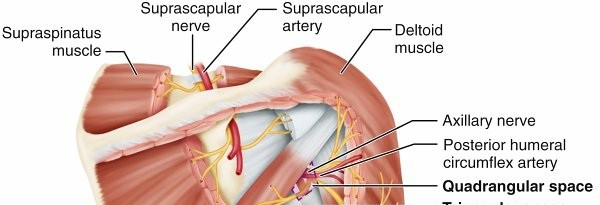
Figure 2: Deeper anterior shoulder musculature and neurovascular structures, illustrating the Pectoralis minor, Subscapularis, and adjacent nerves.
Biomechanics
The intricate balance between stability and mobility is achieved through several force couples:
*
Deltoid-Rotator Cuff Force Couple:
The deltoid initiates abduction, but without the counteracting depressor and centring forces of the rotator cuff (especially subscapularis anteriorly, infraspinatus/teres minor posteriorly, and supraspinatus superiorly), the humeral head would migrate superiorly, leading to impingement.
*
Scapulothoracic Force Couple:
The trapezius (upper, middle, lower fibers) and serratus anterior work synergistically to rotate the scapula upward during overhead motion, maintaining optimal glenoid orientation for the humeral head. Dysfunction in this couple (e.g., serratus anterior palsy) disrupts the scapulothoracic rhythm, causing pain and weakness.
Indications & Contraindications
Surgical intervention involving shoulder girdle muscles is indicated for a wide array of pathologies, primarily aimed at restoring function, alleviating pain, and improving stability.
Indications
- Rotator Cuff Tears: Symptomatic full-thickness tears, partial-thickness tears refractory to non-operative management, massive irreparable tears requiring augmentation or transfer.
- Pectoralis Major Ruptures: Acute, symptomatic tears, especially in active individuals, for restoration of strength and cosmesis.
- Deltoid Avulsion/Dehiscence: Traumatic avulsions, or iatrogenic dehiscence post-surgery, leading to profound abduction weakness.
- Scapular Winging: Chronic long thoracic nerve palsy or trapezius palsy leading to functional impairment, often requiring muscle transfer procedures (e.g., pectoralis major transfer for serratus anterior, Eden-Lange for trapezius).
- Shoulder Instability: When associated with significant labral injury, capsular laxity, or bony defects requiring muscle-tendon manipulation (e.g., subscapularis management in Latarjet or Remplissage).
- Proximal Humerus Fractures: Open reduction and internal fixation (ORIF) often necessitates surgical approaches that mobilize or detach portions of the deltoid or rotator cuff insertions.
- Glenohumeral Arthritis: Total shoulder arthroplasty (TSA) or reverse total shoulder arthroplasty (rTSA) requires careful handling of the rotator cuff, particularly the subscapularis.
- Scapular Fractures: Displaced fractures of the glenoid, scapular neck, or body may require approaches that reflect or incise periscapular muscles.
- Muscle Contractures/Fibrosis: Less common, but may require release (e.g., infraspinatus contracture in brachial plexus birth palsy).
Contraindications
- Active Infection: Absolute contraindication for elective surgery.
- Uncontrolled Systemic Comorbidities: Poor cardiac, pulmonary, or metabolic status that significantly increases surgical risk.
- Severe Osteopenia/Poor Bone Quality: May preclude secure tendon-to-bone or implant fixation.
- Irreparable Muscle Tissue: Chronic tears with severe muscle atrophy, fatty infiltration, or retraction may not be amenable to direct repair.
- Patient Non-compliance: Inability to adhere to post-operative rehabilitation protocols.
- Neurovascular Compromise: Pre-existing, severe, or acute neurovascular injury that complicates the surgical field or prognosis.
- Unrealistic Patient Expectations: Lack of understanding regarding potential outcomes or recovery timelines.
Operative vs. Non-Operative Indications
| Indication Category | Non-Operative Management | Operative Management |
|---|---|---|
| Rotator Cuff Tears | Small, asymptomatic tears; partial-thickness tears; low functional demand; failed prior surgery; significant comorbidities; acute tears in elderly with good function. | Symptomatic full-thickness tears; partial tears >50% thickness or failed non-op management; acute, traumatic tears in young, active individuals; massive irreparable tears with specific transfer indications. |
| Pectoralis Major Ruptures | Partial tears; chronic, asymptomatic tears; low functional demand; significant comorbidities. | Acute, complete tears in active individuals; chronic tears with significant functional deficit; cosmetic deformity. |
| Deltoid Avulsion/Dehiscence | Small, partial avulsions with good residual function; high surgical risk. | Traumatic full avulsions; significant post-operative dehiscence; substantial functional impairment (inability to abduct). |
| Scapular Winging | Acute nerve palsies (observation for 6-12 months); mild, asymptomatic winging; physiotherapy. | Chronic, symptomatic long thoracic nerve or accessory nerve palsy with functional deficits; failed non-operative management; nerve transfers or muscle transfers. |
| Shoulder Instability | First-time dislocations (unless high-risk); subluxations; generalized ligamentous laxity; physiotherapy. | Recurrent instability with labral pathology (Bankart/ALPSA); significant bony defects (glenoid/humeral head); failed non-operative management; traumatic instability in athletes. |
| Proximal Humerus Fractures | Minimally displaced 1-part fractures; stable 2-part surgical neck fractures; low functional demand in elderly. | Displaced 2-, 3-, 4-part fractures; fractures with articular involvement; fractures with neurovascular compromise; fracture-dislocations; failed non-operative management. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful shoulder surgery, minimizing complications and optimizing exposure.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, focusing on pain characteristics, range of motion, strength, stability, and neurovascular status. Assessment of skin integrity and prior surgical scars.
-
Imaging:
- Radiographs: AP, lateral, and axillary views are standard for bony assessment. Stryker notch and West Point views for instability, outlet view for impingement.
- MRI: Gold standard for soft tissue evaluation, particularly rotator cuff tears, labral injuries, and assessment of muscle atrophy/fatty infiltration.
- CT Scan: Essential for complex fractures, glenoid bone loss assessment (instability), and pre-operative planning for arthroplasty.
- Nerve Conduction Studies/EMG: Indicated for suspected nerve palsies (e.g., long thoracic, axillary, suprascapular).
- Surgical Approach Selection: Based on pathology and desired exposure (e.g., deltopectoral, deltoid-splitting, posterior, superior).
- Implant Selection: Appropriate choice of suture anchors, plates, screws, or arthroplasty components.
- Anesthesia Consultation: Evaluation of patient comorbidities, discussion of regional anesthesia (interscalene block) for post-operative pain control.
- Patient Counseling: Detailed discussion of the procedure, potential risks, expected outcomes, and post-operative rehabilitation.
Patient Positioning
The two primary positions for shoulder surgery are beach chair and lateral decubitus.
-
Beach Chair Position:
- Setup: Patient is semi-recumbent (30-70 degrees of trunk elevation). Head secured in a headrest (e.g., 'Mayfield' type) to prevent cervical extension and neural impingement. Torso firmly secured to the operating table. The operative arm is draped free or in a sterile arm holder (e.g., 'Spider' arm holder for arthroscopy).
- Advantages: Excellent access to anterior, superior, and posterior aspects of the shoulder. Familiar for many surgeons. Reduced intra-articular pressure during arthroscopy.
- Disadvantages: Risk of cerebral hypoperfusion (beach chair hypotension), particularly with interscalene block. Potential for airway compromise, cervical spine injury.
- Pearls: Ensure adequate padding for all pressure points. Monitor blood pressure closely. Position the head neutrally. Ensure the patient is far enough towards the edge of the table to allow full shoulder extension.

Figure 3: Patient in the beach chair position for shoulder surgery, demonstrating external stabilization and access.
-
Lateral Decubitus Position:
- Setup: Patient is placed on the non-operative side. Axillary roll positioned beneath the dependent axilla to prevent brachial plexus compression. Torso secured with beanbags or straps. Head positioned neutrally. The operative arm is suspended using traction in an arm tower.
- Advantages: Improved visualization in arthroscopy with gravitational distraction. Excellent access to posterior and inferior structures. Often preferred for complex instability or revision cases. Reduced risk of beach chair hypotension.
- Disadvantages: Potential for brachial plexus injury from excessive traction. Limited access to the anterior-superior shoulder. Positioning can be cumbersome.
- Pearls: Ensure traction weight is minimized and monitored. Pad all bony prominences. Confirm proper axillary roll placement.
Detailed Surgical Approach / Technique
Surgical techniques involving shoulder girdle muscles are diverse, dictated by the underlying pathology. Here, we outline general principles and examples relevant to the muscles discussed.
General Principles
- Internervous Planes: Whenever possible, surgical approaches should utilize internervous planes to minimize muscle damage and preserve function. Examples include the deltopectoral interval (between deltoid/axillary nerve and pectoralis major/pectoral nerves) and the deltoid-splitting approach (within the deltoid, parallel to its fibers, taking care to avoid the axillary nerve).
- Muscle Reflection/Detachment: When direct visualization or access is required, muscles may be carefully reflected or detached from their origins or insertions. Meticulous repair is paramount to restore function.
- Neurovascular Protection: Constant vigilance is required to identify and protect major nerves (axillary, suprascapular, long thoracic, thoracodorsal) and vessels.
- Tension-Free Repair: Achieving a tension-free repair of tendons or muscles is critical for healing and preventing re-rupture.
- Biologic Augmentation: The use of patches, allografts, or growth factors may be considered for massive or revision tears, although evidence for their superiority is mixed.
Common Surgical Approaches and Muscle Involvement
-
Deltopectoral Approach:
- Indications: Proximal humerus fractures (ORIF), total shoulder arthroplasty (TSA), anterior instability, coracoid transfer (Latarjet).
- Technique: Incision from the coracoid process distally towards the deltoid insertion. The interval between the deltoid (laterally) and pectoralis major (medially) is identified. The cephalic vein typically lies within this interval and can be retracted laterally with the deltoid or medially with the pectoralis. Dissection proceeds deep, exposing the clavipectoral fascia, which is incised. The pectoralis minor tendon is identified and may be released from the coracoid for better exposure (repaired at closure). The subscapularis muscle and tendon are exposed. For arthroplasty or extensive instability work, the subscapularis may be taken down via tenotomy (repaired end-to-end), lesser tuberosity osteotomy, or peel-off (repaired with sutures). Protection of the musculocutaneous nerve (medial to the conjoined tendon) is critical.
-
Deltoid-Splitting Approach:
- Indications: Rotator cuff repair (arthroscopic or mini-open), greater tuberosity fractures.
- Technique: A longitudinal incision centered over the acromion, extending distally. The deltoid fibers are carefully split in line with their orientation (anterior and middle fibers, or middle and posterior fibers). The axillary nerve typically crosses the deltoid approximately 5-7 cm distal to the acromion; splits should not exceed 4-5 cm from the acromion to avoid nerve injury. The underlying supraspinatus or infraspinatus tendons are then accessed directly.
-
Posterior Approach (e.g., Judet Approach):
- Indications: Posterior glenohumeral instability, posterior shoulder arthroplasty, posterior scapular fractures.
- Technique: Incision along the posterior aspect of the acromion and scapular spine. The deltoid muscle is split or detached from the scapular spine and retracted. The interval between the infraspinatus and teres minor (often referred to as the "quadrilateral space" superior border) is explored. The teres minor can be detached from its humeral insertion and reflected for wider exposure to the posterior glenoid and humeral head, protecting the axillary nerve and posterior circumflex humeral artery within the quadrilateral space.
Specific Muscle-Related Surgical Techniques
-
Rotator Cuff Repair (Arthroscopic):
- Portal Placement: Establishment of standard posterior, anterior, and lateral portals.
- Bursoscopy & Debridement: Subacromial bursa debridement. Acromioplasty (partial acromionectomy) if impingement is noted.
- Tear Assessment: Visualization of the supraspinatus , infraspinatus , subscapularis , and teres minor tendons, assessing tear size, retraction, and tissue quality.
- Mobilization: Release of adhesions, capsular releases, or interval slides to mobilize the torn tendon to achieve a tension-free repair.
- Footprint Preparation: Decortication of the greater tuberosity to promote healing.
- Anchor Placement: Insertion of suture anchors into the humeral head.
- Suture Passage & Repair: Sutures are passed through the tendon and tied, reapproximating the tendon to its anatomical footprint (single-row, double-row, or transosseous equivalent techniques).
- Closure: Layered closure of portals.
-
Pectoralis Major Tendon Repair:
- Approach: Deltopectoral or direct anterior approach.
- Identification: The retracted torn pectoralis major tendon is identified, often with a hematoma.
- Mobilization: The tendon is mobilized, and adhesions are released.
- Fixation: Suture anchors or transosseous tunnels are created in the humerus at the anatomical insertion site. Strong sutures are passed through the tendon and secured to the bone, aiming for a tension-free repair.
- Augmentation: For chronic tears or poor tissue quality, allograft or autograft may be used to augment the repair.
-
Latissimus Dorsi Transfer for Irreparable Rotator Cuff:
- Approach: Posterior incision extending into the axilla, or two separate incisions.
- Harvest: The latissimus dorsi muscle is dissected free, preserving its neurovascular pedicle (thoracodorsal nerve and vessels). The tendon is detached from the humerus.
- Transfer: The muscle is tunneled superiorly, either superficially or deep to the deltoid, to the posterior-superior aspect of the shoulder.
- Fixation: The tendon is reattached to the greater tuberosity, often augmenting the infraspinatus footprint, typically with suture anchors or transosseous sutures.
Complications & Management
Surgical interventions involving shoulder girdle muscles, despite advancements, carry inherent risks. A thorough understanding of potential complications and their management is crucial.
Common Complications
-
Infection:
- Incidence: Varies by procedure (0.5-2% for arthroscopy, higher for open procedures or arthroplasty).
- Management: Superficial infections may respond to antibiotics. Deep infections often require surgical debridement, irrigation, retention or removal of hardware/implants, and prolonged antimicrobial therapy.
-
Neurovascular Injury:
- Incidence: Axillary nerve (2-5% in dislocations/fractures, <1% in arthroscopy), suprascapular nerve (<1%), long thoracic nerve (<1%).
- Management: Prevention is key (anatomical knowledge, careful dissection, monitoring). Post-operative: observation for neurapraxia, nerve conduction studies/EMG for persistent deficits. Surgical exploration for nerve laceration.
-
Stiffness (Arthrofibrosis):
- Incidence: Common (5-20%), particularly after rotator cuff repair or fracture fixation.
- Management: Aggressive physiotherapy. Manipulation under anesthesia (MUA). Arthroscopic capsular release for refractory cases.
-
Rotator Cuff Rerear:
- Incidence: Highly variable (10-50%), dependent on tear size, tissue quality, patient factors, and repair technique.
- Management: Asymptomatic retears may be observed. Symptomatic retears may require revision repair (if tissue allows), augmentation, or muscle transfer (e.g., latissimus dorsi).
-
Deltoid Dehiscence/Avulsion:
- Incidence: Rare but debilitating (<1%), typically after large open procedures or revision surgery.
- Management: Early surgical repair with strong sutures or anchors, often augmented with allograft or biologic patch. Prolonged immobilization.
-
Implant Failure:
- Incidence: Low (<5%), includes anchor pull-out, plate/screw breakage.
- Management: Revision surgery with removal of failed implants and re-fixation.
-
Nonunion/Malunion (Fractures):
- Incidence: 5-10% for complex proximal humerus fractures.
- Management: Revision ORIF with bone grafting, conversion to arthroplasty (hemiarthroplasty or rTSA).
-
Persistent Pain:
- Incidence: Variable, can be multifactorial (residual pathology, nerve irritation, psychological).
- Management: Comprehensive evaluation, targeted injections, physiotherapy, pain management specialists.
- Anesthetic Complications: Related to interscalene block (phrenic nerve palsy, pneumothorax) or general anesthesia.
Complications and Salvage Strategies
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Infection (Deep) | 0.5-2% | Surgical debridement, irrigation, hardware removal (if applicable), culture-directed IV antibiotics for 4-6 weeks. May require staged reconstruction. |
| Axillary Nerve Palsy | <1% (surgery) | Observation for 3-6 months. EMG/NCS for follow-up. If no recovery, surgical exploration, neurolysis, or nerve graft. Chronic palsy may require deltoid transfer or arthrodesis. |
| Rotator Cuff Rerear | 10-50% | Physiotherapy for asymptomatic tears. Symptomatic: revision repair (if mobile), partial repair, superior capsule reconstruction, biologic augmentation, tendon transfer (e.g., LDD transfer for postero-superior cuff), reverse total shoulder arthroplasty (for cuff tear arthropathy). |
| Adhesive Capsulitis/Stiffness | 5-20% | Aggressive physical therapy, oral anti-inflammatories, intra-articular steroid injections. If refractory: manipulation under anesthesia (MUA), arthroscopic capsular release. |
| Deltoid Dehiscence | Rare (<1%) | Prompt surgical repair with strong non-absorbable sutures to acromion/bone. May require augmentation with allograft or synthetic patch. Prolonged immobilization (6-8 weeks). |
| Pectoralis Major Rerupture | Rare | Revision direct repair. If significant tissue loss or chronic: augmentation with allograft (e.g., Achilles tendon) or synthetic mesh. |
| Scapular Winging (Long Thoracic N. Palsy) | Rare (<1%) | Observation for up to 2 years. If persistent and symptomatic: nerve transfer (e.g., intercostal to long thoracic) or muscle transfers (e.g., pectoralis major to inferior angle of scapula, or transfer of rhomboids to glenoid neck). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical procedure itself, ensuring optimal functional recovery and minimizing the risk of complications. Protocols are typically phased, guided by the specific procedure, tissue integrity, and surgeon's preference.
General Principles
- Protection of Repair: The primary goal in the early phase is to protect the surgical repair from excessive stress while preventing stiffness.
- Progressive Loading: Gradual increase in range of motion (ROM) and strength training as healing progresses.
- Pain Management: Effective analgesia is crucial for patient compliance with rehabilitation.
- Patient Education: Patients must understand the importance of adherence to the protocol and the expected timeline for recovery.
Phased Rehabilitation Example (Rotator Cuff Repair)
This is a typical protocol, but specific variations exist based on tear size, repair quality, and patient factors.
Phase I: Immobilization & Passive Motion (Weeks 0-6)
- Goal: Protect repair, minimize pain, prevent stiffness.
- Immobilization: Arm in sling (often with abduction pillow) continuously, removed only for exercises and hygiene. Duration typically 4-6 weeks for most repairs; longer for massive or revision tears.
-
Exercises:
- Passive Range of Motion (PROM): Initiated immediately or within a few days, performed by therapist or non-operative arm. Forward flexion, external rotation (limited to 0-30 degrees), internal rotation, abduction (limited). Scapular protraction/retraction.
- Elbow/Wrist/Hand ROM: Active exercises to prevent stiffness in uninvolved joints.
- Pendulum Exercises: Gentle, gravity-assisted swings.
- Precautions: NO active ROM of the shoulder. NO lifting, pushing, or pulling. NO weight-bearing on the operative arm. Avoid sudden movements.
Phase II: Early Active Motion & Light Strengthening (Weeks 6-12)
- Goal: Restore full passive ROM, initiate active motion, develop muscular control.
- Immobilization: Sling discontinued gradually (e.g., use only for sleep or public).
-
Exercises:
- Active-Assisted Range of Motion (AAROM): Use of pulleys, cane, or non-operative arm to assist movements.
- Active Range of Motion (AROM): Gradual introduction of unassisted active ROM, starting with gravity-eliminated positions.
- Isometrics: Gentle isometric strengthening of rotator cuff and deltoid, initiated once AROM is established and pain-free.
- Scapular Stabilization: Exercises targeting the trapezius , rhomboids , and serratus anterior (e.g., prone scapular squeezes, wall slides).
- Precautions: NO heavy lifting. Avoid pain with exercises.
Phase III: Progressive Strengthening & Advanced Mobility (Weeks 12-24)
- Goal: Restore full pain-free AROM, significantly improve strength, prepare for return to activity.
-
Exercises:
- Progressive Resistance Exercises (PREs): Using resistance bands, light weights. Concentric and eccentric strengthening of deltoid , rotator cuff (internal and external rotators), and scapular stabilizers .
- Proprioceptive Training: Balance and coordination exercises.
- Endurance Training: Increased repetitions with lighter resistance.
- Core Strengthening: Important for overall kinetic chain stability.
- Precautions: Avoid ballistic or high-impact activities. Progress resistance cautiously.
Phase IV: Return to Activity (Months 6+)
- Goal: Gradual return to sports, work, and recreational activities.
-
Exercises:
- Sport-Specific/Work-Specific Drills: Progressive simulation of activities.
- Plyometrics: For overhead athletes.
- Maintenance Program: Continued strengthening and flexibility exercises.
- Timeline: Return to light work 3-4 months; heavy labor or overhead sports 6-12 months, depending on the specific procedure and individual progress. Full recovery can take up to 12-18 months.
Considerations for Specific Procedures
- Pectoralis Major Repair: Similar progression to rotator cuff, with emphasis on protecting internal rotation and adduction during early phases.
- Latissimus Dorsi Transfer: Specific attention to protecting the transfer site, often involving more prolonged immobilization and slower progression of active motion, especially internal rotation and adduction.
-
Shoulder Arthroplasty (TSA/rTSA):
- TSA: Follows a rotator cuff repair protocol, as the subscapularis is typically repaired. Focus on regaining external rotation.
- rTSA: Different biomechanics. Deltoid function is paramount; rotator cuff not actively engaged for motion. Early passive/active-assisted elevation is emphasized. Avoid internal rotation/adduction past neutral (posterior dislocation risk) and combined internal rotation/adduction/extension (anterior dislocation risk).
Summary of Key Literature / Guidelines
The understanding and management of shoulder girdle muscular pathologies continue to evolve, guided by robust clinical research and consensus guidelines.
-
Rotator Cuff Repair:
- The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines provide evidence-based recommendations for rotator cuff tears, emphasizing patient selection, surgical timing, and rehabilitation.
- Numerous studies highlight factors influencing retear rates, including tear size, muscle quality (fatty infiltration, atrophy), age, and smoking status. Double-row and transosseous equivalent repairs have shown biomechanical superiority but clinical superiority over single-row is debated, particularly for smaller to medium tears.
- Biologic augmentation (e.g., PRP, stem cells, xenografts/allografts) continues to be an active area of research, with current evidence not consistently demonstrating significant clinical benefit in reducing retear rates or improving outcomes for routine repairs.
-
Pectoralis Major Ruptures:
- A strong consensus exists for surgical repair of acute, complete pectoralis major ruptures in active individuals due to superior strength and functional outcomes compared to non-operative management. Chronic tears may also benefit from repair, often with augmentation.
-
Scapular Winging:
- Management of long thoracic nerve palsy often involves an initial period of observation (up to 18-24 months) due to potential for spontaneous recovery. If conservative measures fail, various muscle transfers (e.g., pectoralis major transfer with fascia lata graft to the inferior pole of the scapula for serratus anterior paralysis) have demonstrated functional improvements.
-
Latissimus Dorsi Transfer:
- Established as a viable option for irreparable posterosuperior rotator cuff tears, particularly in younger, active patients, aiming to restore external rotation and elevation. Long-term studies demonstrate sustained improvement in function and pain.
-
Deltoid Preservation:
- Emphasis on minimizing deltoid detachment or injury during shoulder approaches, as deltoid integrity is paramount for shoulder function. Axillary nerve monitoring during surgery is becoming more common, especially in revision cases.
Continued research focusing on tendon-to-bone healing, biologic augmentation, biomechanical analysis of repairs, and optimizing rehabilitation protocols will further refine surgical strategies for shoulder girdle muscular pathologies. The orthopedic surgeon must remain abreast of these developments to provide optimal patient care.
