Proximal 5th Metatarsal Fractures: Surgical Techniques & Management
Key Takeaway
Fractures of the proximal fifth metatarsal require precise classification and tailored management. While acute, non-displaced avulsion fractures often heal with conservative care, metaphyseal-diaphyseal junction fractures exhibit higher nonunion rates due to watershed vascularity. Surgical intervention, primarily via intramedullary screw fixation or corticocancellous inlay grafting, is frequently indicated for competitive athletes, displaced fractures, or chronic nonunions to ensure optimal biomechanical restoration and accelerated return to play.
METATARSALS: ADVANCED PATHOPHYSIOLOGY AND MANAGEMENT
Fractures of the metatarsals represent a significant portion of foot and ankle trauma encountered by the orthopedic surgeon. Among these, a great deal of academic and clinical attention has been directed toward the treatment of fractures involving the proximal portion of the fifth metatarsal. The unique vascular anatomy—specifically the watershed area at the metaphyseal-diaphyseal junction—combined with the complex biomechanical forces exerted by the peroneus brevis and the lateral band of the plantar fascia, makes this region particularly susceptible to delayed union and nonunion.
While midfoot trauma can present in various complex patterns, such as divergent Lisfranc fracture-dislocations requiring extensive arthrodesis for stabilization, isolated fifth metatarsal fractures demand a highly specific, classification-driven approach.
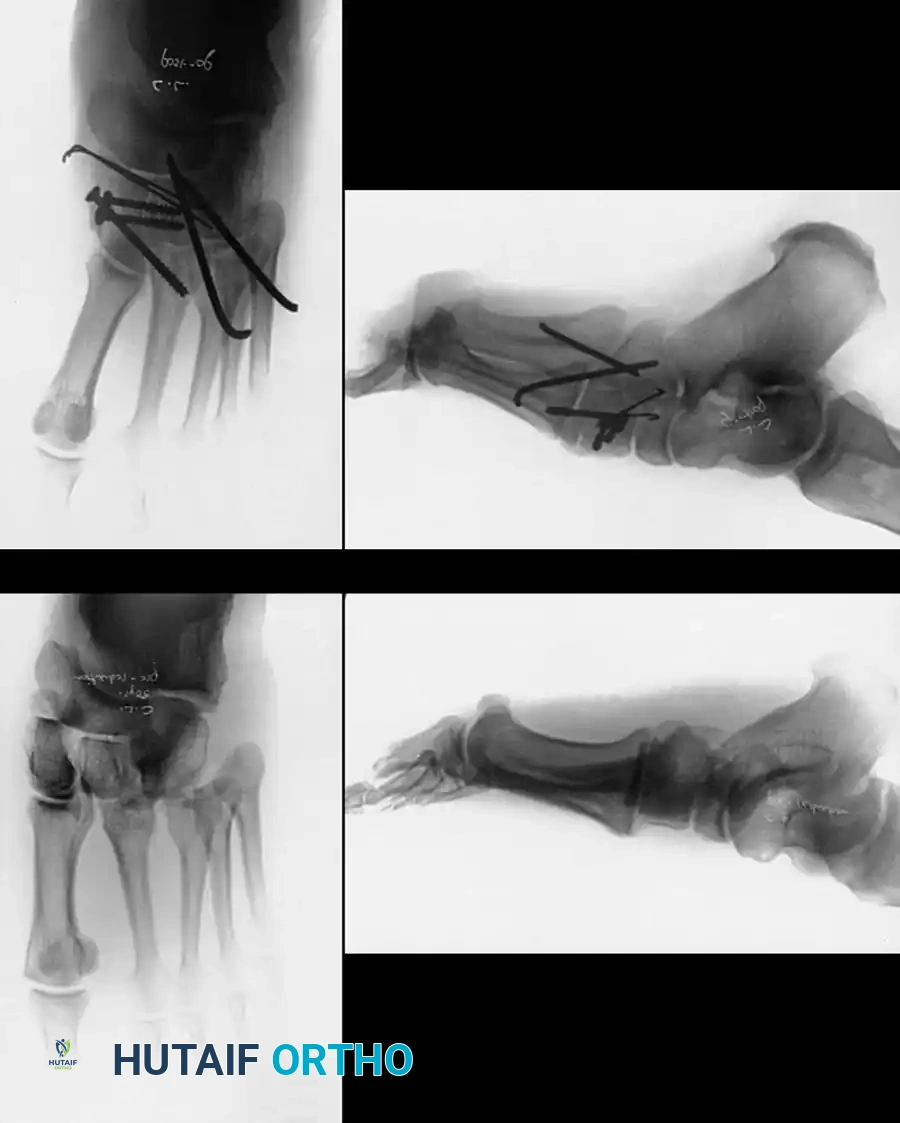
Fig. 86-42 Divergent Lisfranc fracture-dislocation. A and B, Preoperative radiographs demonstrating intercuneiform and naviculocuneiform disruption. C and D, Postoperative radiographs following intracuneiform arthrodesis for stabilization in a high-BMI patient. This highlights the spectrum of severe midfoot trauma that often accompanies or parallels metatarsal injuries.
Classification of Proximal Fifth Metatarsal Fractures
Accurate classification is the cornerstone of appropriate clinical decision-making. The classification system described by DeLee provides a robust framework based on anatomic location, chronicity, and articular involvement.
Table 86-1: DeLee Classification of Fractures of the Base of the Fifth Metatarsal
* Type I: Acute fractures at the metaphyseal-diaphyseal junction.
* Type IA: Nondisplaced.
* Type IB: Displaced or comminuted (or both).
* Type II: Fractures at the metaphyseal-diaphyseal junction with clinical or radiographic evidence of previous injury (e.g., prodromal pain, cortical hypertrophy, canal sclerosis).
* Type III: Fractures of the styloid process of the fifth metatarsal (Avulsion fractures).
* Type IIIA: Without involvement of the fifth metatarsocuboid joint.
* Type IIIB: With involvement of the fifth metatarsocuboid joint.
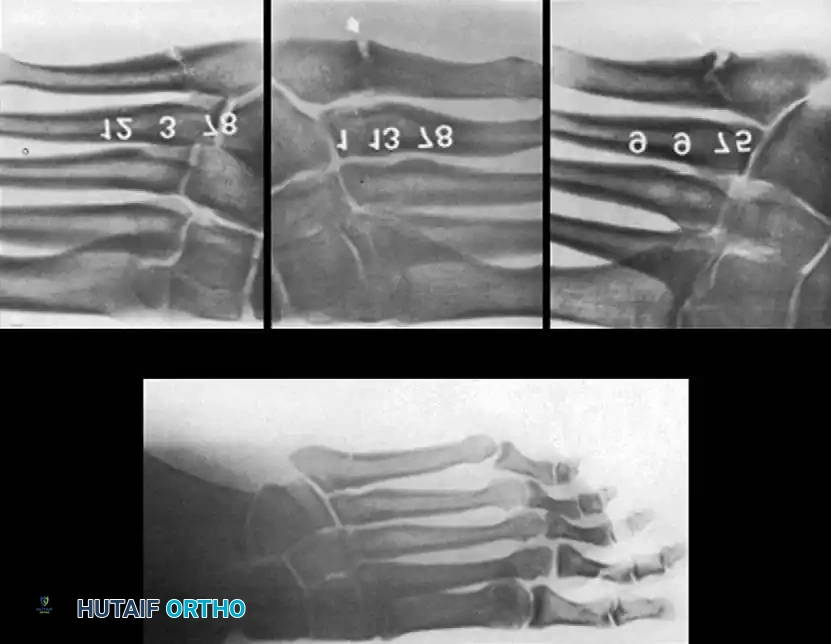
Fig. 86-43 A-D. A, Type IA, acute fracture of the proximal diaphysis of the fifth metatarsal. B-D, Type II fractures demonstrating varying degrees of sclerosis and canal obliteration.
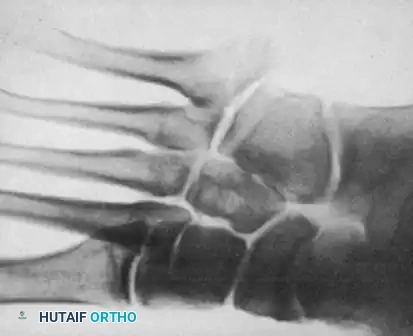
Fig. 86-43 E-F. E, Type IIIA, fracture of the styloid process without articular involvement. F, Type IIIB, fracture of the styloid process with joint involvement.
Biomechanics and Mechanism of Injury
Type I and Type II fractures occur 2 cm or more from the tip of the tuberosity. These are typically caused by vertical or medial-lateral forces applied to the forefoot. The watershed vascular supply in this specific zone severely compromises the healing potential, leading to the notorious reputation of the "Jones fracture."
Conversely, the mechanism of injury for Type III (styloid avulsion) fractures is an inversion injury to the plantar-flexed foot. The sudden tension from the lateral band of the plantar fascia and the peroneus brevis tendon results in an avulsion of the tuberosity.
NON-OPERATIVE MANAGEMENT PROTOCOLS
Treatment of Type I fractures depends heavily on the specific fracture subtype and the functional demands of the patient.
Type I Acute Fractures
For an acute Type IA fracture in a non-competitive athlete, conservative management is the standard of care. The initial protocol involves a non–weight-bearing short leg cast worn for 6 to 8 weeks. This is followed by a weight-bearing cast or controlled ankle motion (CAM) boot until clinical and radiographic union is achieved.
Clinical Pearl: Even with strict non–weight-bearing immobilization for 6 to 8 weeks, Type I fractures have a reported nonunion rate ranging from 7% to 28%. The adjunctive use of electrical bone stimulation or pulsed electromagnetic field (PEMF) therapy may improve healing rates; however, these modalities cannot substitute for rigid internal fixation in high-performance athletes.
Type II Chronic Fractures
In Type II fractures, where clinical or radiographic evidence of chronic injury is manifested by partial or complete medullary canal obliteration and cortical sclerosis, non–weight-bearing casting may occasionally yield satisfactory results. The period of immobilization is generally extended to approximately 8 weeks. However, orthopedic surgeons must warn patients that refracture is highly common in this category due to the biologically inferior sclerotic bone bridging the fracture site.
Type III Styloid Avulsion Fractures
Type III fractures generally have an excellent prognosis with conservative care. They are treated satisfactorily in a short leg cast for 3 weeks, followed by transition to a well-molded arch support or stiff-soled shoe. While nonunions of Type III fractures can occur, they are rarely symptomatic. If they become painful, they are easily managed with simple excision of the avulsed fragment and advancement of the peroneus brevis.
Wiener, Linder, and Giattini conducted a prospective evaluation of Type III injuries (n = 60). Patients were randomly assigned to either a soft Jones-type dressing or a short leg cast. The study found that fractures healed in all patients at an average of 44 days. Crucially, patients treated with a compressive soft dressing who were allowed to bear weight in a cast boot required a significantly shorter recuperation time and reported better modified foot scores than those subjected to rigid cast immobilization.
OPERATIVE MANAGEMENT: INDICATIONS AND PLANNING
Surgical intervention is indicated under the following conditions:
1. Type I Fractures: Delayed union or nonunion failing to heal clinically at 8 to 12 weeks.
2. Type IB Fractures: Displaced and comminuted fractures in competitive athletes to decrease disability time and prevent nonunion.
3. Type II Fractures: Indicated for competitive athletes and individuals whose occupational demands preclude prolonged non–weight-bearing immobilization.
4. Type IIIB Fractures: Open reduction and internal fixation (ORIF) is rarely necessary for avulsion fractures but is reserved for significantly displaced intra-articular fractures in highly competitive individuals to restore the articular congruity of the metatarsocuboid joint.



Fig. 86-44 A-C. Preoperative radiographs of a Type IIIB (DeLee) fifth metatarsal fracture demonstrating significant intra-articular displacement requiring surgical reduction.


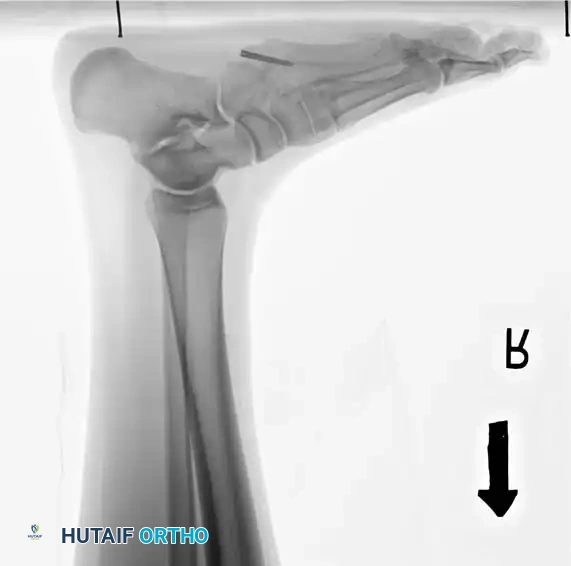
Fig. 86-44 D-F. Postoperative radiographs following precise open reduction and internal screw fixation, restoring the articular surface.
For Type I and Type II fractures requiring surgical intervention, two operative treatments have proven highly successful:
1. Intramedullary Fixation utilizing a 4.5-mm (or larger) malleolar or cannulated screw.
2. Corticocancellous Inlay Bone Grafting (Torg Technique) with complete clearing of the sclerotic medullary canal.
Surgical Warning: Glasgow et al., in a critical review of the surgical management of these fractures, found that the use of screws smaller than a 4.5-mm malleolar screw was directly associated with biomechanical failure and refracture. Furthermore, they attributed the failure of corticocancellous grafting to the use of undersized grafts and incomplete medullary reaming.
While a 4.5-mm malleolar screw is the historical gold standard, modern osteosynthesis allows for a variety of screw types, including variable-pitch compression screws, 5.5-mm (and larger) cannulated screws, and non-cannulated screws with low-profile heads. The choice depends on surgeon preference and the specific medullary canal diameter measured on preoperative templating.

Fig. 86-45 A-C. Type IA (DeLee) fifth metatarsal fracture in a collegiate soccer player, representing an ideal candidate for early intramedullary fixation.





Fig. 86-45 D-F. Postoperative imaging after robust fixation utilizing a variable pitch compression screw, ensuring excellent compression across the fracture site.
SURGICAL TECHNIQUE 86-14: INTERNAL FIXATION WITH A MALLEOLAR SCREW
As demonstrated by Donley et al., the sural nerve—particularly its dorsolateral branch—lies in perilous proximity to the insertion point of the intramedullary screw. Consequently, this technique should not be performed purely percutaneously without direct visualization. Sufficient exposure must be obtained to identify and retract this cutaneous nerve branch.
Step-by-Step Procedure
- Exposure: Expose the proximal 2 cm of the fifth metatarsal on its dorsolateral surface via a longitudinal or slightly curvilinear incision.
- Nerve Protection: Incise the skin carefully. Observe and protect the two vulnerable branches of the sural nerve (one dorsal and one straight lateral).
- Tendon Management: If the insertion of the peroneus brevis obscures the optimal starting portal for the drill, carefully elevate a small portion of the tendon from the bone.
- Guidewire Placement: Use a Kirschner wire to locate the medullary canal. Surgical Pearl: This step can be technically demanding. The drill must lie almost parallel to the lateral border of the hindfoot. Starting slightly dorsal and medial to what appears to be the anatomic center of the tuberosity ("high and inside") helps prevent lateral cortical blowout.
- Drilling: Drive a 3.2-mm drill bit into the medullary canal. Confirm its intraosseous location using multi-planar fluoroscopy (anteroposterior and lateral radiographs).
- Tapping: Tap the narrow isthmus portion of the canal with a 3.2-mm cortical tap and sleeve. Although many modern malleolar screws are self-tapping, pre-tapping the dense diaphyseal cortex prevents excessive torque and iatrogenic comminution.
- Measurement: Estimate the required length of the screw from the intraoperative radiographs. The screw threads must bypass the fracture site and engage the dense diaphyseal bone distal to the fracture.
- Insertion: Countersink the entry portal to prevent hardware prominence, which can cause painful shoe wear, and insert the screw.
- Grafting (Optional): If exposing a nonunion, applying a small cancellous bone graft may enhance union. If severe cortical thickening and sclerosis are present, grafting is highly recommended.
- Closure: Verify final screw placement and fracture compression with fluoroscopy, then close the wound in standard layered fashion.

Fig. 86-46 Internal fixation of fifth metatarsal fracture. A and B, Position of the drill bit confirmed with AP and lateral radiographs. C, A 6.5-mm malleolar screw and small iliac cancellous bone graft were utilized due to cortical hypertrophy and a history of repeated fractures. D, Several months post-union, the screw was removed at the patient’s request, though it may remain in place indefinitely.
Postoperative Protocol for Screw Fixation
A well-padded, short leg, non-walking cast extending to the toes is applied and worn for 6 weeks. This is followed by a walking cast or CAM boot for an additional 4 to 6 weeks, or until the fracture has united clinically and radiographically. Return to competitive sports is strictly discouraged until complete healing is confirmed, which typically requires 10 to 12 weeks.
SURGICAL TECHNIQUE 86-15: INLAY BONE GRAFT (TORG TECHNIQUE)
A consistent pathological finding in the presence of a fifth metatarsal nonunion is the complete obliteration of the medullary canal by dense, avascular sclerotic bone along the fracture margins. Torg et al. postulated that the tendency of this fracture toward nonunion, delayed union, or refracture is directly linked to this poorly organized sclerotic bone, which acts as a mechanical and biological barrier.
The primary objective of the Torg technique is to reestablish the continuity of the medullary canal by excising the sclerotic bone and facilitating osteogenesis via a structural corticocancellous inlay graft.
Step-by-Step Procedure
- Approach: Approach the base of the fifth metatarsal through a curvilinear dorsolateral incision. Expose the fracture site subperiosteally.
- Osteotomy: Using a fine drill, outline a rectangular piece of bone measuring approximately 0.7 cm × 2.0 cm, centered directly over the fracture line. Remove this rectangular window with a sharp osteotome.
- Canal Preparation: Aggressively curet and drill the medullary canal proximally and distally until all sclerotic bone has been eradicated and the normal continuity of the medullary canal is reestablished.
- Graft Harvest: Through a separate incision, harvest an autogenous corticocancellous bone graft measuring 0.7 cm × 2.0 cm from
Associated Surgical & Radiographic Imaging

You Might Also Like
