Metacarpal Head Fractures: Comprehensive Surgical Management

Key Takeaway
Intraarticular metacarpal head fractures present complex reconstructive challenges due to their intricate articular geometry and precarious vascular supply. Typically resulting from axial loading, these injuries demand meticulous anatomical reduction to restore the metacarpophalangeal joint's cam mechanism. This comprehensive guide details evidence-based surgical approaches, from percutaneous Kirschner wire fixation to rigid plate osteosynthesis, emphasizing techniques to mitigate complications such as osteonecrosis and post-traumatic stiffness.
METACARPAL HEAD FRACTURES
Intraarticular metacarpal head fractures are relatively uncommon but highly challenging injuries that demand precise anatomical restoration. Occurring predominantly in the fourth and fifth metacarpals, these fractures are most often caused by the patient sustaining an axial load to a clenched fist—typically from striking a solid object. The resulting impaction, shear, or avulsion forces disrupt the delicate articular congruity of the metacarpophalangeal (MCP) joint.
Because the metacarpal head is largely intra-articular and possesses a tenuous blood supply, fractures in this region are fraught with complications, including post-traumatic arthritis, profound joint stiffness, and osteonecrosis (avascular necrosis). For the practicing orthopedic surgeon, mastering the nuances of biomechanics, surgical approaches, and rigid internal fixation is paramount to achieving optimal functional outcomes.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the MCP joint's anatomy is the foundation of successful surgical intervention. The MCP joint is a diarthrodial condyloid joint, allowing for flexion, extension, abduction, adduction, and limited circumduction.
The Cam Mechanism
The metacarpal head is not perfectly spherical; it is eccentric, being wider on its palmar aspect than on its dorsal aspect. In the sagittal plane, the radius of curvature decreases from palmar to dorsal. This unique geometry creates the "cam effect."
* In Extension: The collateral ligaments are lax, allowing for abduction and adduction of the digits.
* In Flexion: The proximal phalanx glides onto the wider palmar portion of the metacarpal head, maximizing the distance from the center of rotation. This tightly stretches the collateral ligaments, locking the digit in stable flexion and preventing lateral deviation.
Clinical Pearl: Any intra-articular step-off or malunion that alters the cam profile will lead to abnormal ligamentous tension, resulting in a loss of flexion or chronic joint instability. Anatomical reduction must restore both the articular contour and the precise width of the metacarpal head.
Vascular Anatomy and the Risk of Osteonecrosis
The vascular supply to the metacarpal head is precarious. It is primarily perfused by intraosseous vessels entering the metaphyseal flare and capsular vessels supplying the non-articular base of the head. Displaced fractures, particularly those with significant comminution or those requiring extensive dorsal surgical dissection, severely compromise this blood supply. This anatomical vulnerability explains the high incidence of osteonecrosis following metacarpal head fractures, even after successful osteosynthesis.
CLINICAL AND RADIOGRAPHIC EVALUATION
Physical Examination
Patients typically present with localized swelling, ecchymosis, and exquisite tenderness over the affected MCP joint. A thorough examination must assess for:
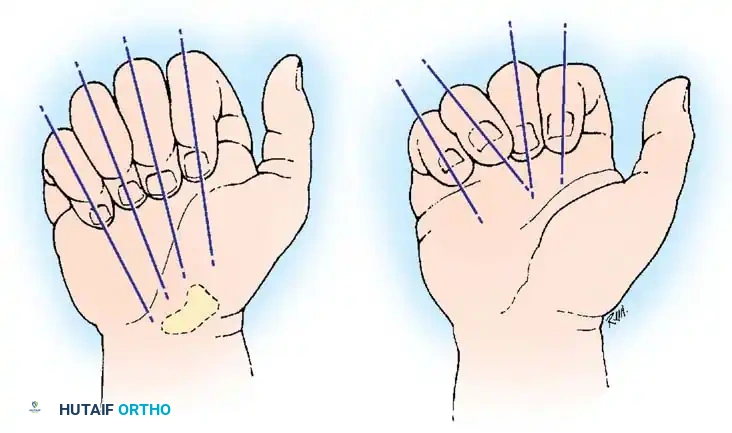
* Rotational Malalignment: Evaluated by observing the digital cascade. In normal flexion, all digits should point toward the scaphoid tubercle. Scissoring or overlapping of the digits indicates a rotational deformity that mandates surgical correction.
* Extensor Mechanism Integrity: Central slip or sagittal band injuries may occur concomitantly, leading to an extensor lag or subluxation of the extensor tendon.
* Open Wounds: "Fight bites" (human tooth strikes) must be meticulously ruled out, as they require urgent irrigation, debridement, and broad-spectrum antibiotic coverage due to the risk of Eikenella corrodens and mixed flora infections.
Imaging Protocols
Standard posteroanterior (PA), lateral, and oblique radiographs of the hand are mandatory. However, the complex overlapping anatomy of the metacarpal heads on a true lateral view often obscures fracture details.
- The Brewerton View: Highly recommended for evaluating the metacarpal head and collateral ligament avulsions. The patient's fingers are placed flat on the cassette with the MCP joints flexed to 65 degrees, and the X-ray tube is angled 15 degrees from ulnar to radial.
- Computed Tomography (CT): A non-contrast CT scan with fine (1 mm) sagittal and coronal reconstructions is the gold standard for preoperative planning. It precisely delineates the degree of articular comminution, fragment size, and step-off, dictating whether the fracture is amenable to screw fixation, K-wire pinning, or requires a more complex reconstructive approach.
CLASSIFICATION OF METACARPAL HEAD FRACTURES
While several classification systems exist, the McElfresh and Dobyns classification is highly practical for guiding surgical decision-making:
1. Epiphyseal Fractures: Horizontal or vertical splits through the articular surface.
2. Collateral Ligament Avulsion Fractures: Typically involving the radial or ulnar condyle.
3. Osteochondral Fractures: Often subtle, requiring CT or MRI for definitive diagnosis.
4. Comminuted Fractures: High-energy impaction injuries with multiple articular fragments.
5. Boxer's Fractures with Intra-articular Extension: Metacarpal neck fractures that propagate into the head.
INDICATIONS FOR OPERATIVE INTERVENTION
Nonoperative management (immobilization in an intrinsic-plus splint for 3 weeks followed by early motion) is strictly reserved for truly nondisplaced fractures with less than 1 mm of articular step-off and no rotational deformity.
Absolute Indications for Surgery:
* Articular step-off or gap greater than 1 mm.
* Involvement of more than 25% of the articular surface.
* Any degree of rotational malalignment.
* Open fractures (requiring I&D and stabilization).
* Multiple adjacent metacarpal fractures leading to loss of the transverse metacarpal arch.
* Joint subluxation or instability.
SURGICAL APPROACHES
The Dorsal Approach to the MCP Joint
The dorsal approach provides optimal exposure of the metacarpal head while protecting the neurovascular bundles.
- Incision: A longitudinal or slightly curvilinear incision is made centered over the dorsal aspect of the affected MCP joint.
- Extensor Mechanism Management:
- Tendon Splitting: The extensor digitorum communis (EDC) tendon can be split longitudinally in its midline. This provides direct access to the dorsal capsule but may lead to postoperative tendon adhesions.
- Tendon Retraction (Chamfering): Alternatively, the sagittal band can be incised on the ulnar or radial side, allowing the entire extensor mechanism to be retracted laterally. This is generally preferred as it preserves the gliding surface of the tendon.
- Capsulotomy: A longitudinal arthrotomy is performed. The capsule is carefully elevated to expose the fracture.
- Preservation of Soft Tissue: It is critical to minimize stripping of the collateral ligaments and the palmar capsule to preserve the remaining blood supply to the articular fragments.
Surgical Warning: Aggressive soft tissue stripping around the metacarpal neck and head will inevitably devascularize the fracture fragments, exponentially increasing the risk of postoperative osteonecrosis. Employ "no-touch" techniques for small articular fragments whenever possible.
TECHNIQUES OF INTERNAL FIXATION
The choice of fixation depends entirely on the fracture pattern, fragment size, and bone quality. The primary goal is absolute stability of the articular surface to allow for immediate postoperative mobilization.
Kirschner Wire Fixation and the Risk of Osteonecrosis
For fractures with fragments too small to accommodate screws, or in cases of severe comminution where rigid fixation is impossible, Kirschner wire (K-wire) fixation remains a viable, albeit less stable, option. K-wires can be used to "skewer" small fragments or act as a buttress.
Consider the classic case documented by McElfresh and Dobyns, illustrating the precarious nature of metacarpal head vascularity:
FIGURE 67-39 A: Radiograph of the hand of a 20-year-old man who sustained a horizontally directed fracture of the fourth metacarpal head. Note the palmar fragment displaced proximally, disrupting the cam mechanism.

FIGURE 67-39 B: The fracture was reduced via an open approach and held in place with multiple crossed Kirschner wires. While K-wires provide provisional stability, they lack interfragmentary compression.

FIGURE 67-39 C: At 4 months postoperatively, radiographs demonstrated early osteonecrosis of the metacarpal head. The sclerosis and early collapse are indicative of the disrupted intraosseous blood supply inherent to this injury pattern.

FIGURE 67-39 D: At 2.5 years, radiographs showed some biological remodeling, but definite incongruities of the metacarpal head persisted, predisposing the patient to early-onset post-traumatic osteoarthritis. (From McElfresh EC, Dobyns JH: Intra-articular metacarpal head fractures, J Hand Surg 8A:383, 1983.)
Headless Compression Screw Fixation
For simple vertical or oblique split fractures (e.g., collateral ligament avulsion fractures with a large bony fragment), headless compression screws (1.5 mm to 2.4 mm) are the current gold standard.
1. The fracture is anatomically reduced and provisionally held with a reduction forceps or a 0.035-inch K-wire.
2. The guidewire for the headless screw is inserted perpendicular to the fracture plane to maximize compression.
3. The screw is inserted and countersunk beneath the articular cartilage to prevent mechanical impingement during MCP joint motion.
4. Multiple screws may be used if the fragment size permits, providing rotational stability.
Plate and Screw Osteosynthesis for Complex Fracture Patterns
When metacarpal head fractures extend into the metaphyseal shaft, or when multiple adjacent digits are involved, rigid plate osteosynthesis is required to restore the longitudinal and transverse arches of the hand. Low-profile titanium mini-fragment plates (1.5 mm or 2.0 mm systems) are utilized.

FIGURE 67-40 A: Preoperative radiograph demonstrating displaced, closed fractures of the metaphyseal shafts of the right middle, ring, and small digits, accompanied by a highly comminuted intraarticular fracture of the head and distal metaphysis of the index finger. This complex injury pattern results in profound instability and loss of the hand's architectural framework.

FIGURE 67-40 B: Postoperative radiograph demonstrating tubular plate fixation of the index, middle, ring, and small metacarpals. For the index finger, the plate acts as a neutralization/buttress plate, bridging the comminuted metaphyseal segment while securing the reconstructed articular head. (From Hastings H II: Unstable metacarpal and phalangeal fractures treatment with screws and plates, Clin Orthop Relat Res 214:37, 1987.)
Technical Considerations for Plating:
* T-Plates and Condylar Plates: Specifically designed for periarticular fractures, allowing multiple small screws to capture the metacarpal head fragments.
* Dorsal Placement: Plates are typically placed dorsally. Care must be taken to ensure the distal edge of the plate does not impinge on the dorsal capsule during MCP joint extension.
* Lag Screw Principle: Whenever possible, articular fragments should be lagged together independently before applying the neutralization plate.
Alternative and Salvage Techniques
- Cerclage Wiring: In cases of severe "eggshell" comminution where screws would cause further fragmentation, fine cerclage wires or absorbable sutures can be used to bundle the fragments together (ligamentotaxis).
- External Fixation: Dynamic external fixation can be employed for highly comminuted, open fractures with significant bone loss, utilizing the principle of ligamentotaxis to maintain joint space while soft tissues heal.
- Primary Arthroplasty: In elderly, low-demand patients with non-reconstructable comminution, primary silicone arthroplasty may be considered to allow for immediate motion and pain relief.
POSTOPERATIVE REHABILITATION PROTOCOL
The ultimate success of metacarpal head fracture surgery relies heavily on the postoperative rehabilitation phase. The MCP joint is notoriously prone to stiffness due to capsular contracture and extensor tendon adhesions.
- Phase I (0-2 Weeks): If rigid internal fixation was achieved, the patient is placed in a forearm-based intrinsic-plus splint (wrist extended 30 degrees, MCP joints flexed 70-90 degrees, IP joints free). Active range of motion (AROM) of the IP joints is encouraged immediately. Gentle, supervised AROM of the MCP joint may begin within 3 to 5 days postoperatively.
- Phase II (2-6 Weeks): Splinting is transitioned to between exercises and at night. Active and active-assisted ROM exercises are progressed. Dynamic flexion/extension splinting may be initiated if stiffness develops.
- Phase III (6+ Weeks): Strengthening exercises begin once radiographic evidence of clinical union is observed. Full unrestricted activity is typically allowed by 10 to 12 weeks.
Pitfall: Prolonged immobilization (greater than 3 weeks) of a metacarpal head fracture, even if treated nonoperatively, will almost certainly result in permanent MCP joint extension contracture. The collateral ligaments will shorten and fibrose in the lax position.
COMPLICATIONS AND MANAGEMENT
1. Osteonecrosis (Avascular Necrosis)
As highlighted in Figure 67-39, AVN is a devastating complication resulting from the disruption of the tenuous blood supply. It presents as late-onset pain, loss of motion, and radiographic evidence of sclerosis and subchondral collapse.
* Management: Early stages may be treated with offloading and NSAIDs. Late-stage collapse with arthritis requires salvage procedures such as MCP joint arthroplasty or, less commonly, arthrodesis.
2. Post-Traumatic Stiffness
The most common complication. It is caused by a combination of articular incongruity, capsular contracture, and extensor tendon adhesions.
* Management: Aggressive hand therapy is the first line of defense. If conservative measures fail after 6 months, surgical intervention via dorsal tenolysis and MCP joint capsulotomy may be indicated.
3. Malunion
Failure to correct rotational deformity or articular step-off leads to malunion. Rotational malunion causes digit scissoring, significantly impairing grip strength and hand function.
* Management: Corrective osteotomy (typically performed at the metacarpal base or shaft to avoid the previously injured joint capsule) is required to realign the digit.
4. Post-Traumatic Osteoarthritis
Even with perfect anatomical reduction, the initial cartilage impact can lead to chondrocyte death and progressive joint degeneration. Patients must be counseled preoperatively about this long-term risk. Symptomatic arthritis is managed with activity modification, injections, and eventually arthroplasty if conservative measures fail.
CONCLUSION
Metacarpal head fractures are complex injuries that threaten the fundamental mechanics of hand function. Successful management requires a high index of suspicion for subtle articular injuries, meticulous preoperative planning with advanced imaging, and a mastery of diverse surgical techniques. By prioritizing anatomical articular reduction, rigid internal fixation, and early mobilization, the orthopedic surgeon can mitigate the high risks of osteonecrosis and stiffness, ultimately restoring the patient's functional capacity.
You Might Also Like