FRACTURES AROUND THE SHOULDER
Fractures of the shoulder girdle represent a diverse and biomechanically complex group of injuries. Encompassing the scapula, clavicle, and proximal humerus, these fractures demand a rigorous understanding of the superior suspensory shoulder complex (SSSC), regional vascularity, and dynamic muscle forces. The ultimate goal of treatment—whether nonoperative or surgical—is the restoration of a painless, stable, and functional articulation that permits early mobilization.
Fractures of the Scapula
The scapula is heavily protected by a robust muscular envelope, meaning that fractures of this bone typically result from high-energy blunt trauma. Consequently, open reduction with or without internal fixation (ORIF) is rarely required for the vast majority of scapular body fractures. Computed tomography (CT) with 3D reconstruction is often necessary for the accurate assessment of these injuries, particularly to evaluate intra-articular glenoid extension and angular deformity.
Most scapular fractures can be managed successfully by supporting the upper extremity in a sling and instituting early active-assisted motion as pain allows. However, specific anatomical disruptions severely compromise the biomechanics of the shoulder and necessitate operative intervention.
Operative Indications for Scapular Fractures
The following fracture patterns may require open reduction and internal fixation:
-
Significantly Displaced Fractures of the Acromion and Lateral Scapular Spine:
Fractures with inferior displacement or retraction of the fragment can cause severe encroachment on the subacromial space. Although extremely rare, if deltoid function is impaired by loss of its origin, or if the subacromial space is significantly compromised (causing impingement of the greater tuberosity during abduction), ORIF is indicated. Fixation is typically achieved using tension band constructs, Kirschner wires, or customized reconstruction plates and screws. -
Fractures of the Coracoid with Acromioclavicular (AC) Separation:
If a fracture of the coracoid base occurs in conjunction with a dislocation of the outer end of the clavicle, the SSSC is doubly disrupted. Open reduction with internal fixation of the coracoid—using a lag screw or heavy nonabsorbable suture—combined with repair or reconstruction of the coracoclavicular (CC) and acromioclavicular ligaments should be performed to restore suspensory stability. -
Glenoid Rim Fractures:
Fractures of the anterior or posterior glenoid rim associated with traumatic glenohumeral dislocations are likely more common than historically recognized. - Surgical Indication: If a glenoid rim fracture involves greater than 25% (one-fourth) of the articulating surface, primary open reduction and internal fixation are required to prevent recurrent instability, subluxation, or accelerated post-traumatic arthropathy.
- Nonoperative Management: Small, minimally displaced glenoid rim fractures following a successfully reduced dislocation should be treated by the standard nonoperative measures used for the dislocation itself.

Fig. 54-7 A, Fracture of anterior glenoid rim usually is produced by medially directed blow to humeral head. B, Large anterior glenoid rim fracture with associated posterior Hill-Sachs lesion. C and D, Open reduction and internal fi xation of glenoid rim fracture with single screw.
Other fractures of the glenoid fossa and scapular neck usually can be treated by sling support of the extremity and early active motion. If the glenoid is markedly angulated or medially displaced (medialization >2 cm or angulation >45 degrees), lateral traction through an olecranon pin for 3 to 4 weeks was historically described, though modern practice favors ORIF via a posterior Judet approach for severe displacements. Fractures of the scapular neck rarely require internal fixation; despite severe radiographic displacement, functional results usually remain quite satisfactory due to the compensatory motion of the scapulothoracic articulation.


Fractures and Fracture-Dislocations of the Shoulder
Fractures and fracture-dislocations of the shoulder are ubiquitous injuries occurring across all age groups. In pediatric populations, these injuries generally involve the proximal humeral epiphysis. While most pediatric physeal fractures are successfully managed by closed reduction and conservative measures due to immense remodeling potential, open reduction occasionally may be required for severely displaced Salter-Harris injuries.
External Fixation of Clavicular Fractures
While intramedullary fixation and superior/anteroinferior plating remain the gold standards for displaced midshaft clavicle fractures, external fixation is a highly specialized technique reserved for specific indications, such as open fractures with severe soft-tissue compromise or infected nonunions.
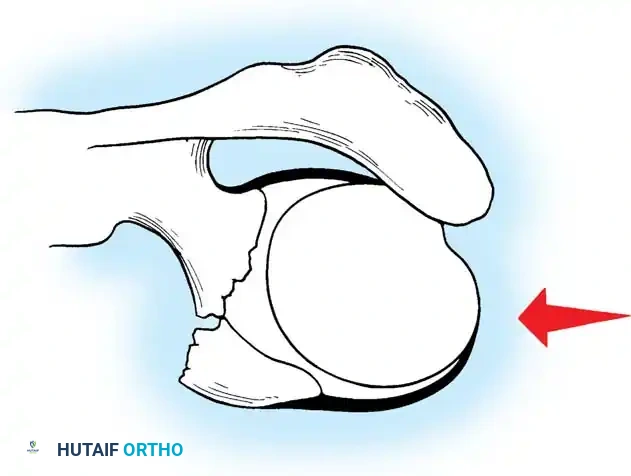

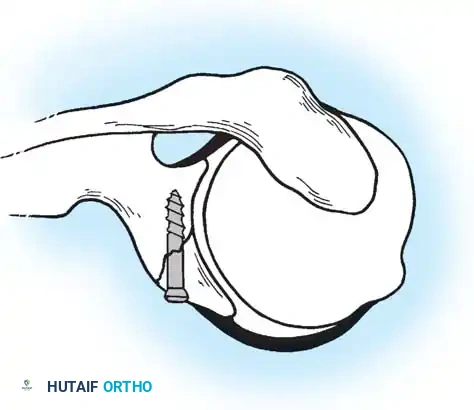
Fig. 54-6 Pin placement in external fi xation of clavicular fractures. (From Schuind F, Pay-Pay E, Andrianni Y, et al: External fi xation of the clavicle for fracture or non-union in adults, J Bone Joint Surg 70A:692, 1988.)
🔪 Surgical Technique 54-3: External Fixation of the Clavicle
1. Exposure: Expose the fracture through a limited curvilinear incision centered over the defect.
2. Debridement: Meticulously débride the wound and fracture site if the injury is open. Crucial Pitfall: Do not strip the periosteum, as the clavicle relies heavily on its periosteal blood supply for union.
3. Neurovascular Protection: In exposing displaced fracture fragments, use extreme care to avoid injury to the subclavian neurovascular structures and the pleural dome lying immediately beneath the middle third of the clavicle.
4. Pin Insertion: Predrill and insert two noninterrupted, threaded, 3-mm, C-model, Blount-type Hoffman pins (or modern equivalents) through the wound into each fragment.
* Medial Pins: Insert from anterior to posterior in an ascending or horizontal direction to strictly avoid the pleural dome.
* Lateral Pins: Insert from superior to inferior in an anterior or almost vertical direction.
5. Frame Assembly: Reduce the fracture under direct vision or fluoroscopy, and connect the pins with a simple half-frame construct.AFTERTREATMENT: Postoperative management is similar to that described for intramedullary fixation of the clavicle, with the critical addition of routine, meticulous pin site care to prevent superficial tract infections.

Proximal Humeral Fractures
"Use adequate radiograms to understand the traumatic lesion, be careful denying older patients effective treatment, use a safe and simple surgical approach, know the options for internal fi xation, recognize the value of prosthetic replacement, avoid technical pitfalls, and thoughtfully supervise the postoperative patient care." — R.H. Cofi eld (1988)
Cofield’s seminal summary encapsulates the profound difficulty of treating proximal humeral fractures—from initial evaluation to final rehabilitation. Despite decades of advancement, controversy and confusion persist, and no single treatment protocol or algorithm has proven universally effective. Areas of ongoing debate include the reliability of radiographic diagnosis, the threshold for operative versus nonoperative treatment, the influence of patient age and bone density, the choice of surgical approach (deltopectoral vs. anterolateral), and the selection between fracture fixation (ORIF/pinning) and arthroplasty (hemiarthroplasty or reverse total shoulder arthroplasty).
Literature reflects this dichotomy. Zyto et al. suggested that nonoperative treatment may be preferable for displaced three-part proximal humeral fractures in elderly patients, yet pain and significant loss of function are frequently reported. Conversely, Court-Brown et al. reported good or excellent results in 81% of impacted valgus fractures in elderly patients treated nonoperatively. In a study of geographical incidence and treatment variation, Sporer et al. found massive discrepancies in the percentage of proximal humeral fractures treated operatively, ranging from 6.4% to 60% across different regions. The sheer variety of fixation techniques available for a single fracture type underscores the complexity of these injuries.
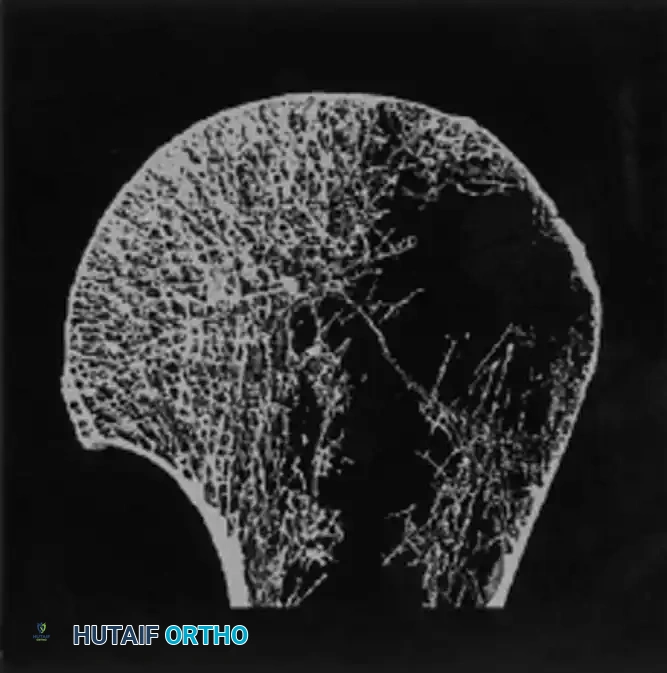
Anatomy and Vascularity
Understanding the blood supply to the proximal humerus is paramount, particularly when assessing the risk of avascular necrosis (AVN). The primary arterial supply is derived from the anterior and posterior humeral circumflex arteries. The anterolateral branch of the anterior humeral circumflex artery (the arcuate artery) is the major intraosseous supply to the humeral head. Disruption of the medial hinge (calcar) and severe displacement of the anatomic neck drastically increase the risk of ischemia.
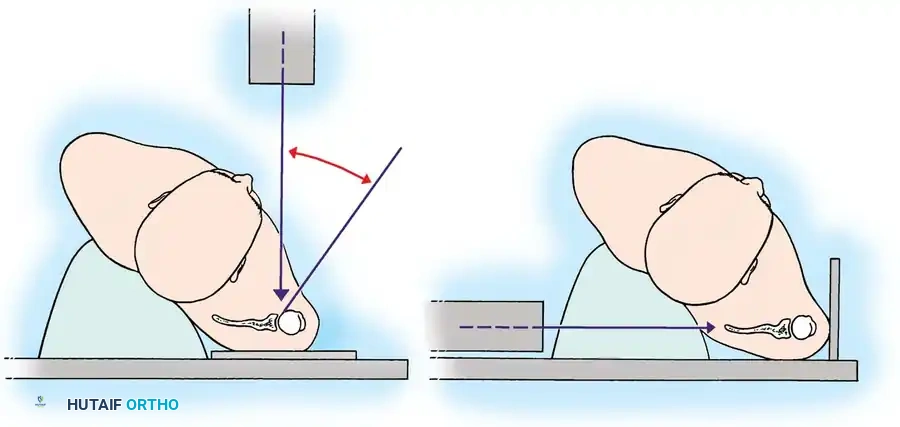
Fig. 54-9 Blood supply of proximal humerus. Note the critical contributions of the anterior and posterior humeral circumflex arteries and the arcuate artery.

Neer Classification System
The most universally recognized classification system for proximal humeral fractures is that of Neer. Although critics cite limited inter-observer reliability and intra-observer reproducibility, it remains the conceptual foundation for guiding treatment.
The classification is based on the four-part anatomy of the proximal humerus:
1. The Humeral Head (Articular segment)
2. The Lesser Tuberosity
3. The Greater Tuberosity
4. The Proximal Humeral Shaft
The Neer Criterion for Displacement: A segment is considered a "separate part" only if it is displaced by greater than 1 cm or angulated by more than 45 degrees.
Displaced three-part and four-part fractures markedly alter the articular congruity of the glenohumeral joint and have the highest likelihood of disrupting the major blood supply. Osteonecrosis is most likely after displaced four-part fractures and anatomic neck fractures.
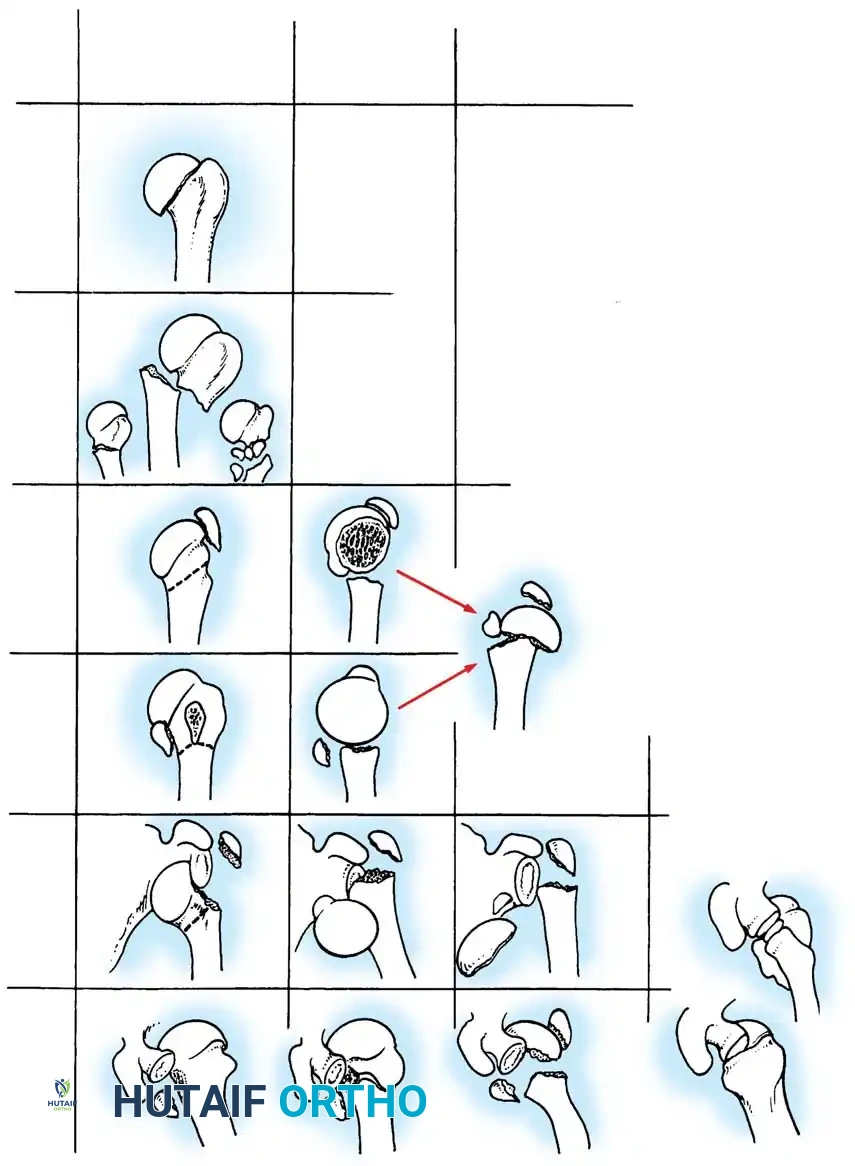
Fig. 54-8 Neer’s terminology of four-segment classifi cation of displaced fractures and fracture-dislocations relates pattern of displacement (two-part, three-part, or four-part) and key segment displaced.
Radiographic Evaluation
A standard shoulder trauma series is mandatory for all patients suspected of a proximal humeral fracture. This series must include:
1. Anteroposterior (AP) View in the Plane of the Scapula (Grashey View): Prevents overlap of the humeral head and glenoid.
2. Lateral View of the Scapula (Y View): Assesses anterior or posterior dislocation and scapular body integrity.
3. Supine Axillary View: The most critical view for evaluating the glenohumeral joint articulation, tuberosity displacement, and articular head-splitting components.
Fig. 54-10 A and B, Special radiographic view perpendicular to plane of scapula to show glenohumeral joint in profi le (A) and parallel to plane of scapula to show anterior and posterior displacement (B).
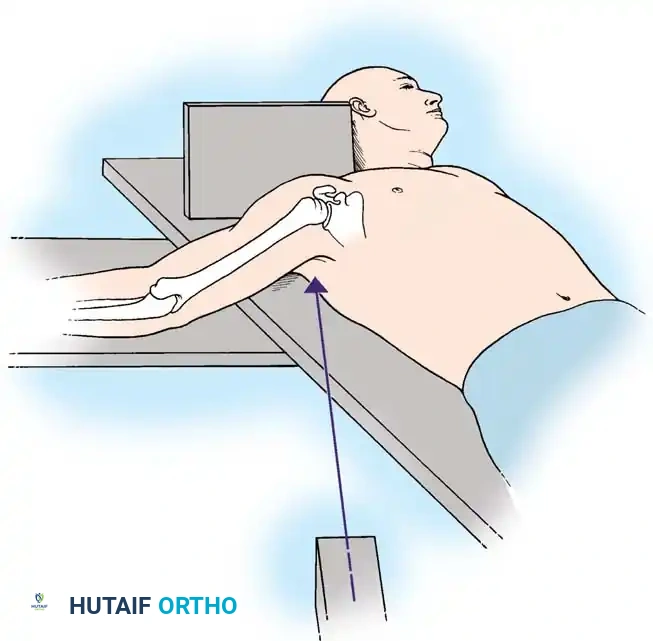
Fig. 54-11 Method of obtaining axillary view of glenohumeral joint. Minimal abduction of injured arm is required to determine anteroposterior relationships.
If the amount of displacement of the humeral head or tuberosity fragments remains unclear on plain radiographs, an axial CT scan with 2-mm sections and 3D reconstructions is strictly indicated. CT is invaluable for preoperative planning, particularly for assessing head-splitting fractures, tuberosity comminution, and glenoid rim involvement.

Fig. 54-12 CT scan of humeral head–splitting fracture.
Nonoperative Treatment
Nonoperative treatment can yield a highly functional, painless extremity in the majority of minimally displaced proximal humeral fractures. The glenohumeral joint's immense range of motion can accommodate moderate angular deformity without significant functional loss.
Neer described acceptable angulation as less than 45 degrees and less than 1 cm of displacement. While not absolute, these criteria provide a reliable heuristic.
* Patient Selection: An elderly, infirm patient can tolerate functional loss better than a young, high-demand laborer.
* Stability Assessment: The critical step is determining if the humeral head and shaft move as a unit. If the fracture is stable and in an acceptable position, a sling is utilized for comfort.
* Rehabilitation: A physical therapy regimen emphasizing passive pendulum exercises is initiated early, usually within 7 to 10 days, to prevent adhesive capsulitis. If the head and shaft do not move as a unit, therapy may be delayed for 2 to 4 weeks. Prolonged immobilization correlates directly with prolonged therapy and greater permanent disability.

Operative Treatment
The decision to proceed with operative treatment is nuanced. Fracture displacement is the primary indicator of instability. The surgical goal is the anatomic restoration of the proximal humerus with stable fixation that permits early functional range of motion. Chronic malunions and nonunions treated surgically at a later stage are notoriously associated with poor outcomes; thus, primary recreation of normal anatomy (tuberosity reduction and head-neck angle) is imperative.
Indications for Operative Treatment:
* Displaced two-part surgical neck fractures.
* Displaced (>5 mm) greater tuberosity fractures (due to subacromial impingement risk).
* Displaced three-part fractures.
* Displaced four-part fractures (especially in young, active patients).
The modality of fixation—transosseous suture fixation, percutaneous pinning, intramedullary nailing, or locked plate fixation—depends heavily on patient age, bone mineral density, fracture morphology, and surgeon expertise.
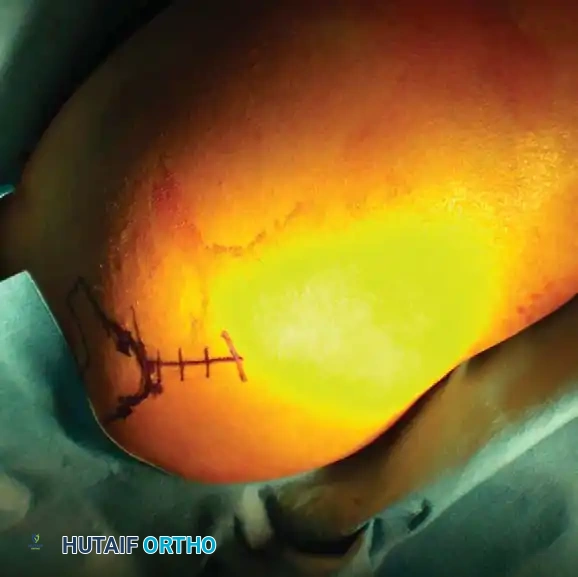
Transosseous Suture Fixation
Transosseous suture fixation techniques are well-defined and highly effective, particularly in osteoporotic bone where metal hardware may cut out. Park et al. reported 78% excellent results in patients with two-part and three-part fractures treated with this method.
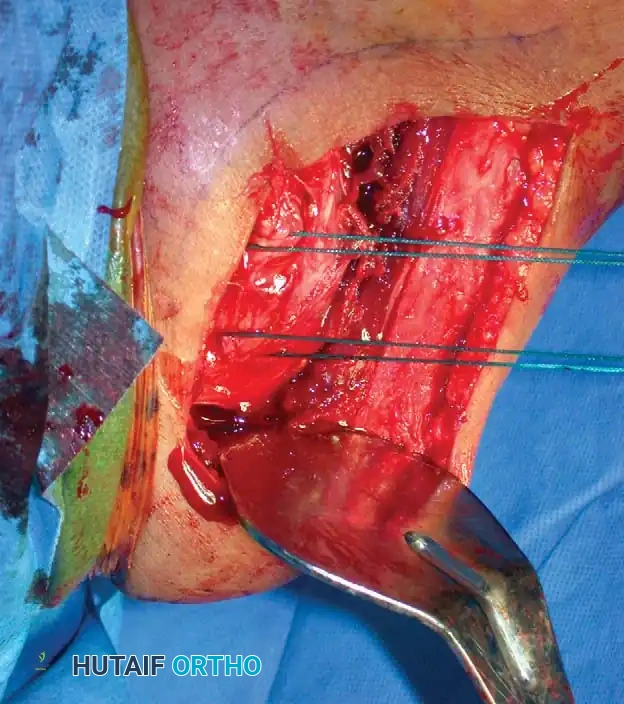
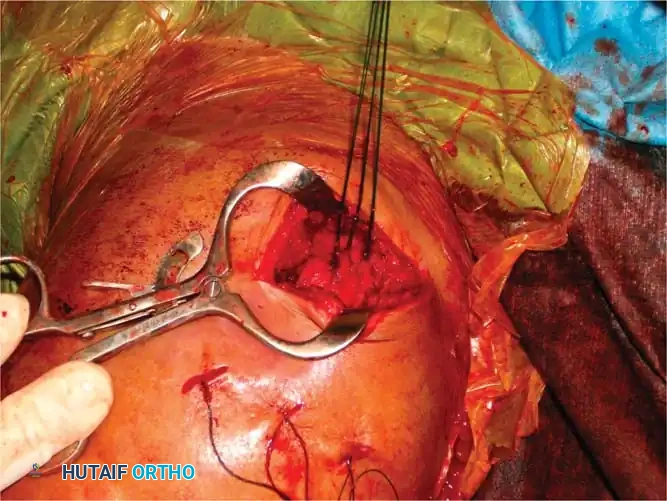
Clinical Pearl: The use of heavy, nonabsorbable sutures allows the surgeon to incorporate the robust rotator cuff insertions (supraspinatus/infraspinatus for the greater tuberosity; subscapularis for the lesser tuberosity) to neutralize deforming muscle forces and secure the tuberosity fragments.
This technique requires minimal soft-tissue stripping, preserving the delicate vascular envelope and resulting in relatively low rates of osteonecrosis. However, the construct is inherently less rigid than locked plating, requiring careful patient compliance during early rehabilitation to prevent loss of reduction.
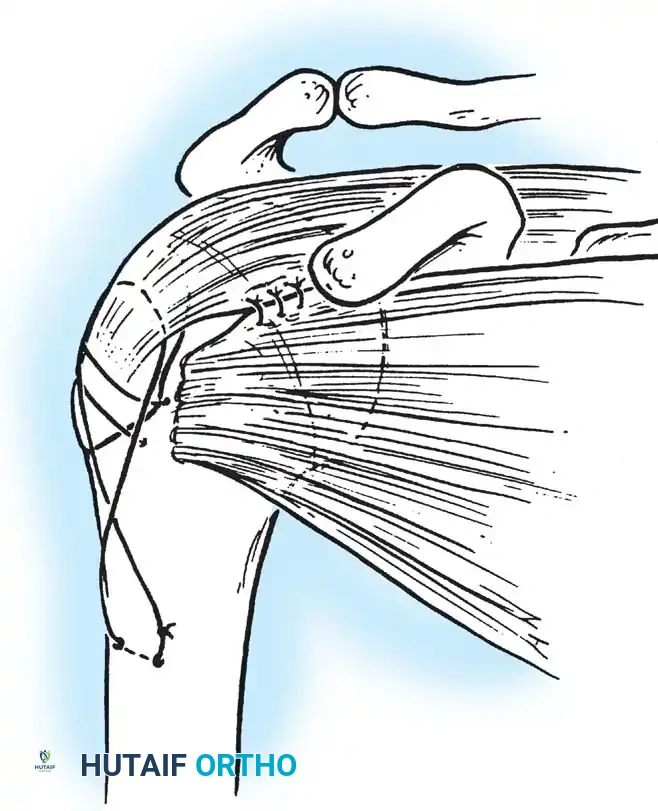
Fig. 54-13 Transosseous nonabsorbable sutures incorporate rotator cuff to increase fi xation and help control tuberosity fragments.

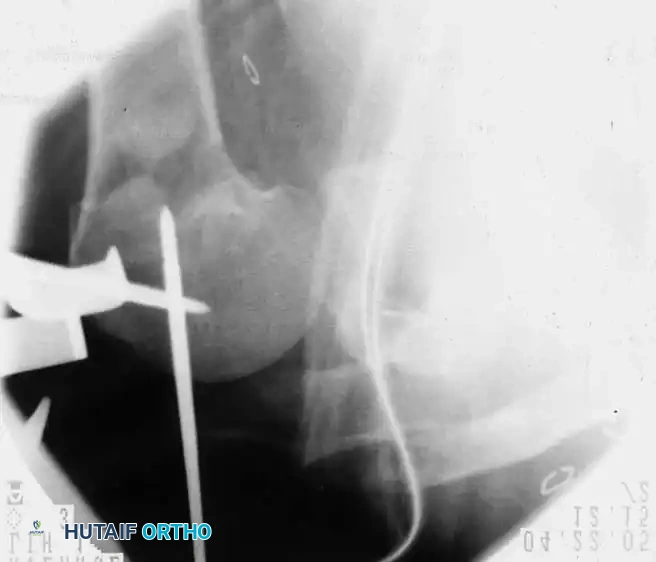
Percutaneous Pinning
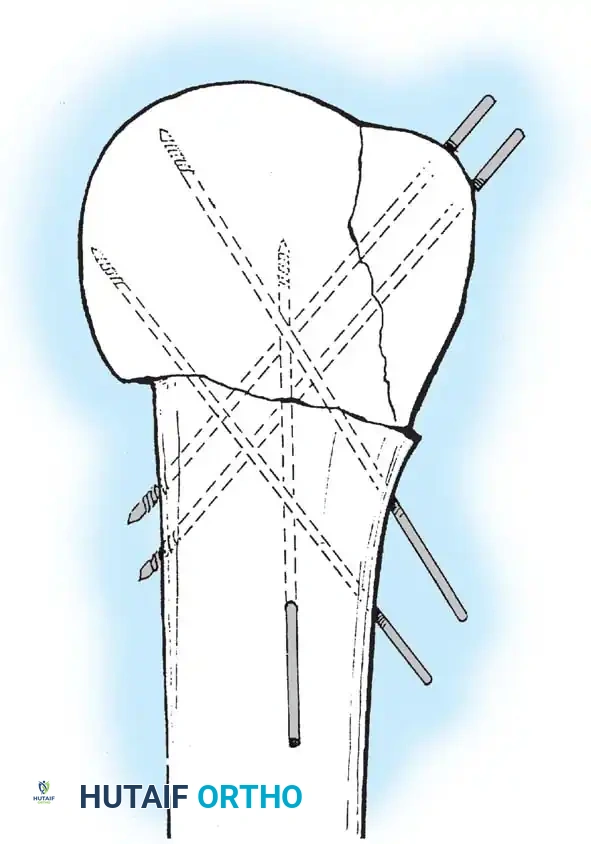
Percutaneous pinning offers the distinct advantage of avoiding extensive soft-tissue dissection, thereby maximally preserving the blood supply to the humeral head. It is a minimally invasive, cost-effective technique. Jaberg et al. and Resch et al. have reported excellent outcomes using threaded pins or Kirschner wires.
Technique Overview:
* Closed reduction is achieved under fluoroscopy using traction, abduction, and manipulation.
* Pins are introduced percutaneously from the lateral humeral cortex, directed superomedially into the humeral head.
* Additional pins may be placed anteriorly to secure the lesser tuberosity or superiorly for the greater tuberosity.
* Warning: The axillary nerve is at risk during lateral pin insertion. Pins must be placed carefully, often utilizing a small stab incision and blunt dissection to the bone.
Open Reduction and Internal Fixation (Locked Plating)
For complex three- and four-part fractures, particularly in patients with osteoporotic bone, proximal humeral locking plates have revolutionized treatment. These fixed-angle constructs provide superior biomechanical stability compared to conventional non-locking plates.
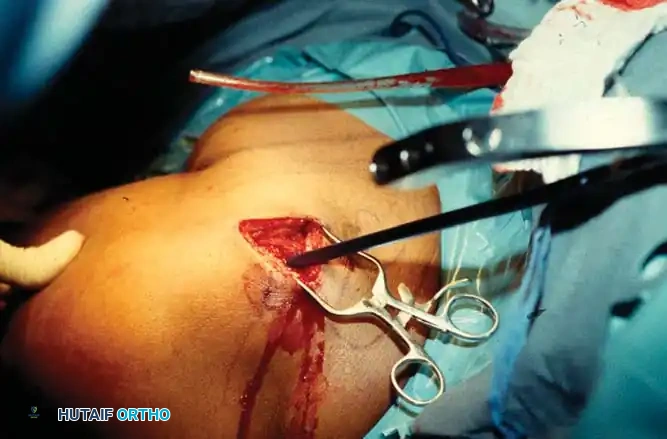
Surgical Approach:
* The deltopectoral approach is the workhorse for proximal humeral ORIF, utilizing the internervous plane between the deltoid (axillary nerve) and pectoralis major (medial/lateral pectoral nerves).
* The cephalic vein is identified and typically retracted laterally with the deltoid to protect its tributaries.
Fixation Principles:
* Anatomic reduction of the medial calcar hinge is critical to prevent varus collapse.
* Heavy nonabsorbable sutures are passed through the rotator cuff tendons and tied to the plate to neutralize tuberosity pull.
* Locking screws are placed into the humeral head, ensuring they do not penetrate the articular surface (subchondral placement is ideal).

Postoperative Rehabilitation
Regardless of the fixation method, the success of proximal humeral fracture management hinges on a meticulously supervised rehabilitation protocol.
* Phase I (0-4 weeks): Sling immobilization. Passive range of motion (PROM) including pendulum exercises and gentle passive forward elevation/external rotation, strictly within the safe zone determined intraoperatively.
* Phase II (4-8 weeks): Transition to active-assisted range of motion (AAROM) as radiographic evidence of early callus formation appears.
* Phase III (8-12 weeks): Active range of motion (AROM) and initiation of isometric strengthening.
* Phase IV (>12 weeks): Progressive resistance exercises and return to functional activities.



By adhering to strict biomechanical principles, respecting the delicate vascular anatomy, and tailoring the surgical approach to the individual patient's fracture morphology and physiologic demand, the orthopaedic surgeon can navigate the profound complexities of shoulder girdle trauma to achieve optimal clinical outcomes.
