Comprehensive Introduction and Patho-Epidemiology
The posterolateral corner (PLC) of the knee represents one of the most enigmatic and functionally critical regions in orthopedic sports medicine. Historically underappreciated and frequently misdiagnosed, the PLC is an area of profound anatomical complexity. When injured, it has the potential to cause significant, often debilitating, disability for our patients. The evolution of our understanding of this region—from viewing it as a homogenous "dark side of the knee" to recognizing its discrete, highly specialized layered anatomy—has revolutionized our approach to posterolateral instability.
Definition and Clinical Significance
The PLC is a complex nexus of static and dynamic stabilizers that collectively resist varus angulation, external tibial rotation, and posterior tibial translation. While isolated injuries to the PLC structures are relatively uncommon, accounting for approximately 2% of all acute ligamentous knee injuries, their clinical significance cannot be overstated. The structures of the PLC act in concert with the central pivot (the anterior and posterior cruciate ligaments) to maintain normal knee kinematics. Disruption of this harmonious relationship leads to profound alterations in joint contact forces and kinematics.
Failure to recognize and adequately treat PLC injuries is a well-documented cause of catastrophic failure in cruciate ligament reconstructions. The continuous abnormal varus and external rotation forces placed on an isolated anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL) graft in the setting of an untreated PLC deficiency will inevitably lead to graft elongation, fatigue, and eventual rupture. Therefore, a comprehensive understanding of the PLC is not merely an academic exercise, but a mandatory prerequisite for any surgeon undertaking complex knee reconstruction.
Pathogenesis and Injury Mechanisms
Understanding the precise mechanisms by which these injuries occur allows the orthopedic surgeon to anticipate the specific pattern of structural damage. PLC injuries most commonly result from high-energy trauma, such as motor vehicle accidents, or complex sports-related injuries. Approximately 40% of these injuries occur during athletic participation, particularly in contact sports like American football, rugby, and soccer.

The classic mechanism for an isolated PLC injury is a hyperextension force combined with a varus moment. This frequently occurs when a player receives a direct, blunt trauma to the anteromedial aspect of the proximal tibia while the foot is planted and the knee is in extension. Alternatively, a severe non-contact hyperextension injury alone can sequentially disrupt the posterior capsule and the posterolateral structures. When a severe external rotation torque is applied to the tibia, particularly in varying degrees of knee flexion, the popliteus complex and the lateral collateral ligament are subjected to massive tensile loads, often resulting in midsubstance tears or avulsions from their femoral or fibular attachments.
The Challenge of Combined Ligamentous Injuries
A critical operative pearl that must be ingrained in every knee surgeon's mind is the exceptionally high incidence of combined ligament injuries associated with PLC pathology. Literature suggests that up to 72% of PLC injuries occur in conjunction with ruptures of the ACL, PCL, or both (a true knee dislocation). When you encounter a clinically significant PLC injury, you must maintain an incredibly high index of suspicion for concomitant central pivot damage.

The diagnostic challenge lies in the fact that the dramatic presentation of a cruciate rupture can often mask the more subtle signs of posterolateral instability. Conversely, the surgeon must meticulously evaluate the entire knee to ensure all components of instability are addressed simultaneously. Staged reconstructions in the setting of multiligamentous knee injuries involving the PLC are generally discouraged, as the untreated compartment will place immediate and deleterious stress on the newly reconstructed grafts.
Long-Term Implications of Untreated Pathology
Chronic instability stemming from an untreated or inadequately treated PLC injury is truly debilitating. Patients typically present with a characteristic varus-thrust gait—a dynamic, visually striking lateral bowing of the knee during the stance phase of walking. This is often accompanied by a persistent sensation of instability, particularly during the toe-off phase when the knee extends and the lateral compartment is subjected to maximal loads.
This instability is exacerbated by the inherent convexity of the lateral tibial plateau articulating with the convex lateral femoral condyle, lacking the intrinsic bony stability seen in the medial compartment. Over time, this chronic insufficiency progresses predictably to tricompartmental degenerative joint disease. Biomechanical studies have definitively shown massive increases in patellofemoral and medial compartment contact pressures with combined PLC and PCL sectioning. Our primary surgical objective is to halt this degenerative cascade through meticulous, anatomically precise surgical reconstruction.
Detailed Surgical Anatomy and Biomechanics
Before making a single incision, the orthopedic surgeon must possess a three-dimensional, deep understanding of the intricate anatomy of the PLC. This region is a highly organized, layered structure. Navigating it with precision is paramount not only to effectively address the pathology but, more importantly, to protect the vital neurovascular elements that traverse this space.
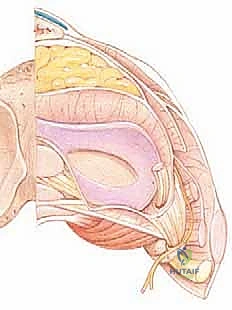
The Layered Architecture of the Posterolateral Corner
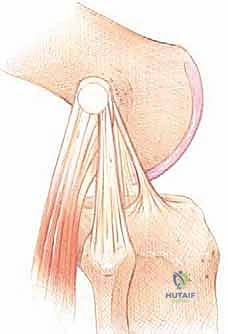
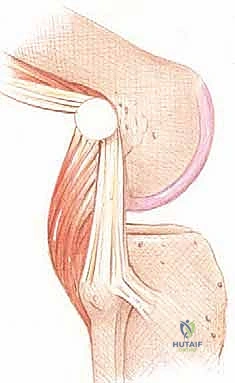
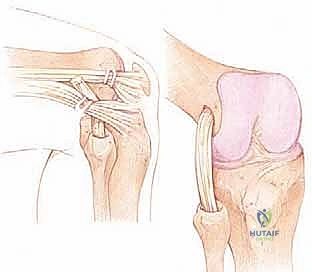
Seebacher and colleagues elegantly organized the posterolateral structures into three distinct layers, a classification system that remains the bedrock of our surgical approach today. Layer I, the superficial layer, is defined anteriorly by the iliotibial (IT) tract and posteriorly by the biceps femoris muscle and its tendon. The IT band is a robust structure inserting on Gerdy's tubercle. It is unique biomechanically; it becomes taut posteriorly in knee flexion, exerting an external rotation force, but relaxes and moves anteriorly in extension. Due to its relaxed state in extension, it is rarely injured in acute PLC trauma, making it a highly reliable surgical landmark.
Layer II, the middle layer, comprises the quadriceps retinaculum anteriorly, and the patellofemoral and patellomeniscal ligaments posteriorly. These structures contribute accessory static stability to the patellofemoral joint and the anterior aspect of the PLC. Layer III, the deep layer, is arguably the most critical in terms of static stability. It directly reinforces the joint capsule and contains the primary stabilizers we aim to reconstruct: the lateral collateral ligament (LCL), the popliteus tendon, the popliteofibular ligament (PFL), and the arcuate ligament complex.
Key Static Stabilizers
The primary static stabilizers of the deep layer demand meticulous attention. The Lateral Collateral Ligament (LCL) is a primary, cord-like structure originating from the lateral epicondyle of the femur, precisely 1.4 mm proximal and 3.1 mm posterior to the lateral epicondyle prominence. It inserts onto the lateral aspect of the fibular head, typically 8.2 mm posterior to the anterior margin of the fibular head. The LCL is the primary static restraint to varus stress, particularly between 0 and 30 degrees of knee flexion.

The Popliteus complex is equally vital. The popliteus muscle originates from the posterior tibia, courses intra-articularly through the hiatus of the coronary ligament, and inserts onto the lateral femoral condyle, consistently 18.5 mm anterior and distal to the LCL origin. The popliteofibular ligament (PFL) is a critical static attachment that runs from the posterior aspect of the fibular styloid to the popliteus tendon. Together, the popliteus tendon and PFL act as the primary restraint to external tibial rotation. The Arcuate Ligament Complex acts as a dynamic and static "sling" providing restraint to posterolateral rotation, often avulsing from the fibular styloid in high-energy trauma (the classic "arcuate sign" on radiographs).
Dynamic Stabilizers and Secondary Restraints
While our surgical reconstructions focus on the static stabilizers, the dynamic stabilizers play a massive role in overall knee kinematics. The Biceps Femoris is a powerful muscle that inserts primarily on the fibular head but possesses complex fascial attachments to the IT band, Gerdy's tubercle, the LCL, and the posterolateral capsule. Its contraction dynamically stabilizes the PLC, particularly against external rotation and anterior translation of the femur on the tibia.
The Iliotibial (IT) Tract, while primarily a superficial structure, contributes to overall knee stability through its dynamic tension and capsular attachments. Furthermore, the Lateral Head of the Gastrocnemius, originating on the lateral femoral condyle (often associated with a sesamoid fabella), contributes dynamic support to the posterior capsule. During rehabilitation, optimizing the function of these dynamic stabilizers is crucial to protect the healing reconstructed static ligaments.
Critical Neurovascular Structures: The Common Peroneal Nerve
The common peroneal nerve is the single most critical neurovascular structure in the posterolateral operative field. It courses superficially from the posterior thigh, winding intimately around the fibular neck, deep to the long head of the biceps femoris tendon and superficial to the lateral head of the gastrocnemius. Injury to this nerve—whether through direct transection, traction, or ischemic compression—can lead to a devastating foot drop and profound sensory loss over the dorsum of the foot.
Identification, neurolysis, and meticulous protection of the common peroneal nerve are paramount during the very first steps of the posterolateral dissection. In the setting of chronic injuries, increased scar tissue formation distorts normal tissue planes, making nerve identification exponentially more challenging and demanding extreme caution. The surgeon must routinely dissect the nerve free from its fascial encasements to allow it to safely retract during fibular tunnel preparation.
Comprehensive Clinical Assessment and Diagnostic Imaging
A thorough, systematic history and physical examination form the cornerstone of diagnosing PLC injuries. Because these injuries rarely occur in isolation, a comprehensive assessment evaluating every single ligamentous structure of the knee is an absolute requirement.
History and Physical Examination
Patients with acute PLC injuries typically report a distinct "pop" followed by localized pain and swelling in the posterolateral aspect of the knee. A rapid, massive hemarthrosis strongly suggests concomitant intra-articular pathology, such as a cruciate ligament tear. However, it is vital to note that if the posterolateral capsule is extensively torn, the intra-articular fluid may extravasate into the soft tissues of the calf, resulting in a deceptively diminished knee effusion but significant calf swelling and ecchymosis.
During the physical examination, observation of the patient's gait (if they are able to bear weight) is critical. A varus thrust gait is the hallmark of chronic PLC deficiency. Palpation should systematically assess the LCL, fibular head, and lateral joint line. Range of motion must be carefully documented; a mechanical block to extension may indicate an incarcerated meniscus or an osteochondral fragment. Always assess for the "external rotation recurvatum" sign: lifting both legs by the great toes will reveal asymmetric hyperextension, varus, and external rotation of the tibia on the injured side.
Specific Instability Testing
Specific stress testing is required to isolate the damaged structures. The Varus Stress Test is performed at both 0 and 30 degrees of knee flexion. At 30 degrees, the cruciate ligaments are relaxed, and the LCL is isolated. Increased laxity without a firm endpoint indicates an LCL tear. If varus laxity is present at 0 degrees of extension, this indicates a massive injury involving not only the LCL and PLC but also the posterior capsule and likely the cruciate ligaments.
The Dial Test is the gold standard for diagnosing posterolateral rotatory instability. With the patient supine or prone, the knee is flexed to 30 degrees and then 90 degrees, and an external rotation force is applied to the feet. A side-to-side difference of greater than 10-15 degrees is considered positive. Crucially, increased rotation at 30 degrees that reduces at 90 degrees suggests an isolated PLC injury. If the increased external rotation persists or worsens at 90 degrees, it strongly indicates a combined PLC and PCL injury. The Reverse Pivot-Shift test can also be utilized, where a palpable clunk is felt as the posteriorly subluxated lateral tibial plateau reduces as the knee is brought from flexion into extension.
Advanced Diagnostic Imaging
While the physical examination dictates the diagnosis, advanced imaging is essential for surgical planning. Standard radiographs (AP, lateral, skyline, and Rosenberg views) should be scrutinized for avulsion fractures. The "arcuate sign"—a small fleck of bone avulsed from the fibular styloid—is pathognomonic for a PLC injury. Segond fractures (lateral capsular avulsions) correlate highly with ACL injuries but also indicate lateral compartment trauma.
Magnetic Resonance Imaging (MRI) is the imaging modality of choice. High-resolution MRI, particularly utilizing coronal oblique sequences oriented parallel to the popliteus tendon, allows for detailed visualization of the LCL, popliteus, and PFL. The radiologist and surgeon must look for edema, discontinuity, or avulsion of these structures. Bone bruising patterns, typically involving the anteromedial femoral condyle and anteromedial tibia (contrecoup injury from hyperextension/varus), further corroborate the injury mechanism.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a PLC injury requires a nuanced understanding of the injury grade, chronicity, concomitant injuries, and the patient's functional demands. Non-operative management is generally reserved for isolated, low-grade injuries, which are exceedingly rare.
Surgical Decision Making
The consensus in modern orthopedic sports medicine is that high-grade (Grade III) PLC injuries, characterized by complete disruption of the ligamentous complex with gross instability, require surgical intervention. Historically, primary repair was attempted; however, literature has definitively shown that primary repair of mid-substance tears yields unacceptably high failure rates due to the poor tissue quality and high biomechanical stresses in this region. Therefore, anatomic reconstruction using robust grafts is the gold standard for both acute and chronic Grade III injuries.
Timing is also a critical factor. Acute reconstructions (performed within 2 to 3 weeks of injury) are generally preferred before massive scar tissue formation distorts the anatomy and the tissue planes become obliterated. In the chronic setting, the surgeon must carefully evaluate limb alignment. Chronic PLC deficiency often leads to progressive varus deformity. If a patient has a mechanical axis that falls medial to the medial tibial spine, an isolated soft-tissue reconstruction will inevitably stretch out and fail.
Absolute and Relative Indications
Absolute indications for PLC reconstruction include acute Grade III isolated PLC injuries, any PLC injury in the setting of a multiligamentous knee injury (e.g., combined ACL/PLC or PCL/PLC), and chronic symptomatic posterolateral instability causing a varus thrust gait or giving way during activities of daily living.
| Indication Category | Specific Clinical Scenarios |
|---|---|
| Absolute Indications | Acute Grade III isolated PLC tear; Combined ACL/PLC or PCL/PLC ruptures; Chronic symptomatic instability with varus thrust; Knee dislocations (KD-III or KD-IV). |
| Relative Indications | Grade II injuries in high-demand elite athletes; Symptomatic partial tears failing conservative management of >3-6 months. |
| Absolute Contraindications | Active joint infection; Severe, uncorrected genu varum (requires staged HTO first); Advanced tricompartmental osteoarthritis; Medically unstable patient. |
| Relative Contraindications | Poor soft tissue envelope; Patient non-compliance with complex postoperative rehabilitation; Grade I/II isolated sprains. |
Contraindications to Reconstruction
Contraindications must be strictly respected to avoid catastrophic outcomes. The most critical biomechanical contraindication is severe, uncorrected varus malalignment. In a patient with chronic PLC deficiency and a varus mechanical axis, a High Tibial Osteotomy (HTO) must be performed either as a staged procedure (prior to ligament reconstruction) or concomitantly to offload the lateral compartment. Attempting a soft-tissue reconstruction in a profoundly varus knee is a guaranteed recipe for graft failure.
Other absolute contraindications include active local or systemic infection, severe tricompartmental osteoarthritis where an arthroplasty would be more appropriate, and a compromised soft-tissue envelope that cannot support a surgical incision. Relative contraindications include profound patient non-compliance, as the postoperative rehabilitation protocol is rigorous, prolonged, and absolutely critical to the success of the procedure.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the hallmark of a master surgeon. Reconstructing the PLC is technically demanding, requiring precise tunnel placement to restore normal kinematics. Any deviation from anatomic isometric points will result in either restricted range of motion or recurrent laxity.
Graft Selection and Preparation
Graft selection is a critical early step. For an anatomic PLC reconstruction, a robust, long graft is required. The split Achilles tendon allograft is highly favored by many complex knee surgeons due to its excellent tensile strength and the presence of a bone block, which can be fixed securely in the femoral tunnels. Alternatively, a large, doubled semitendinosus allograft or autograft can be utilized.

When using soft tissue grafts, the graft must be meticulously prepared on the back table. For the LaPrade anatomic technique, a graft length of at least 24 cm is required. The ends are tubularized with heavy, non-absorbable whipstitches (e.g., #2 FiberWire or equivalent) to allow for secure passage and tensioning. If a bone block is used, it must be sized to precisely fit the femoral tunnel, typically 8 or 9 mm in diameter.
Pre-Operative Templating and Fluoroscopy
Preoperative templating using true lateral radiographs is highly recommended to identify the anatomic insertions of the LCL and popliteus on the lateral femoral condyle. The LCL origin is slightly proximal and posterior to the lateral epicondyle, while the popliteus origin is anterior and distal, situated in the anterior aspect of the popliteal sulcus.
Intraoperative fluoroscopy is an invaluable adjunct, particularly for surgeons early in their learning curve or in revision scenarios where bony landmarks are distorted. A true lateral fluoroscopic view ensures that the femoral tunnels are placed anatomically and do not intersect with each other or with previously placed cruciate ligament tunnels. The fibular tunnel trajectory must also be planned to avoid breaching the lateral cortex or the proximal tibiofibular joint.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia, often supplemented with a regional nerve block (such as a saphenous or adductor canal block) for postoperative pain control. A sciatic block is generally avoided as it masks the ability to assess common peroneal nerve function immediately postoperatively.

The patient is positioned supine on the operating table. A lateral post or a specialized leg holder is utilized to allow the knee to be manipulated freely through a full range of motion. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the posterolateral aspect of the knee into better view. A sterile tourniquet is applied high on the thigh. The entire limb is prepped and draped to allow access from the iliac crest (if autograft bone is needed) down to the toes, ensuring the foot is visible to monitor for any inadvertent peroneal nerve stimulation during dissection.
Step-by-Step Surgical Approach and Fixation Technique
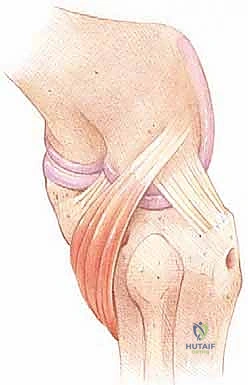
The anatomic reconstruction of the PLC, popularized by LaPrade and colleagues, aims to reconstruct the three primary static stabilizers: the LCL, the popliteus tendon, and the popliteofibular ligament. This requires a highly systematic, step-by-step approach.
Incision and Superficial Dissection
A broad, lateral hockey-stick incision is utilized. It begins laterally along the IT band, approximately 4-5 cm proximal to the lateral epicondyle, extends distally across the joint line, and curves gently anteriorly to end between Gerdy's tubercle and the fibular head.
The subcutaneous tissues are divided to expose the superficial fascia. The first critical window is developed posterior to the long head of the biceps femoris. The common peroneal nerve must be identified immediately. Using blunt dissection and a nerve hook, the nerve is traced from proximal to distal as it crosses the fibular neck. A vessel loop is placed around the nerve to allow for gentle, atraumatic retraction throughout the procedure. Meticulous hemostasis in this area is vital to prevent postoperative hematoma and subsequent nerve compression.
Deep Dissection and Identification of Bony Landmarks
Once the nerve is secured, the deep dissection begins. A longitudinal incision is made through the IT band in line with its fibers to expose the lateral femoral epicondyle. The anatomic footprints of the LCL and the popliteus tendon must be precisely identified. The LCL origin is located on a small bony prominence proximal and posterior to the epicondyle. The popliteus origin is found by palpating the popliteal sulcus; the footprint is at the anterior, proximal aspect of this groove.

Distally, the fibular head is exposed. The biceps bursa is incised to reveal the LCL insertion on the lateral aspect of the fibular head. The posterior aspect of the fibular styloid is exposed to identify the insertion site of the popliteofibular ligament. Finally, a small window is made through the anterior tibialis fascia to expose the flat spot on the posterolateral tibia, which serves as the anatomic exit point for the popliteus bypass graft.
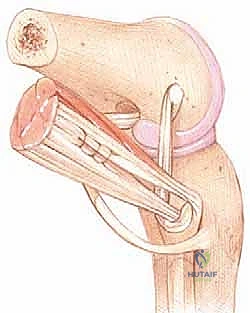
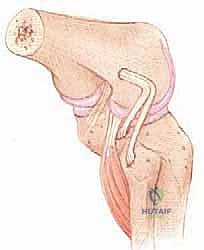
Tunnel Preparation and Graft Passage
Tunnel preparation must be exact. Two femoral tunnels are drilled at the anatomic footprints of the LCL and popliteus, typically 8 or 9 mm in diameter and 25 mm deep. A fibular tunnel (typically 7 mm) is drilled from the LCL insertion site on the lateral fibular head, aiming distally and posteriorly to exit at the PFL insertion site on the posteromedial fibular styloid. Extreme care is taken to protect the peroneal nerve during this step with a retractor. A tibial tunnel (typically 9 mm) is drilled from anterior to posterior, exiting at the popliteus musculotendinous junction on the posterolateral tibia.
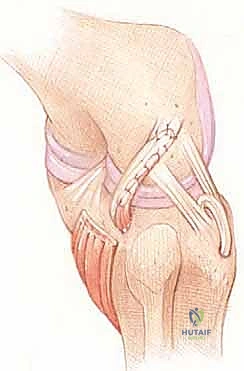
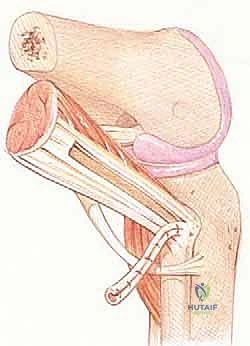
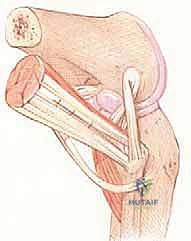
Graft passage follows a specific sequence. The graft is first secured in the femoral tunnels. The LCL limb of the graft is passed distally, deep to the IT band, and threaded through the fibular tunnel from anterior to posterior. This limb then becomes the PFL graft and is routed medially to join the popliteus limb. Both limbs are then passed from posterior to anterior through the tibial tunnel. This complex routing anatomically recreates the dynamic sling of the posterolateral corner.
Fixation Sequence and Tensioning
The sequence of graft fixation is arguably the most critical step to ensure appropriate joint kinematics. The grafts are first rigidly fixed in the femoral tunnels using bioabsorbable or biocomposite interference screws.
Next, the LCL limb is tensioned. The knee is placed in 20 to 30 degrees of flexion, and a valgus force is applied to close the lateral joint space. The foot is maintained in neutral rotation. While holding this tension, an interference screw is placed in the fibular tunnel to secure the LCL. Finally, the popliteus and PFL limbs are tensioned. The knee is maintained at 60 degrees of flexion, and a slight internal rotation force is applied to the tibia to reduce the posterolateral subluxation. The grafts are then fixed in the anterior tibial tunnel
