Introduction to Malignant Soft-Tissue Tumors
The operative management of malignant soft-tissue tumors (soft-tissue sarcomas) represents one of the most complex challenges in orthopedic oncology. These heterogeneous neoplasms arise from mesenchymal cell lines and require a rigorous, multidisciplinary approach to optimize both oncological outcomes and limb salvage. Historically, amputation was the standard of care; however, advancements in multimodal therapy—combining wide surgical resection with neoadjuvant or adjuvant radiotherapy and chemotherapy—have made limb-sparing surgery possible in over 90% of cases.
This comprehensive guide delineates the pathological characteristics, advanced imaging protocols, biomechanical considerations, and step-by-step surgical techniques required for the management of specific soft-tissue sarcoma subtypes.
Clinical Pearl: The initial biopsy is the most critical step in sarcoma management. Poorly planned biopsies can contaminate neurovascular bundles or distinct anatomical compartments, converting a resectable tumor into one requiring amputation. Always utilize longitudinal incisions and ensure the biopsy tract can be excised en bloc with the definitive specimen.
General Surgical Principles and Approaches
Preoperative Planning and Imaging
Accurate staging is paramount. The standard imaging protocol includes plain radiographs to assess for osseous involvement or intralesional calcifications, and contrast-enhanced Magnetic Resonance Imaging (MRI) of the entire anatomical compartment. MRI is the gold standard for delineating the tumor's relationship to major neurovascular structures and fascial planes. Staging for distant metastasis typically requires a high-resolution Computed Tomography (CT) scan of the chest, as the lungs are the most common site of dissemination for most sarcomas.
Surgical Margins
The goal of surgical intervention is a wide resection, defined as the removal of the tumor with a continuous cuff of normal, healthy tissue in all dimensions.
* Intralesional: Macroscopic tumor left behind (unacceptable for curative intent).
* Marginal: Dissection through the pseudocapsule (high risk of local recurrence).
* Wide: Dissection through normal tissue outside the reactive zone.
* Radical: Removal of the entire anatomical compartment.
Step-by-Step Surgical Approach for Wide Resection
- Positioning and Tourniquet: Position the patient to allow access to the entire compartment. A tourniquet may be applied but should not be exsanguinated with an Esmarch bandage to prevent proximal tumor embolization; elevate the limb for gravity exsanguination instead.
- Incision: Incorporate the previous biopsy tract with an elliptical incision, maintaining a minimum 2-3 cm margin of normal skin.
- Exposure and Dissection: Develop flaps within normal tissue planes. Identify and protect major neurovascular bundles early in the dissection, tracing them from normal proximal anatomy into the zone of resection.
- Resection: Excise the tumor en bloc with its surrounding cuff of normal muscle and fascia. Do not violate the tumor pseudocapsule.
- Tumor Bed Marking: Place radiopaque surgical clips at the margins of the resection bed to guide postoperative radiotherapy.
- Reconstruction and Closure: Perform soft-tissue reconstruction (e.g., rotational or free flaps) if primary closure is under tension or if critical structures are exposed.
Specific Tumor Subtypes
Undifferentiated Pleomorphic Sarcoma (Formerly Malignant Fibrous Histiocytoma)
The literature regarding Malignant Fibrous Histiocytoma (MFH) has undergone a significant paradigm shift. Formerly regarded as the most commonly diagnosed soft-tissue sarcoma in adults, modern immunohistochemistry and molecular diagnostics have led authorities to reclassify it. Today, "MFH" is largely considered a descriptive term for a heterogeneous group of tumors with no distinct line of differentiation, now more accurately termed Undifferentiated Pleomorphic Sarcoma (UPS).
Conventionally, this tumor describes a pleomorphic soft-tissue sarcoma exhibiting a storiform histological pattern of growth. It predominantly affects patients aged 50 to 70 years. Patients typically present with a large (>5 cm), painless, deep-seated mass, most frequently located in the thigh.
Imaging:
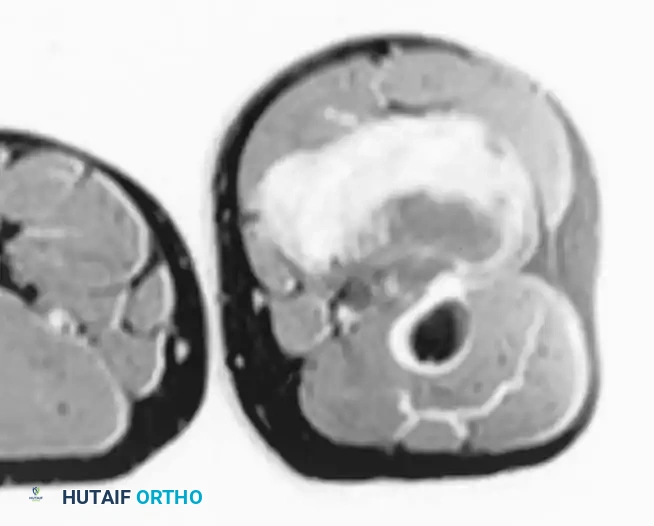
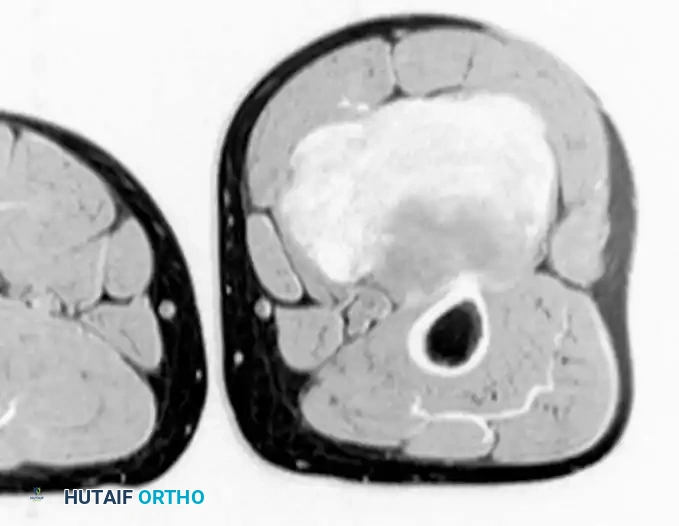
Conventional radiographs may demonstrate a non-specific soft-tissue density but are usually normal. MRI reveals a well-circumscribed mass that is typically isointense to muscle on T1-weighted images and hyperintense on T2-weighted images. Central necrosis is a hallmark of larger, high-grade tumors.
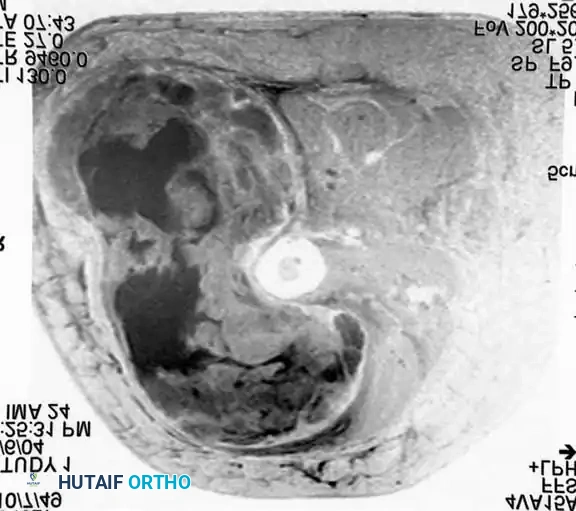
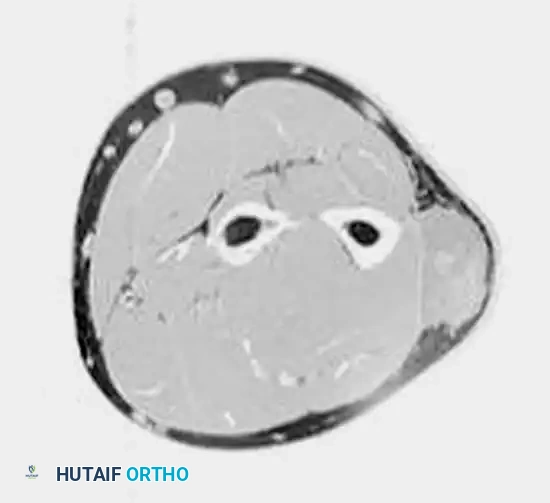
Axial MRI showing a large soft-tissue mass in the thigh with mixed signal intensity, characteristic of UPS/MFH.
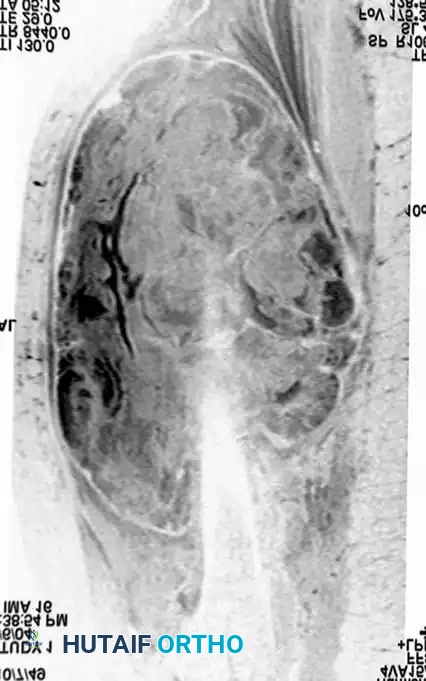
Coronal MRI demonstrating the proximal-distal extent of the tumor within the muscular compartment.
Treatment and Prognosis:
The cornerstone of treatment is wide surgical resection.
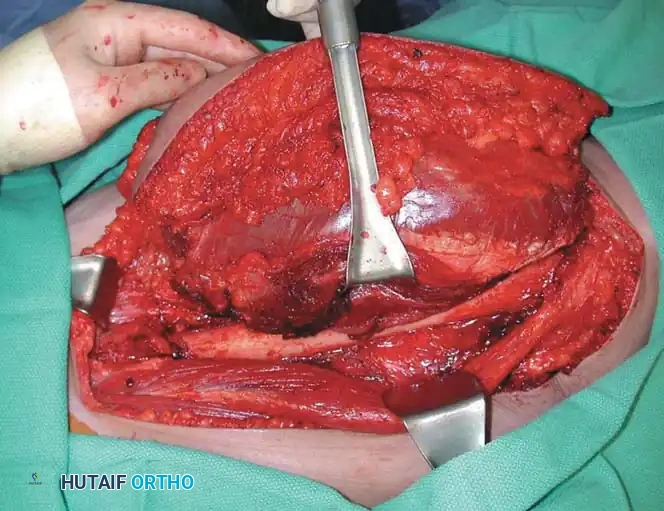
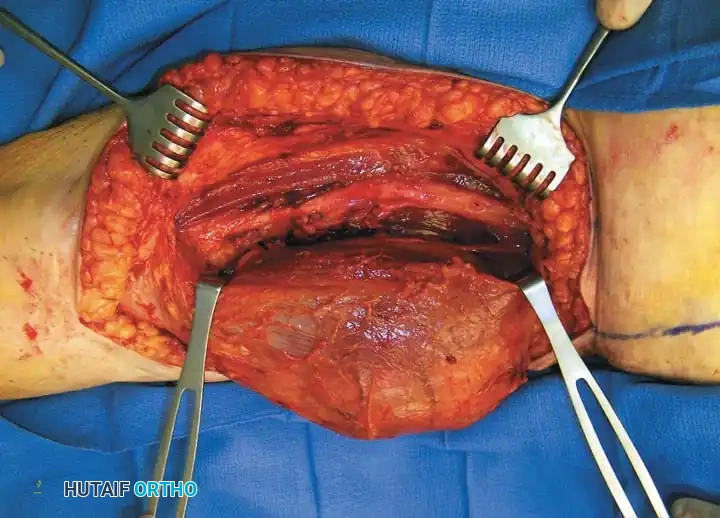
Intraoperative photograph demonstrating the tumor being resected with wide margins. Note that the biopsy tract is kept in continuity with the tumor specimen.
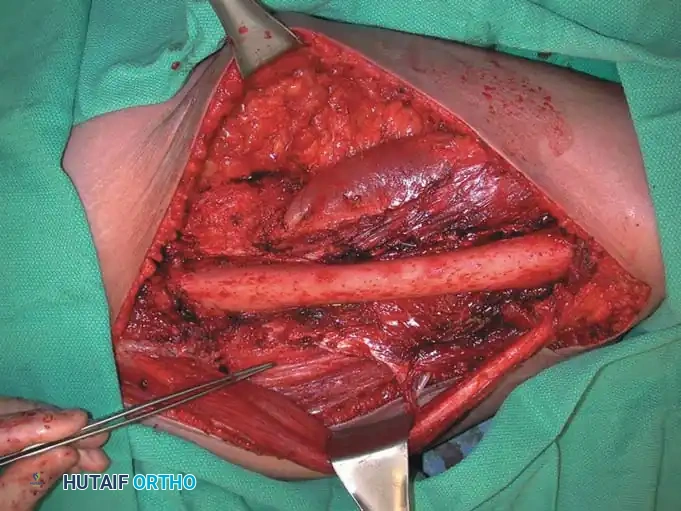
The tumor bed following wide resection, showing clean fascial and muscular margins.

Photograph of the resected specimen. The plane of dissection is entirely through normal muscle tissue, ensuring negative margins.
Radiation therapy is utilized as an adjuvant treatment for large, high-grade tumors or when surgical margins are close (<1 cm). Preoperative radiation is strongly considered for tumors initially deemed unresectable to facilitate downstaging. Chemotherapy remains controversial for adult soft-tissue sarcomas, though it is often considered for large (>5 cm), deep, high-grade lesions. With multimodal treatment, local recurrence rates should be maintained below 10%. The 5-year survival rate is approximately 60%, with poor prognostic indicators including high histological grade, large size, deep location, and the presence of pulmonary metastases.
Desmoid Tumors (Aggressive Fibromatosis)
While technically classified as intermediate (locally aggressive) rather than frankly malignant, desmoid tumors are critical to discuss due to their infiltrative growth and high propensity for local recurrence. They do not metastasize but can cause severe morbidity through local destruction.
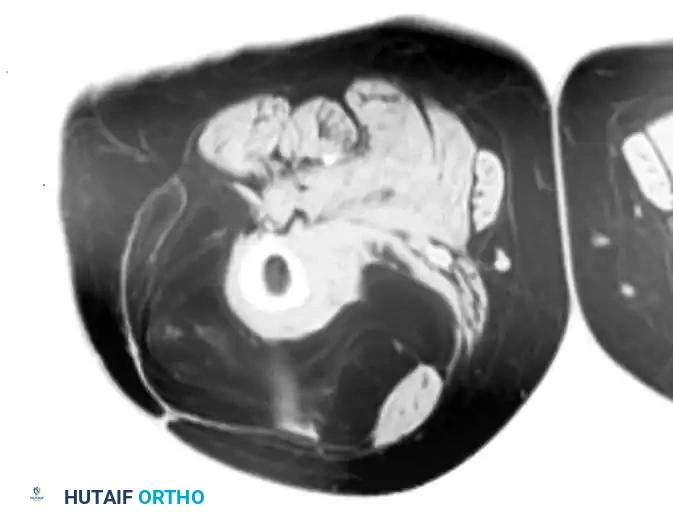
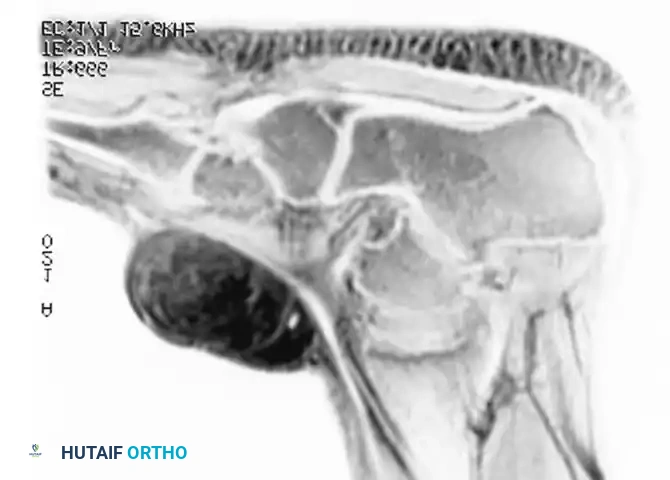
T1-weighted MRI of a desmoid tumor in the posterior thigh, demonstrating dark signal intensity.
T2-weighted MRI of the same desmoid tumor.

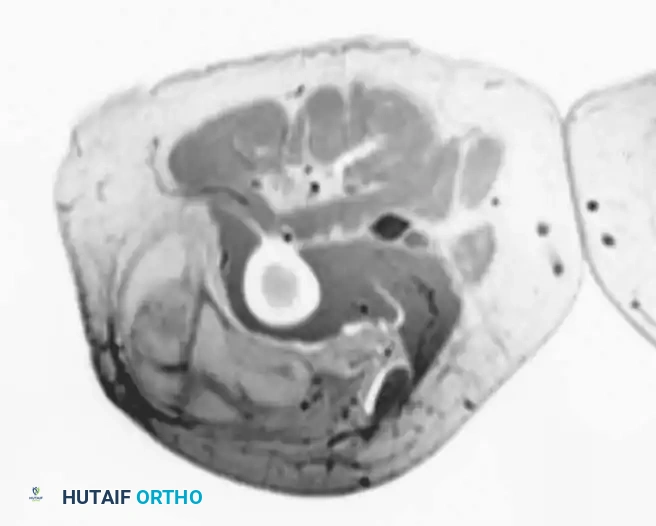
Sagittal MRI revealing a lobular mass tracking along the sciatic nerve.

Resected specimen of the desmoid tumor, characterized by dense, rubbery fibrous tissue.
Liposarcoma
Liposarcoma is the second most commonly diagnosed soft-tissue sarcoma. Similar to UPS, it predominantly affects adults over 50 years of age, presenting as a large, painless, deep-seated mass in the proximal extremities or retroperitoneum.
Histological Subtypes:
1. Well-Differentiated Liposarcoma (Atypical Lipomatous Tumor): Low-grade, locally aggressive, minimal metastatic potential.
2. Dedifferentiated Liposarcoma: High-grade progression from well-differentiated lesions.
3. Myxoid Liposarcoma: Intermediate to high grade, unique propensity for extrapulmonary metastases (e.g., retroperitoneum, spine).
4. Pleomorphic Liposarcoma: High-grade, aggressive, poor prognosis.
Imaging:
MRI is highly specific for well-differentiated variants, demonstrating fat signal intensity (bright on T1, suppresses on STIR/Fat-Sat) with thick, nodular septations.
T1-weighted MRI of a well-differentiated liposarcoma (atypical lipoma) of the thigh.
Contrast-enhanced, fat-suppressed axial MRI of the same lesion. Note the multiple thick, enhancing septa distinguishing it from a benign lipoma.
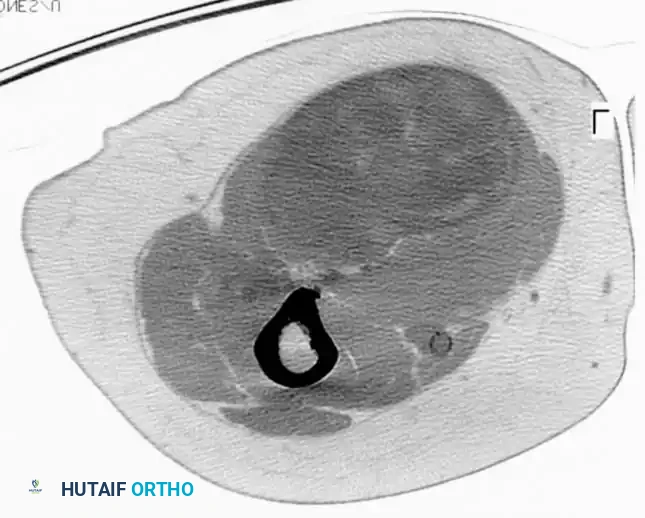
CT scan of the thigh in a 73-year-old patient demonstrating a large pleomorphic liposarcoma adjacent to the sciatic nerve.
Intraoperative photograph demonstrating the wide resection of the pleomorphic liposarcoma, requiring meticulous dissection to preserve the sciatic nerve.
Treatment:
Well-differentiated liposarcomas of the extremities are treated with wide surgical excision alone. Higher-grade variants (myxoid, pleomorphic, dedifferentiated) require multimodal therapy analogous to UPS. Patients with myxoid liposarcoma require specialized staging, including CT of the abdomen and pelvis, and whole-spine MRI due to their unique metastatic patterns.
Synovial Sarcoma
Synovial sarcoma presents unique clinical features compared to other adult soft-tissue sarcomas. It frequently affects young adults (15-40 years) and has a strong predilection for the distal extremities, particularly around the knee, foot, and hand.
Surgical Warning: The term "synovial sarcoma" is a historical misnomer. These tumors rarely arise from intra-articular synovial tissue; rather, they occur in the periarticular soft tissues. Do not assume joint involvement without clear MRI evidence.
Clinically, they often present as slow-growing, deceptively small (<5 cm) masses that may be painful, leading to frequent misdiagnosis as benign cysts or tendinopathy.
Imaging and Pathology:
Plain radiographs show amorphous, stippled calcifications within the soft-tissue mass in up to 30% of cases. Genetically, they are characterized by the pathognomonic t(X;18) chromosomal translocation.

AP radiograph of the wrist in a 67-year-old patient showing irregular calcifications within a soft-tissue mass.

CT scan better delineating the intralesional calcifications.

MRI demonstrating the full extent of the synovial sarcoma in the distal forearm/wrist.

Intraoperative photograph during the wide resection of the synovial sarcoma, requiring careful mobilization of tendons and neurovascular structures.

Intraoperative photograph of the tumor bed after complete wide resection.
Treatment:
Treatment consists of wide resection and radiotherapy. Notably, synovial sarcoma has a higher incidence of lymph node metastasis (up to 20%) compared to other sarcomas. Regional lymph nodes must be carefully evaluated clinically and radiographically.
Fibrosarcoma and Epithelioid Sarcoma
Fibrosarcoma:
True adult fibrosarcoma is now considered a rare diagnosis of exclusion. Microscopically, it is characterized by spindle cells arranged in a classic "herringbone" pattern. It typically presents as a deep, painless mass in the lower extremity. Treatment mirrors that of UPS.
Epithelioid Sarcoma:
This is a rare, slow-growing tumor that typically affects adolescents and young adults, frequently involving the distal upper extremities (hands and fingers). It often presents as a superficial, ulcerated nodule, mimicking benign conditions like warts, granulomas, or squamous cell carcinoma.
* Clinical Pitfall: Due to its indolent appearance, it is frequently subjected to unplanned, inadequate excisions.
* Behavior: It is highly aggressive, with a propensity for proximal lymphatic spread and a local recurrence rate exceeding 50%. Treatment requires aggressive wide resection
Associated Surgical & Radiographic Imaging





📚 Medical References
- soft-tissue sarcoma, J Bone Joint Surg 71A:370, 1989.
- Beltran J, Aparisi F, Bonmati LM, et al: Eosinophilic granuloma: MRI manifestations, Skeletal Radiol 22:157, 1993.
- Benedetti M, Catani F, Donati D, et al: Muscle performance about the knee joint in patients who had distal femoral replacement after resection of a bone tumor: an objective study with use of gait analysis, J Bone Joint Surg 82A:1619, 2000.
- Bibbo C, Patel DV, Benevenia J: Perioperative considerations in patients with metastatic bone disease, Orthop Clin North Am 31:577, 2000.
- Bielack S, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols, J Clin Oncol 20:776, 2002.
- Bieling P, Rehan N, Winkler P, et al: Tumor size and prognosis in aggressively treated osteosarcoma, J Clin Oncol 14:848, 1996.
- Bini SA, Gill K, Johnston JO:
