Introduction to Magnetic Resonance Imaging in Orthopaedics
Aside from routine radiography, no imaging modality has exerted as profound an effect on the contemporary practice of orthopaedic surgery as Magnetic Resonance Imaging (MRI). By providing unsurpassed soft-tissue contrast, multiplanar imaging capabilities, and spatial resolution that rivals Computed Tomography (CT), MRI has fundamentally altered diagnostic algorithms. Consequently, MRI has largely superseded older, invasive imaging modalities such as myelography, conventional arthrography, and diagnostic angiography.
In complex anatomic regions such as the knee, shoulder, and spine, MRI has evolved into an indispensable diagnostic instrument, empowering the orthopaedic surgeon to evaluate intra-articular and extra-articular structures that remain imperceptible to other noninvasive techniques. As an evolving technology, the ultimate boundaries of MRI in orthopaedics are continually expanding. Ongoing advancements in hardware (e.g., ultra-high-field magnets) and software (e.g., artificial intelligence-driven image reconstruction) will undoubtedly further solidify the role of MRI in musculoskeletal medicine.
Fundamental Principles of MRI Physics
MRI is fundamentally distinct from radiographic imaging techniques that rely on ionizing radiation. Instead, MRI images are generated by exploiting the quantum mechanical properties of atomic nuclei when placed in a robust external magnetic field.
The Magnetic Field and Proton Alignment
The patient is positioned within a powerful superconducting magnet, typically generating a magnetic field ($B_0$) approximately 30,000 to 60,000 times stronger than the Earth’s magnetic field. This magnetic force interacts with nuclei possessing an odd number of protons or neutrons. In biological tissues, the most abundant and clinically relevant element satisfying this criterion is hydrogen, which is ubiquitous in water and lipid molecules.
Hydrogen nuclei (protons) possess an intrinsic angular momentum known as "quantum spin." When subjected to the $B_0$ magnetic field, these protons align their spin axes either parallel (low energy) or anti-parallel (high energy) to the field. Because all imaging is performed within this constant magnetic force, this alignment establishes a steady state of longitudinal magnetization, or equilibrium.
Radiofrequency Excitation and Relaxation
To generate an image, this steady state must be perturbed. A radiofrequency (RF) pulse ($B_1$) is applied at the specific resonant frequency (Larmor frequency) of the hydrogen protons. This pulse excites the magnetized protons, flipping their magnetization vector away from the longitudinal axis and into the transverse plane.
Once the RF pulse is terminated, the protons begin to "relax" or return to their baseline equilibrium state. During this relaxation phase, the protons emit a radiofrequency signal. A receiver coil (antenna) captures this emitted signal. Through the application of localizing gradient magnetic fields and complex mathematical algorithms (Fourier transformation), these signals are spatially encoded and converted into the high-resolution MRI images utilized in clinical practice.
Clinical Pearl: Understanding the physics of relaxation is critical for the orthopaedic surgeon. The rate at which protons return to the longitudinal axis is the T1 relaxation time, while the rate at which they lose phase coherence in the transverse plane is the T2 relaxation time. These intrinsic tissue properties dictate the contrast seen on the final image.
Types of Magnetic Resonance Imaging Sequences
Although all MRI studies involve magnetization and RF signals, the precise timing of excitation and signal acquisition can be manipulated to alter tissue contrast. Most musculoskeletal MRI protocols rely heavily on the spin-echo technique, which produces T1-weighted, T2-weighted, and proton density (PD)-weighted images.
T1, T2, and Proton Density Weighting
By varying the repetition time (TR)—the interval between successive RF pulses—and the echo time (TE)—the time between the RF pulse and signal acquisition—specific tissue characteristics are accentuated:
- T1-Weighted Images (Short TR, Short TE): Provide excellent anatomic detail. Fat yields a high signal (bright), making T1 ideal for evaluating bone marrow, subacute hemorrhage, and lipomatous tumors.
- T2-Weighted Images (Long TR, Long TE): Highly sensitive to water content. Fluid yields a high signal (bright). T2 sequences are the workhorse for identifying pathology, as edema, inflammation, infection, and tumors typically exhibit increased water content.
- Proton Density (PD) Images (Long TR, Short TE): Maximize the signal from the number of hydrogen protons present. PD sequences provide exceptional spatial resolution and are the gold standard for evaluating fibrocartilaginous structures like the menisci and the glenoid labrum.
Signal Characteristics of Musculoskeletal Tissues:
* High Signal (Bright) on T1: Subcutaneous fat, yellow bone marrow, gadolinium contrast.
* High Signal (Bright) on T2: Synovial fluid, edema, cysts, cerebrospinal fluid (CSF).
* Low Signal (Dark) on All Sequences: Cortical bone, tendons, ligaments, and fibrocartilage (due to a lack of mobile protons).
Fast Spin-Echo and Fat Suppression Techniques
Faster imaging methods, such as the Fast Spin-Echo (FSE) technique, utilize a train of multiple echoes to reduce the acquisition time of T2-weighted sequences by two-thirds or more. However, FSE can introduce a blurring artifact that may obscure subtle abnormalities, such as nondisplaced meniscal tears. Furthermore, fat remains paradoxically bright on FSE T2-weighted images, which can mask adjacent bone marrow edema.
To counteract this, Fat Suppression Techniques are employed. Chemical shift fat suppression exploits the slight difference in resonant frequencies between water and fat protons, selectively nulling the fat signal. Alternatively, Short-Tau Inversion Recovery (STIR) sequences use a specific inversion pulse to suppress fat uniformly, even in the presence of magnetic field inhomogeneities.
Surgical Warning: When evaluating a patient for occult fractures, osteomyelitis, or soft-tissue neoplasms, fat-suppressed T2-weighted or STIR images are mandatory. Without fat suppression, pathological edema may be indistinguishable from normal adjacent adipose tissue.
Chemical Shift Fat-Suppression Technique in Tumor Imaging:
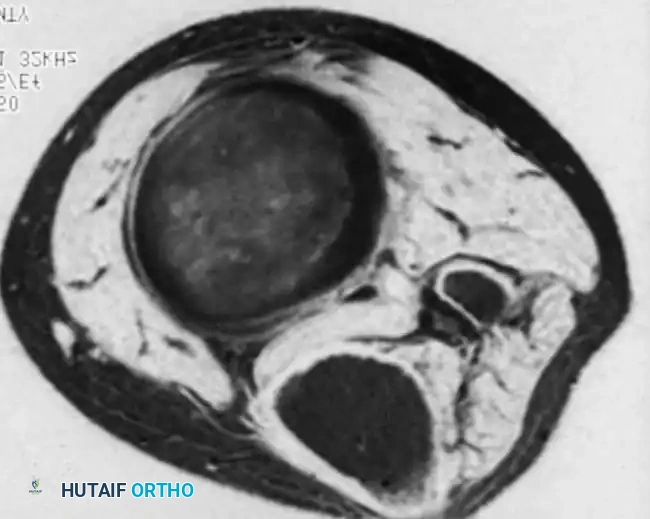
Figure 2-1A: Axial fast spin-echo, T2-weighted image of a large soft-tissue mass in the calf. The hyperintense (bright) fat blends with the anterior and posterior margins of the lesion, making the exact surgical boundaries difficult to ascertain.
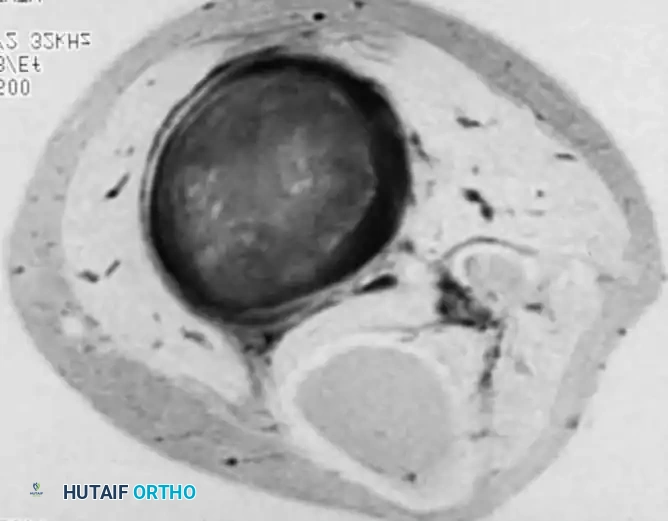
Figure 2-1B: The addition of chemical shift fat suppression on the same axial slice. The fat signal is nulled (dark), allowing for stark contrast between the hyperintense tumor and the surrounding suppressed tissues. This precise delineation of tumor margins is critical for preoperative surgical planning and determining the necessary resection margins.
Gradient-Echo (GRE) Techniques
Gradient-echo sequences utilize variable flip angles and gradient reversals rather than a 180-degree refocusing pulse. This makes GRE highly sensitive to magnetic susceptibility artifacts (useful for detecting hemosiderin in pigmented villonodular synovitis or loose hardware). GRE is also selectively utilized for high-resolution articular cartilage imaging and evaluating the glenoid labrum.
Hardware Considerations: Field Strength and Coil Technology
A wide variety of MRI systems are commercially available, primarily categorized by their magnetic field strength, measured in Tesla (T).
High-Field vs. Low-Field Scanners
- High-Field Scanners (1.0 T to 3.0 T): Generate a higher signal-to-noise ratio (SNR). This allows for shorter scanning times, thinner anatomical slices, and smaller fields of view, resulting in superior spatial resolution. High-field systems are essential for advanced techniques like chemical shift fat suppression and high-resolution cartilage mapping.
- Low-Field Scanners (≤ 0.3 T): Often feature an "open" configuration, which significantly improves patient comfort, reduces claustrophobia, and facilitates the imaging of off-axis structures (e.g., kinematic studies of the wrist or elbow). While less expensive to operate, they lack the SNR required for advanced fat suppression.
Evidence-Based Note: While high-field scanners are the gold standard, some comparative studies suggest that the diagnostic accuracy of low-field scanners for gross meniscal and ligamentous pathology in the knee may be clinically acceptable. However, for complex articular cartilage evaluation or tumor staging, high-field MRI remains imperative.
Surface Coils and Phased-Array Technology
While the main body coil is sufficient for large regions (chest, abdomen, pelvis, thighs), the evaluation of smaller articular structures (menisci, rotator cuff, carpal ligaments) requires specialized surface coils. These coils act as localized antennae placed directly adjacent to the region of interest, markedly improving the SNR and spatial resolution.
Modern MRI systems utilize phased-array technology, which combines multiple small surface coils into a single unit. This provides the high SNR of a small coil while offering the expanded anatomic coverage of a larger coil. Optimal coil selection and meticulous patient positioning are mandatory prerequisites for high-quality musculoskeletal imaging.
Regional Orthopaedic Applications
Because imaging planes (axial, sagittal, coronal, oblique) and sequence types are chosen at the outset, an advanced understanding of the clinical problem is required to tailor the MRI protocol.
The Knee
MRI is the definitive noninvasive modality for the knee.
* Menisci: Normal menisci appear as uniformly dark, wedge-shaped structures on all sequences. Pathological conditions, such as myxoid degeneration (Grade 1 and 2 signal) or true tears (Grade 3 signal extending to an articular surface), are best evaluated on sagittal and coronal PD-weighted images.
* Cruciate Ligaments: The Anterior Cruciate Ligament (ACL) is evaluated on sagittal and oblique-sagittal planes. Primary signs of rupture include discontinuity, abnormal orientation, and diffuse hyperintensity. Secondary signs include bone bruises in the lateral femoral condyle and posterolateral tibial plateau (the "kissing contusion" mechanism).
* Articular Cartilage: High-resolution FSE or GRE sequences are utilized to detect chondral fissuring, delamination, or full-thickness defects, directly influencing the choice between microfracture, osteochondral autograft transfer (OATS), or autologous chondrocyte implantation (ACI).
The Shoulder
MRI, particularly MR arthrography (MRA), is invaluable for shoulder pathology.
* Rotator Cuff: Coronal oblique and sagittal oblique planes are aligned parallel and perpendicular to the supraspinatus tendon. MRI accurately differentiates between tendinosis, partial-thickness tears (articular vs. bursal sided), and full-thickness tears, while also assessing muscle atrophy and fatty infiltration (Goutallier classification), which dictates surgical repairability.
* Labrum and Instability: The glenoid labrum is best evaluated with MRA in the axial and ABER (Abduction and External Rotation) positions. This distends the joint capsule, allowing contrast to interpose into Bankart lesions, SLAP (Superior Labrum Anterior and Posterior) tears, and capsular stripping.
The Hip
- Osteonecrosis (Avascular Necrosis): MRI is the most sensitive modality for early detection of AVN. The pathognomonic "double-line sign" on T2-weighted images represents the reactive interface between ischemic necrotic bone and advancing granulation tissue.
- Occult Trauma: In elderly patients with hip pain and negative radiographs, coronal T1 and STIR sequences rapidly identify occult femoral neck or intertrochanteric fractures, allowing for prompt surgical fixation and preventing catastrophic displacement.
- Femoroacetabular Impingement (FAI): Radial sequences around the femoral neck axis are used to evaluate the alpha angle (cam morphology) and assess the acetabular labrum and adjacent chondral delamination.
The Spine
- Intervertebral Disc Disease: Sagittal and axial T2-weighted images clearly delineate disc desiccation (loss of bright T2 signal), annular fissures (high-intensity zones), and the exact morphology of disc herniations (bulge, protrusion, extrusion, sequestration) in relation to the thecal sac and exiting nerve roots.
- Postoperative Back Pain: Differentiating recurrent disc herniation from postoperative epidural fibrosis is a common clinical dilemma. The administration of intravenous gadolinium contrast is essential; vascularized epidural scar tissue will enhance, whereas an avascular recurrent disc fragment will not.
- Spinal Tumors and Infection: MRI is the modality of choice for evaluating vertebral osteomyelitis, discitis, and epidural abscesses, as well as staging primary and metastatic spinal neoplasms.
Foot and Ankle
- Tendon Injuries: The Achilles, posterior tibial, and peroneal tendons are evaluated for tenosynovitis, tendinosis, and tears. Axial images are particularly useful for assessing tendon cross-sectional morphology and identifying longitudinal split tears.
- Ligament Injuries: The anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) are assessed in chronic lateral ankle instability to plan for Broström-Gould anatomical repairs.
- Osteochondral Lesions: MRI stages osteochondral lesions of the talus (OCLT), assessing the stability of the osteochondral fragment by identifying high T2 signal (fluid) undercutting the lesion.
Hand, Wrist, and Elbow
- Carpal Ligaments: High-resolution imaging with dedicated wrist coils is required to evaluate the scapholunate (SL) and lunotriquetral (LT) interosseous ligaments, as well as the Triangular Fibrocartilage Complex (TFCC).
- Elbow: MRI evaluates the Ulnar Collateral Ligament (UCL) in throwing athletes (often utilizing MR arthrography), distal biceps tendon ruptures, and the extent of tendinosis in lateral epicondylitis prior to surgical debridement.
Musculoskeletal Tumor Imaging
MRI is the cornerstone of the staging and surgical planning for musculoskeletal neoplasms. The primary goals are to determine the exact anatomic extent of the lesion, its relationship to major neurovascular bundles, and the presence of skip metastases within the same bone.
- T1-Weighted Images: Essential for evaluating the extent of marrow replacement. Normal bright fatty marrow is replaced by the dark signal of the tumor cells.
- T2-Weighted Fat-Suppressed Images: Crucial for defining the extraosseous soft-tissue extension and peritumoral edema. As demonstrated in Figure 2-1, fat suppression allows the surgeon to accurately delineate the tumor margins, which is a prerequisite for planning limb-sparing wide local excisions.
- Gadolinium Enhancement: Intravenous contrast helps differentiate cystic/necrotic areas from solid, vascularized tumor tissue, guiding the orthopaedic oncologist to the most viable region for a diagnostic biopsy.
Summary
Magnetic Resonance Imaging has fundamentally transformed the diagnostic landscape of orthopaedic surgery. By mastering the principles of MRI physics, understanding the nuances of various imaging sequences, and recognizing the specific indications for regional applications, the orthopaedic surgeon can leverage this powerful modality to formulate precise diagnoses. Whether evaluating a subtle meniscal tear, planning a complex rotator cuff repair, or staging a high-grade sarcoma, a profound understanding of MRI is an indispensable component of modern, evidence-based orthopaedic practice.
