Introduction to Limb-Length Discrepancy
Limb-length equality in the lower extremity is not merely a cosmetic concern; it is a profound functional and biomechanical imperative. The presence of a significant limb-length discrepancy (LLD) alters normal gait kinematics, resulting in a "short leg gait." This compensatory mechanism is inherently awkward and substantially increases energy expenditure due to the excessive vertical rise and fall of the pelvis during the stance phase. Over time, long-standing and significant discrepancies can lead to secondary musculoskeletal pathology.
While Papaioannou et al., in a study of 23 young adults with untreated LLDs ranging from 1.2 to 5.2 cm, noted compensatory scoliosis and decreased spinal mobility without overt back pain, larger epidemiological studies present a different consensus. Giles and Taylor, alongside Friberg, evaluated much larger patient cohorts and definitively concluded that significant limb-length discrepancy is a direct catalyst for low back pain. Furthermore, they demonstrated that this pain is reliably diminished following successful limb equalization procedures.
Etiology of Limb-Length Inequality
The etiology of LLD is highly variable and dictates both the natural history of the discrepancy and the optimal treatment strategy. Causes can be broadly categorized into:
* Trauma or Infection: Damage to the physis (e.g., Salter-Harris fractures, osteomyelitis, or septic arthritis) leading to premature partial or complete physeal arrest.
* Paralytic Conditions: Asymmetrical muscle forces and decreased weight-bearing in conditions such as poliomyelitis or cerebral palsy (spastic hemiplegia/diplegia) often result in hypoplasia of the affected limb.
* Tumors and Tumor-like Conditions: Pathologies that stimulate asymmetrical bone growth via localized hyperemia. Conditions such as juvenile rheumatoid arthritis (JRA), fibrous dysplasia, or post-fracture hypervascularity (commonly seen in pediatric femoral shaft fractures) can lead to limb overgrowth.
* Congenital and Idiopathic: Idiopathic unilateral hypoplasia (e.g., proximal focal femoral deficiency, fibular hemimelia) and hyperplasia (e.g., hemihypertrophy syndromes) remain common presentations in pediatric orthopedics.
Clinical Pearl: The treatment of limb-length discrepancy must be meticulously tailored to the specific conditions and needs of the individual patient. A "cookie-cutter" approach is destined to fail. Treatment plans can only be formulated after a comprehensive evaluation assessing chronological and skeletal age, current and predicted discrepancy, predicted adult height, joint functional status, and the psychosocial background of the patient's family.
Clinical Assessment
The foundation of LLD management is a rigorous clinical examination. The simplest, yet often most functionally accurate, means of measuring limb-length discrepancy is the clinical block test. Wooden blocks of known heights are placed under the foot of the short leg until the examiner palpates a level pelvis (assessed at the anterior superior iliac spines [ASIS] and iliac crests).
While tape measurement from the ASIS to the medial malleolus is a standard clinical tool, it is fraught with inaccuracies due to variations in patient positioning, pelvic obliquity, and asymmetrical pelvic development.
Comprehensive clinical evaluation must also include an assessment for:
* Rotational and angular deformities.
* Foot height differences (often overlooked but critical for total limb length).
* Compensatory or structural scoliosis.
* Pelvic obliquity.
* Joint mobility and function.
Surgical Warning: Flexion contractures of the knee and hip will make the limb appear artificially shorter on both clinical and radiographic examinations. Always perform a Thomas test to rule out hip flexion contractures and assess maximum knee extension before finalizing LLD measurements.
In certain paralytic conditions, the goals of treatment may deviate from perfect equality. For instance, in spastic diplegia, a mild shortness of the paralytic side can actually improve gait mechanics by allowing the paralytic foot to clear the floor more easily during the swing phase, preventing a steppage gait or circumduction. Conversely, in patients with rigid scoliosis and an oblique lumbosacral takeoff, maintaining some degree of LLD may be desirable to preserve a balanced spine.
Radiographic Assessment
Radiographic measurements are paramount for surgical accuracy, as clinically palpable landmarks are subject to soft tissue interference. Two commonly used radiographic techniques are the standing orthoradiograph and the scanogram.
The Orthoradiograph and Scanogram
Both techniques involve placing a radiopaque ruler behind the patient's limbs.
* Orthoradiograph: Made on a single long cassette that includes the hip, knee, and ankle on a single exposure. A magnification marker placed on the leg at the level of the bone minimizes magnification error. Standing orthoradiographs offer the critical additional benefit of demonstrating overall mechanical limb alignment. It is imperative that the legs be positioned with the patellae facing strictly forward to avoid rotational artifact.
* Scanogram: Utilizes three separate, localized exposures of the hip, knee, and ankle joints. Because the x-ray beam is centered directly over each joint, parallax error is virtually eliminated. However, it requires the child to remain absolutely still for all three exposures.

Advanced Imaging: CT Scanograms
Computed Tomography (CT) scanograms have largely superseded standard plain-film scanograms in modern centers. They offer reduced radiation exposure without compromising accuracy. Crucially, as demonstrated by Huurman et al., lateral CT scanograms allow for highly accurate measurements even in limbs with severe flexion deformities. Furthermore, biplanar CT scanograms, proposed by Carey et al., allow for the precise measurement of foot height, ensuring the entire functional limb length is accounted for.
Skeletal Age Determination
A standardized radiograph of the left wrist and hand is obtained to estimate skeletal age using the Greulich and Pyle atlas. Note that this is generally unnecessary for children younger than 5 years old, as skeletal and chronological ages do not significantly diverge in this demographic.
Growth Prediction and Timing of Intervention
Determining the precise timing for limb equalization procedures—particularly epiphysiodesis—requires accurate growth prediction. Several validated methods exist, each with distinct advantages and limitations.
The Green-Anderson and Moseley Methods
The Green-Anderson growth-remaining chart was the historical gold standard. It requires the clinician to estimate the percentage of growth inhibition by taking two interval measurements separated by at least 3 months. The growth difference between the involved and normal limb is multiplied by 100, then divided by the growth of the normal limb.
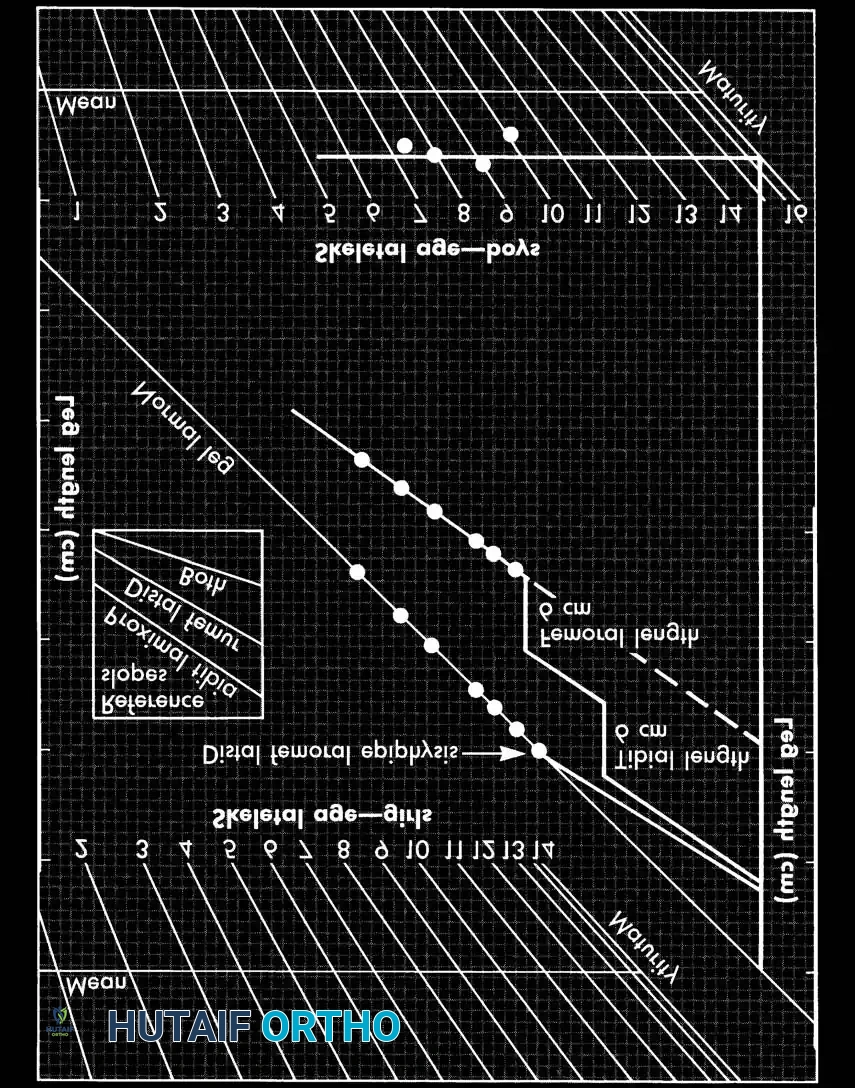
Moseley simplified this by mathematically manipulating the original data to fit a straight-line graph, making it visually intuitive. It avoids complex mathematical calculations of growth inhibition and provides a ready prediction of the results of epiphysiodesis, lengthening, and shortening.
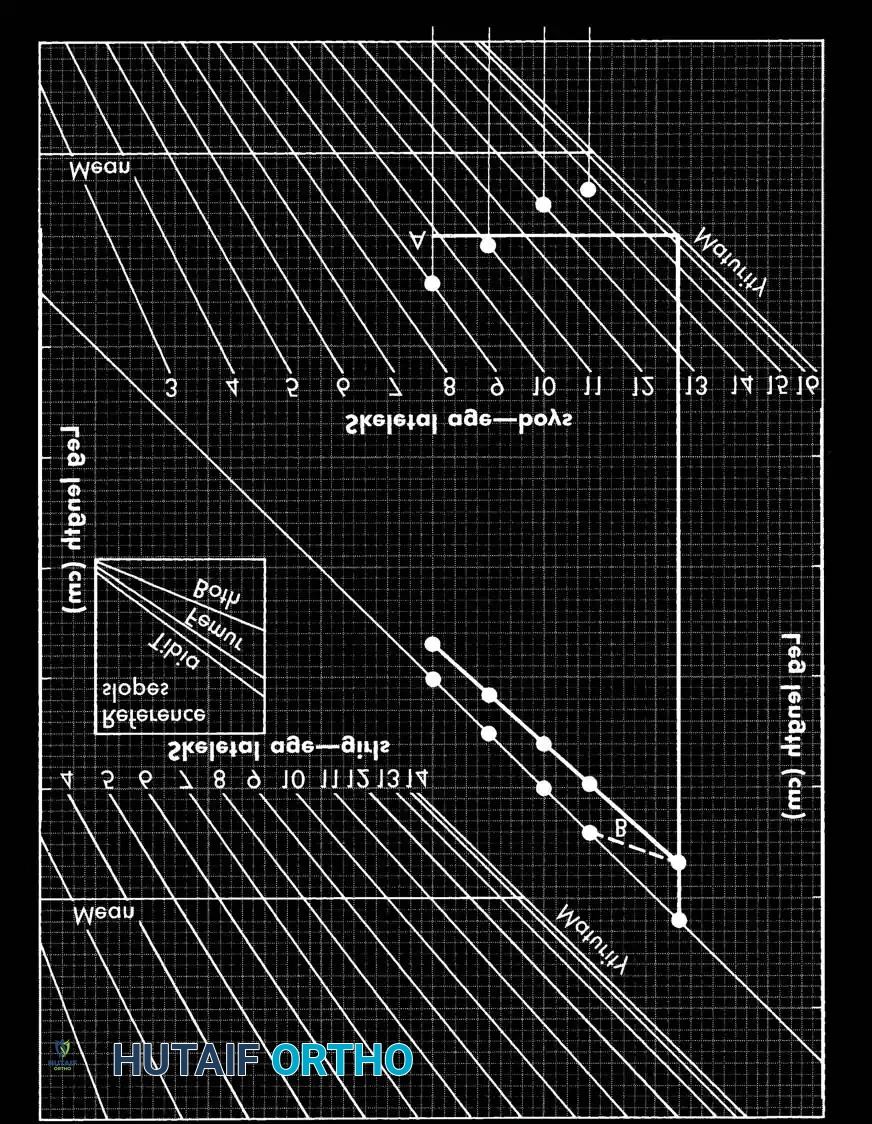
Instructions for the Moseley Straight-Line Graph:
1. Depiction of Past Growth: Plot the length of the normal leg, short leg, and skeletal age. Successive plots create a growth line. Inhibition is the difference in slope between the two lines.
2. Prediction of Future Growth: Extend the short leg's growth line to the maturity line. The vertical distance at maturity represents the predicted final discrepancy.
3. Effect of Surgery: For epiphysiodesis, a new growth line is drawn parallel to the reference slope for the fused physis (Distal femur = 37% of total leg growth; Proximal tibia = 28%; Both = 65%). For lengthening, the line is displaced upward by the exact length achieved, maintaining the same slope.
Critiques of Moseley/Green-Anderson: These methods do not inherently account for foot height. Furthermore, human growth is influenced by nutritional and hormonal factors, making it not perfectly mathematically predictable. Shapiro identified five distinct patterns of LLD, noting that conditions like JRA or Perthes disease may follow an "upward slope–downward slope" pattern where the discrepancy self-corrects, defying standard charts.
The Menelaus Method
The Menelaus method is a highly practical, arithmetic approach requiring no special charts. It relies on chronological age rather than skeletal age. Menelaus assumes:
* Distal femur grows 3/8 inch (approx. 1 cm) per year.
* Proximal tibia grows 1/4 inch (approx. 0.6 cm) per year.
* Growth ceases at age 14 in girls and 16 in boys.
Using this simple formula, Menelaus achieved a final LLD of less than 3/4 inch in 94 patients undergoing epiphysiodesis.
The Multiplier Method
Developed by Paley, Bhave, Herzenberg, and Bowen, the Multiplier method is currently favored for its rapid clinical utility. By dividing femoral and tibial lengths at skeletal maturity by their lengths at each age across percentiles, they derived a universal "multiplier."
Formulas using this multiplier predict LLD at skeletal maturity, growth remaining, and the exact timing for epiphysiodesis based on only one or two data points. Aguilar et al. clinically validated the Multiplier method, demonstrating it to be more accurate than both Moseley and Anderson methods, particularly for epiphysiodesis planning.
Surgical Management Strategies
The goals of treatment are a balanced spine and pelvis, equal limb lengths (a final clinical discrepancy of 1 to 1.5 cm is considered an excellent outcome), and a correct mechanical weight-bearing axis.
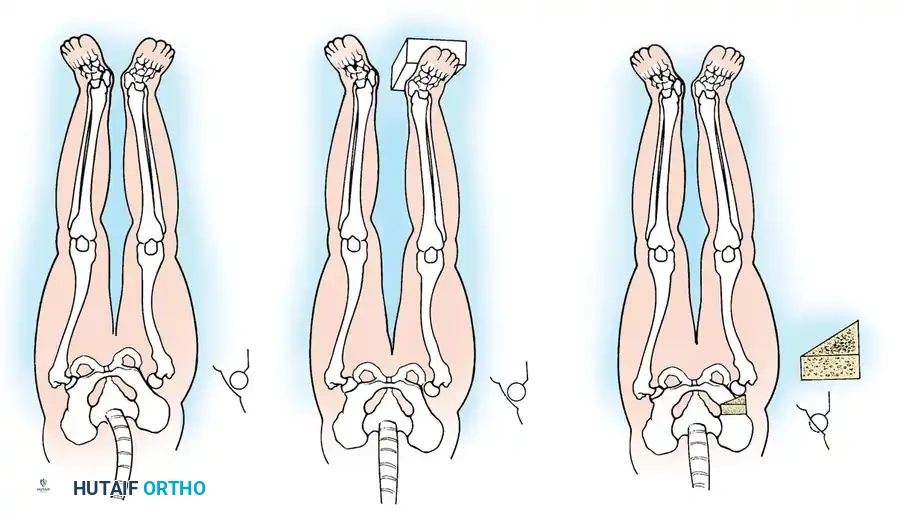
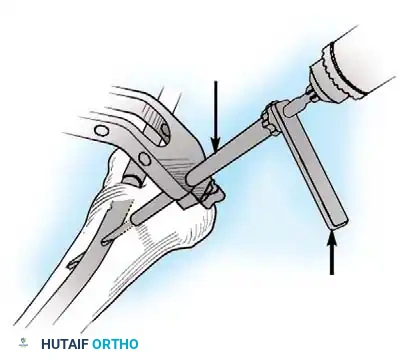
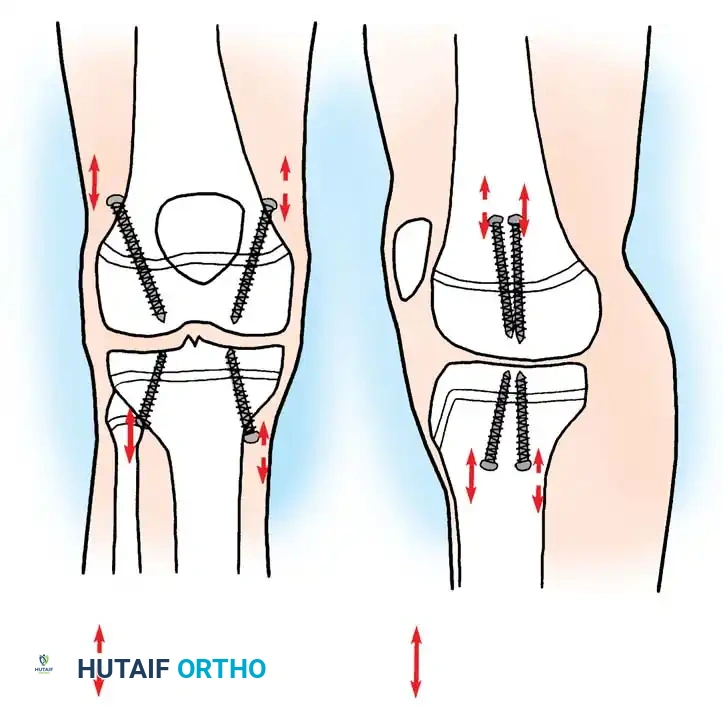
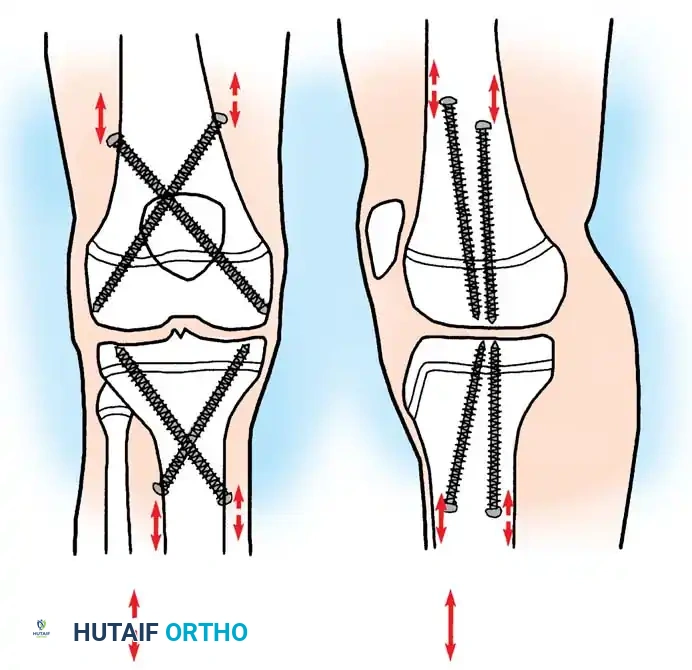
1. Epiphysiodesis
Epiphysiodesis (surgical arrest of the physis) of the longer limb is the procedure of choice for predicted discrepancies of 2 to 5 cm in growing children. It is minimally invasive, carries a low complication rate, and allows for rapid return to full weight-bearing.
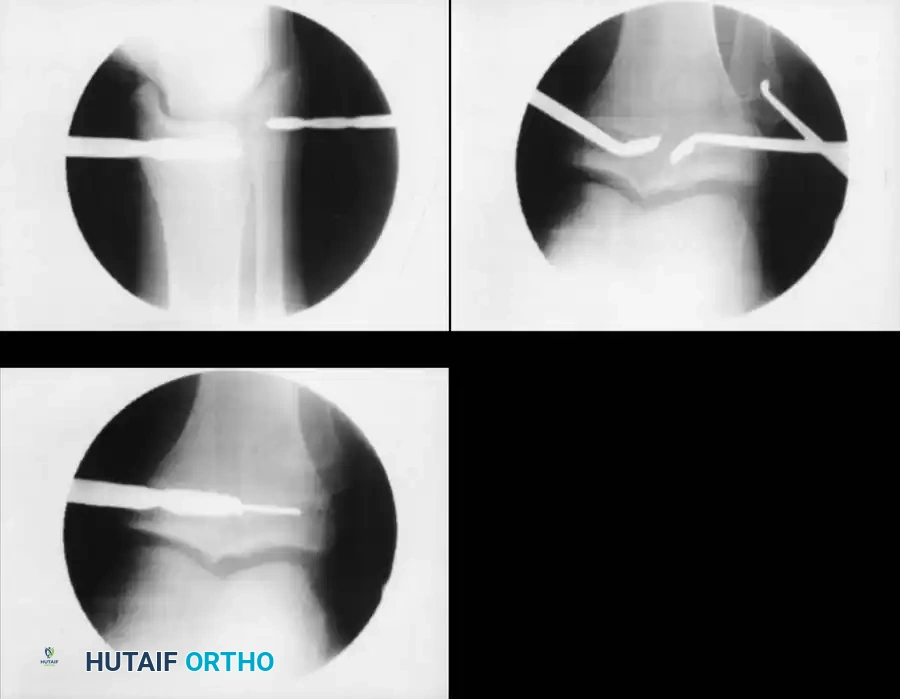
Surgical Technique (Percutaneous Approach):
1. Positioning: Supine on a radiolucent table. Fluoroscopy is mandatory.
2. Localization: The physis (distal femur or proximal tibia/fibula) is identified under AP and lateral fluoroscopy.
3. Incision and Drilling: Small medial and lateral incisions are made. A cannulated drill or specialized curette is introduced into the physis.
4. Ablation: The physeal cartilage is systematically destroyed in all quadrants. Care is taken to avoid violating the articular surface or the metaphyseal cortex.
5. Postoperative Protocol: Immediate weight-bearing as tolerated. Return to sports is typically permitted at 4 to 6 weeks once soft tissue healing is complete.
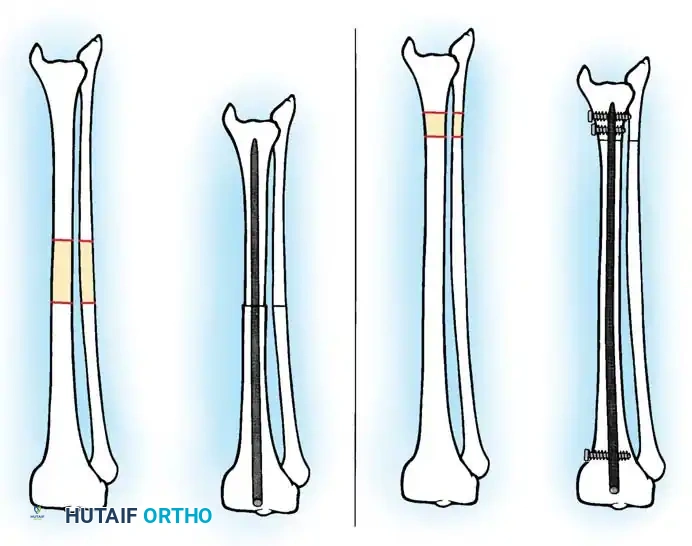
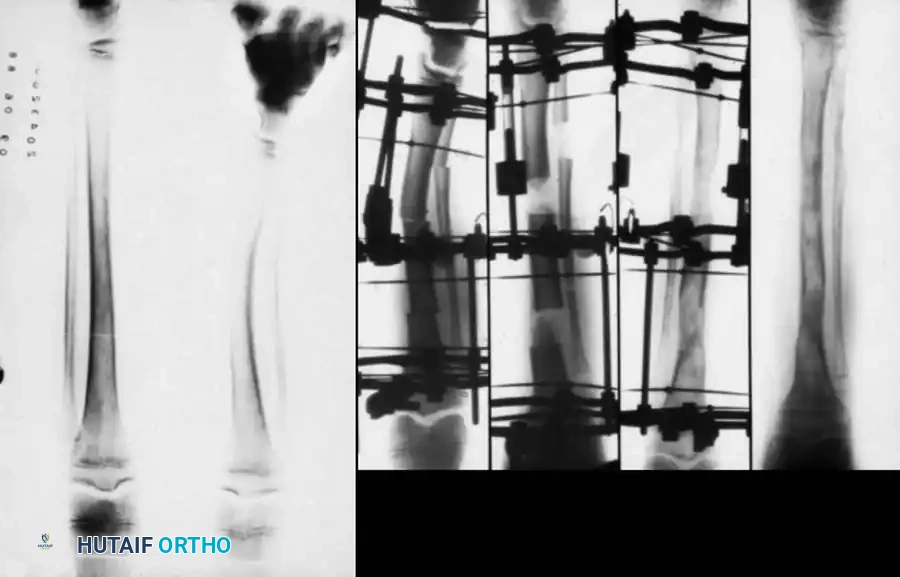
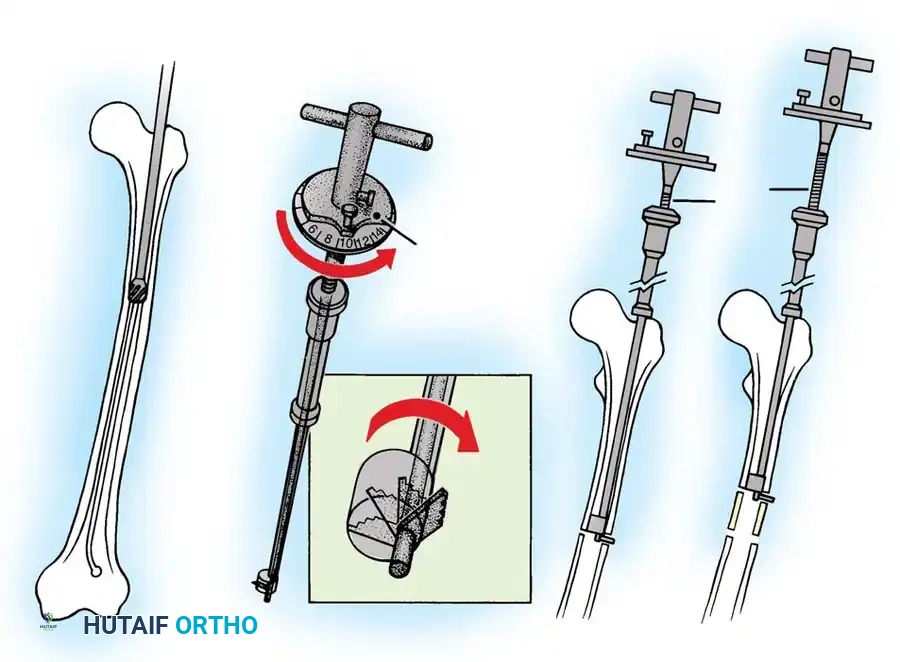
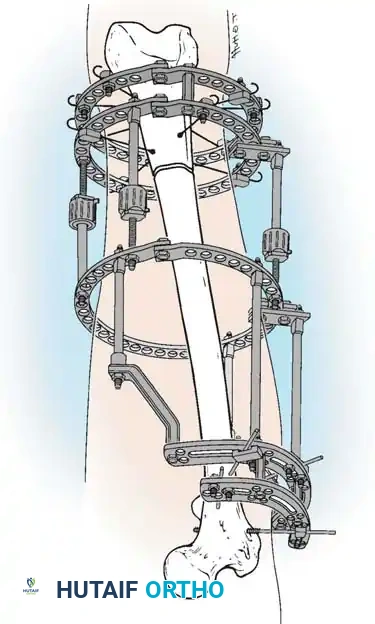
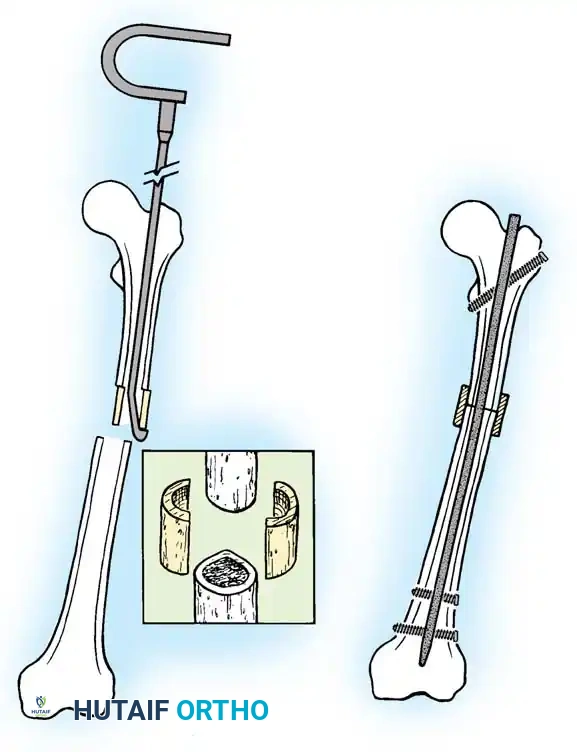
2. Limb Lengthening (Distraction Osteogenesis)
For discrepancies exceeding 5 cm, or when shortening the normal leg would result in unacceptable loss of overall height, lengthening of the short limb is indicated. This relies on the principles of distraction osteogenesis pioneered by Ilizarov.
Key Principles:
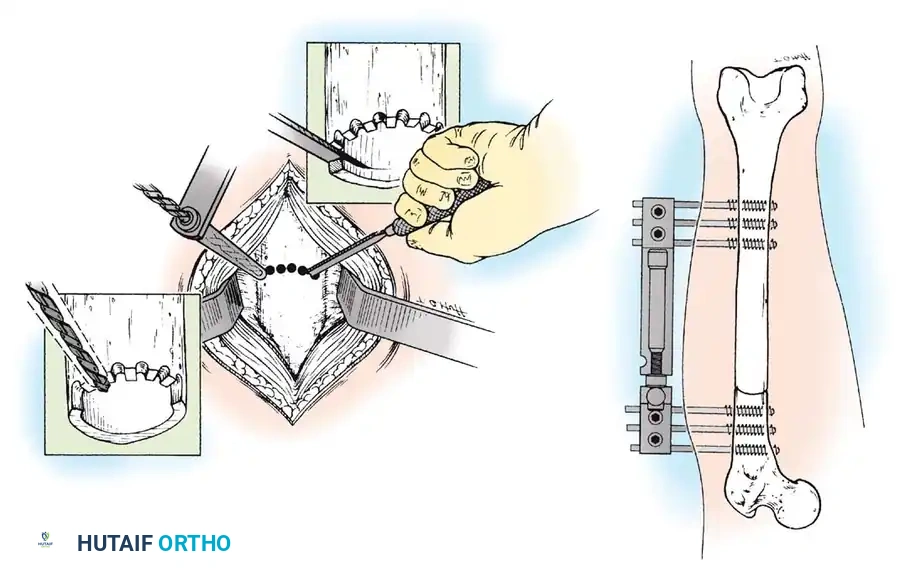
* Corticotomy: A low-energy osteotomy preserving the endosteal and periosteal blood supply.
* Latency Period: A delay of 5 to 7 days post-osteotomy before distraction begins, allowing for the initial formation of a soft callus.
* Rate and Rhythm: Distraction is typically performed at a rate of 1 mm per day, divided into four 0.25 mm increments.
* Consolidation: The frame or nail remains in place until the regenerate bone fully corticates.
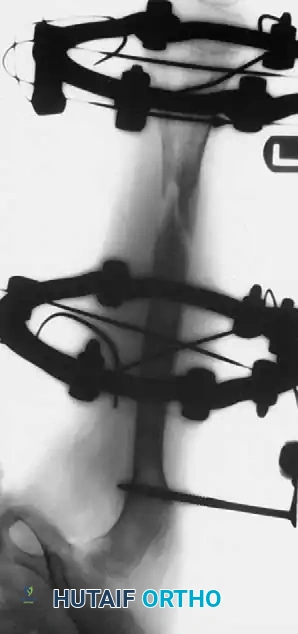
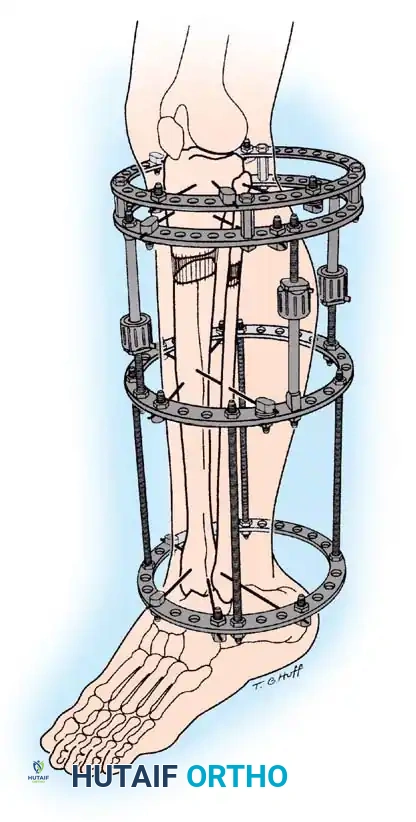
Techniques:
* External Fixation: Circular (Ilizarov/Taylor Spatial Frame) or monolateral frames. Excellent for simultaneous correction of angular deformities. However, pin-tract infections and joint stiffness are common.
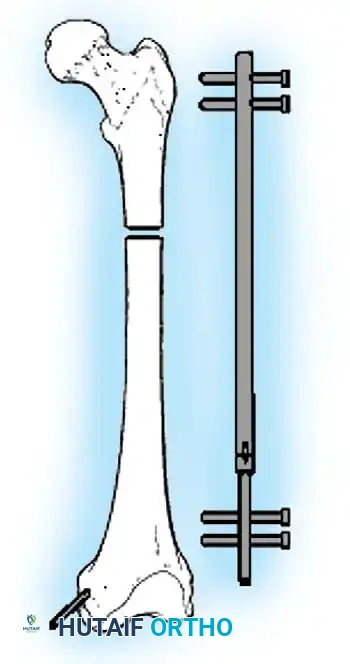
* Intramedullary Lengthening Nails: Motorized, magnetically controlled intramedullary nails (e.g., PRECICE) have revolutionized lengthening. They eliminate pin-tract infections, improve patient comfort, and provide excellent axial stability.
Pitfall: Lengthening the femur by more than 15-20% of its original length significantly increases the risk of knee subluxation, hip dysplasia, and severe soft tissue contractures. Prophylactic IT band release or concurrent physical therapy is mandatory.
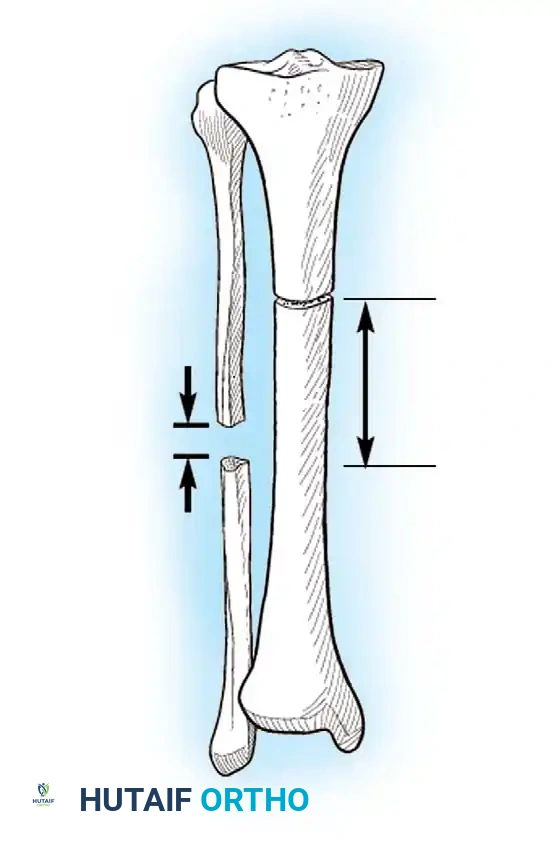
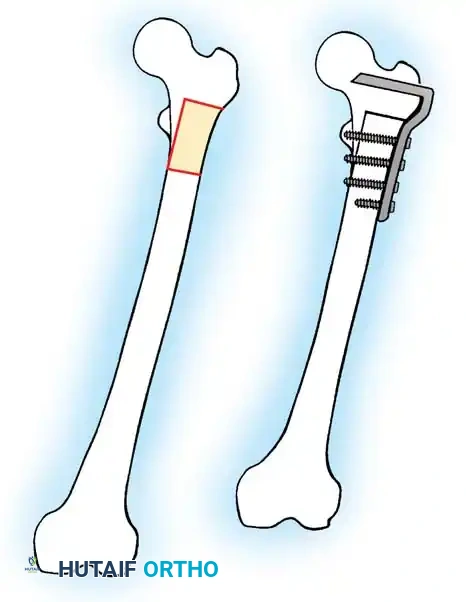
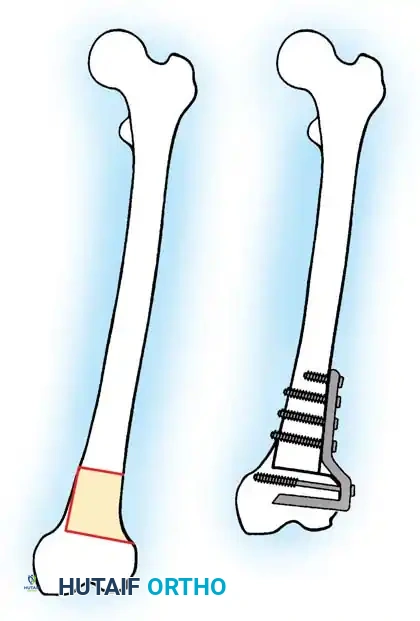
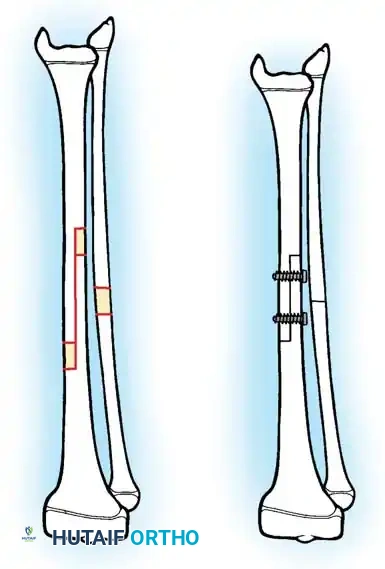
3. Acute Shortening Osteotomy
In skeletally mature patients with discrepancies of 2 to 5 cm, acute shortening of the longer limb is a highly effective, one-stage procedure.
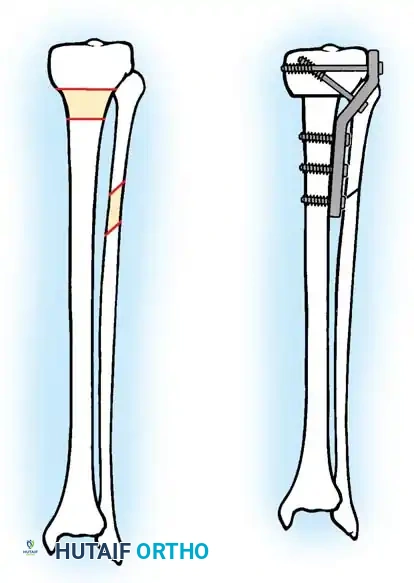
Femoral Shortening:
Typically performed in the subtrochanteric or diaphyseal region. A precise segment of bone is resected, and the femur is stabilized with an intramedullary nail. The maximum safe acute shortening in the femur is approximately 5 to 6 cm; beyond this, the redundant soft tissue envelope (quadriceps) loses its mechanical advantage, leading to profound weakness.
Tibial Shortening:
Less commonly performed due to the risk of compartment syndrome and the cosmetic deformity of a bulky calf. Maximum acute shortening is limited to 2 to 3 cm. Prophylactic anterior compartment fasciotomy is strongly recommended.

Postoperative Protocols and Complication Management
Regardless of the surgical technique chosen, meticulous postoperative care is required to ensure optimal outcomes.
- Physical Therapy: Aggressive mobilization of adjacent joints is critical, particularly during distraction osteogenesis, to prevent fixed contractures.
- Radiographic Monitoring: During lengthening, bi-weekly radiographs are necessary to assess the quality of the regenerate bone and ensure the distraction rate is appropriate (avoiding premature consolidation or non-union).
- Infection Control: For external fixators, daily pin-site care using chlorhexidine or half-strength hydrogen peroxide is standard protocol to mitigate superficial infections before they progress to osteomyelitis.
Conclusion
The management of limb-length discrepancy requires a masterclass understanding of pediatric growth biomechanics, precise radiographic interpretation, and versatile surgical skills. Whether utilizing the elegant simplicity of the Menelaus method for a percutaneous epiphysiodesis or orchestrating a complex multi-apical correction with a motorized intramedullary nail, the orthopedic surgeon's goal remains steadfast: the restoration of a balanced, functional, and pain-free mechanical axis.


📚 Medical References
- limb-length discrepancy following total hip arthroplasty, J Bone Joint Surg 85A:2310, 2003.
- Ranawat CS, Rao RR, Rodriguez JA, et al: Correction of limblength inequality during total hip arthroplasty, J Arthroplasty 16:715, 2001.
- Williamson JA, Reckling FW: Limb length discrepancy and related problems following total hip replacement, Clin Orthop 134:135, 1978.
- Dislocation and Subluxation Alberton GM, High WA, Morrey BF: Dislocation after revision total hip arthroplasty: an analysis of risk factors and treatment options, J Bone Joint Surg 84A:1788, 2002.
- Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty, J Bone Joint Surg 86A:9, 2004.
- Berry DJ, von Knoch M, Schleck CD, et al: Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty, J Bone Joint Surg 87A:2456, 2005.
- Callaghan JJ, O’Rourke MR, Goetz DD, et al: Use of a constrained tripolar acetabular liner to treat intraoperative instability and postoperative dislocation after total hip arthroplasty: a review of our experience, Clin Orthop Relat Res 429:117, 2004.
- Chiu FY, Chen CM, Chung TY, et al: The effect of posterior capsulorrhaphy in primary total hip arthroplasty: a prospective randomized study, J Arthroplasty 15:194, 2000.
- Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty, J Bone Joint Surg 74A:1334, 1992.
- DeWal H, Maurer S, Tsai P, et al: Effi cacy of abduction bracing in the management of total hip arthroplasty dislocation, J Arthroplasty 19:733, 2004.
- Dion MC, Scott RD, Schai PA, et al: A simple capsulorrhaphy in a posterior approach for total hip arthroplasty, J Arthroplasty 19:373, 2004.
- Ekelund A: Trochanteric osteotomy for recurrent dislocation of total hip arthroplasty, J Arthroplasty 8:629, 1993.
- Fackler CD, Poss R: Dislocation of total hip arthroplasties, Clin Orthop Relat Res 151:169, 1980.
- Goldstein WM, Gleason TF, Kopplin M, et al: Prevalence of dislocation after total hip arthroplasty through a posterolateral approach with partial capsulotomy and capsulorrhaphy, J Bone Joint Surg 83A:2, 2001.
- Kaplan SJ, Thomas WH, Poss R: Trochanteric advancement for recurrent dislocation after total hip arthroplasty, J Arthroplasty 2:119, 1987.
- Lewinnek GE, Lewis JL, Torr R, et al: Dislocations after total hip replacement arthroplasties, J Bone Joint Surg 60A:217, 1978.
- McLaren RH: Prosthetic hip angulation, Radiology 107:705, 1973.
- Osmani O, Malkani A: Posterior capsular repair following total hip arthroplasty: a modifi ed technique, Orthopedics 27:553, 2004.
- von Knoch M, Berry DJ, Harmsen S, et al: Late dislocation after total hip arthroplasty, J Bone Joint Surg 84A:1949, 2002.
- Weeden SH, Paprosky WG, Bowling JW: The early dislocation rate in primary total hip arthroplasty following the posterior approach with posterior soft-tissue repair, J Arthroplasty 18:709, 2003.
- Woo RY, Morrey BF: Dislocations after total hip arthroplasty, J Bone Joint Surg 64A:1295, 1982.
- Fracture Beals RK, Tower SS: Periprosthetic fractures of the femur, Clin Orthop Relat Res 327:238, 1996.
- Berry DJ: Periprosthetic fractures after major joint replacement: epidemiology: hip and knee, Orthop Clin North Am 30:183, 1999.
- Bethea JS III, De Andrade JR, Fleming LL, et al: Proximal femoral fractures following total hip arthroplasty, Clin Orthop Relat Res 170:95, 1982.
- Chao EYS, Coventry MB: Fracture of the femoral component after total hip replacement: an analysis of fi fty-eight cases, J Bone Joint Surg 63A:1078, 1981.
- Della Valle CJ, Momberger NG, Paprosky WG: Periprosthetic fractures of the acetabulum associated with a total hip arthroplasty, Instr Course Lect 52:281, 2003.
- Duncan CP, Masri BA: Fracture of the femur after hip replacement, Instr Course Lect 44:293, 1995.
- Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty, Instr Course Lect 52:309, 2003.
- Johannsson JE, McBroom R, Barrington TW, et al: Fracture of the ipsilateral femur in patients with total hip replacement, J Bone Joint Surg 63A:1435, 1981.
- Larsen E, Menck H, Rosenklint A: Fractures after hemialloplastic hip replacement, J Trauma 27:72, 1986.
- Lee S-R, Bostrom MPG: Periprosthetic fractures of the femur after total hip arthroplasty, Instr Course Lect 53:111, 2004.
- Mallory TH, Krause TJ, Vollen BK: Intraoperative femoral fractures associated with cementless THA, Orthopedics 12:231, 1989.
- McElfresh EC, Coventry MB: Femoral and pelvic fractures after total hip arthroplasty, J Bone Joint Surg 56A:483, 1974.
- Montijo H, Ebert FR, Lennox DA: Treatment of proximal femur fractures associated with total hip arthroplasty, J Arthroplasty 4:115, 1989.
- Zenni EJ Jr, Pomeroy DL, Caudle RJ: Ogden plate and other fi xations for fractures complicating femoral endoprostheses, Clin Orthop Relat Res 231:83, 1988.
- Trochanteric Nonunion and Migration Amstutz HC, Maki S: Complications of trochanteric osteotomy in total hip replacement, J Bone Joint Surg 60A:214, 1978.
- Bal BS, Maurer BT, Harris WH: Trochanteric union following revision total hip arthroplasty, J Arthroplasty 13:29, 1998.
- Chin KR, Brick GW: Reattachment of the migrated ununited greater trochanter after revision hip arthroplasty: the abductor slide technique, J Bone Joint Surg 82A:401, 2000.
- Hamadouche M, Zniber B, Dumaine V, et al: Reattachment of the ununited greater trochanter following total hip arthroplasty: surgical technique, J Bone Joint Surg 86A(suppl 1, pt 2):112, 2004.
- Hodgkinson JP, Shelley P, Wroblewski BM: Re-attachment of the un-united trochanter in Charnley low friction arthroplasty, J Bone Joint Surg 71B:523, 1989.
- McCarthy JC, Bono JV, Turner RH, et al: The outcome of trochanteric reattachment in revision total hip arthroplasty with a cable grip system, J Arthroplasty 14:810, 1999.
- Ritter MA, Gioe TJ, Steinger EA: Functional signifi cance of nonunion of the greater trochanter, Clin Orthop Relat Res 159:177, 1981.
- Stefanich RJ, Jabbur MT: Autogeneic cancellous bone grafting following transtrochanteric hip arthroplasty: an attempt to facilitate union of the greater trochanter, Clin Orthop Relat Res 228:141, 1988.
- Weber M, Berry DJ: Abductor avulsion after primary total hip arthroplasty: results of repair, J Arthroplasty 12:202, 1997.
- Osteolysis Benson ER, Christensen CP, Monesmith EA, et al: Particulate bone grafting of osteolytic femoral lesions around stable cementless stems. Presented at the Sixty-seventh Annual Meeting of the American Academy of Orthopaedic Surgeons, Orlando, Fla, March 15-19, 2000.
- Chiba J, Rubash HE, Kim KJ, et al: The characterization of cytokines in the interface tissue obtained from failed cementless total hip arthroplasty with and without femoral osteolysis, Clin Orthop Relat Res 300:304, 1994.
- Goldring SR, Schiller AL, Roelke M, et al: The synovial-like membrane at the bone-cement interface in loose total hip replacements and its proposed role in bone lysis, J Bone Joint Surg 65A:575, 1983.
- Hodgkinson JP, Shelley P, Wroblewski BM: The correlation between the roentgenographic appearance and operative fi ndings at the bone-cement junction of the socket in Charnley low friction arthroplasties, Clin Orthop Relat Res 228:105, 1988.
- Malik MH, Fisher N, Gray J, et al: Prediction of Charnley femoral stem aseptic loosening by early post-operative radiological features, Int Orthop 29:268, 2005.
- Maloney WJ, Herzwurm P, Paprosky W, et al: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement, J Bone Joint Surg 79A:1628, 1997.
- Maloney WJ, Smith RL, Schmalzried TP, et al: Isolation and characterization of wear particles generated in patients who have had failure of a hip arthroplasty without cement, J Bone Joint Surg 77A:1301, 1995.
- McKellop HA, Campbell P, Park SH, et al: The origin of submicron polyethylene wear debris in total hip arthroplasty, Clin Orthop Relat Res 311:3, 1995.
- Schmalzried TP, Jasty M, Harris WH: Periprosthetic bone loss in total hip arthroplasty: polyethylene wear debris and the concept of the effective joint space, J Bone Joint Surg 74A:849, 1992.
- Springer BD, Hanssen AD, Lewallen DG: Cementation of an acetabular liner into a well-fi xed acetabular shell during revision total hip arthroplasty, J Arthroplasty 18(suppl 1):126, 2003.
- Tanzer M, Maloney WJ, Jasty M, et al: The progression of femoral cortical osteolysis in association with total hip arthroplasty without cement, J Bone Joint Surg 74A:404, 1992.
- Loosening Barrack RL, Mulroy RD, Harris WH: Improved cementing techniques and femoral component loosening in young patients with hip arthroplasty: a 12-year radiographic review, J Bone Joint Surg 74B:385, 1992.
- Berry DJ, Harmsen WS, Ilstrup DM: The natural history of debonding of the femoral component from the cement and its effect on long-term survival of Charnley total hip replacements, J Bone Joint Surg 80A:715, 1998.
- Chambers IR, Fender D, McCaskie AW, et al: Radiological features predictive of aseptic loosening in cemented Charnley femoral stems, J Bone Joint Surg 83B:838, 2001.
- DeLee JG, Charnley J: Radiological demarcation of cemented sockets in total hip replacement, Clin Orthop Relat Res 121:20, 1976.
- Engh CA, Bobyn JD: The infl uence of stem size and extent of porous coating on femoral bone resorption after primary cementless hip arthroplasty, Clin Orthop Relat Res 231:7, 1988.
- Goodman S, Rubenstein J, Schatzker J, et al: Apparent changes in the alignment of the femoral component in hip arthroplasties associated with limb positioning, Clin Orthop Relat Res 221:242, 1987.
- Gruen TA, McNeice GM, Amstutz HC: “Modes of failure” of cemented stem-type femoral components: a radiographic analysis of loosening, Clin Orthop Relat Res 141:17, 1979.
- Hodgkinson JP, Shelley P, Wroblewski BM: The correlation between the roentgenographic appearance and operative fi ndings at the bone-cement junction of the socket in Charnley low friction arthroplasties, Clin Orthop Relat Res 228:105, 1988.
- Jasty M, Maloney WJ, Bragdon CR, et al: Histomorphological studies of the long-term skeletal responses to well fi xed cemented femoral components, J Bone Joint Surg 72A:1220, 1990.
- Leopold SS, Rosenberg AG, Ghatt RD, et al: Cementless acetabular revision, Clin Orthop Relat Res 369:179, 1999.
- Maloney WJ, Sychterz C, Bragdon C, et al: The Otto Aufranc Award. Skeletal response to well fi xed femoral components inserted with and without cement, Clin Orthop Relat Res 333:15, 1996.
- Mumme T, Reinartz P, Alfer J, et al: Diagnostic values of positron emission tomography versus triple-phase bone scan in hip arthroplasty loosening, Arch Orthop Trauma Surg 125:322, 2005.
- Poss R, Staehlin P, Larson M: Femoral expansion in total hip arthroplasty, J Arthroplasty 2:259, 1987.
- Salvati EA, Ghelman B, McLaren T, et al: Subtraction technique in arthrography for loosening of total hip replacement fi xed with radiopaque cement, Clin Orthop Relat Res 101:105, 1974.
- Schmalzried TP, Kwong LM, Jasty M, et al: The mechanism of loosening of cemented acetabular components in total hip arthroplasty: analysis of specimens retrieved at autopsy, Clin Orthop Relat Res 274:60, 1992.
- Revision Bargar WL, Murzic WJ, Taylor JK, et al: Management of bone loss in revision total hip arthroplasty using custom cementless femoral components, J Arthroplasty 8:245, 1993.
- Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty, J Bone Joint Surg 75A:66, 1993.
- Berry DJ, Sutherland CJ, Trousdale RT, et al: Bilobed oblong porous coated acetabular components in revision total hip arthroplasty, Clin Orthop Relat Res 371:154, 2000.
- Bierbaum BE: Acetabular revision arthroplasty. In Turner RH, Scheller AD Jr, eds: Revision total hip arthroplasty, New York, 1982, Grune & Stratton. Blackley HRL, Davis AM, Hutchison CR, et al: Proximal femoral allografts for reconstruction of bone stock in revision arthroplasty of the hip: a nine to fi fteen-year follow-up, J Bone Joint Surg 83A:346, 2001.
- Caillouette JT, Gorab RS, Klapper RC, et al: Revision arthroplasty facilitated by ultrasonic tool cement removal, I: in vitro evaluation, Orthop Rev 20:353, 1991.
- Caillouette JT, Gorab RS, Klapper RC, et al: Revision arthroplasty facilitated by ultrasonic tool cement removal, II: histologic analysis of endosteal bone after cement removal, Orthop Rev 20:435, 1991.
- Cameron HU: Proximal femoral osteotomy in diffi cult revision hip surgery: how to revise the unrevisable, Contemp Orthop 18:565, 1989.
- Cameron HU: Use of a distal trochanteric osteotomy in hip revision, Contemp Orthop 23:235, 1991.
- Capello WN: Revision techniques in hip and knee arthroplasty: impaction grafting plus cement for femoral component fi xation in revision hip arthroplasty, Orthopedics 17:878, 1994.
- Chandler HP, Clark J, Murphy S, et al: Reconstruction of major segmental loss of the proximal femur in revision total hip arthroplasty, Clin Orthop Relat Res 298:67, 1994.
- Chassin EP, Silverton CD, Berzins A, et al: Implant stability in revision total hip arthroplasty: allograft bone packing following extended proximal femoral osteotomy, J Arthroplasty 12:863, 1997.
- Collis D, Dubrul W: The removal of fractured prosthetic components from medullary cavities: a new technique, Contemp Orthop 8:61, 1984.
- D’Antonio J, McCarthy JC, Bargar WL, et al: Classifi cation of femoral abnormalities in total hip arthroplasty, Clin Orthop Relat Res 296:133, 1993.
- Della Valle CJ, Paprosky WG: Classifi cation and an algorithmic approach to the reconstruction of femoral defi ciency in revision total hip arthroplasty, J Bone Joint Surg 85A(suppl 4):1, 2003.
- Dennis DA, Dingman CA, Meglan DA, et al: Femoral cement removal in revision total hip arthroplasty: a biomechanical analysis, Clin Orthop Relat Res 220:142, 1987.
- de Thomasson E, Mazel C, Gagna G, et al: A simple technique to remove well-fi xed, all-polyethylene cemented acetabular component in revision hip arthroplasty, J Arthroplasty 16:538, 2001.
- Dohmae Y, Bechtold JE, Sherman RE, et al: Reduction in cement-bone interface shear strength between primary and revision arthroplasty, Clin Orthop Relat Res 236:214, 1988.
- Elting JJ, Mikhail EM, Zicat BA, et al: Preliminary report of impaction grafting for exchange femoral arthroplasty, Clin Orthop Relat Res 319:159, 1995.
- Emerson RH Jr, Head WC, Higgins LL: Clinical and radiographic analysis of the Mallory-Head femoral component in revision total hip arthroplasty: a minimum 8.8-year and average eleven-year follow-up study, J Bone Joint Surg 85A:1921, 2005.
- Emerson RH, Malinin TI, Cuellar AD, et al: Cortical allografts in the reconstruction of the femur in revision total hip arthroplasty: a basic science and clinical study, Clin Orthop Relat Res 285:35, 1992.
- Engh CA, Glassman AH, Griffi n WL, et al: Results of cementless revision for failed cemented total hip arthroplasty, Clin Orthop Relat Res 235:91, 1988.
- Estok D II, Harris WH: Long-term results of cemented femoral revision surgery using second-generation techniques: an average 11.7-year follow-up evaluation, Clin Orthop Relat Res 299:190, 1994.
- Fehring TK, Cohen B: Aspiration as a guide to sepsis in revision total hip arthroplasty, J Arthroplasty 11:543, 1996.
- Garbuz D, Morsi E, Gross AE: Revision of the acetabular component of total hip arthroplasty with a massive structural allograft, J Bone Joint Surg 78A:693, 1996.
- Gardiner R, Hozack WJ, Nelson C, et al: Revision total hip arthroplasty using ultrasonically driven tools: a clinical evaluation, J Arthroplasty 8:517, 1993.
- Gie GA, Linder L, Ling RSM, et al: Contained morselized allograft in revision total hip arthroplasty, Orthop Clin North Am 24:717, 1993.
- Gie GA, Linder L, Ling RSM, et al: Impacted cancellous allografts and cement for revision total hip arthroplasty, J Bone Joint Surg 75B:14, 1993.
- Glassman AH, Engh CA: The removal of porous-coated femoral hip stems, Clin Orthop Relat Res 285:164, 1992.
- Glassman AH, Engh CA, Bobyn JD: Proximal femoral osteotomy as an adjunct in cementless revision total hip arthroplasty, J Arthroplasty 2:47, 1987.
- Gross AE, Hutchison CR: Proximal femoral allografts for reconstruction of bone stock in revision hip arthroplasty, Orthopedics 21:999, 1998.
- Head WC, Mallory TH, Berklacich FM, et al: Extensile exposure of the hip for revision arthroplasty, J Arthroplasty 2:265, 1987.
- Head WC, Wagner RA, Emerson RH, et al: Revision total hip arthroplasty in the defi cient femur with a proximal loadbearing prosthesis, Clin Orthop Relat Res 298:119, 1994.
- Hellman EJ, Capello WN, Feinberg JR: Nonunion of extended trochanteric osteotomies in impaction grafting femoral revisions, J Arthroplasty 13:945, 1998.
- Hultmark P, Kärrholm J, Strömberg C, et al: Cemented fi rst-time revisions of the femoral component: prospective 7 to 13 years’ follow-up using second-generation and third-generation technique, J Arthroplasty 15:551, 2000.
- Jando VT, Greidanus NV, Masri BA, et al: Trochanteric osteotomies in revision total hip arthroplasty: contemporary techniques and results, Instr Course Lect 54:143, 2005.
- Katz RP, Callaghan JJ, Sullivan PM, et al: Results of cemented femoral revision total hip arthroplasty using improved cementing techniques, Clin Orthop Relat Res 319:178, 1995.
- Kim YH, Franks DJ: Cementless revision of cemented stem failures associated with massive femoral bone loss: a technical note, Orthop Rev 21:375, 1992.
- Kim YY, Ko CU, Lee SW, Kwak BM: Replacement arthroplasty using the Charnley prosthesis in old tuberculosis of the hip, Int Orthop 3:81, 1979.
- Klapper RC, Caillouette JT: The use of ultrasonic tools in revision arthroplasty procedures, Contemp Orthop 20:273, 1990.
- Klein AH, Rubash HE: Femoral windows in revision total hip arthroplasty, Clin Orthop Relat Res 291:164, 1993.
- Kurtz S, Mowat F, Ong K, et al: Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002, J Bone Joint Surg 87A:1487, 2005.
- LaPorte DM, Mont MA, Pierre-Jacques H, et al: Technique for acetabular liner revision in a nonmodular metal-backed component, J Arthroplasty 13:348, 1998.
- Lawrence JM, Engh CA, Macalino GE: Revision total hip arthroplasty: long-term results without cement, Orthop Clin North Am 24:635, 1993.
- Mallory TH: Preparation of the proximal femur in cementless total hip revision, Clin Orthop Relat Res 235:47, 1988.
- McCarthy JC, Mattingly D, Turner RH, et al: Revision of the defi cient femur with a modular femoral component, Orthop Trans 17:996, 1993.
- McGann WA, Welch RB, Picetti GD III: Acetabular preparation in cementless revision total hip arthroplasty, Clin Orthop Relat Res 235:35, 1988.
- Mikhail WEM, Weidenhielm LRA, Wretenberg P, et al: Femoral bone regeneration subsequent to impaction grafting during hip revision: histologic analysis of a human biopsy specimen, J Arthroplasty 14:849, 1999.
- Moreland JR, Marder R, Anspach WE Jr: The window technique for the removal of broken femoral stems in total hip replacement, Clin Orthop Relat Res 212:245, 1986.
- Morsi E, Garbuz D, Gross AE: Revision total hip arthroplasty with shelf bulk allografts: a long-term follow-up study, J Arthroplasty 11:86, 1996.
- Nelissen RGHH, Bauer TW, Weidenhielm RA, et al: Revision hip arthroplasty with the use of cement and impaction grafting, J Bone Joint Surg 77A:412, 1995.
- Padgett DE, Kull L, Rosenberg A, et al: Revision of the acetabular component without cement after total hip arthroplasty, J Bone Joint Surg 75A:663, 1993.
- Pak JH, Paprosky WG, Jablonsky WS, et al: Femoral strut allografts in cementless revision total hip arthroplasty, Clin Orthop Relat Res 295:172, 1993.
- Paprosky WG, Greidanus NV, Antoniou J: Minimum of 10-year results of extensively porous-coated stems in revision hip arthroplasty, Clin Orthop Relat Res 369:230, 1999.
- Paprosky WG, Jablosky W, Magnus RE: Cementless femoral revision in the presence of severe proximal femoral bone loss using diaphyseal fi xation, Orthop Trans 17:965, 1993.
- Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: acetabular technique, Clin Orthop Relat Res 298:147, 1994.
- Paprosky WG, Perona PG, Lawrence JM: Acetabular defect classifi cation on surgical reconstruction in revision arthroplasty, J Arthroplasty 9:33, 1994.
- Peters CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: subsidence of proximally porous-coated femoral components, J Bone Joint Surg 77A:1217, 1995.
- Pollock FH, Whiteside LA: The fate of massive allografts in total hip acetabular revision surgery, J Arthroplasty 7:271, 1992.
- Robinson DE, Lee MB, Smith EJ, et al: Femoral impaction grafting in revision hip arthroplasty with irradiated bone, J Arthroplasty 17:834, 2002.
- Rubash HE, Harris WH: Revision of nonseptic, loose, cemented femoral components using modern cementing techniques, J Arthroplasty 3:241, 1988.
- Schatzker J, Woong MK: Acetabular revision: the role of rings and cages, Clin Orthop Relat Res 369:187, 1999.
- Schurman DJ, Maloney WJ: Segmental cement extraction at revision total hip arthroplasty, Clin Orthop Relat Res 285:158, 1992.
- Springer BD, Berry DJ, Cabanela ME, et al: Early postoperative transverse pelvic fracture: a new complication related to revision arthroplasty with an uncemented cup, J Bone Joint Surg 87A:2626, 2005.
- Stiehl JB: Acetabular allograft reconstruction in total hip arthroplasty, I: current concepts in biomechanics, Orthop Rev 20:339, 1991.
- Stiehl JB: Acetabular allograft reconstruction in total hip arthroplasty, II: surgical approach and aftercare, Orthop Rev 20:425, 1991.
- Turner RH, Mattingly DA, Scheller A: Femoral revision total hip arthroplasty using a long-stem femoral component, J Arthroplasty 2:247, 1987.
- Ullmark G, Hallin G, Nilsson O: Impacted corticocancellous allografts and cement for revision of the femur component in total hip arthroplasty, J Arthroplasty 17:140, 2002.
- Winter E, Piert M, Volkmann R, et al: Allogeneic cancellous bone graft and a Burch-Schneider ring for acetabular reconstruction in revision hip arthroplasty, J Bone Joint Surg 83A:862, 2001.
- Wroblewski BM: A method of management of the fractured stem in total hip replacement, Clin Orthop Relat Res 141:71, 1979.
- Wuh HCK, Chin AK, Moll FH, et al: A new technique of cement extraction for revision total hip arthroplasty, Orthop Trans 15:60, 1991 (abstract). Younger TI, Bradford MS, Magnus RE, et al: Extended proximal femoral osteotomy: a new technique for femoral revision arthroplasty, J Arthroplasty 10:329, 1995.
- Younger TI, Bradford MS, Paprosky WG: Removal of a wellfi xed cementless femoral component with an extended proximal femoral osteotomy, Contemp Orthop 30:375, 1995.
- Resurfacing Amstutz HC, Graff-Radford A, Gruen TA, et al: THARIES surface replacements: a review of the fi rst 100 cases, Clin Orthop Relat Res 134:87, 1978.
- Beaulé PE, Amstutz HC, LeDuff M, et al: Surface arthroplasty for osteonecrosis of the hip: hemiresurfacing versus metal-onmetal hybrid resurfacing, J Arthroplasty 19:54, 2004.
- Beaulé PE, Antoniades J: Patient selection and surgical technique for surface arthroplasty of the hip, Orthop Clin North Am 36:177, 2005.
- Buechel FF, Drucker D, Jasty M, et al: Osteolysis around uncemented acetabular components of cobalt-chrome surface replacement hip arthroplasty, Clin Orthop Relat Res 298:202, 1994.
- Capello WN, Ireland PH, Trammell TR, et al: Conservative total hip arthroplasty: a procedure to conserve bone stock, Clin Orthop Relat Res 134:59, 1978.
- Daniel J, Pynsent PB, McMinn DJ: Metal-on-metal resurfacing of the hip in patients under the age of 55 years with osteoarthritis, J Bone Joint Surg 86B:177, 2004.
- Eftekhar NS, Smith DM, Henry JH, et al: Revision arthroplasty using Charnley low-friction arthroplasty technic: with reference to specifi cs of technic and comparison of results with primary low friction arthroplasty, Clin Orthop Relat Res 95:48, 1973.
- Engh CA: Hip arthroplasty with a Moore prosthesis with porous coating: a fi ve-year study, Clin Orthop Relat Res 176:52, 1983.
- Freeman MAR: Some anatomical and mechanical considerations relevant to the surface replacement of the femoral head, Clin Orthop Relat Res 134:19, 1978.
- Grigoris P, Roberts P, Panousis K, et al: The evolution of hip resurfacing arthroplasty, Orthop Clin North Am 36:125, 2005.
- Howie DW, Cornish BL, Vernon-Roberts B: The viability of the femoral head after resurfacing hip arthroplasty in humans, Clin Orthop Relat Res 291:171, 1993.
- Hungerford MW, Mont MA, Scott R, et al: Surface replacement hemiarthroplasty for the treatment of osteonecrosis of the femoral head, J Bone Joint Surg 80A:1656, 1998.
- Itayem R, Arndt A, Nistor L, et al: Stability of the Birmingham hip resurfacing arthroplasty at two years: a radiosterophotogrammatric analysis study, J Bone Joint Surg 87B:158, 2005.
- Little CP, Ruiz AL, Harding IJ, et al: Osteonecrosis in retrieved femoral heads after failed resurfacing arthroplasty of the hip, J Bone Joint Surg 87B:320, 2005.
- Loughead JM, Chesney D, Holland JP, et al: Comparison of offset in Birmingham hip resurfacing and hybrid total hip arthroplasty, J Bone Joint Surg 87B:163, 2005.
- Schmalzried TP, Fowble VA, Ure KJ, et al: Metal on metal surface replacement of the hip: technique, fi xation, and early results, Clin Orthop Relat Res 329(suppl):106, 1996.
- Shimmin AJ, Back D: Femoral neck fractures following Birmingham hip resurfacing: a national review of 50 cases, J Bone Joint Surg 87B:463, 2005.
- Shimmin AJ, Bare J, Back DL: Complications associated with hip resurfacing arthroplasty, Orthop Clin North Am 36:187, 2005.
- Siguier M, Judet T, Siguier T, et al: Preliminary results of partial surface replacement of the femoral head in osteonecrosis, J Arthroplasty 14:45, 1999.
- Silva M, Lee KH, Heisel C, et al: The biomechanical results of total hip resurfacing arthroplasty, J Bone Joint Surg 86A:40, 2004.
- Tanaka S: Surface replacement of the hip joint, Clin Orthop Relat Res 134:75, 1978.
- Tooke SM, Amstutz HC, Delaunay C: Hemiresurfacing for femoral head osteonecrosis, J Arthroplasty 2:125, 1987.
- Treacy RBC, McBryde CW, Pynsent PB: Birmingham hip resurfacing arthroplasty: a minimum follow-up of fi ve years, J Bone Joint Surg 87B:167, 2005.
