Ligament: Your Guide to Structure, Function, Injury, and Healing
Introduction & Epidemiology
Ligaments are critical components of the musculoskeletal system, functioning as essential stabilizers of synovial joints. Comprising dense connective tissue, they bridge bones, articulate joint kinematics, and provide crucial proprioceptive feedback. Injuries to ligaments are exceedingly common, spanning a wide spectrum from minor sprains to complete ruptures, often necessitating intricate surgical management and prolonged rehabilitation.
Epidemiologically, ligamentous injuries represent a significant burden on healthcare systems and individual functional capacity. The knee, ankle, and shoulder are particularly susceptible. Anterior cruciate ligament (ACL) ruptures, for instance, occur at an incidence of 30-78 per 100,000 person-years, with a disproportionately high prevalence in athletes, particularly in pivoting and contact sports. Medial collateral ligament (MCL) sprains are frequently encountered, often concurrently with ACL tears. Ankle sprains, predominantly involving the lateral collateral ligament complex (anterior talofibular ligament - ATFL, calcaneofibular ligament - CFL), are among the most common musculoskeletal injuries, affecting millions annually. These injuries often lead to chronic instability, functional limitations, and an increased risk of post-traumatic osteoarthritis if not appropriately managed. Understanding the intricate biological and biomechanical properties of ligaments is paramount for effective diagnosis, surgical intervention, and rehabilitation strategies.
Surgical Anatomy & Biomechanics
-
Characteristics
- Originates and inserts on bone, primarily via Sharpey's fibers.
- Stabilizes joints, preventing excessive translation, rotation, and displacement of articulating bones.
- Contains mechanoreceptors (Ruffini, Pacinian, Golgi-Mazzoni corpuscles) and free nerve endings that facilitate joint proprioception, kinesthesia, and nociception.
- Displays viscoelastic behavior, allowing for energy absorption and controlled deformation under load.
-
Structure and Composition
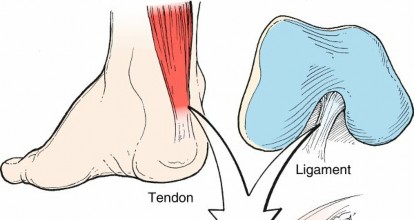
Ligaments are complex hierarchical structures.

FIG. 1.44 Tendon and ligament architecture.
From Brinker MR, Miller MD: Fundamentals of orthopaedics,
Philadelphia, 1999, Saunders, p 15.-
Composition :
- Water : 60%–70% of total weight, contributing to viscoelastic properties.
-
Dry Weight Components
:
-
Collagen
: Approximately 80% of dry weight.
- Predominantly type I collagen (90%), providing tensile strength. Types III, V, VI, XI, and XIV collagen are also present in smaller quantities.
- Collagen type I concentration is highest at the origin and insertion sites (entheses), while type III collagen is more prevalent in the midsubstance and plays a role in early healing and scar formation.
- Collagen fibers exhibit a characteristic crimp pattern, allowing initial elongation under low loads without fiber damage (toe region of the stress-strain curve).
- Elastin : Approximately 1% of dry weight, providing elasticity and recoil. More prominent in certain ligaments like the ligamentum flavum.
- Proteoglycans (PGs) : Approximately 1% of dry weight, including decorin, biglycan, and aggrecan. PGs contribute to water retention, osmotic swelling pressure, and influence the viscoelastic behavior and collagen fibril organization.
-
Collagen
: Approximately 80% of dry weight.
-
Cells :
- Fibroblasts (Ligamentocytes) : The primary cell type, oriented longitudinally parallel to collagen fibers. These cells are responsible for synthesizing and maintaining the extracellular matrix (ECM), including collagen, elastin, and proteoglycans. Ligamentocytes have a lower metabolic rate compared to tenocytes.
-
Extracellular Matrix (ECM) Architecture :
- Collagen fibrils are organized into fibers, which then coalesce into fascicles, creating a hierarchical structure. This organization provides robust tensile strength along the long axis of the ligament.
- Ligaments can be broadly classified as capsular (e.g., glenohumeral ligaments), which are thickenings of the joint capsule, or extracapsular (e.g., LCL), which lie outside the capsule, and intra-articular (e.g., ACL), traversing the joint space. The vascular supply and healing potential often differ based on this classification.
-
Epiligament :
- Similar in structure to epitenon in tendons, the epiligament is a thin, loose connective tissue sheath surrounding the ligament. It carries the neurovascular and lymphatic supply, facilitating nutrient delivery and waste removal. The vascularity of ligaments is generally lower than that of tendons, particularly in the midsubstance of intra-articular ligaments.
-
Entheses (Bone-Ligament Interface) :
- Ligaments transition into bone through specialized structures called entheses. These can be direct or indirect.
- Direct Enthesis : Characterized by four distinct zones: ligament, unmineralized fibrocartilage, mineralized fibrocartilage, and bone. This gradual transition helps dissipate stress and prevents abrupt failure at the interface.
- Indirect Enthesis : Collagen fibers insert directly into the periosteum and outer cortical bone via Sharpey's fibers.
-
-
Biomechanics
-
Viscoelasticity
: Ligaments exhibit time- and load-dependent mechanical properties.
- Stress-Strain Curve : Characterized by a "toe region" (initial elongation due to collagen crimp), a "linear region" (elastic deformation of collagen fibers), a "yield point" (microscopic failure), and a "failure point" (macroscopic rupture).
- Creep : Continued deformation under constant load over time.
- Stress Relaxation : Decrease in stress over time when held at a constant length.
- Hysteresis : Energy dissipation observed during cyclic loading and unloading, contributing to shock absorption.
- Load-to-Failure : The ultimate tensile strength of ligaments varies significantly by anatomical location, age, and individual factors. This property dictates the load required to cause rupture.
- Joint Stability : Ligaments are primary static stabilizers, limiting excessive joint motion. They work in conjunction with dynamic stabilizers (muscles and tendons) to provide overall joint stability. Ligament injury disrupts this intricate balance, leading to joint laxity and functional instability.
- Proprioception : The mechanoreceptors within ligaments provide afferent feedback to the central nervous system, contributing to joint position sense and motor control. Injury to these structures can impair proprioception, increasing the risk of recurrent injury.
-
Viscoelasticity
: Ligaments exhibit time- and load-dependent mechanical properties.
Indications & Contraindications
The decision-making process for operative versus non-operative management of ligamentous injuries is complex and multifactorial, considering patient factors, injury characteristics, and functional goals.
Indications for Surgical Intervention
- Acute Complete Ruptures with Instability : Particularly in high-demand patients or where non-operative management has a high failure rate (e.g., ACL rupture, Grade III MCL in multi-ligament knee injuries, acute ATFL rupture in professional athletes).
- Chronic Instability : Symptomatic instability causing recurrent giving way, pain, or functional limitations that impact activities of daily living or sport performance, despite adequate conservative management.
- Associated Injuries : Concomitant injuries (e.g., meniscal tears, chondral damage, osteochondral fractures, or other ligamentous injuries) that necessitate surgical intervention and where addressing the ligamentous injury simultaneously is prudent.
- Specific Anatomical Lesions : Such as a Stener lesion in the ulnar collateral ligament of the thumb, where interposition of the adductor aponeurosis prevents healing.
- Pediatric Patients : With epiphyseal avulsion fractures or where physeal-sparing techniques are employed to restore stability and prevent growth disturbance.
- Failure of Non-Operative Management : Documented persistent symptomatic instability or functional deficit after a structured and compliant non-operative treatment program.
Indications for Non-Operative Management
- Partial Tears or Low-Grade Sprains : Grade I or II sprains where structural integrity is largely maintained (e.g., most Grade I/II MCL sprains, low-grade ATFL sprains).
- Low Functional Demands : Patients with sedentary lifestyles or those not intending to return to high-impact activities.
- Concomitant Medical Comorbidities : Conditions that significantly increase surgical risk (e.g., severe cardiovascular disease, uncontrolled diabetes, active infection).
- Advanced Age : Where surgical risks outweigh potential benefits, especially in the absence of debilitating instability.
- Good Functional Stability : Despite imaging evidence of ligamentous injury, the patient demonstrates adequate functional stability and does not experience symptomatic instability.
- Patient Preference : After thorough counseling on risks, benefits, and alternatives, the patient may opt for non-operative management.
Contraindications for Surgical Intervention
-
Absolute Contraindications
:
- Active systemic or local joint infection.
- Uncontrolled severe medical comorbidities precluding safe anesthesia and surgery.
- Non-ambulatory status where restoration of ligamentous integrity offers no functional benefit.
-
Relative Contraindications
:
- Advanced osteoarthritis (consider osteotomy or arthroplasty as primary treatment).
- Severe generalized ligamentous laxity.
- Poor bone quality (osteoporosis) compromising fixation.
- Severe soft tissue compromise or extensive scarring around the joint.
- Unrealistic patient expectations or non-compliance with post-operative rehabilitation.
Operative vs. Non-Operative Indications
| Factor | Operative Management | Non-Operative Management |
|---|---|---|
| Injury Grade/Type | Complete ruptures (Grade III), certain acute Grade III (e.g., ACL) | Partial tears (Grade I/II), most Grade I/II (e.g., MCL, ATFL) |
| Functional Demand | High-demand athletes, manual laborers | Low-demand, sedentary individuals |
| Symptom Profile | Debilitating instability, recurrent giving way, pain | Mild/moderate pain, stable with bracing/therapy |
| Associated Injuries | Multi-ligament injuries, meniscal tears, chondral defects | Isolated low-grade ligament injury |
| Failure of Conservative Rx | Documented failure after adequate PT/bracing | Initial injury presentation, first-line for low-grade injury |
| Specific Pathology | Stener lesion, physeal avulsions (in children) | N/A |
| Patient Factors | Young, healthy, motivated, good bone quality | Elderly, significant comorbidities, poor bone quality (relative contraindication for surgery) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful ligamentous surgery, minimizing complications and optimizing outcomes.
Pre-Operative Planning
-
Comprehensive Patient Evaluation :
- History : Detailed mechanism of injury, symptom duration, previous treatments, functional limitations, activity level, and patient goals.
- Physical Examination : Specific ligamentous stress tests (e.g., Lachman, anterior drawer, varus/valgus stress, pivot shift, Talar tilt, external rotation stress), range of motion, neurovascular status, and assessment for associated injuries (meniscus, cartilage, other ligaments).
-
Imaging Review
:
- Radiographs : AP, lateral, and oblique views to rule out fractures, assess joint alignment, and identify chronic changes (e.g., osteophytes). Stress radiographs (e.g., varus/valgus stress for collateral ligaments, gravity stress views for syndesmosis) provide objective measures of instability.
- MRI : The gold standard for soft tissue assessment, confirming ligament integrity, tear patterns, and identifying associated meniscal, chondral, and bone bruise injuries. Crucial for surgical planning.
- CT Scan : May be used for complex avulsion fractures, assessment of rotational malalignment, or pre-operative 3D planning for multi-ligament reconstructions.
-
Surgical Strategy Development :
-
Graft Choice (for reconstruction)
:
- Autograft : Patellar tendon (BTB), hamstrings (semitendinosus/gracilis), quadriceps tendon. Advantages: no disease transmission, good incorporation. Disadvantages: donor site morbidity.
- Allograft : Cadaveric tissue (e.g., tibialis anterior, Achilles). Advantages: no donor site morbidity, larger graft options. Disadvantages: slower incorporation, potential for disease transmission (rare), immunogenicity, higher cost.
- Synthetic Grafts : Limited use in primary repairs/reconstructions due to long-term failure rates and complications, but may be considered for augmentation or in revision settings.
- Surgical Approach : Arthroscopic, open, or combined. Dictated by the specific ligament, associated injuries, and surgeon preference.
- Fixation Method : Interference screws (bioabsorbable or metallic), cortical buttons, suspensory fixation devices, staples, suture anchors, post-and-tie. Choice depends on graft type, bone quality, and desired biomechanical properties.
- Associated Procedures : Plan for meniscal repair/meniscectomy, chondroplasty, microfracture, osteotomy, or addressing other ligamentous injuries.
- Pre-operative Rehabilitation : Pre-habilitation to optimize range of motion, strength, and reduce swelling prior to surgery may improve post-operative outcomes.
-
Graft Choice (for reconstruction)
:
-
Informed Consent : Thorough discussion with the patient regarding the diagnosis, proposed surgical procedure, graft choice, potential risks (infection, nerve/vascular injury, DVT/PE, persistent instability, stiffness, pain, graft failure, donor site morbidity), expected benefits, alternative treatments, and post-operative rehabilitation requirements.
Patient Positioning
Patient positioning must allow optimal surgical exposure, visualization, graft harvest (if applicable), and maintain patient safety throughout the procedure.
-
Supine Position :
- Knee (e.g., ACL, MCL) : Supine on the operating table. A leg holder or knee bolster is typically used to allow full flexion and extension. A lateral post is often employed to apply valgus stress for medial compartment access. Tourniquet on the proximal thigh. Well-padded throughout, especially common peroneal nerve at the fibular head.
- Ankle (e.g., ATFL, Syndesmosis) : Supine, often with a bump under the ipsilateral hip to internally rotate the limb. Tourniquet on the proximal thigh or calf.
-
Lateral Decubitus Position :
- Shoulder (e.g., AC Joint, Coracoclavicular Ligaments) : Lateral decubitus with the affected arm draped free and suspended in traction (e.g., 5-10 lbs) via a sterile traction tower. Axillary roll for nerve protection, careful head and neck positioning.
-
Beach Chair Position :
- Shoulder : Patient is semi-sitting. Allows for easier conversion to open if needed and better access to posterior structures. Requires careful blood pressure monitoring to prevent cerebral hypoperfusion, especially during interscalene block.
General Positioning Principles
:
*
Padding
: All pressure points, bony prominences, and neurovascular bundles (e.g., ulnar nerve at elbow, common peroneal nerve at fibular head, brachial plexus in shoulder) must be meticulously padded.
*
Tourniquet
: Applied proximally, inflated to appropriate pressure (e.g., 250-300 mmHg) to maintain a bloodless field. Duration monitored to minimize ischemia-reperfusion injury.
*
Sterile Prep and Drape
: Wide sterile field, often extending from the hip to the toes for knee/ankle, or neck to iliac crest for shoulder.
Detailed Surgical Approach / Technique
The specific surgical technique for ligament repair or reconstruction is highly dependent on the anatomical location, type of injury, and surgeon preference. However, general principles guide all procedures.
General Principles of Ligament Surgery
- Anatomical Understanding : A thorough understanding of the specific ligament's origin, insertion, trajectory, and biomechanical function is paramount. Anatomic reconstruction aims to restore normal kinematics.
- Minimally Invasive Approach : Utilizing arthroscopy or small open incisions to minimize soft tissue dissection, reduce post-operative pain, and potentially accelerate recovery, while maintaining adequate visualization and access.
- Preservation of Native Structures : Whenever possible, remnants of the native ligament are preserved to allow for biological augmentation and potentially improved proprioception.
- Isometric Placement : For reconstructions, achieving isometric graft placement (minimal length change throughout the range of motion) is crucial to prevent graft impingement, elongation, or overtensioning.
- Robust Fixation : Secure fixation of the graft to bone or the ligament ends to their attachments is essential for initial stability and to allow for biological healing and graft incorporation.
- Avoidance of Neurovascular Structures : Meticulous dissection and careful use of instruments are critical to protect adjacent nerves and vessels.
Detailed Surgical Approach (Illustrative Example: ACL Reconstruction)
This example highlights common steps in ligament reconstruction.
-
Pre-operative Preparation :
- Patient positioned supine on the operating table. Leg holder and lateral post applied. Tourniquet inflated.
- Thorough sterile prep and drape of the entire lower limb from mid-thigh to foot.
- Diagnostic arthroscopy performed via anteromedial (AM) and anterolateral (AL) portals to assess the joint, confirm injury, and address any associated pathology (meniscal tears, chondral lesions). Debride remaining ACL stump if necessary, but preserve viable tissue.
-
Graft Harvest (Autograft Example: Hamstring Tendon) :
- A ~2-3 cm oblique incision is made over the pes anserinus at the anteromedial aspect of the proximal tibia.
- Dissection through subcutaneous tissue to expose the sartorius fascia.
- The sartorius fascia is incised, and the semitendinosus and gracilis tendons are identified and harvested using a specialized tendon stripper.
- Careful hemostasis and wound closure after graft harvest.
- The harvested tendons are prepared on a back table, folded into a quadruple or quintuple bundle, and whip-stitched at the ends for robust fixation. Graft diameter is measured.
-
Femoral Tunnel Creation :
- The AM portal is commonly used for femoral tunnel drilling. A guide pin is inserted into the anatomical footprint of the ACL on the lateral femoral condyle. The ideal position is typically between the AM and PL bundles.
- Careful attention to the angle and depth to avoid posterior wall blowout and ensure appropriate graft length.
- A cannulated drill bit is advanced over the guide pin to create the femoral tunnel. The tunnel length should accommodate the graft and fixation device.
-
Tibial Tunnel Creation :
- A tibial guide is used to place a guide pin from the anteromedial tibia into the anatomical footprint of the ACL on the tibial plateau. The ideal position avoids impingement in extension and is slightly posterior to the anterior horn of the lateral meniscus.
- Over-drilling with a cannulated drill bit creates the tibial tunnel.
-
Graft Passage :
- A suture loop is passed through both the femoral and tibial tunnels.
- The prepared graft is attached to the suture loop and gently pulled through the tunnels, ensuring it is not twisted or kinked.
-
Graft Tensioning and Fixation :
- Femoral Fixation : Typically achieved first. Cortical suspensory fixation devices (e.g., Endobutton, adjustable loop devices) are passed through the femoral tunnel and flipped on the lateral cortex. Interference screws (metallic or bioabsorbable) can also be used.
- Tibial Fixation : The knee is typically cycled several times to "pre-tension" the graft. The graft is then tensioned with the knee in 20-30 degrees of flexion (to prevent graft overtensioning in extension) and fixed with an interference screw, post-and-tie, or staple. Final tensioning can be adjusted to achieve appropriate stability without overtightening.
-
Closure :
- Arthroscopic portals are closed with a single suture or sterile strips.
- Graft harvest site and other small incisions are closed in layers.
- Sterile dressing and knee brace applied.
Internervous Planes (for Open Ligament Repair/Reconstruction)
In open procedures, understanding internervous planes is crucial to minimize muscle damage and facilitate recovery.
*
Knee (Medial Approach for MCL)
: The medial approach to the knee, often utilized for MCL repair or reconstruction, involves dissecting between the sartorius (innervated by femoral nerve) and the gracilis/semitendinosus (innervated by obturator/tibial nerves). This plane allows access to the superficial and deep MCL without significant muscle transection.
*
Ankle (Lateral Approach for ATFL)
: The lateral approach to the ankle for ATFL repair (e.g., Brostrom-Gould) typically involves an incision anterior to the fibula, dissecting through skin and subcutaneous tissue to expose the retinacular structures. The plane is often between the peroneal tendons posteriorly and the extensor digitorum longus anteriorly, minimizing nerve and muscle injury. The superficial peroneal nerve branches must be identified and protected.
Complications & Management
Despite advancements in surgical techniques, ligament repair and reconstruction procedures are associated with potential complications. Thorough understanding and prompt management are crucial for optimal outcomes.
General Surgical Complications
-
Infection
: Superficial or deep surgical site infection. Incidence: 0.5-2%.
- Management : Antibiotics, incision and drainage, debridement. For deep infections involving implants, hardware removal may be necessary.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE)
: Thromboembolic events are a risk following lower extremity surgery. Incidence: DVT 0.5-10%, PE <1%.
- Management : Prophylactic anticoagulation (chemical or mechanical), early mobilization. Treatment involves therapeutic anticoagulation.
-
Neurovascular Injury
: Damage to adjacent nerves (e.g., common peroneal nerve in knee surgery, superficial peroneal nerve in ankle surgery, saphenous nerve in hamstring harvest) or vessels. Incidence: <1%.
- Management : Meticulous surgical technique, anatomical knowledge. Post-op nerve injury may require observation, neurolysis, or repair. Vascular injury requires immediate repair.
- Anesthesia-Related Complications : Risks associated with general or regional anesthesia.
Ligament-Specific Complications
-
Persistent Instability / Rerupture
: Failure to restore stability or subsequent re-injury of the reconstructed ligament. Incidence: 5-10% for ACL reconstruction.
- Etiology : Non-anatomical graft placement, improper tensioning, graft failure (early necrosis, late elongation), inadequate fixation, premature return to activity, recurrent trauma.
- Salvage Strategies : Revision surgery with careful analysis of failure mechanism, often using different graft source, altered tunnel placement, or adjunctive procedures (e.g., osteotomy).
-
Stiffness / Arthrofibrosis
: Restricted range of motion due to excessive scar tissue formation within the joint. Incidence: 2-5%.
- Etiology : Delayed or inadequate rehabilitation, excessive inflammatory response, graft impingement, early surgery after acute injury with significant effusion.
- Salvage Strategies : Aggressive physical therapy, manipulation under anesthesia, arthroscopic lysis of adhesions (LOA), or even open arthrolysis in severe cases.
-
Pain
: Chronic pain at the joint, donor site, or related to hardware.
- Etiology : Neuroma (e.g., saphenous nerve at hamstring harvest), hardware prominence, persistent inflammation, early osteoarthritis.
- Salvage Strategies : Analgesics, physical therapy, nerve blocks, hardware removal (if symptomatic), targeted injections.
-
Graft-Specific Complications
:
-
Autograft Donor Site Morbidity
:
- Patellar Tendon (BTB) : Anterior knee pain, patellar fracture (rare), patellar tendon rupture (rare), patellar tendinopathy, quadriceps weakness.
- Hamstrings : Medial knee pain, hamstring weakness, saphenous nerve dysesthesia.
- Quadriceps Tendon : Anterior knee pain, quadriceps weakness.
- Allograft Complications : Slower graft incorporation, theoretical risk of disease transmission (extremely low with current processing), immunologic reaction (rare).
- Synthetic Grafts : High rates of synovitis, infection, breakage, and early failure leading to limited use.
-
Autograft Donor Site Morbidity
:
-
Hardware-Related Issues
: Prominence, migration, breakage, or loosening of fixation devices.
- Etiology : Poor bone quality, improper placement, excessive loading.
- Salvage Strategies : Hardware removal if symptomatic, revision fixation.
-
Growth Plate Injury (in pediatric patients)
: Risk of growth arrest or deformity with traditional transphyseal tunnels.
- Etiology : Damage to the physis during tunnel drilling.
- Salvage Strategies : Physeal-sparing techniques (epiphyseal, over-the-top, or all-epiphyseal), guided growth procedures if deformity develops.
-
Cyclops Lesion
: Intra-articular fibrous nodule often anterior to the ACL graft, causing mechanical impingement and extension loss.
- Etiology : Scar tissue formation from remnants of the native ACL or surrounding synovium.
- Salvage Strategies : Arthroscopic debridement.
Common Complications and Management
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Persistent Instability/Rerupture | 5-10% (ACL) | Revision surgery (graft change, tunnel reposition), adjunctive procedures (osteotomy), bracing, physical therapy. |
| Arthrofibrosis/Stiffness | 2-5% (ACL) | Aggressive physical therapy, manipulation under anesthesia, arthroscopic lysis of adhesions, open arthrolysis. |
| Infection | 0.5-2% | Antibiotics, incision and drainage, debridement, hardware removal (if deep/persistent). |
| Donor Site Pain | 5-15% (BTB/Hamstring) | Physical therapy, analgesics, nerve blocks, hardware removal (if applicable). |
| Nerve Injury | <1% | Observation, neurolysis, nerve repair. |
| DVT/PE | DVT: 0.5-10%, PE: <1% | Therapeutic anticoagulation, filter placement (rare). |
| Hardware Prominence | Variable | Hardware removal if symptomatic. |
| Cyclops Lesion | 2-5% | Arthroscopic debridement. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical determinant of functional outcomes following ligament surgery. Protocols are structured to protect the repair/reconstruction while progressively restoring range of motion (ROM), strength, proprioception, and functional capacity. These are generalized principles; specific protocols vary based on the ligament, surgical technique, and surgeon preference.
Core Principles
- Protection : Safeguarding the healing ligament or graft from excessive stress during the initial healing phases.
- Gradual Restoration of ROM : Achieving full, pain-free motion while respecting tissue healing constraints.
- Progressive Strengthening : Restoring muscle strength and endurance around the joint.
- Neuromuscular Control and Proprioception : Re-establishing the afferent and efferent pathways for dynamic stability.
- Functional Progression : Gradually advancing activities from basic movements to sport-specific drills.
- Criteria-Based Advancement : Progressing through phases based on objective milestones rather than strict timelines.
Phases of Rehabilitation (Example: ACL Reconstruction)
Phase I: Protection & Early Motion (Weeks 0-6)
- Goals : Control pain and swelling, achieve full knee extension, protect the graft, initiate muscle activation.
- Bracing : Often a hinged knee brace locked in extension for ambulation, gradually unlocked for ROM exercises. Weight-bearing status is typically protected (crutches) initially, progressing to full weight-bearing as tolerated.
-
Exercises
:
- ROM : Passive and active-assisted knee extension (crucial for preventing arthrofibrosis), gentle flexion (e.g., heel slides).
- Muscle Activation : Quadriceps sets, gluteal sets, ankle pumps.
- Cryotherapy & Compression : For pain and edema control.
- Key Milestones : Full passive knee extension, good quadriceps control (straight leg raise without extensor lag), minimal pain/effusion.
Phase II: Intermediate Strengthening & Neuromuscular Control (Weeks 6-12+)
- Goals : Restore full ROM, improve strength, enhance neuromuscular control, protect graft during maturation.
- Bracing : May be discontinued or used for high-risk activities.
-
Exercises
:
- ROM : Continue working towards full flexion and extension.
- Strengthening : Progressive resistance exercises (PREs) – open kinetic chain (OKC) exercises (e.g., knee extension machine, typically restricted to 0-45 degrees to limit anterior tibial translation stress on ACL graft), closed kinetic chain (CKC) exercises (e.g., wall squats, lunges, leg press). Hamstring strengthening (curls, bridges).
- Neuromuscular Control : Balance training (single leg stance, unstable surfaces), proprioceptive drills.
- Cardiovascular : Stationary cycling, elliptical trainer.
- Key Milestones : Full knee ROM, pain-free ambulation, quadriceps strength >70% contralateral, no effusion.
Phase III: Advanced Strengthening & Return to Sport Preparation (Months 3-6+)
- Goals : Maximize strength, power, and endurance; introduce agility and sport-specific drills.
- Bracing : Usually discontinued.
-
Exercises
:
- Strength & Power : Advanced PREs, plyometric exercises (box jumps, hopping), advanced OKC/CKC exercises.
- Agility : Ladder drills, cone drills, lateral shuffling, cutting maneuvers (gradual introduction).
- Sport-Specific Training : Mimicking movements and demands of the patient's intended sport.
- Running Progression : Gradually introduce running on flat surfaces.
- Key Milestones : Quadriceps strength >80% contralateral, improved proprioception and dynamic stability, pain-free high-impact activities. Graft maturation is ongoing; caution advised.
Phase IV: Return to Sport (Months 6-12+)
- Goals : Safe return to competitive sport or high-impact activities.
-
Criteria for Return to Sport (RTS)
:
- Time from surgery (minimum 6-9 months, often 9-12 months for ACL).
- No pain or swelling.
- Full ROM.
- Quadriceps and hamstring strength symmetry >90% contralateral.
- Successful completion of functional tests (e.g., single-leg hop tests, T-test, agility tests) >90% contralateral.
- Psychological readiness (fear of re-injury).
- Exercises : Continued advanced sport-specific drills, gradual re-integration into training and competition.
- Considerations : RTS timing is crucial to minimize re-injury risk, as graft maturation continues for up to 1-2 years. Decision-making is typically collaborative between surgeon, physical therapist, and athlete.
Specific Considerations
- Internal Brace Augmentation : When used, may allow for accelerated rehabilitation protocols due to enhanced initial construct stability, though biological healing remains a limiting factor.
- Multi-Ligament Injuries : Often require more cautious and prolonged rehabilitation due to the complexity and multiple healing tissues involved.
- Ligament Repair vs. Reconstruction : Repairs (e.g., MCL, some ATFL) may allow for slightly faster initial progression as native tissue is preserved, but still require protection.
- Patient Adherence : Strict compliance with the protocol is paramount for successful outcomes.
Summary of Key Literature / Guidelines
Evidence-based practice is the cornerstone of modern orthopedic surgery. The understanding and management of ligamentous injuries have been profoundly shaped by a robust body of literature and professional society guidelines.
Evolution of Concepts
- Anatomic Reconstruction : The shift from non-anatomic or isometric reconstructions to an anatomical approach (e.g., in ACL reconstruction) has been a significant development, aiming to restore native kinematics and improve rotational stability. This includes single-bundle vs. double-bundle techniques, with current consensus favoring meticulous single-bundle anatomic reconstruction for most patients.
- Graft Choice : Extensive research has compared various autograft (BTB, hamstring, quadriceps) and allograft options. While autografts remain the gold standard for most primary ACL reconstructions due to superior long-term outcomes and lower re-rupture rates, allografts are considered for revision surgeries or lower-demand patients. The debate on optimal graft for specific patient profiles continues.
- Fixation Techniques : Advancements in fixation hardware (e.g., adjustable loop cortical buttons, interference screws) have improved initial graft stability and simplified surgical techniques. Biomechanical studies have guided the choice of fixation based on graft type and desired strength.
- Biologic Augmentation : The role of biologics such as platelet-rich plasma (PRP) and mesenchymal stem cells (MSCs) in enhancing ligament healing and graft incorporation is an active area of research. While promising in basic science, clinical evidence for routine use in primary ligament reconstruction remains mixed and generally not conclusive enough for widespread adoption.
- Internal Bracing : The concept of augmenting a primary ligament repair with a synthetic high-strength suture (internal brace) has gained traction, particularly for collateral ligament repairs and certain ankle ligament injuries. Early evidence suggests improved initial stability and potentially accelerated rehabilitation.
- Rehabilitation Protocols : Evidence-based rehabilitation has moved towards a criteria-based progression, emphasizing early range of motion, gradual loading, and functional return-to-sport testing, rather than strict time-based protocols. The importance of neuromuscular control and objective strength testing (e.g., isokinetic dynamometry) for safe return to activity is well-established.
Key Literature & Professional Guidelines
-
ACL Reconstruction : The body of literature for ACL reconstruction is vast.
- Systematic Reviews and Meta-analyses : Consistently demonstrate the efficacy of ACL reconstruction in restoring stability and function, with autografts generally yielding lower re-rupture rates compared to allografts, especially in younger, active individuals.
- Randomized Controlled Trials (RCTs) : Compare different graft types, fixation methods, and rehabilitation protocols. The Scandinavian ACL Study Group (SACS) and the Multicenter ACL Revision Study (MARS) have provided invaluable insights into factors affecting primary and revision ACL outcomes.
- AAOS Clinical Practice Guidelines : Provide evidence-based recommendations on diagnostic modalities, surgical indications, graft selection, and post-operative management for ACL injuries.
- ESSKA and ISAKOS Consensus Statements : Offer international perspectives and recommendations on complex topics like revision ACL surgery, pediatric ACL tears, and prevention strategies.
-
MCL and LCL Injuries :
- MCL : The literature supports non-operative management for isolated Grade I/II MCL injuries. Grade III injuries, particularly in multi-ligament settings or those with significant instability, often warrant surgical repair or reconstruction. The role of surgical repair in isolated Grade III tears is debated, with some evidence suggesting favorable outcomes with non-operative management even for complete tears, provided other structures are intact.
- LCL Complex : Isolated LCL injuries are less common and often associated with more significant knee trauma. Surgical repair or reconstruction is more frequently indicated due to the poor healing potential and significant posterolateral instability that can result.
-
Ankle Ligament Injuries (Lateral Collateral Ligament Complex) :
- Acute Sprains : Most acute ankle sprains (Grade I/II ATFL/CFL) are managed non-operatively with RICE, early mobilization, and progressive rehabilitation.
- Chronic Instability : For patients with chronic symptomatic lateral ankle instability refractory to conservative management, anatomical repair (e.g., Brostrom-Gould procedure) or reconstruction (with or without internal brace augmentation) is highly effective. Comparative studies have shown good long-term outcomes for both techniques.
Future Directions
- Tissue Engineering and Regenerative Medicine : Further research into biologics (e.g., optimized PRP delivery, stem cell therapies) and bio-scaffolds to enhance native ligament healing and graft incorporation, potentially reducing re-injury rates and accelerating recovery.
- Robotics and Navigation : Increasing use of robotic assistance and computer navigation systems for precision tunnel placement and graft tensioning, aiming for more consistent anatomical reconstruction.
- Patient-Specific Implants : Development of customized fixation devices or grafts based on individual patient anatomy and biomechanics.
- Injury Prevention Strategies : Continued research into understanding risk factors and developing effective training programs to reduce the incidence of ligamentous injuries, particularly in athletes.
- Outcomes Research and Registries : Expanded use of patient-reported outcome measures (PROMs) and national/international registries to track long-term outcomes, identify best practices, and refine clinical guidelines.
In conclusion, the surgical management of ligamentous injuries is a dynamic field that continues to evolve with ongoing research into anatomy, biomechanics, surgical techniques, and rehabilitation strategies. Adherence to evidence-based principles and a comprehensive understanding of the current literature are essential for delivering optimal care to patients with these challenging conditions.
