INTRODUCTION TO VASCULARIZED FREE FIBULAR TRANSFER
The vascularized free fibular transfer (VFFT) represents a cornerstone technique in modern reconstructive microsurgery and orthopedic oncology. First popularized in the late 1970s, the fibula has become the premier donor site for bridging massive segmental bone defects (typically those exceeding 6 cm), reconstructing post-traumatic nonunions, managing congenital pseudarthrosis, and restoring skeletal integrity following wide oncologic resections.
The fibula's unique biomechanical and anatomical properties make it an ideal autograft. It is a straight, dense, tubular cortical bone that provides exceptional structural support. Furthermore, its dual blood supply—an endosteal supply via the nutrient artery and a robust periosteal supply via musculoperiosteal branches of the peroneal artery—allows for reliable harvest as a living composite tissue flap. When transferred with its vascular pedicle intact, the fibula bypasses the creeping substitution phase required by non-vascularized grafts, leading to primary bone healing, rapid hypertrophy in response to mechanical loading, and superior resistance to infection.
The lateral approach is the gold standard for harvesting the fibular graft. It provides direct, extensile access to the lateral compartment of the leg, allowing for safe identification and isolation of the peroneal neurovascular bundle while preserving the critical stabilizing structures of the knee and ankle.
Surgical Pearl: The success of a vascularized fibular graft hinges entirely on the meticulous preservation of its blood supply. The nutrient artery typically enters the middle third of the fibula. Therefore, the harvested segment must invariably include this region to ensure endosteal perfusion.
PREOPERATIVE PLANNING AND INDICATIONS
Indications
- Massive Bone Defects: Traumatic bone loss or post-debridement defects exceeding 6 cm where conventional cancellous grafting would fail.
- Oncologic Reconstruction: Intercalary reconstruction following diaphyseal tumor resection (e.g., osteosarcoma, Ewing sarcoma).
- Avascular Necrosis (AVN): Core decompression and vascularized fibular grafting for pre-collapse AVN of the femoral head.
- Congenital Deformities: Congenital pseudarthrosis of the tibia or radius.
- Recalcitrant Nonunions: Atrophic nonunions with poor local biology or previous failed reconstructions.
Contraindications
- Peripheral Vascular Disease (PVD): Severe atherosclerosis compromising the peroneal artery or rendering the leg dependent on the peroneal artery for distal perfusion (e.g., occluded anterior and posterior tibial arteries).
- Venous Insufficiency: Severe deep vein thrombosis history in the donor limb.
- Local Trauma: Previous severe trauma or compartment syndrome in the donor leg that has distorted the vascular anatomy.
Preoperative Imaging
A thorough vascular assessment is mandatory. Preoperative CT angiography (CTA) or conventional angiography of the bilateral lower extremities must be performed to confirm a patent three-vessel runoff to the foot. The surgeon must verify that the peroneal artery is not the dominant supply to the foot (arteria peronea magna), as harvesting it in such cases would result in catastrophic distal ischemia.
SURGICAL ANATOMY OF THE LATERAL LEG
A profound understanding of the cross-sectional anatomy of the leg is non-negotiable for this procedure. The fibula is bordered by three distinct muscular compartments:
1. Lateral Compartment: Contains the peroneus longus and brevis muscles, innervated by the superficial peroneal nerve.
2. Anterior Compartment: Contains the extensor digitorum longus (EDL), extensor hallucis longus (EHL), and tibialis anterior. The deep peroneal nerve and anterior tibial vessels course through this compartment.
3. Posterior Compartment: Divided into superficial (gastrocnemius, soleus) and deep (tibialis posterior, flexor hallucis longus, flexor digitorum longus) layers.
The peroneal artery, the lifeblood of the graft, arises from the tibioperoneal trunk. It descends through the deep posterior compartment, coursing distally just medial and posterior to the fibula, nestled between the tibialis posterior and the flexor hallucis longus (FHL). It gives off multiple musculoperiosteal perforators to the fibula and a distinct nutrient artery that enters the medullary canal.
SURGICAL TECHNIQUE: THE LATERAL APPROACH
Patient Positioning and Preparation
The patient is placed in the supine position with a bump under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the fibula into direct view. Alternatively, a lateral decubitus position can be utilized depending on the requirements of the recipient site. A sterile tourniquet is applied to the proximal thigh. The entire lower extremity is prepped and draped free to allow for intraoperative manipulation.
Incision and Superficial Dissection
- Incision: A longitudinal incision is made directly over the lateral surface of the fibula, extending from the fibular head to the lateral malleolus, depending on the anticipated length of the bone required.
- Fascial Incision: The subcutaneous tissues are divided to expose the deep fascia. The fascia is incised longitudinally in line with the skin incision.
- Identifying the Plane: The critical plane of dissection is the interval between the peroneus longus/brevis muscles (anteriorly) and the soleus muscle (posteriorly).
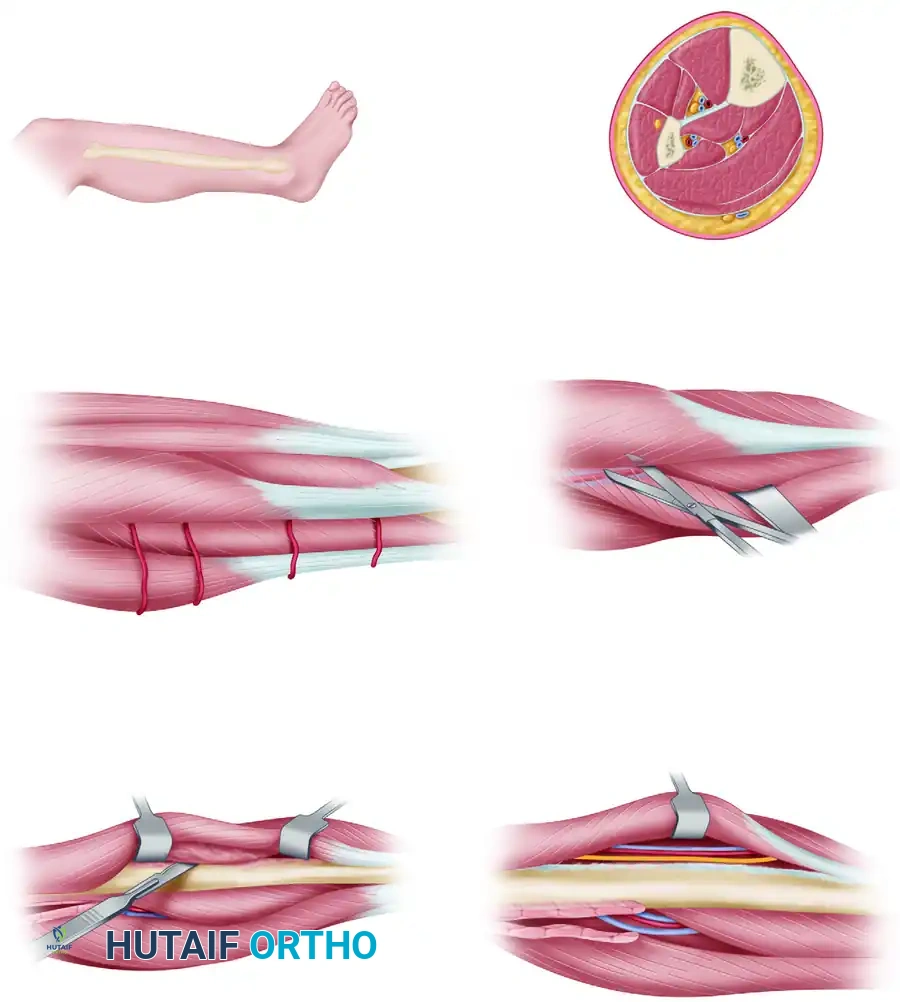
Deep Dissection and Muscle Release
- Soleus Release: The interval between the soleus and the peroneal muscles is defined and developed. The peroneal vessels are identified just distal and deep to the fibular origin of the soleus muscle in the proximal part of the dissection. The soleus origin is carefully released from the posterior aspect of the fibula using scissor dissection.
- Peroneal Muscle Elevation: Proceeding anteriorly, the peroneus longus and brevis muscles are released from the lateral fibular shaft in a strict extraperiosteal fashion.
> Surgical Warning: The common peroneal nerve wraps around the fibular neck proximally. When elevating the peroneal muscles, meticulous care must be taken to protect the superficial peroneal nerve within the muscle belly and the common peroneal nerve at the proximal extent of the dissection. - Anterior Compartment Release: The anterior dissection continues through the anterior intermuscular septum. The anterior compartment muscles (EDL, EHL) are released off the anterior surface of the fibula. This must be done extraperiosteally to avoid injuring the deep peroneal nerve and the anterior tibial vessels, which lie just medial to these muscles on the interosseous membrane.
Fibular Osteotomies
Before proceeding with the deep posterior dissection, the proximal and distal osteotomies are performed to mobilize the bone and facilitate access to the deep vascular pedicle.
- Determining Osteotomy Sites: The required length of the graft is measured. To preserve knee and ankle stability, a minimum of 6 to 8 cm of the proximal fibula (including the fibular head) and 6 to 8 cm of the distal fibula (lateral malleolus) must be retained.
- Distal Osteotomy: Bluntly develop an extraperiosteal plane closely around the fibula where the distal osteotomy is to be made. Retract the superficial and deep peroneal nerves, along with the anterior tibial vessels, anteriorly. Retract the peroneal vessels posteriorly. Osteotomize the fibula using a Gigli saw, protecting the surrounding soft tissues.
- Proximal Osteotomy: Place a Gigli saw around the fibula where the proximal osteotomy is to be made.
> Clinical Pearl: The proximal osteotomy must be situated within the proximal third of the fibula to guarantee that the nutrient artery (which typically enters the middle third) is included within the harvested segment.
Mobilization and Pedicle Isolation
With the osteotomies complete, the fibular segment is now mobile, allowing for the most critical phase of the operation: isolating the peroneal pedicle.
- FHL Elevation: Sharply elevate the flexor hallucis longus (FHL) off the fibula for a distance of 1 cm proximal and distal to the distal osteotomy site. Retract the fibula anteriorly and the FHL posteriorly. The peroneal vessels are well protected posteriorly by the FHL and can be seen coursing distally within the muscle.
- Distal Pedicle Ligation: In the distal part of the leg, identify the peroneal vessels coursing close to the fibula. They may perforate the interosseous membrane to continue anteriorly. Once definitively identified, ligate and divide the distal continuation of the peroneal artery and venae comitantes.
- Interosseous Membrane Release: Grasp the mobilized fibular segment with a bone clamp (e.g., a Lewin clamp) and gently externally rotate it. Apply gentle lateral traction and incise the interosseous membrane close to the fibula from distal to proximal.
> Surgical Warning: Take extreme care not to avulse the musculoperiosteal perforators connecting the fibula to the peroneal vessels during this traction.
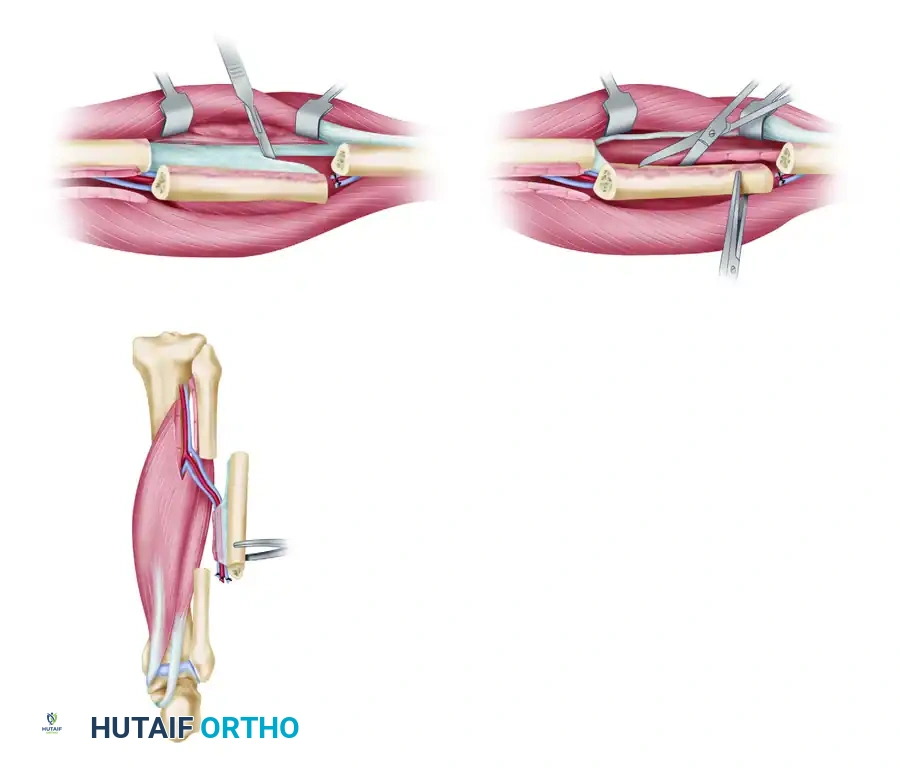
- Tibialis Posterior Release: From an anterior perspective, release the tibialis posterior muscle from the medial aspect of the fibula while directly observing the peroneal vessels. Small muscular branches from the peroneal artery supplying the tibialis posterior should be meticulously clipped or cauterized with bipolar electrocautery.
- Final FHL Release: Release the remaining flexor hallucis longus from the posterior fibula. Crucially, leave a thin, 1- to 2-mm layer of FHL muscle attached to the posterior aspect of the fibula. This muscle cuff protects the delicate musculoperiosteal perforators arising from the peroneal artery.
- Pedicle Harvest: The fibular graft is now completely isolated on its proximal vascular pedicle (the peroneal artery and venae comitantes). The tourniquet is deflated.
> Clinical Pearl: We routinely allow the bone to be perfused in situ for 15 to 20 minutes prior to pedicle division. This minimizes total ischemic time and allows the surgeon to confirm robust bleeding from the medullary canal and muscle cuff, verifying graft viability. - Pedicle Division: Once the recipient site is fully prepared, the peroneal artery and venae comitantes are ligated and divided at their origin from the tibioperoneal trunk.
Donor Site Closure
Meticulous hemostasis is obtained. The remaining FHL muscle belly is loosely sutured to the interosseous membrane to prevent herniation and dead space. A closed suction drain is placed deep in the wound. The subcutaneous tissues and skin are closed in layers.
🚨 CRITICAL PITFALL: Under no circumstances should the deep fascia of the leg be closed. Attempting to close the fascial layers significantly increases the risk of postoperative acute compartment syndrome.
PEDIATRIC CONSIDERATIONS: PREVENTING VALGUS DRIFT
Harvesting the fibular shaft in children with significant remaining skeletal growth presents a unique biomechanical challenge. The distal fibula acts as a critical lateral buttress for the ankle mortise. When the diaphyseal continuity is disrupted, the proximal migration of the lateral malleolus can occur due to the pull of the surrounding musculature and normal growth mechanics. This inevitably leads to a progressive, debilitating valgus deformity of the ankle.
To prevent this complication, a prophylactic distal tibiofibular syndesmosis fusion is strictly recommended in the pediatric population.
🔪 Surgical Technique 63-26: Distal Tibiofibular Fusion
- Preparation: After the successful harvest of the fibular graft as described above, direct attention to the distal fibular remnant and the adjacent tibia.
- Decortication: Decorticate a 2- to 3-cm area of the facing articular surfaces of the tibia and the distal fibular remnant, situated just above the distal metaphysis.
- Graft Placement: Obtain a 3-cm segment of bone. This can be harvested from the discarded ends of the fibular graft or from the remaining proximal fibular stump. Place this bone block as a strut between the decorticated surfaces of the tibia and fibula.
- Fixation: Insert two fully threaded cortical screws transversely across the fibula, through the intercalary bone graft, and into the tibia. Utilize standard AO lag screw techniques to achieve rigid compression across the fusion site.

Postoperative Care for Pediatric Fusion:
The pediatric patient must be placed in a long-leg, bent-knee, strictly non-weight-bearing cast for 6 weeks. This is followed by a transition to a patellar tendon-bearing (PTB) cast for an additional 6 weeks to ensure solid arthrodesis of the syndesmosis before physiological loading.
RECIPIENT SITE FIXATION AND MICROVASCULAR ANASTOMOSIS
When transferred to the recipient site, the fibular graft must be rigidly fixed to the host bone. The preferred method involves doweling (invaginating) each end of the fibular strut into the reamed medullary canals of the recipient bone segments. This provides intrinsic biomechanical stability. Supplemental fixation with bridging plates and screws is almost universally applied to neutralize rotational and bending forces.
The method of fixation is highly dependent on recipient site factors (e.g., femur vs. radius, tumor vs. trauma). However, before any definitive osteosynthesis is performed, the surgeon must give careful consideration to pedicle length, geometry, and positioning. The pedicle must reach the recipient artery and vein without tension, kinking, or twisting.
Once rigid skeletal fixation is complete, the microvascular team proceeds with the arterial and venous anastomoses using standard microsurgical techniques (typically end-to-end or end-to-side anastomoses using 8-0 or 9-0 nylon sutures).
POSTOPERATIVE CARE AND REHABILITATION
Graft Monitoring
Immediate postoperative monitoring of the buried vascularized bone graft is challenging. A technetium-99m methylene diphosphonate (Tc-99m MDP) bone scan is usually obtained within the first 3 to 7 days postoperatively. Focal uptake within the grafted segment confirms microvascular patency and endosteal perfusion. Alternatively, an implantable venous Doppler probe can be placed around the venous anastomosis for continuous real-time monitoring in the ICU.
Immobilization and Weight-Bearing
Immobilization protocols are dictated entirely by the recipient site:
* Lower Extremity Reconstructions (e.g., Tibia): If the graft is placed below the knee, a long-leg cast with the knee flexed is applied to prevent weight-bearing and rotational stress. This non-weight-bearing status is strictly maintained for 3 to 5 months.
* Femur or Knee Arthrodesis: If the graft is applied for a knee fusion, femoral reconstruction, or in a small child, a long-leg cast with a pelvic band or a full 1.5 spica cast may be required to immobilize the limb sufficiently to permit undisturbed healing.
Long-Term Rehabilitation
Union of the graft to the recipient host bone is evaluated via serial orthogonal radiographs and clinical examination. Full weight-bearing is never permitted until the graft begins to demonstrate clear radiographic signs of hypertrophy (cortical thickening in response to Wolff's Law).
Because the fibula is significantly narrower than the femur or tibia, it must hypertrophy to match the mechanical demands of the lower extremity. This hypertrophic phase is prolonged and may require 15 months or more. During this transitional period, when healing is progressing but the bone is not yet fully hypertrophied, a custom-molded orthosis (e.g., a PTB brace or KAFO) must be fitted. The orthosis is worn continuously during ambulation until the reconstructed limb is biomechanically strong enough to support full, unprotected physiological weight-bearing. In cases of delayed union at the host-graft junctions, supplemental conventional autologous cancellous bone grafting (e.g., from the iliac crest) may be required.
