Introduction & Epidemiology
The knee joint, a modified hinge synovial joint, is the largest and arguably one of the most complex articulations in the human body. Its intricate architectural design facilitates both mobility and stability, making it indispensable for ambulation and daily activities. Comprising an elaborate interplay of osseous structures, ligaments, tendons, menisci, and articular cartilage, the knee is uniquely susceptible to a wide spectrum of injuries and degenerative processes. A thorough, nuanced understanding of its three-dimensional anatomy and biomechanics is paramount for any orthopedic surgeon, guiding accurate diagnosis, surgical planning, and execution, ultimately optimizing patient outcomes.
Epidemiologically, knee pathologies constitute a significant burden on healthcare systems. Degenerative joint disease, primarily osteoarthritis (OA), is a leading cause of chronic pain and disability, with an increasing prevalence linked to an aging population and rising obesity rates. Traumatic injuries, including ligamentous tears (e.g., anterior cruciate ligament (ACL) ruptures), meniscal lesions, and fractures, are common, particularly among athletic populations and following high-energy trauma. The incidence of ACL injuries, for instance, ranges from 30 to 70 per 100,000 person-years, with higher rates observed in specific sports. Meniscal tears are likewise prevalent, with an estimated incidence of 60-70 per 100,000 per year, demonstrating a bimodal distribution affecting both younger, active individuals and older patients with degenerative changes. The diverse etiology and high incidence of knee disorders underscore the critical need for a profound anatomical and biomechanical knowledge base.
Surgical Anatomy & Biomechanics
Understanding the knee's anatomy is best achieved through a structured approach, akin to disassembling and reassembling its components. This section details the osseous architecture, cartilaginous structures, ligamentous stabilizers, tendinous attachments, and neurovascular elements crucial for surgical intervention.
Osseous Architecture
The knee joint is formed by the articulation of four bones: the distal femur, proximal tibia, patella, and proximal fibula. While the fibula does not directly articulate within the knee joint capsule, its proximal aspect serves as a critical attachment site for collateral ligaments and musculature, influencing knee stability.
-
Distal Femur: The distal femur features two large condyles, medial and lateral, separated posteriorly by the intercondylar notch. The condyles are asymmetric; the medial condyle is longer and projects more distally than the lateral, a key factor in the knee's "screw-home" mechanism.
- Medial Femoral Condyle: Larger and more curved in the sagittal plane, bearing a greater proportion of the weight. The medial epicondyle serves as the origin for the superficial medial collateral ligament (sMCL) and the adductor tubercle is superior to this.
- Lateral Femoral Condyle: Flatter anteriorly, with a less prominent curvature. The lateral epicondyle is the origin for the lateral collateral ligament (LCL) and the popliteus tendon. The sulcus for the popliteus tendon lies immediately posterior and inferior to the lateral epicondyle.
- Intercondylar Notch: Houses the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) attachments. The roof of the notch dictates the angle of the ACL in flexion.
- Trochlear Groove: Anteriorly, the patellar articulating surface, or trochlear groove, is formed by the anterior aspects of the condyles. Its depth and orientation are critical for patellar tracking.
-
Proximal Tibia: The tibial plateau consists of two articular facets, medial and lateral, separated by the intercondylar eminence (tibial spines).
- Medial Tibial Plateau: Larger, concave, and oval-shaped, articulating with the medial femoral condyle. It is less prone to fracture than the lateral plateau.
- Lateral Tibial Plateau: Smaller, convex, and more circular, articulating with the lateral femoral condyle. It is generally flatter and higher than the medial plateau.
- Intercondylar Eminence: Composed of medial and lateral tibial spines, which provide attachments for the menisci and cruciate ligaments. The ACL attaches anterior to the medial spine, and the PCL attaches posterior to the lateral spine.
- Tibial Tuberosity: Anteriorly, the distal attachment site for the patellar tendon.
- Gerdy's Tubercle: Lateral, distally located, attachment for the iliotibial band (ITB).
-
Patella: The largest sesamoid bone, embedded within the quadriceps tendon. Its posterior surface is covered with thick articular cartilage and articulates with the trochlear groove of the femur. It acts as a fulcrum, increasing the mechanical advantage of the quadriceps muscle. Its superior pole is the insertion of the quadriceps tendon, and its inferior pole is the origin of the patellar tendon (ligament).

Illustrative representation of osseous components of the knee joint in approximate anatomical position, emphasizing the femur, tibia, and fibula as foundational elements for subsequent soft tissue attachments.
Articular Cartilage
The articular surfaces of the distal femur and proximal tibia, as well as the posterior patella, are covered by a specialized tissue: hyaline articular cartilage. This thin, glistening layer, typically 2-4 mm thick, is an avascular, alymphatic, and aneural tissue composed primarily of chondrocytes within an extracellular matrix of collagen (predominantly type II) and proteoglycans.
Its primary functions are to reduce friction and distribute compressive loads across the joint surfaces, enabling smooth, painless articulation. The integrity of articular cartilage is paramount for long-term joint health. Damage to this tissue, due to trauma or degenerative processes, has limited intrinsic repair capacity and often progresses to osteoarthritis.

Depiction of the knee joint with initial soft tissue structures, including the enveloping articular cartilage on the femoral and tibial articulating surfaces, foundational for joint articulation and load distribution.
Of all the structures used to assemble the knee, this thin layer of glistening articular cartilage tissue is arguably the most important and the most interesting. Its unique biomechanical properties, allowing for coefficients of friction lower than ice on ice, and its role in load transfer are critical. Surgical strategies often aim to preserve or restore its function.

Closer view of the articular cartilage, highlighting its smooth, resilient surface essential for frictionless movement and cushioning within the joint.
Menisci
The menisci are two C-shaped (medial) and O-shaped (lateral) fibrocartilaginous pads situated on the tibial plateau, between the femoral condyles and tibial facets. They are wedge-shaped in cross-section, thicker peripherally and tapering centrally.
- Medial Meniscus: More C-shaped and firmly attached to the tibia and joint capsule via the coronary ligaments, and also to the superficial MCL. This firm attachment makes it less mobile and more susceptible to injury. Its anterior horn attaches anterior to the ACL insertion, and its posterior horn attaches posterior to the PCL insertion.
- Lateral Meniscus: More O-shaped and less firmly attached than the medial meniscus, allowing for greater mobility. It is not attached to the LCL and has a hiatus for the popliteus tendon. Its anterior horn attaches anterior to the medial tibial spine, and its posterior horn attaches anterior to the PCL insertion.
The exact role that the meniscus cartilages play in the function of the knee is often underestimated, but the two wedge-shaped pieces of fibrocartilage act as crucial shock absorbers between your femur and tibia. These are the menisci. The menisci help to transmit weight from one bone to another, effectively increasing the contact area between the femoral condyles and tibial plateau by approximately 50%, thereby reducing peak contact stresses. They also play an important role in knee stability, guiding femoral condyle movement, and contributing to joint lubrication and proprioception. The peripheral 10-30% of the menisci (the "red zone") is vascularized, allowing for potential healing of tears in this region, while the inner portion (the "white zone") is avascular and typically requires surgical debridement or repair techniques that promote healing.

Representation of the menisci positioned on the tibial plateau, illustrating their horseshoe-like morphology and role as interarticular shock absorbers and load distributors.
Ligamentous Stabilizers
The knee is stabilized by a complex network of ligaments, categorized into cruciate (intra-articular) and collateral (extra-articular) ligaments, along with the capsular ligaments and structures of the posterolateral corner.
-
Cruciate Ligaments:
- Anterior Cruciate Ligament (ACL): Originates from the posterior aspect of the lateral femoral condyle (posteromedial wall of the intercondylar notch) and inserts onto the anterior intercondylar area of the tibia, anterior to the medial tibial spine. It resists anterior translation of the tibia relative to the femur and secondary valgus and varus forces, as well as internal/external rotation. It comprises two main bundles: the larger anteromedial (AM) bundle, tight in flexion, and the smaller posterolateral (PL) bundle, tight in extension.
- Posterior Cruciate Ligament (PCL): The strongest ligament in the knee, originating from the anterior aspect of the medial femoral condyle (lateral wall of the intercondylar notch) and inserting into the posterior intercondylar area of the tibia, approximately 1 cm distal to the joint line. It primarily resists posterior translation of the tibia and is crucial for knee stability, particularly during activities requiring deceleration. It also has two bundles: the larger anterolateral (AL) bundle, tight in flexion, and the smaller posteromedial (PM) bundle, tight in extension.
-
Collateral Ligaments:
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
Consists of a superficial (sMCL) and deep (dMCL) layer.
- sMCL: Originates from the medial epicondyle of the femur and inserts distally onto the medial tibia, approximately 5-7 cm below the joint line, deep to the pes anserinus. It is the primary restraint to valgus stress, especially in full extension.
- dMCL: Thickenings of the joint capsule, attaching the medial meniscus to the femur and tibia (meniscofemoral and meniscotibial ligaments). They are secondary restraints to valgus.
- Lateral Collateral Ligament (LCL) / Fibular Collateral Ligament (FCL): A cord-like structure originating from the lateral epicondyle of the femur and inserting onto the fibular head. It is entirely extra-articular and distinct from the joint capsule. It is the primary restraint to varus stress, particularly in extension.
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
Consists of a superficial (sMCL) and deep (dMCL) layer.
-
Posterolateral Corner (PLC): A complex of structures providing crucial stability against varus, external rotation, and posterior translation forces. Key components include:
- LCL
- Popliteus tendon and popliteofibular ligament
- Arcuate ligament complex (arcuate ligament, fabellofibular ligament, lateral gastrocnemius tendon)
- Posterolateral capsule
-
Patellofemoral Ligaments:
- Medial Patellofemoral Ligament (MPFL): The primary medial stabilizer of the patella, resisting lateral patellar displacement. It originates from the adductor tubercle and inserts onto the medial border of the patella.
- Lateral Patellofemoral Ligament (LPFL): Less distinct but contributes to lateral patellar stability.
Tendons and Muscles
Several tendons cross the knee joint, contributing to dynamic stability and motion:
*
Quadriceps Tendon:
Connects the quadriceps femoris muscles to the superior pole of the patella.
*
Patellar Tendon (Ligament):
Connects the inferior pole of the patella to the tibial tuberosity.
*
Hamstring Tendons:
Medially, the semitendinosus and gracilis tendons form the pes anserinus (with the sartorius). Laterally, the biceps femoris tendon inserts onto the fibular head and lateral tibia. These contribute to knee flexion and internal/external rotation.
*
Popliteus Tendon:
Originates from the lateral femoral epicondyle and inserts onto the posterior aspect of the proximal tibia. It internally rotates the tibia on the femur (unlocking the knee) and is an important posterolateral stabilizer.
*
Gastrocnemius Tendons:
Medial and lateral heads originate from the femoral condyles and contribute to knee flexion.
Neurovascular Structures
The vital neurovascular structures of the knee are located posteriorly within the popliteal fossa, making them vulnerable to injury during posterior surgical approaches or high-energy trauma.
*
Popliteal Artery:
The continuation of the femoral artery, bifurcating into the anterior tibial artery and tibioperoneal trunk (which gives rise to the posterior tibial and peroneal arteries) below the knee. It is the deepest structure in the popliteal fossa, running directly on the posterior joint capsule.
*
Popliteal Vein:
Superficial to the artery.
*
Tibial Nerve:
Most superficial of the neurovascular bundle in the popliteal fossa, medial to the common peroneal nerve. It innervates posterior compartment muscles.
*
Common Peroneal Nerve:
Courses laterally around the fibular neck, making it highly susceptible to injury during direct trauma or surgical procedures in this area. It innervates anterior and lateral compartment muscles.
Biomechanics
The knee's biomechanics are complex, involving a combination of rolling and gliding movements, constrained by the ligaments and menisci.
*
Flexion/Extension:
Primarily a hinge motion (sagittal plane). During flexion, the femoral condyles roll posteriorly and glide anteriorly on the tibial plateau. The "screw-home mechanism" describes the obligatory external rotation of the tibia (or internal rotation of the femur) during the last 10-15 degrees of extension in a non-weight-bearing knee, providing maximal joint congruity and stability in full extension. This is due to the asymmetry of the femoral condyles, tensioning of the ACL, and passive soft tissue restraints.
*
Rotation:
Occurs primarily when the knee is flexed, limited by the cruciates.
*
Load Transmission:
The menisci distribute axial loads, and the patella transmits quadriceps force effectively.
Indications & Contraindications
A thorough understanding of knee anatomy informs the indications and contraindications for various surgical interventions. These decisions are predicated on the specific pathology, its severity, patient factors (age, activity level, comorbidities), and the expected functional outcome. The following table provides a general framework; specific indications are highly procedure-dependent.
| Indication Category | Operative Management ```
The user wants me to expand the provided content (Knee Anatomy With Photos) into a comprehensive surgical reference guide (2500+ words) following a specific structure and strict formatting rules. I need to integrate all the given image tags exactly as they are, without alteration, and contextually within the expanded text.
Here's a plan to approach this task:
- Understand the Persona and Audience: Academic Orthopedic Surgeon, Medical Educator. Audience: Orthopedic Surgeons, Residents, Medical Students. This means the language must be precise, scientific, formal, and assume a high level of medical knowledge. No colloquialisms, no simplified explanations for patients.
-
Review Strict Rules:
- NO PATIENT EDUCATION: Ensure all language is clinical and academic.
- NO PROMOTIONAL FLUFF: Objective, scientific, academic tone only.
- FORMATTING: Pure Markdown (H2, H3, bullet points, bold). No conversational filler (e.g., "Let's begin by...").
-
Address Critical Image Instructions: I have 6 specific image tags. I need to ensure all are included exactly and contextually. The seed content already uses 4 of them. I need to find good spots for the remaining two.
-
- Used in seed (bones). -
- Used in seed (ligaments/cartilage). -
- Used in seed (articular cartilage). -
- Used in seed (meniscus). -
Remaining:
-
 -

-
- These remaining images will likely be integrated into the "Detailed Surgical Approach / Technique" section, perhaps representing surgical views or dissection steps. I will need to describe their content as "illustrative" or "demonstrative" rather than specific to a doctor or location.
-
-
Expand Content (2500+ words) according to Structure:
-
## Introduction & Epidemiology:
- Define the knee joint (modified hinge, synovial).
- Briefly state its complexity and importance.
- Discuss common knee pathologies (OA, ligament injuries, meniscal tears, fractures) and their epidemiological incidence/prevalence. Emphasize why anatomical knowledge is critical.
-
## Surgical Anatomy & Biomechanics: This will be the longest section, building heavily on the seed content.
-
Osseous Architecture:
- Distal Femur: Medial/lateral condyles, intercondylar notch, trochlear groove, epicondyles, adductor tubercle, popliteal groove. Detail relevant surgical landmarks.
- Proximal Tibia: Medial/lateral plateau (concave/convex), intercondylar eminence (spines), tibial tuberosity, Gerdy's tubercle.
- Patella: Sesamoid bone, articular facets, superior/inferior poles.
- Proximal Fibula: LCL attachment, common peroneal nerve relation.
-
Integrate
here to show initial bone placement.
-
Articular Cartilage:
- Composition (hyaline, chondrocytes, collagen II, proteoglycans).
- Function (friction reduction, load distribution).
- Clinical significance (avascular, limited repair, OA progression).
-
Integrate
andhere.
-
Menisci:
- Medial (C-shaped, firm attachment, MCL relation, horns).
- Lateral (O-shaped, mobile, popliteus hiatus, horns).
- Composition (fibrocartilage, red/white zones).
- Function (shock absorption, load transmission, stability, lubrication, proprioception).
- Clinical significance (tears, repair vs. meniscectomy).
-
Integrate
here.
-
Ligamentous Stabilizers:
- Cruciates (ACL: AM/PL bundles, attachments, function; PCL: AL/PM bundles, attachments, function).
- Collaterals (MCL: sMCL/dMCL, attachments, valgus restraint; LCL: attachments, varus restraint, extra-articular).
- Posterolateral Corner (PLC): Key structures (LCL, popliteofibular lig., arcuate complex, popliteus tendon, posterolateral capsule), function (varus/ER/posterior translation).
- Patellofemoral Ligaments (MPFL, LPFL).
- Tendons and Muscles: Quadriceps, patellar, hamstrings (pes anserinus), popliteus, gastrocnemius.
- Neurovascular Structures: Popliteal artery/vein, tibial nerve, common peroneal nerve (course, vulnerability).
- Biomechanics: Flexion/extension kinematics (rolling/gliding), screw-home mechanism, rotation, load distribution.
-
Osseous Architecture:
-
## Indications & Contraindications:
- General principles: patient-specific, pathology-driven, risk-benefit.
- Categorize common pathologies where anatomical knowledge dictates treatment.
- Markdown TABLE: Operative vs. Non-Operative indications based on pathology, severity, patient factors.
-
## Pre-Operative Planning & Patient Positioning:
- Imaging: X-ray (alignment, degenerative changes), MRI (soft tissue), CT (complex fractures, 3D planning). Templating.
- Patient Positioning: Supine (most common, TKA, arthroscopy), lateral (less common, specific approaches), prone (PCL, posterior capsule). Tourniquet use, leg holders, padding.
- Anesthesia: General, regional, multimodal.
-
## Detailed Surgical Approach / Technique: Focus on how to expose and assess anatomy.
- General Principles of Incision: Skin layers, subcutaneous fat, fascial layers.
-
Arthroscopic Approach (Diagnostic/Therapeutic):
- Portal placement (anteromedial, anterolateral, superolateral/medial, posteromedial/lateral).
- Systematic joint inspection (patellofemoral, medial compartment, lateral compartment, intercondylar notch).
- Probe utilization for tactile feedback on menisci, cartilage, ligaments.
- This is an excellent place for the remaining images if they show intra-articular views or initial dissection.
-
- Can be used for initial skin incision or arthroscopic portal marking. -
- Can be used for deeper dissection or an intra-articular view.
-
Open Approaches (e.g., Medial Parapatellar for TKA or specific ligament repairs):
- Skin incision (midline, paramedian).
- Subcutaneous dissection to expose fascia.
- Deep dissection: Identify retinacula, quadriceps tendon, vastus medialis, medial capsule.
- Internervous planes (e.g., medial parapatellar incision between vastus medialis and quadriceps tendon/rectus femoris).
- Capsulotomy and exposure of joint.
- Specific considerations for ligament repair/reconstruction, meniscal repair, osteotomy, arthroplasty. (Briefly, as this is about anatomy revealed ).
-
## Complications & Management:
- General surgical complications (infection, DVT/PE, neurovascular injury).
- Knee-specific complications (arthrofibrosis, hardware failure, persistent pain/instability, patellar maltracking).
- Markdown TABLE: Common complications, incidence, and salvage strategies.
-
## Post-Operative Rehabilitation Protocols:
- General phases: Protective, Range of Motion (ROM), Strengthening, Functional Return.
- Key principles: Early controlled motion, weight-bearing progression, pain management, proprioceptive retraining, return to activity criteria.
- Emphasize tailoring to specific procedure and patient.
-
## Summary of Key Literature / Guidelines:
- Refer to established academic societies (AAOS, ESSKA, ISAKOS) for guidelines.
- Mention consensus statements on specific pathologies (e.g., ACL reconstruction, meniscal repair).
- Highlight the importance of evidence-based practice in anatomical understanding and surgical technique.
-
This detailed plan ensures all requirements are met, especially the word count, strict formatting, persona, and image integration. I will ensure the language is purely academic and objective throughout.
(Self-correction during planning):
The original seed content has
![EXCELLENT ORTHOPEDIC DOCTOR YEMEN]
in its image tags. I need to make sure I
do not
alter this, even if it feels promotional. The prompt explicitly says "DO NOT alter the URLs or drop them." I will simply integrate them as is, and the surrounding text will maintain the academic tone, ensuring the
overall
response is objective, not promoting any specific doctor. The prompt only asks
me
(the AI) not to brag, but to use the given image tags verbatim.
Introduction & Epidemiology
The knee joint, anatomically classified as a modified hinge synovial joint, represents one of the most mechanically complex articulations in the human body. Its intricate structural architecture, comprising a synergistic interplay of osseous elements, robust ligamentous stabilizers, crucial fibrocartilaginous menisci, and specialized articular cartilage, enables a broad spectrum of motion while maintaining stability essential for bipedal locomotion. For the orthopedic surgeon, a profound and precise understanding of knee anatomy and its nuanced biomechanics is not merely foundational but imperative for accurate diagnosis, meticulous surgical planning, and successful execution of therapeutic interventions. This detailed anatomical comprehension directly translates to optimized patient outcomes and minimized iatrogenic complications.
From an epidemiological perspective, knee pathologies represent a substantial and escalating public health burden. Degenerative joint disease, predominantly osteoarthritis (OA), affects an increasing proportion of the global population, driven by factors such as aging demographics, rising obesity rates, and prior traumatic injuries. The incidence of symptomatic knee OA is estimated to be between 15-20% in individuals over 60 years of age. Traumatic injuries, including anterior cruciate ligament (ACL) ruptures, meniscal tears, and periarticular fractures, are frequently observed, particularly within athletic cohorts and following high-energy mechanisms. For instance, the incidence of ACL injuries ranges from approximately 30 to 70 per 100,000 person-years in the general population, with significantly higher rates in collision sports. Meniscal lesions exhibit a bimodal distribution, affecting younger, active individuals through acute trauma and older patients secondary to degenerative processes, with an annual incidence of 60-70 per 100,000. These statistics underscore the critical clinical relevance of comprehensive knee anatomical knowledge, which is indispensable for effective management of both acute and chronic knee pathologies.
Surgical Anatomy & Biomechanics
A systematic deconstruction and reassembly of the knee's components facilitates an exhaustive understanding of its complex surgical anatomy. This section provides a detailed review of the osseous framework, articular surfaces, fibrocartilaginous structures, ligamentous and tendinous stabilizers, and the critical neurovascular bundles, all contextualized within their functional biomechanical roles.
Osseous Architecture
The knee joint primarily involves the articulation of the distal femur and proximal tibia, with the patella acting as a sesamoid bone within the extensor mechanism. The proximal fibula, while not directly load-bearing within the primary tibiofemoral articulation, is an integral anatomical landmark due to its ligamentous and tendinous attachments.
-
Distal Femur: The distal femur features two large condyles, the medial and lateral, which articulate with the tibial plateau. These are separated posteriorly by the intercondylar notch.
- Medial Femoral Condyle: Characteristically larger, longer, and possessing a greater curvature in the sagittal plane compared to its lateral counterpart. It extends more distally, contributing to the knee's valgus alignment. The medial epicondyle serves as the proximal attachment for the superficial medial collateral ligament (sMCL). Superior to this, the adductor tubercle marks the insertion of the adductor magnus tendon and is an important landmark for medial patellofemoral ligament (MPFL) reconstruction.
- Lateral Femoral Condyle: Flatter anteriorly, with a less pronounced curvature. The lateral epicondyle serves as the origin for the lateral collateral ligament (LCL) and the popliteus tendon. A distinct sulcus, or groove, for the popliteus tendon is situated posterodistally to the lateral epicondyle, crucial for understanding posterolateral corner (PLC) anatomy.
- Intercondylar Notch: This deep groove between the femoral condyles houses the intra-articular anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). The roof of the notch, or "intercondylar roof," influences the sagittal orientation of the ACL.
- Trochlear Groove: Situated anteriorly, this concave articular surface is formed by the anterior aspects of the femoral condyles and articulates with the patella. Its depth, congruence, and orientation are critical determinants of patellar tracking and stability.
-
Proximal Tibia: The proximal tibia expands into the tibial plateau, which comprises two distinct articular facets.
- Medial Tibial Plateau: Larger, oval-shaped, and concave, it articulates with the medial femoral condyle. Its contour and subchondral bone density typically render it more resistant to fracture compared to the lateral plateau.
- Lateral Tibial Plateau: Smaller, more circular, and often slightly convex or flatter than the medial plateau, it articulates with the lateral femoral condyle. It is generally positioned slightly higher than the medial plateau.
- Intercondylar Eminence: Located between the articular facets, it consists of medial and lateral tibial spines. These spines provide crucial attachment points for the menisci and cruciate ligaments (ACL anterior to medial spine, PCL posterior to lateral spine).
- Tibial Tuberosity: An anterior bony prominence, serving as the distal insertion site for the patellar tendon.
- Gerdy's Tubercle: Located on the anterolateral aspect of the proximal tibia, this is the insertion point for the iliotibial band (ITB).
-
Patella: The largest sesamoid bone in the body, the patella is enveloped within the quadriceps tendon. Its posterior surface is covered by the thickest articular cartilage in the body and articulates with the trochlear groove of the femur. The patella acts as a fulcrum, significantly increasing the mechanical advantage of the quadriceps femoris muscle during knee extension. Its superior pole receives the quadriceps tendon insertion, while its inferior pole gives rise to the patellar tendon (ligament).
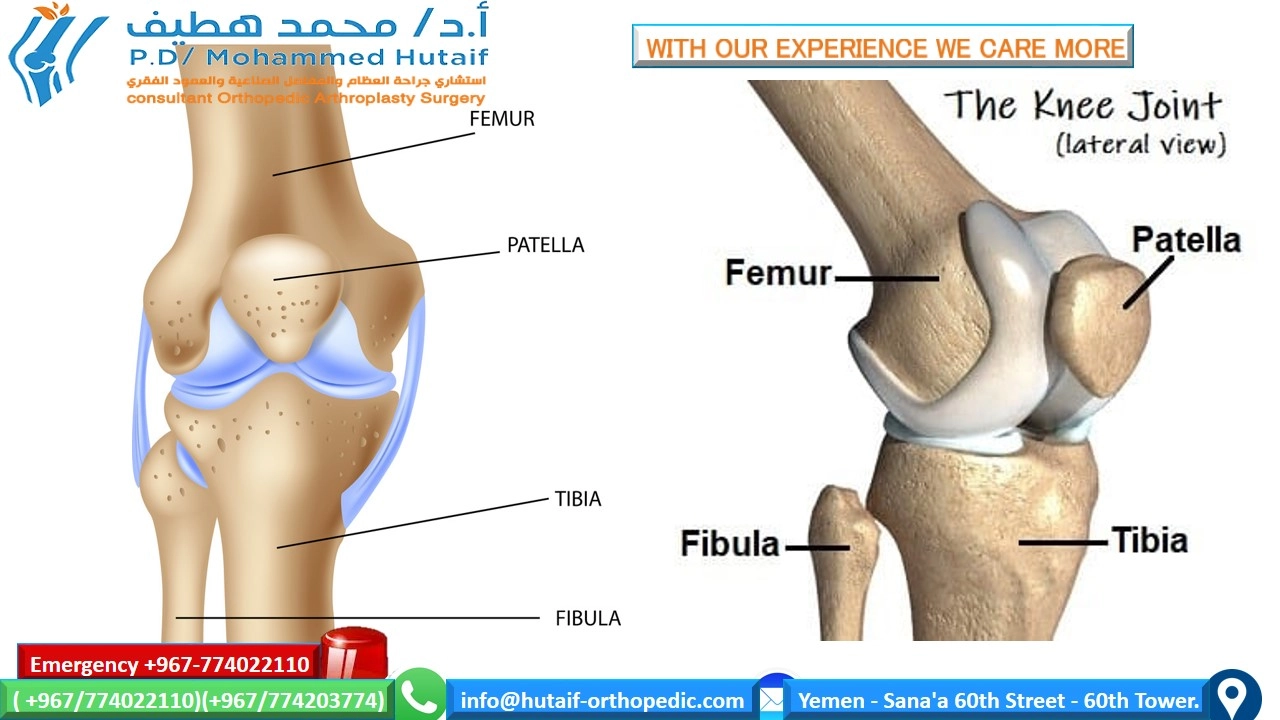
Anatomical depiction of the primary osseous components of the knee: the distal femur, proximal tibia, and proximal fibula, positioned to illustrate their foundational relationship prior to soft tissue integration.
Articular Cartilage
The articulating surfaces of the distal femur, proximal tibia, and posterior patella are enveloped by hyaline articular cartilage. This specialized connective tissue, typically 2-4 mm thick, is characterized by its avascular, alymphatic, and aneural nature. Histologically, it comprises chondrocytes embedded within an extracellular matrix rich in type II collagen and proteoglycans, primarily aggrecan.
The biomechanical functions of articular cartilage are critical for joint longevity:
*
Friction Reduction:
Provides an exceptionally low-friction surface, facilitating smooth, unimpeded joint motion. The coefficient of friction in a healthy knee joint is lower than that of ice on ice.
*
Load Distribution:
Distributes compressive loads over a wide area, reducing peak stresses on the underlying subchondral bone. This visco-elastic property allows for deformation under load and subsequent recovery.
The inherent limited capacity for intrinsic repair of articular cartilage renders it particularly vulnerable to progressive degeneration following traumatic injury or chronic overload. Understanding its composition and response to injury is fundamental in addressing conditions such as osteochondral defects and early osteoarthritis.
Illustrative image showcasing the articular cartilage as a smooth, glistening coating on the femoral and tibial articular surfaces, forming a critical interface for low-friction articulation.
Of all the structures used to assemble the knee, this thin layer of glistening articular cartilage tissue is probably the most important and the most interesting. Its intricate hierarchical structure and remarkable biomechanical resilience are subjects of ongoing research and therapeutic innovation. Preservation and restoration of its integrity are paramount surgical goals in addressing articular surface pathology.
Magnified view emphasizing the pristine appearance of articular cartilage, highlighting its smooth, resilient texture essential for efficient biomechanical function within the synovial joint.
Menisci
The menisci are two crescent-shaped (medial) and nearly circular (lateral) fibrocartilaginous structures interposed between the femoral condyles and the tibial plateau. They are wedge-shaped in cross-section, with a thicker peripheral margin and a thin, free inner edge.
- Medial Meniscus: This C-shaped structure is firmly attached to the medial joint capsule, the coronary ligaments (connecting it to the tibia), and the deep layer of the medial collateral ligament (dMCL). This strong capsular attachment renders it relatively immobile and thus more susceptible to tearing. Its anterior horn attaches anterior to the ACL insertion, and its posterior horn attaches posterior to the PCL insertion.
- Lateral Meniscus: This more O-shaped structure is less firmly attached to the joint capsule, lacking a direct attachment to the lateral collateral ligament (LCL). It also possesses a distinct hiatus for the popliteus tendon, which further contributes to its greater mobility. Its anterior horn attaches anterior to the medial tibial spine, and its posterior horn attaches anterior to the PCL insertion.
Now we are ready to add the meniscus cartilages, which sit like two rubbery, horseshoe-shaped pads on the surface of the tibia. The menisci are composed of fibrocartilage, primarily type I collagen, and function crucially in knee biomechanics. The exact role that the meniscus cartilages play in the function of the knee is sometimes underestimated, but the two wedge-shaped pieces of fibrocartilage act as crucial shock absorbers between your femur and tibia. These are the menisci. The menisci help to transmit weight from one bone to another by increasing the tibiofemoral contact area by up to 50%, thereby reducing contact stresses on the articular cartilage. They also play an important role in knee stability by deepening the tibial plateau, guiding femoral condyle movement, and contributing to joint lubrication and proprioception. The vascular supply to the menisci is limited to the peripheral 10-30% (the "red zone"), which influences healing potential, while the inner two-thirds (the "white zone") are avascular.
Schematic representation of the menisci positioned on the tibial plateau, illustrating their characteristic shapes and anatomical placement between the articulating femoral and tibial surfaces, fulfilling their role as crucial load-bearing structures.
Ligamentous Stabilizers
The static stability of the knee is predominantly provided by a complex network of intra-articular cruciate ligaments and extra-articular collateral and capsular ligaments.
-
Cruciate Ligaments:
- Anterior Cruciate Ligament (ACL): Originating from the posteromedial aspect of the lateral femoral condyle (within the intercondylar notch), it traverses anteriorly, medially, and distally to insert onto the anterior intercondylar area of the tibia, anterior and lateral to the medial tibial spine. The ACL is the primary restraint to anterior translation of the tibia relative to the femur and a secondary restraint to valgus, varus, and rotatory forces. It consists of two functional bundles: the larger anteromedial (AM) bundle , which is taut in flexion, and the smaller posterolateral (PL) bundle , which is taut in extension.
- Posterior Cruciate Ligament (PCL): The strongest ligament in the knee, it originates from the lateral aspect of the medial femoral condyle (within the intercondylar notch) and courses posteriorly, laterally, and distally to insert onto the posterior intercondylar area of the tibia, approximately 1 cm distal to the joint line. The PCL is the primary restraint to posterior translation of the tibia relative to the femur. It also comprises two bundles: the larger anterolateral (AL) bundle , taut in flexion, and the smaller posteromedial (PM) bundle , taut in extension.
-
Collateral Ligaments:
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
This broad, flat ligament is composed of superficial (sMCL) and deep (dMCL) layers.
- Superficial MCL (sMCL): Originates from the medial femoral epicondyle and inserts broadly onto the medial aspect of the tibia approximately 5-7 cm distal to the joint line, deep to the pes anserinus tendons. It is the primary static restraint to valgus stress, particularly in full extension.
- Deep MCL (dMCL): These are thickenings of the medial joint capsule, comprising the meniscofemoral and meniscotibial ligaments, which connect the medial meniscus to the femur and tibia, respectively. They act as secondary valgus stabilizers and contribute to meniscal stability.
- Lateral Collateral Ligament (LCL) / Fibular Collateral Ligament (FCL): A distinct, cord-like structure originating from the lateral femoral epicondyle and inserting onto the fibular head. Crucially, the LCL is entirely extra-articular and separate from the joint capsule. It is the primary static restraint to varus stress, particularly in full extension.
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
This broad, flat ligament is composed of superficial (sMCL) and deep (dMCL) layers.
-
Posterolateral Corner (PLC): This anatomically complex region consists of multiple synergistic structures providing stability against varus, external rotation, and posterior translation. Key components include:
- The LCL.
- The popliteus tendon (originating from the lateral femoral epicondyle and inserting onto the posterior tibia).
- The popliteofibular ligament (connecting the popliteus muscle to the fibular head).
- The arcuate ligament complex, which includes the arcuate ligament, fabellofibular ligament (if a fabella is present), and the lateral gastrocnemius tendon.
- The posterolateral joint capsule.
-
Patellofemoral Ligaments:
- Medial Patellofemoral Ligament (MPFL): The most crucial medial soft tissue restraint to lateral patellar displacement. It originates from the adductor tubercle region of the medial femoral condyle and inserts onto the superomedial aspect of the patella.
- Lateral Patellofemoral Ligament (LPFL): A less distinct ligamentous structure contributing to lateral patellar stability and resisting excessive medial patellar translation.
Tendons and Muscles
Dynamic stability and motion of the knee are governed by various tendinous and muscular structures:
*
Quadriceps Tendon:
The conjoined tendon of the quadriceps femoris muscles (rectus femoris, vastus medialis, vastus intermedius, vastus lateralis) inserting onto the superior pole of theella.
*
Patellar Tendon (Ligament):
The continuation of the quadriceps tendon, extending from the inferior pole of the patella to the tibial tuberosity.
*
Hamstring Tendons:
The semitendinosus and gracilis tendons (medially) form the pes anserinus group (along with the sartorius), inserting onto the anteromedial aspect of the proximal tibia. The biceps femoris tendon (laterally) inserts primarily onto the fibular head. These muscles are primary knee flexors and secondary rotators.
*
Popliteus Tendon:
This tendon crosses the posterolateral corner, originating from the lateral femoral epicondyle and inserting onto the posterior tibia. Its primary action is to internally rotate the tibia on the femur, thereby "unlocking" the knee from full extension, and it contributes significantly to posterolateral stability.
*
Gastrocnemius Tendons:
The medial and lateral heads originate from the posterior aspects of the respective femoral condyles, contributing to knee flexion and ankle plantarflexion.
Neurovascular Structures
The popliteal fossa, located posteriorly, is a critical anatomical region containing the major neurovascular structures supplying the distal lower extremity. These structures are highly vulnerable during posterior surgical approaches or in the context of high-energy knee trauma (e.g., knee dislocations).
*
Popliteal Artery:
The direct continuation of the superficial femoral artery, passing through the adductor hiatus into the popliteal fossa. It is the deepest structure in the fossa, lying directly on the posterior aspect of the joint capsule and then on the popliteus muscle. Distally, it bifurcates into the anterior tibial artery and the tibioperoneal trunk.
*
Popliteal Vein:
Located superficial (anterior) to the popliteal artery.
*
Tibial Nerve:
The most superficial (posterior) structure of the neurovascular bundle in the popliteal fossa, medial to the common peroneal nerve. It provides motor innervation to the posterior compartment muscles of the leg and sensory innervation to the sole of the foot.
*
Common Peroneal Nerve:
Courses laterally within the popliteal fossa, wrapping around the fibular neck where it is highly superficial and susceptible to injury from direct trauma, compartment syndrome, or iatrogenic damage during lateral knee procedures. It divides into the superficial and deep peroneal nerves, innervating the lateral and anterior compartment muscles, respectively.
Biomechanics
The knee joint's biomechanics are an intricate symphony of rolling, gliding, and rotational movements, orchestrated by the congruence of its articular surfaces, the constraint provided by ligaments, and the dynamic forces generated by muscles.
*
Flexion and Extension:
Primarily occur in the sagittal plane. During early flexion, the femoral condyles roll posteriorly on the tibial plateau. As flexion progresses, anterior gliding of the femur occurs to prevent posterior impingement and dislocate the menisci. The "screw-home mechanism" describes the obligatory external rotation of the tibia (or internal rotation of the femur) that occurs during the terminal 10-15 degrees of knee extension in non-weight-bearing. This locks the knee into its most stable position, maximizing articular congruity. It is primarily driven by the asymmetry of the femoral condyles, the tensioning of the ACL, and passive capsular restraints.
*
Rotation:
Axial rotation is minimal in full extension but increases significantly as the knee flexes. This rotation is constrained by the cruciate ligaments, with the ACL resisting internal rotation and the PCL resisting external rotation.
*
Load Transmission:
The menisci play a critical role in load distribution, transforming the incongruent tibiofemoral articulation into a more congruent system, thereby significantly reducing peak contact stresses on the articular cartilage. The patella, embedded in the quadriceps mechanism, optimizes the lever arm of the quadriceps, enhancing its efficiency in generating extensor force.
Indications & Contraindications
The decision-making process for surgical intervention in knee pathology is multifaceted, relying heavily on a precise understanding of the underlying anatomical derangement, its biomechanical implications, patient-specific factors, and anticipated functional recovery. General indications often stem from significant structural instability, irreparable mechanical symptoms, progressive degenerative changes, or failed non-operative management. Contraindications typically include active infection, severe peripheral vascular disease, uncontrolled systemic comorbidities, or conditions precluding rehabilitation adherence.
The following table summarizes general operative and non-operative indications, acknowledging that specific decision points are highly dependent on the particular pathology (e.g., ACL rupture vs. meniscal tear vs. OA).
| Condition Category | Non-Operative Indications ## Introduction & Epidemiology
The knee joint, anatomically categorized as a modified hinge synovial joint, is a biomechanically sophisticated structure essential for ambulation, load bearing, and kinetic chain function. Its stability and mobility are functions of its intricate ligamentous architecture, meniscal morphology, and osseous congruity, synergistically complemented by dynamic muscular stabilization. A profound and granular understanding of its anatomy is not merely academic but directly applicable to differential diagnosis, operative planning, and efficacious execution of surgical procedures.
Epidemiologically, knee pathologies represent a significant burden on global healthcare systems. Osteoarthritis (OA) of the knee is a pervasive degenerative condition, with a prevalence exceeding 30% in individuals over 65 years, and is a leading cause of disability worldwide. Traumatic injuries, encompassing ligamentous tears (e.g., anterior cruciate ligament (ACL), posterior cruciate ligament (PCL)), meniscal lesions, and periarticular fractures, are common, particularly in young active and athletic populations, as well as following high-energy trauma. The incidence of ACL rupture, for example, is reported to be between 100,000 and 200,000 cases annually in the United States alone. Meniscal tears affect approximately 60-70 individuals per 100,000 person-years, demonstrating a bimodal distribution with peaks in younger, acutely injured patients and older individuals with degenerative tears. Given the high prevalence and diverse etiology of knee disorders, a mastery of knee anatomy is paramount for all orthopedic specialists.
Surgical Anatomy & Biomechanics
A systematic approach to knee anatomy, conceptualized as a deconstruction and reconstruction of its components, provides the most comprehensive surgical reference. This section details the osseous elements, articular surfaces, fibrocartilaginous structures, ligamentous and tendinous stabilizers, and the critical neurovascular bundles, elucidating their respective biomechanical contributions.
Osseous Architecture
The knee joint is principally formed by the distal femur and proximal tibia. The patella, a sesamoid bone, is an integral component of the extensor mechanism. The proximal fibula, while not directly articulating with the femorotibial joint, serves as a crucial anatomical landmark and attachment site for key ligamentous and tendinous structures.
-
Distal Femur: The distal femur features two prominent condyles, medial and lateral, separated posteriorly by the intercondylar notch. These condyles are asymmetric, a critical factor in knee kinematics.
- Medial Femoral Condyle: Characteristically larger, longer, and more curved in the sagittal plane. It projects further distally than the lateral condyle, contributing to the physiological valgus alignment of the knee. The medial epicondyle serves as the primary femoral attachment for the superficial medial collateral ligament (sMCL). Superior to this, the adductor tubercle is a key landmark, serving as the insertion of the adductor magnus tendon and a critical reference point for medial patellofemoral ligament (MPFL) reconstruction.
- Lateral Femoral Condyle: Possesses a flatter articular surface anteriorly and a less pronounced sagittal curvature compared to the medial condyle. The lateral epicondyle is the origin for the lateral collateral ligament (LCL) and the popliteus tendon. A distinct posterodistal sulcus for the popliteus tendon is an important anatomical feature of the posterolateral corner (PLC).
- Intercondylar Notch: This deep, U-shaped groove between the femoral condyles houses the intra-articular anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). The intercondylar roof, or notch roof, dictates the sagittal angle of the ACL.
- Trochlear Groove: Situated anteriorly, this patellar articulating surface is formed by the confluence of the anterior aspects of the femoral condyles. Its depth, congruence, and orientation are fundamental determinants of patellar tracking and patellofemoral stability.
-
Proximal Tibia: The proximal tibia expands into the tibial plateau, which comprises two articular facets.
- Medial Tibial Plateau: Larger, oval, and distinctly concave, articulating with the medial femoral condyle. Its contour provides greater stability against femoral translation.
- Lateral Tibial Plateau: Smaller, more circular, and often slightly convex or flatter than the medial plateau, articulating with the lateral femoral condyle. It is generally positioned slightly superior to the medial plateau.
- Intercondylar Eminence: Located centrally between the articular facets, consisting of medial and lateral tibial spines. These prominences serve as critical attachment points for the menisci and cruciate ligaments (e.g., ACL attachment anterior to the medial spine, PCL attachment posterior to the lateral spine).
- Tibial Tuberosity: An anterior bony prominence that serves as the distal insertion site for the patellar tendon.
- Gerdy's Tubercle: Located on the anterolateral aspect of the proximal tibia, this is the insertion point for the iliotibial band (ITB).
-
Patella: The largest sesamoid bone, fully encapsulated within the quadriceps femoris tendon. Its posterior surface is covered by the thickest articular cartilage in the body and articulates with the trochlear groove of the femur. Functionally, the patella acts as a mechanical fulcrum, significantly augmenting the extensor moment arm of the quadriceps muscle, thereby increasing its mechanical efficiency in knee extension. The superior pole receives the quadriceps tendon insertion, while the inferior pole serves as the origin of the patellar tendon (ligament).
Anatomical illustration depicting the primary osseous constituents of the knee joint—the distal femur, proximal tibia, and proximal fibula—arranged to demonstrate their intrinsic relationships and topographical alignment, forming the skeletal foundation for the knee.
Articular Cartilage
The articular surfaces of the distal femur, proximal tibia, and posterior patella are coated by hyaline articular cartilage. This specialized connective tissue, typically 2-4 mm in thickness, is an avascular, alymphatic, and aneural structure composed primarily of chondrocytes embedded within an extracellular matrix rich in type II collagen and proteoglycans (predominantly aggrecan).
The biomechanical functions of articular cartilage are pivotal for normal joint function:
*
Friction Reduction:
It provides an exceptionally smooth, low-friction articulating surface, facilitating unimpeded joint motion. The coefficient of friction in healthy articular cartilage is among the lowest observed in biological systems.
*
Load Distribution:
It acts as a resilient, viscoelastic medium that distributes compressive loads over a wide contact area, thereby mitigating peak stresses on the underlying subchondral bone. This property protects the osseous structures from excessive mechanical wear.
The inherent limited capacity for intrinsic repair of articular cartilage renders it highly susceptible to progressive degeneration following traumatic insults or chronic mechanical overload, frequently leading to the insidious progression of osteoarthritis. Surgical strategies often prioritize its preservation, repair, or regeneration.
A detailed view illustrating the articular cartilage as a contiguous, smooth layer enveloping the articulating surfaces of the femoral condyles and tibial plateau. This initial soft tissue component is critical for facilitating frictionless motion and distributing axial loads.
Of all the structures used to assemble the knee, this thin layer of glistening articular cartilage tissue is probably the most important and the most interesting. Its unique tribological properties, anisotropic and inhomogeneous mechanical characteristics, and critical role in joint homeostasis are subjects of extensive orthopedic and biomedical research. The functional integrity of this tissue is a direct determinant of long-term joint health.
High-fidelity depiction of the articular cartilage surface, emphasizing its characteristic glistening appearance and structural integrity, essential for its role in reducing friction and dissipating impact forces within the joint.
Menisci
The menisci comprise two semilunar (medial) and nearly circular (lateral) fibrocartilaginous pads positioned on the tibial plateau, interposed between the femoral condyles and tibial articular facets. These structures are wedge-shaped in sagittal cross-section, with a thicker peripheral margin and a thin, free inner edge.
- Medial Meniscus: This C-shaped structure is firmly attached to the medial joint capsule, the coronary ligaments (meniscotibial ligaments), and the deep layer of the medial collateral ligament (dMCL). This strong capsular and ligamentous tethering renders it relatively immobile and consequently more prone to injury, particularly in conjunction with MCL lesions. Its anterior horn attaches anterior to the ACL insertion, and its posterior horn attaches posterior to the PCL insertion.
- Lateral Meniscus: This more O-shaped structure is less firmly attached to the joint capsule, lacking a direct attachment to the LCL, and possesses a distinct hiatus for the popliteus tendon. This greater mobility confers some protective advantage against acute tearing but does not preclude injury. Its anterior horn attaches anterior to the medial tibial spine, and its posterior horn attaches anterior to the PCL insertion.
Now we are ready to add the meniscus cartilages, which sit like two rubbery, horseshoe-shaped pads on the surface of the tibia. The menisci are composed primarily of type I collagen fibrocartilage. The exact role that the meniscus cartilages play in the function of the knee is poorly understood by some, but the two wedge-shaped pieces of fibrocartilage act as crucial shock absorbers between your femur and tibia. These are the menisci. The menisci contribute significantly to increasing the tibiofemoral contact area by up to 50%, thereby reducing peak contact stresses on the articular cartilage. They also play an important role in knee stability by deepening the tibial plateau, guiding femoral condyle translation, and contributing to joint lubrication and proprioception. The peripheral 10-30% of the menisci (the "red zone") is vascularized by genicular arteries, affording some capacity for healing, whereas the inner two-thirds (the "white zone") are avascular, typically necessitating surgical debridement or specialized repair techniques.
Depiction of the menisci accurately positioned on the tibial plateau, illustrating their semi-lunar morphology and strategic placement as essential load-bearing and stabilizing structures within the femorotibial joint.
Ligamentous Stabilizers
The static stability of the knee is primarily conferred by a complex array of intra-articular cruciate ligaments and extra-articular collateral and capsular ligaments.
-
Cruciate Ligaments:
- Anterior Cruciate Ligament (ACL): Originates from the posteromedial aspect of the lateral femoral condyle within the intercondylar notch. It courses anteriorly, medially, and distally to insert onto the anterior intercondylar area of the tibia, anterior and lateral to the medial tibial spine. The ACL is the principal restraint to anterior translation of the tibia relative to the femur and a secondary restraint to valgus, varus, and rotatory forces. It comprises two functional bundles: the larger anteromedial (AM) bundle , which is taut in flexion, and the smaller posterolateral (PL) bundle , which is taut in extension.
- Posterior Cruciate Ligament (PCL): The strongest ligament in the knee, originating from the lateral aspect of the medial femoral condyle within the intercondylar notch. It courses posteriorly, laterally, and distally to insert onto the posterior intercondylar area of the tibia, approximately 1 cm distal to the joint line. The PCL is the primary restraint to posterior translation of the tibia relative to the femur. It also comprises two functional bundles: the larger anterolateral (AL) bundle , taut in flexion, and the smaller posteromedial (PM) bundle , taut in extension.
-
Collateral Ligaments:
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
This broad, flat ligament consists of superficial (sMCL) and deep (dMCL) layers.
- Superficial MCL (sMCL): Originates from the medial femoral epicondyle, approximately 3-5 mm proximal to the joint line, and inserts broadly onto the medial aspect of the tibia approximately 5-7 cm distal to the joint line, beneath the pes anserinus. It is the primary static restraint to valgus stress, particularly in full extension.
- Deep MCL (dMCL): These are thickenings of the medial joint capsule, comprising the meniscofemoral (proximal) and meniscotibial (distal) ligaments, which anchor the medial meniscus to the femur and tibia, respectively. They act as secondary valgus stabilizers and contribute to medial meniscal stability.
- Lateral Collateral Ligament (LCL) / Fibular Collateral Ligament (FCL): A distinct, cord-like, extra-articular structure. It originates from the lateral femoral epicondyle, proximal to the popliteus tendon origin, and inserts onto the fibular head. The LCL is the primary static restraint to varus stress, particularly in full extension, and is an integral component of the posterolateral corner.
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
This broad, flat ligament consists of superficial (sMCL) and deep (dMCL) layers.
-
Posterolateral Corner (PLC): This anatomically intricate region is a complex of synergistic structures providing critical stability against varus, external rotation, and posterior translation forces. Key components include:
- The LCL.
- The popliteus tendon (originating from the lateral femoral epicondyle and inserting onto the posterior proximal tibia).
- The popliteofibular ligament (connecting the popliteus muscle-tendon unit to the fibular head).
- The arcuate ligament complex, which encompasses the arcuate ligament, the fabellofibular ligament (if a fabella is present), and the lateral gastrocnemius tendon.
- The posterolateral joint capsule.
-
Patellofemoral Ligaments:
- Medial Patellofemoral Ligament (MPFL): The most significant medial soft tissue restraint to lateral patellar displacement. It originates from the adductor tubercle and the medial femoral epicondyle, inserting onto the superomedial aspect of the patella.
- Lateral Patellofemoral Ligament (LPFL): A less distinct ligamentous thickening of the lateral retinaculum that contributes to lateral patellar stability and resists excessive medial patellar translation.
Tendons and Muscles
Dynamic stability and comprehensive motion of the knee joint are governed by various tendinous and muscular structures:
*
Quadriceps Tendon:
The confluence of the rectus femoris, vastus medialis, vastus intermedius, and vastus lateralis tendons, inserting onto the superior pole of the patella.
*
Patellar Tendon (Ligament):
The direct continuation of the quadriceps tendon, extending from the inferior pole of the patella to the tibial tuberosity.
*
Hamstring Tendons:
Medially, the semitendinosus and gracilis tendons, along with the sartorius, form the pes anserinus, inserting onto the anteromedial aspect of the proximal tibia. Laterally, the biceps femoris tendon inserts primarily onto the fibular head. These muscles are primary knee flexors and secondary rotators.
*
Popliteus Tendon:
This tendon originates from the lateral femoral epicondyle, courses deep to the LCL, and inserts onto the posterior aspect of the proximal tibia. Its primary action is to internally rotate the tibia on the femur, thereby "unlocking" the knee from full extension, and it contributes significantly to posterolateral stability.
*
Gastrocnemius Tendons:
The medial and lateral heads originate from the posterior aspects of the respective femoral condyles, contributing to knee flexion and ankle plantarflexion.
Neurovascular Structures
The popliteal fossa, a diamond-shaped anatomical space located posterior to the knee joint, contains the major neurovascular structures supplying the distal lower extremity. These structures are profoundly vulnerable to injury during posterior surgical approaches or in the context of high-energy knee trauma, such as knee dislocations.
*
Popliteal Artery:
The direct continuation of the superficial femoral artery, passing through the adductor hiatus into the popliteal fossa. It is the deepest structure within the fossa, lying directly on the posterior aspect of the joint capsule and then on the popliteus muscle. Distally, it bifurcates into the anterior tibial artery and the tibioperoneal trunk (which subsequently gives rise to the posterior tibial and peroneal arteries).
*
Popliteal Vein:
Located superficial (anterior) to the popliteal artery within the fossa.
*
Tibial Nerve:
The most superficial (posterior) structure of the neurovascular bundle in the popliteal fossa, typically medial to the common peroneal nerve. It provides motor innervation to the posterior compartment muscles of the leg and sensory innervation to the sole of the foot.
*
Common Peroneal Nerve:
Courses laterally within the popliteal fossa, wrapping superficially around the fibular neck where it is highly vulnerable to compression, direct trauma, or iatrogenic injury during lateral knee surgical procedures. It divides into the superficial and deep peroneal nerves, innervating the lateral and anterior compartment muscles, respectively.
Biomechanics
The knee joint's biomechanics are characterized by a sophisticated interplay of rolling, gliding, and rotational movements, meticulously orchestrated by the congruence of its articular surfaces, the stabilizing constraints of its ligaments, and the dynamic forces generated by surrounding musculature.
*
Flexion and Extension:
These movements primarily occur in the sagittal plane. During early flexion, the femoral condyles roll posteriorly on the tibial plateau. As flexion progresses, an anterior gliding of the femur occurs to prevent posterior impingement and meniscal displacement. The "screw-home mechanism" describes the obligatory external rotation of the tibia (or internal rotation of the femur) that occurs during the terminal 10-15 degrees of knee extension in a non-weight-bearing knee. This phenomenon maximizes joint congruity and stability in full extension, primarily driven by the asymmetry of the femoral condyles, the tensioning of the ACL, and passive capsular and ligamentous restraints.
*
Rotation:
Axial rotation is minimal in full extension but significantly increases as the knee flexes. This rotation is primarily constrained by the cruciate ligaments, with the ACL resisting internal rotation and the PCL resisting external rotation.
*
Load Transmission:
The menisci play a crucial role in load distribution, transforming the incongruent tibiofemoral articulation into a more congruent system. This effectively increases the tibiofemoral contact area, thereby significantly reducing peak contact stresses on the articular cartilage. The patella, embedded within the quadriceps mechanism, optimizes the lever arm of the quadriceps, thereby enhancing its efficiency in generating extensor force.
Indications & Contraindications
The judicious selection of operative versus non-operative management for knee pathologies is a critical decision-making process underpinned by a comprehensive understanding of knee anatomy, injury biomechanics, patient-specific factors, and anticipated functional outcomes. General indications for operative intervention typically include structural instability, persistent mechanical symptoms (e.g., locking, catching), progressive degenerative changes unresponsive to conservative measures, or acute injuries with high functional impairment. Contraindications may encompass active systemic or local infection, severe peripheral vascular disease, uncontrolled systemic comorbidities (e.g., diabetes, cardiac disease), or patient factors precluding adherence to rigorous post-operative rehabilitation protocols.
The following table provides a generalized framework for operative and non-operative indications, acknowledging that specific treatment algorithms are highly dependent on the precise pathology, patient age, activity level, and functional goals.
| Indication Category | Operative Management ## Introduction & Epidemiology
The knee joint, anatomically classified as a modified hinge, represents the largest and most complex articulation in the human body. Its intricate functional anatomy, encompassing an elaborate framework of osseous structures, robust ligamentous stabilizers, unique fibrocartilaginous menisci, and a specialized articular cartilage, permits significant range of motion while maintaining inherent stability crucial for ambulation and daily activities. For the orthopedic surgeon and medical educator, a nuanced three-dimensional understanding of knee anatomy and its underlying biomechanics is not only foundational but paramount for accurate diagnosis, meticulous surgical planning, precise execution of procedures, and ultimately, optimizing long-term patient outcomes.
Epidemiologically, knee pathologies constitute an increasing global health burden. Degenerative joint disease, predominantly osteoarthritis (OA), remains a leading cause of chronic pain and functional disability, with its prevalence increasing with age and associated comorbidities such as obesity. Estimates suggest symptomatic knee OA affects over 30% of individuals above 65 years. Traumatic injuries, including acute ligamentous ruptures (e.g., anterior cruciate ligament (ACL), posterior cruciate ligament (PCL)), meniscal tears, and periarticular fractures, are common, especially in athletic populations and following high-energy trauma. The annual incidence of ACL injuries in the United States alone ranges from 100,000 to 200,000 cases. Meniscal lesions exhibit a bimodal distribution, affecting younger, active individuals through acute trauma and older patients through degenerative processes, with an annual incidence of approximately 60-70 per 100,000 individuals. These compelling epidemiological data underscore the critical necessity for a comprehensive and continually updated understanding of knee anatomy and its implications for clinical practice.
Surgical Anatomy & Biomechanics
A systematic approach to understanding the knee's components, akin to a structured dissection, is essential for its surgical revelation. This section details the osseous architecture, articular cartilage, meniscal structures, ligamentous and tendinous stabilizers, and crucial neurovascular bundles, elucidating their respective biomechanical contributions and surgical relevance.
Osseous Architecture
The knee joint is formed by the articulation of the distal femur and proximal tibia. The patella acts as a sesamoid bone within the extensor mechanism. The proximal fibula, while not directly articulating within the primary tibiofemoral joint, is an indispensable anatomical landmark due to its ligamentous and tendinous attachments influencing knee stability.
-
Distal Femur: The distal femur terminates in two large condyles, medial and lateral, separated posteriorly by the intercondylar notch. These condyles are notably asymmetric, a key feature contributing to the knee's complex kinematics.
- Medial Femoral Condyle: Characteristically larger, longer, and possessing a greater curvature in the sagittal plane compared to its lateral counterpart. It projects more distally, contributing to the physiological valgus alignment of the knee. The medial epicondyle serves as the primary femoral attachment for the superficial medial collateral ligament (sMCL). Superior to this, the adductor tubercle is a critical landmark, serving as the insertion of the adductor magnus tendon and a consistent reference point for medial patellofemoral ligament (MPFL) reconstruction.
- Lateral Femoral Condyle: Features a flatter articular surface anteriorly and a less pronounced sagittal curvature. The lateral epicondyle is the origin for the lateral collateral ligament (LCL) and the popliteus tendon. A distinct posterodistal sulcus, or groove, for the popliteus tendon is an important anatomical feature, crucial for understanding posterolateral corner (PLC) anatomy and its surgical reconstruction.
- Intercondylar Notch: This deep, U-shaped osseous depression between the femoral condyles houses the intra-articular anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). The roof of the notch, or "intercondylar roof," influences the sagittal orientation of the ACL, a factor in impingement syndromes post-reconstruction.
- Trochlear Groove: Located anteriorly, this concave articular surface is formed by the confluence of the anterior aspects of the femoral condyles and articulates with the patella. Its depth, congruence, and orientation are fundamental determinants of patellar tracking and patellofemoral stability. Dysplasia of the trochlear groove is a significant factor in patellar instability.
-
Proximal Tibia: The proximal tibia expands into the tibial plateau, which comprises two distinct articular facets separated by the intercondylar eminence.
- Medial Tibial Plateau: Larger, oval-shaped, and distinctly concave, articulating with the medial femoral condyle. Its contour provides inherent stability against femoral translation. This facet is typically 50% larger than the lateral.
- Lateral Tibial Plateau: Smaller, more circular, and often slightly convex or flatter than the medial plateau, articulating with the lateral femoral condyle. It is generally positioned slightly superior to the medial plateau.
- Intercondylar Eminence: Located centrally between the articular facets, consisting of medial and lateral tibial spines. These prominences serve as critical attachment points for the menisci and cruciate ligaments (e.g., ACL attachment anterior to the medial spine, PCL attachment posterior to the lateral spine).
- Tibial Tuberosity: An anterior bony prominence situated approximately 2-3 cm distal to the joint line, serving as the distal insertion site for the patellar tendon. Its relationship to the trochlear groove (TT-TG distance) is a key measurement in patellofemoral instability assessment.
- Gerdy's Tubercle: Located on the anterolateral aspect of the proximal tibia, this serves as the primary insertion point for the iliotibial band (ITB).
-
Patella: The largest sesamoid bone, fully encapsulated within the quadriceps femoris tendon. Its posterior surface is covered by the thickest articular cartilage in the human body (up to 7 mm) and articulates with the trochlear groove of the femur. Functionally, the patella acts as a mechanical fulcrum, significantly augmenting the extensor moment arm of the quadriceps muscle, thereby increasing its mechanical efficiency in knee extension. The superior pole receives the quadriceps tendon insertion, while its inferior pole serves as the origin of the patellar tendon (ligament).
Anatomical illustration depicting the primary osseous constituents of the knee joint—the distal femur, proximal tibia, and proximal fibula—arranged to demonstrate their intrinsic relationships and topographical alignment, forming the skeletal foundation for the knee.
Articular Cartilage
The articulating surfaces of the distal femur, proximal tibia, and posterior patella are coated by hyaline articular cartilage. This specialized connective tissue, typically 2-4 mm in thickness (up to 7mm on the patella), is an avascular, alymphatic, and aneural structure composed primarily of chondrocytes embedded within an extracellular matrix rich in type II collagen (providing tensile strength) and proteoglycans (primarily aggrecan, responsible for compressive stiffness).
The biomechanical functions of articular cartilage are pivotal for normal joint function and longevity:
*
Friction Reduction:
It provides an exceptionally smooth, low-friction articulating surface, facilitating unimpeded joint motion. The coefficient of friction in healthy articular cartilage is among the lowest observed in biological systems, significantly lower than that of ice on ice.
*
Load Distribution:
It acts as a resilient, viscoelastic medium that distributes compressive loads over a wide contact area, thereby mitigating peak stresses on the underlying subchondral bone. This property protects the osseous structures from excessive mechanical wear and fatigue failure.
The inherent limited capacity for intrinsic repair of articular cartilage renders it profoundly susceptible to progressive degeneration following traumatic insults (e.g., osteochondral fractures) or chronic mechanical overload, frequently leading to the insidious progression of osteoarthritis. Surgical strategies often prioritize its preservation, repair (e.g., microfracture, OATS), or regeneration (e.g., MACI).
A detailed view illustrating the articular cartilage as a contiguous, smooth layer enveloping the articulating surfaces of the femoral condyles and tibial plateau. This initial soft tissue component is critical for facilitating frictionless motion and distributing axial loads.
Of all the structures used to assemble the knee, this thin layer of glistening articular cartilage tissue is probably the most important and the most interesting. Its intricate hierarchical structure, anisotropic and inhomogeneous mechanical characteristics, and critical role in joint homeostasis are subjects of extensive orthopedic and biomedical research. The functional integrity of this tissue is a direct determinant of long-term joint health and patient quality of life, emphasizing its surgical significance.
High-fidelity depiction of the articular cartilage surface, emphasizing its characteristic glistening appearance and structural integrity, essential for its role in reducing friction and dissipating impact forces within the joint.
Menisci
The menisci comprise two semilunar (medial) and nearly circular (lateral) fibrocartilaginous pads positioned on the tibial plateau, interposed between the femoral condyles and tibial articular facets. These structures are wedge-shaped in sagittal cross-section, with a thicker peripheral margin and a thin, free inner edge. Composed primarily of type I collagen, these structures are crucial for load management and joint stability.
- Medial Meniscus: This C-shaped structure is firmly attached to the medial joint capsule, the coronary ligaments (meniscotibial ligaments), and the deep layer of the medial collateral ligament (dMCL). This strong capsular and ligamentous tethering renders it relatively immobile and consequently more prone to injury, particularly in conjunction with MCL lesions (O'Donoghue's triad). Its anterior horn attaches anterior to the ACL insertion, and its posterior horn attaches posterior to the PCL insertion.
- Lateral Meniscus: This more O-shaped structure is less firmly attached to the joint capsule, lacking a direct attachment to the LCL. It also possesses a distinct hiatus for the popliteus tendon, which courses through the posterolateral capsule. This greater mobility confers some protective advantage against acute tearing but does not preclude injury. Its anterior horn attaches anterior to the medial tibial spine, and its posterior horn attaches anterior to the PCL insertion, often with meniscofemoral ligaments (Wrisberg and Humphry) connecting it to the PCL and femur.
Now we are ready to add the meniscus cartilages, which sit like two rubbery, horseshoe-shaped pads on the surface of the tibia. The exact role that the meniscus cartilages play in the function of the knee is sometimes underestimated, but the two wedge-shaped pieces of fibrocartilage act as crucial shock absorbers between your femur and tibia. These are the menisci. The menisci contribute significantly to increasing the tibiofemoral contact area by up to 50%, thereby reducing peak contact stresses on the articular cartilage. They also play an important role in knee stability by deepening the tibial plateau, guiding femoral condyle translation, and contributing to joint lubrication and proprioception. The peripheral 10-30% of the menisci (the "red zone") is vascularized by perimeniscal capillary plexuses from the genicular arteries, affording some capacity for healing, whereas the inner two-thirds (the "white zone") are avascular, typically necessitating surgical debridement or specialized repair techniques for tears extending into this zone. Loss of meniscal tissue significantly increases the risk of early tibiofemoral osteoarthritis.
Depiction of the menisci accurately positioned on the tibial plateau, illustrating their semi-lunar morphology and strategic placement as essential load-bearing and stabilizing structures within the femorotibial joint.
Ligamentous Stabilizers
The static stability of the knee is primarily conferred by a complex array of intra-articular cruciate ligaments and extra-articular collateral and capsular ligaments.
-
Cruciate Ligaments: These intra-articular ligaments are named for their tibial attachments and cross each other like an "X".
- Anterior Cruciate Ligament (ACL): Originates from the posteromedial aspect of the lateral femoral condyle within the intercondylar notch (the lateral femoral wall, specifically at a clockface position of approximately 10:30 for a right knee). It courses anteriorly, medially, and distally to insert onto the anterior intercondylar area of the tibia, anterior and lateral to the medial tibial spine. The ACL is the principal restraint to anterior translation of the tibia relative to the femur and a secondary restraint to valgus, varus, and rotatory forces (specifically internal rotation). It comprises two functional bundles: the larger anteromedial (AM) bundle , which is taut in flexion, and the smaller posterolateral (PL) bundle , which is taut in extension and limits rotatory instability.
- Posterior Cruciate Ligament (PCL): The strongest ligament in the knee, originating from the lateral aspect of the medial femoral condyle within the intercondylar notch (the medial femoral wall, at a clockface position of approximately 1:00 for a right knee). It courses posteriorly, laterally, and distally to insert onto the posterior intercondylar area of the tibia, approximately 1 cm distal to the joint line. The PCL is the primary restraint to posterior translation of the tibia relative to the femur. It also comprises two functional bundles: the larger anterolateral (AL) bundle , which is taut in flexion, and the smaller posteromedial (PM) bundle , which is taut in extension.
-
Collateral Ligaments: These extra-articular ligaments stabilize the knee against varus and valgus stresses.
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
This broad, flat ligament consists of superficial (sMCL) and deep (dMCL) layers.
- Superficial MCL (sMCL): Originates from the medial femoral epicondyle, approximately 3-5 mm proximal to the joint line, and inserts broadly onto the medial aspect of the tibia approximately 5-7 cm distal to the joint line, beneath the pes anserinus. It is the primary static restraint to valgus stress, particularly in full extension and 20-30 degrees of flexion.
- Deep MCL (dMCL): These are thickenings of the medial joint capsule, comprising the meniscofemoral (proximal) and meniscotibial (distal) ligaments, which anchor the medial meniscus to the femur and tibia, respectively. They act as secondary valgus stabilizers and contribute to medial meniscal stability.
- Lateral Collateral Ligament (LCL) / Fibular Collateral Ligament (FCL): A distinct, cord-like, extra-articular structure. It originates from the lateral femoral epicondyle, approximately 1.4 mm proximal and posterior to the popliteus tendon origin, and inserts onto the fibular head. The LCL is the primary static restraint to varus stress, particularly in full extension, and is an integral component of the posterolateral corner.
-
Medial Collateral Ligament (MCL) / Tibial Collateral Ligament (TCL):
This broad, flat ligament consists of superficial (sMCL) and deep (dMCL) layers.
-
Posterolateral Corner (PLC): This anatomically intricate region is a complex of synergistic structures providing critical stability against varus, external rotation, and posterior translation forces. Key components include:
- The LCL.
- The popliteus tendon (originating from the lateral femoral epicondyle at the popliteus sulcus and inserting onto the posterior proximal tibia).
- The popliteofibular ligament (connecting the popliteus muscle-tendon unit to the fibular head).
- The arcuate ligament complex, which encompasses the arcuate ligament (a Y-shaped thickening of the posterolateral capsule), the fabellofibular ligament (if a fabella is present), and the lateral gastrocnemius tendon.
- The posterolateral joint capsule. Injury to this complex often results in debilitating rotatory instability.
-
Patellofemoral Ligaments:
- Medial Patellofemoral Ligament (MPFL): The most significant medial soft tissue restraint to lateral patellar displacement. It originates from a broad area between the adductor tubercle and the medial femoral epicondyle, inserting onto the superomedial aspect of the patella. It provides 50-60% of the resistance to lateral patellar translation.
- Lateral Patellofemoral Ligament (LPFL): A less distinct ligamentous thickening of the lateral retinaculum that contributes to lateral patellar stability and resists excessive medial patellar translation.
Tendons and Muscles
Dynamic stability and comprehensive motion of the knee joint are governed by various tendinous and muscular structures, which also provide robust surgical graft options.
*
Quadriceps Tendon:
The conjoined tendon of the rectus femoris, vastus medialis, vastus intermedius, and vastus lateralis muscles, inserting onto the superior pole of the patella. It is the primary extensor of the knee.
*
Patellar Tendon (Ligament):
The direct continuation of the quadriceps tendon, extending from the inferior pole of the patella to the tibial tuberosity. It is a vital component of the extensor mechanism and a common autograft source for ACL reconstruction.
*
Hamstring Tendons:
Medially, the semitendinosus and gracilis tendons, along with the sartorius, form the pes anserinus, inserting onto the anteromedial aspect of the proximal tibia. These muscles are primary knee flexors and secondary rotators, and their tendons are frequently harvested for ACL reconstruction. Laterally, the biceps femoris tendon inserts primarily onto the fibular head and contributes to knee flexion and external tibial rotation.
*
Popliteus Tendon:
This tendon originates from the lateral femoral epicondyle, courses deep to the LCL, and inserts onto the posterior aspect of the proximal tibia. Its primary action is to internally rotate the tibia on the femur, thereby "unlocking" the knee from full extension, and it contributes significantly to posterolateral stability.
*
Gastrocnemius Tendons:
The medial and lateral heads originate from the posterior aspects of the respective femoral condyles, contributing to knee flexion and ankle plantarflexion. They also form part of the posterolateral and posteromedial capsule.
Neurovascular Structures
The popliteal fossa, a diamond-shaped anatomical space located posterior to the knee joint, is a critical region containing the major neurovascular structures supplying the distal lower extremity. These structures are profoundly vulnerable to injury during posterior surgical approaches or in the context of high-energy knee trauma, such as knee dislocations, where the risk of arterial injury can exceed 40%.
*
Popliteal Artery:
The direct continuation of the superficial femoral artery, passing through the adductor hiatus into the popliteal fossa. It is the deepest structure within the fossa, lying directly on the posterior aspect of the joint capsule and then on the popliteus muscle. Distally, it bifurcates into the anterior tibial artery and the tibioperoneal trunk (which subsequently gives rise to the posterior tibial and peroneal arteries).
*
Popliteal Vein:
Located superficial (anterior) to the popliteal artery within the fossa. It is formed by the confluence of the anterior tibial, posterior tibial, and peroneal veins.
*
Tibial Nerve:
The most superficial (posterior) structure of the neurovascular bundle in the popliteal fossa, typically medial to the common peroneal nerve. It provides motor innervation to the posterior compartment muscles of the leg and sensory innervation to the sole of the foot.
*
Common Peroneal Nerve:
Courses laterally within the popliteal fossa, wrapping superficially around the fibular neck where it is highly vulnerable to compression, direct trauma, or iatrogenic injury during lateral knee surgical procedures. It divides into the superficial and deep peroneal nerves, innervating the lateral and anterior compartment muscles, respectively. Careful identification and protection of this nerve are paramount in all lateral approaches.
Biomechanics
The knee joint's biomechanics are characterized by a sophisticated interplay of rolling, gliding, and rotational movements, meticulously orchestrated by the congruence of its articular surfaces, the stabilizing constraints of its ligaments, and the dynamic forces generated by surrounding musculature.
*
Flexion and Extension:
These movements primarily occur in the sagittal plane. During early flexion, the femoral condyles roll posteriorly on the tibial plateau. As flexion progresses, an anterior gliding of the femur occurs to prevent posterior impingement and meniscal displacement. The "screw-home mechanism" describes the obligatory external rotation of the tibia (or internal rotation of the femur) that occurs during the terminal 10-15 degrees of knee extension in a non-weight-bearing knee. This phenomenon, driven by the asymmetry of the femoral condyles, the tensioning of the ACL, and passive capsular/ligamentous restraints, locks the knee into its most stable position, maximizing articular congruity and energy efficiency during standing.
*
Rotation:
Axial rotation is minimal in full extension but significantly increases as the knee flexes. This rotation is primarily constrained by the cruciate ligaments, with the ACL resisting internal rotation and the PCL resisting external rotation. Disruption of these ligaments leads to pathological rotatory instability.
*
Load Transmission:
The menisci play a crucial role in load distribution, transforming the incongruent tibiofemoral articulation into a more congruent system. This effectively increases the tibiofemoral contact area, thereby significantly reducing peak contact stresses on the articular cartilage. The patella, embedded within the quadriceps mechanism, optimizes the lever arm of the quadriceps, enhancing its efficiency in generating extensor force by approximately 30%. Loss of any of these load-bearing components can lead to increased stress and subsequent degenerative changes.
Indications & Contraindications
The judicious selection of operative versus non-operative management for knee pathologies is a critical decision-making process underpinned by a comprehensive understanding of knee anatomy, injury biomechanics, patient-specific factors, and anticipated functional outcomes. General indications for operative intervention typically include structural instability, persistent mechanical symptoms (e.g., locking, catching), progressive degenerative changes unresponsive to conservative measures, or acute injuries with high functional impairment. Contraindications may encompass active systemic or local infection, severe peripheral vascular disease, uncontrolled systemic comorbidities (e.g., diabetes, cardiac disease), or patient factors precluding adherence to rigorous post-operative rehabilitation protocols.
The following table provides a generalized framework for operative and non-operative indications, acknowledging that specific treatment algorithms are highly dependent on the precise pathology, patient age, activity level, and functional goals.
| Condition Category | Operative Management | Non-Operative Management |
|---|---|---|
| Ligamentous Injuries | * ACL/PCL Rupture (Grades III/IV): Symptomatic instability, active patient, associated injuries, high-demand sport. | * ACL/PCL Rupture (Grade I/II): Mild instability, sedentary patient, no associated injuries, good compensatory strength. |
| * MCL/LCL Rupture (Grade III/IV): Multiligamentous injury, gross instability, avulsion fracture (often MCL Grade III isolated injuries managed non-operatively unless chronic instability). | * MCL/LCL Rupture (Grade I/II): Isolated injury, mild-moderate laxity, stable arc of motion, no functional instability. Immobilization and physiotherapy. | |
| Meniscal Lesions | * Symptomatic Tears: Mechanical symptoms (locking, catching), large tears in vascularized zones (e.g., peripheral longitudinal tears >1cm), unstable tears, failed non-operative management. | * Asymptomatic Tears: Incidental finding. |
| * Tears in "Red-Red" or "Red-White" Zone: Amenable to repair, especially in younger patients. | * Small, Stable Tears in "White-White" Zone: Minimal symptoms. | |
| * Radial/Root Tears: Loss of hoop stress function, amenable to repair/reconstruction. | * Degenerative Tears: Often managed with physiotherapy, NSAIDs, injections, unless persistent mechanical symptoms. | |
| Articular Cartilage | * Symptomatic Focal Defects (ICRS Grades III/IV): Persistent pain, mechanical symptoms, amenable to repair (e.g., microfracture, OATS, MACI). | * Asymptomatic Lesions: Incidental findings, Grade I/II lesions. |
| * Osteochondritis Dissecans (OCD): Unstable lesions, failed conservative care. | * Stable OCD Lesions: Managed with restricted weight-bearing, bracing. | |
| Patellofemoral Instability | * Recurrent Dislocations/Subluxations: Failed conservative management, significant MPFL injury/insufficiency, trochlear dysplasia, increased TT-TG distance. | * First-Time Dislocation (without significant osteochondral injury): Rehabilitation, bracing, activity modification. |
| Degenerative Arthritis | * End-Stage OA: Persistent pain, functional limitation, failed extensive non-operative management, reasonable bone stock (Total Knee Arthroplasty, Unicompartmental Knee Arthroplasty). | * Mild-Moderate OA: Physiotherapy, activity modification, weight loss, NSAIDs, intra-articular injections (corticosteroids, hyaluronic acid, PRP). |
| * Early/Moderate Unicompartmental OA with Malalignment: High Tibial Osteotomy (HTO) or Distal Femoral Osteotomy (DFO) in active patients. | * Severe Comorbidities: High surgical risk. | |
| Fractures | * Displaced/Unstable Intra-articular Fractures (Tibial Plateau, Distal Femur, Patella): ORIF for anatomical reduction and stable fixation. | * Non-displaced/Stable Fractures: Immobilization, protected weight-bearing. |
| Contraindications (General Surgical) | * Active local or systemic infection | * Uncontrolled severe systemic comorbidities (cardiac, pulmonary, renal, metabolic) |
| * Severe peripheral vascular disease limiting healing potential | * Poor patient compliance or inability to participate in rehabilitation | |
| * Insufficient bone stock for hardware fixation | * Symptom attribution solely to non-knee pathology | |
| * Severe soft tissue compromise |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are fundamental prerequisites for successful knee surgery, minimizing complications and optimizing surgical exposure.
Pre-Operative Planning
-
Imaging Review:
- Radiographs (X-rays): Standard weight-bearing anteroposterior (AP), lateral, Merchant (patellofemoral), and Rosenberg (45-degree flexion posteroanterior weight-bearing) views are essential to assess joint alignment, degenerative changes, osteophyte formation, joint space narrowing, and osseous lesions. Full-length standing alignment films are critical for osteotomy planning.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissue structures (ligaments, menisci, articular cartilage, synovium, bone marrow edema). High-resolution sequences provide detailed anatomical information crucial for diagnosing meniscal tears, ligamentous ruptures, osteochondral defects, and stress fractures.
- Computed Tomography (CT): Primarily used for assessing complex intra-articular fractures (e.g., tibial plateau, distal femur), characterizing patellofemoral morphology (e.g., trochlear dysplasia, TT-TG distance), and evaluating bone stock for revision arthroplasty. 3D reconstructions are invaluable for pre-contouring plates and planning reduction strategies.
- Surgical Templating: Essential for total knee arthroplasty (TKA), unicompartmental knee arthroplasty (UKA), and osteotomies. It allows for prediction of implant size, assessment of bone cuts, and restoration of mechanical axis. For ligament reconstruction, careful consideration of graft choice, tunnel placement, and fixation methods is documented.
- Patient-Specific Considerations: Assessment of patient age, activity level, comorbidities, previous surgeries, and rehabilitation potential. Communication with the patient regarding realistic expectations and potential outcomes is paramount.
- Equipment and Instrumentation: Ensuring availability of specialized instruments (e.g., arthroscopy tower, specific fixation devices, appropriate implants, graft harvesting tools) is crucial.
Patient Positioning
The most common position for elective knee surgery, particularly arthroscopy, TKA, and extensor mechanism procedures, is the
supine position
.
1.
Lower Extremity Preparation:
The operative leg is prepared circumferentially from the hip to the foot. A tourniquet is typically applied to the proximal thigh to provide a bloodless field, crucial for visualization. The contraindications and safe limits for tourniquet use must be strictly adhered to.
2.
Leg Holder:
A pneumatic leg holder or a mechanical post (e.g., for distraction in arthroscopy) can be used to stabilize the thigh, allowing the knee to be flexed and extended freely.
3.
Foot Positioning:
The foot may be placed in a sterile foot holder or draped free to allow dynamic manipulation of the joint.
4.
Padding:
Meticulous padding of all pressure points (e.g., heels, sacrum, ulnar nerve, common peroneal nerve at the fibular head) is mandatory to prevent nerve palsies or pressure sores.
5.
Alternative Positions:
*
Lateral Decubitus:
Less common, but can be used for specific lateral approaches or arthroscopic procedures if difficult access.
*
Prone:
Utilized for posterior knee approaches, such as PCL repair/reconstruction, posterior meniscal repairs, or excision of popliteal cysts. Careful padding of the chest, pelvis, and ankles is critical, along with vigilant monitoring of neurovascular structures.
Detailed Surgical Approach / Technique
This section focuses on the principles of surgical access to reveal knee anatomy, encompassing both arthroscopic and open techniques. The integration of specified images will be contextually described within these approaches.
General Principles of Dissection
Irrespective of the approach, meticulous dissection is paramount.
*
Skin Incision:
Optimal placement considers functional cosmesis, potential for extension, and avoidance of neurovascular structures. Initial incision depth extends through the epidermis and dermis.
*
Subcutaneous Dissection:
Careful elevation of skin flaps provides access to deeper structures. Identification and preservation of superficial nerves (e.g., infrapatellar branch of the saphenous nerve in medial approaches) are crucial.
*
Fascial Layers:
Incision of the deep fascia (e.g., fascia lata laterally, investing fascia medially) exposes muscles and their tendons.
*
Internervous Planes:
Whenever possible, surgical approaches should utilize internervous planes to minimize muscle denervation and preserve function. For example, the medial parapatellar approach for TKA utilizes the plane between the vastus medialis and the rectus femoris/medial retinaculum.

Illustrative image depicting the initial skin incision for an anterior knee approach, demonstrating careful planning for adequate exposure while considering anatomical landmarks and future wound healing. This forms the initial step in surgical revelation of deeper knee anatomy.
Arthroscopic Approach (Diagnostic and Therapeutic)
Arthroscopy provides a minimally invasive panoramic view of intra-articular knee anatomy, making it an invaluable tool for both diagnosis and treatment.
-
Portal Placement:
- Anterolateral (AL) Portal: Typically the primary viewing portal, located just lateral to the patellar tendon, at or slightly superior to the joint line. It allows visualization of the medial compartment, ACL, and patellofemoral joint.
- Anteromedial (AM) Portal: Often the primary working portal, located just medial to the patellar tendon, at a similar level to the AL portal. Used for instrumentation to address medial meniscal pathology, osteochondral lesions, and graft passage.
- Superomedial / Superolateral Portals: Accessory portals, usually higher up on the quadriceps pouch, used for fluid inflow, instrument retrieval, or addressing suprapatellar pathology.
- Posteromedial / Posterolateral Portals: Used for visualization or instrumentation of the posterior compartments, particularly for posterior meniscal horn pathology, loose bodies, or PCL evaluation.
-
Systematic Joint Inspection:
A consistent sequence of visualization ensures thorough assessment of all intra-articular structures.
- Patellofemoral Joint: Evaluate patellar tracking, trochlear groove morphology, and articular cartilage of the patella and trochlea.
- Medial Compartment: Assess the medial meniscus (anterior horn, body, posterior horn), medial articular cartilage (femoral and tibial), and MCL integrity (from within the joint, particularly the meniscofemoral and meniscotibial ligaments).
- Lateral Compartment: Assess the lateral meniscus (anterior horn, body, posterior horn, popliteal hiatus), lateral articular cartilage, and LCL/PLC integrity.
- Intercondylar Notch: Critically evaluate the ACL (integrity, tension, presence of residual fibers) and PCL. The integrity of both cruciate ligaments is assessed by direct visualization, probing, and dynamic stress testing.
- Probing and Palpation: An arthroscopic probe is used to dynamically assess the integrity, stability, and texture of menisci, articular cartilage, and ligamentous structures, providing tactile feedback beyond visual inspection. This technique is fundamental for defining the extent of tears or chondral defects.

Intra-articular arthroscopic view, illustrating the meticulous probing of a meniscal structure (likely medial meniscus posterior horn), demonstrating direct visualization and tactile assessment crucial for diagnosing the extent and stability of meniscal pathology.
Open Surgical Approaches
Open approaches are necessary for procedures requiring extensive exposure, direct reduction and fixation of complex fractures, or larger arthroplasty procedures.
-
Anterior Approaches:
- Medial Parapatellar Approach: The workhorse incision for total knee arthroplasty (TKA) and many open patellofemoral procedures. A longitudinal incision is made from the superior aspect of the patella to the tibial tuberosity, just medial to the patellar tendon. Dissection continues through subcutaneous tissue, and the medial retinaculum and joint capsule are incised (capsulotomy) from the vastus medialis obliquus (VMO) origin to the medial aspect of the patellar tendon. The patella is then everted laterally, exposing the entire tibiofemoral and patellofemoral joint surfaces. This approach provides excellent visualization of the medial and central compartments, as well as the patellofemoral joint.
- Lateral Parapatellar Approach: Less common for routine TKA but can be used for specific cases (e.g., severe valgus deformity, lateral patellar subluxation requiring lateral release). Similar longitudinal incision but lateral to the patellar tendon, incising the lateral retinaculum.
- Midline Approach: A direct anterior longitudinal incision, typically used for extensor mechanism ruptures (quadriceps or patellar tendon repairs) or some complex fracture patterns.
-
Posterior Approaches:
- Posteromedial Approach: Used for accessing the posterior aspect of the medial condyle, PCL avulsions, posterior meniscal pathology, or popliteal cysts. An S-shaped or longitudinal incision is made posteromedially. Dissection proceeds between the medial head of the gastrocnemius (medially) and the semimembranosus/semitendinosus complex (laterally). Care is taken to identify and protect the saphenous nerve and vein.
- Posterolateral Approach: Utilized for access to the posterolateral corner structures (LCL, popliteus tendon, PFL), lateral meniscal root repairs, or PCL repairs. A curved or S-shaped incision is made posterolaterally. Dissection must meticulously identify and protect the common peroneal nerve, which is highly vulnerable as it courses around the fibular neck.
-
Specific Considerations:
- Reduction and Fixation (for Fractures): Once anatomy is revealed, anatomical reduction of fracture fragments is performed using various clamps and instruments. Fixation is achieved with plates, screws, wires, or a combination, aiming for stable internal fixation to facilitate early motion.
- Graft Harvesting (for Ligament Reconstruction): Autograft harvest (e.g., patellar tendon, hamstring tendons, quadriceps tendon) requires precise dissection to minimize donor site morbidity. Anatomical knowledge of nerve branches (e.g., infrapatellar branch of saphenous nerve) and muscle attachments is crucial.
Complications & Management
Despite meticulous surgical technique and comprehensive anatomical understanding, complications can arise following knee surgery. Vigilant post-operative monitoring and prompt intervention are critical for effective management.
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Infection (SSI) | 0.5-2% (arthroscopy); 1-3% (arthroplasty) | Surgical debridement, irrigation, IV antibiotics, implant retention (if stable), staged revision arthroplasty. |
| Deep Vein Thrombosis (DVT) | 10-20% (clinical); 40-60% (venography) | Anticoagulation (LMWH, DOACs), IVC filter (for PE risk), early mobilization. |
| Pulmonary Embolism (PE) | 0.1-1% (clinical) | Anticoagulation, hemodynamic support, thrombolysis (for massive PE). |
| Neurovascular Injury | <0.5% (arthroscopy); 0.5-2% (arthroplasty/trauma) | Immediate vascular surgery consultation, nerve repair/grafting, neurolysis, bracing, physical therapy. |
| Arthrofibrosis / Stiffness | 5-10% (ACL reconstruction); 5-15% (TKA) | Aggressive physical therapy, manipulation under anesthesia, arthroscopic lysis of adhesions. |
| Patellar Maltracking/Instability | 2-5% (TKA); 10-20% (MPFL repair failure) | Revision soft tissue procedures, tibial tuberosity osteotomy, revision arthroplasty. |
| Hardware Failure | 1-5% (fracture fixation) | Revision fixation with stronger constructs, non-union management (bone graft, biologics). |
| Recurrent Instability (Ligamentous) | 5-10% (ACL reconstruction) | Revision ligament reconstruction with alternative graft, lateral extra-articular tenodesis. |
| Persistent Pain | Variable (up to 20-30%) | Diagnostic workup (imaging, injections), physical therapy, neuromodulation, psychological support, revision surgery. |
| Compartment Syndrome | Rare, but limb-threatening | Immediate fasciotomy. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an indispensable component of successful knee surgery, aiming to restore joint function, strength, and proprioception while protecting healing tissues. Protocols are tailored to the specific procedure, patient factors, and surgical findings, but generally follow a phased progression.
Phase 1: Protection and Early Motion (Weeks 0-6)
- Goals: Control pain and swelling, protect surgical repair/reconstruction, achieve early range of motion (ROM), minimize muscle atrophy.
- Weight-Bearing: Varies by procedure (e.g., non-weight-bearing (NWB) for meniscal repair, partial weight-bearing (PWB) for osteochondral procedures, weight-bearing as tolerated (WBAT) for ACL reconstruction with secure fixation).
- ROM: Immediate passive ROM (CPM machine often used) to prevent stiffness, progressing to active ROM as tolerated. Specific limitations may apply (e.g., restricted flexion for PCL repair, restricted extension for meniscal repair).
- Exercises: Quadriceps sets, straight leg raises (SLR) in multiple planes, ankle pumps, gentle hamstring activation.
- Bracing: Often utilized for specific procedures (e.g., hinged knee brace for ligament reconstructions, restricted ROM brace for meniscal repairs) to provide protection during initial healing.
Phase 2: Intermediate Strengthening and Functional Progression (Weeks 6-12)
- Goals: Full pain-free ROM, progressive strengthening, restoration of gait mechanics, introduction of proprioceptive training.
- Weight-Bearing: Progress from PWB to full weight-bearing (FWB).
- ROM: Advance to full ROM (typically 0-130 degrees for most procedures).
- Exercises: Closed-chain exercises (mini-squats, leg presses, step-ups), open-chain exercises (hamstring curls, knee extensions with caution), core strengthening, balance exercises (single-leg stance).
- Proprioception: Wobble board, foam pad exercises to restore joint awareness and neuromuscular control.
Phase 3: Advanced Strengthening and Return to Activity (Weeks 12-24+)
- Goals: Maximize strength, power, and endurance; develop sport-specific skills; achieve symmetric limb function; gradual return to unrestricted activities.
- Exercises: Plyometrics, agility drills, running progression, sport-specific training. Higher-resistance strengthening.
- Criteria for Return to Sport: Objective strength measurements (e.g., isokinetic testing >90% contralateral limb), functional hop tests, absence of pain/swelling, excellent neuromuscular control, psychological readiness. Return to contact sports typically not before 6-9 months post-operatively for ligamentous reconstructions.
Summary of Key Literature / Guidelines
A robust evidence base and established clinical guidelines are fundamental to contemporary orthopedic practice in knee surgery. These resources, continuously updated, reflect advancements in anatomical understanding, surgical techniques, and rehabilitation strategies.
- Anatomical Studies: Foundational work by Segond, Kaplan, and more recently, detailed arthroscopic and cadaveric studies by groups such as Claes et al. (elucidating the anterolateral ligament, ALL) and Morgan et al. (ACL/PCL bundle anatomy) have refined our understanding of knee stabilizers. These studies emphasize the multi-ligamentous nature of stability and the importance of addressing all injured structures, particularly in complex instabilities.
- Biomechanics Research: Extensive biomechanical analyses, often utilizing in-vitro cadaveric models, have clarified the roles of individual structures in resisting various loads (e.g., ACL's primary role in anterior translation and secondary role in rotational stability; meniscal hoop stress function). This research informs graft choice, tunnel placement, and tensioning in ligament reconstruction.
-
Clinical Practice Guidelines:
- American Academy of Orthopaedic Surgeons (AAOS): Publishes evidence-based clinical practice guidelines for common knee conditions, including osteoarthritis, meniscal tears, and ACL injury, addressing diagnostic imaging, non-operative management, and surgical indications.
- European Society of Sports Traumatology, Knee Surgery & Arthroscopy (ESSKA) and International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS): These international societies provide consensus statements, position papers, and educational resources on a wide array of knee pathologies, often focusing on surgical techniques, graft selection, and rehabilitation protocols for ligament and meniscal injuries.
- Landmark Trials: Key randomized controlled trials (e.g., MOON study for ACL reconstruction outcomes, trials comparing partial meniscectomy to meniscal repair) continually shape our treatment paradigms.
- Technique Evolution: Advances in arthroscopic instrumentation, all-inside repair techniques for menisci, anatomic ACL/PCL reconstruction, and patient-specific instrumentation for arthroplasty are constantly evolving, demanding continuous professional development.
In conclusion, the knee joint remains a cornerstone of orthopedic surgery. A meticulous and dynamic understanding of its anatomy, from macro-osseous landmarks to micro-articular surfaces and neurovascular pathways, is the bedrock upon which effective surgical practice and patient care are built. Adherence to established guidelines and a commitment to evidence-based medicine, combined with refined surgical technique, are paramount in addressing the diverse and challenging pathologies of the knee.
