Operative Management of Knee and Proximal Tibiofibular Joint Dislocations

Key Takeaway
Knee dislocations are severe, limb-threatening injuries requiring immediate neurovascular assessment and precise reduction. While historically considered rare, true incidence is likely higher due to spontaneous reductions. Management dictates early recognition of irreducible variants, temporary stabilization using external fixation or transarticular pins, and staged ligamentous reconstruction. Similarly, proximal tibiofibular joint dislocations demand accurate diagnosis, often via CT, to prevent chronic lateral knee instability and peroneal nerve compromise.
Comprehensive Management of Knee Dislocations
Dislocation of the knee has historically been considered a rare orthopaedic emergency; however, contemporary trauma registries suggest its frequency has increased significantly over the years. In a seminal report of 22 knee dislocations, Kennedy implied that the true incidence is likely much higher than recognized. This discrepancy occurs because many knee dislocations spontaneously reduce or are reduced by emergency medical personnel at the scene of the injury without subsequent accurate reporting of the initial dislocated state.
Knee dislocations are highly morbid injuries that threaten the viability of the limb due to their intimate association with the popliteal artery and peroneal nerve. They are designated directionally as anterior, posterior, medial, lateral, or rotary, strictly according to the displacement of the tibia in relation to the femur. Rotary dislocations are further subclassified as anteromedial, anterolateral, posteromedial, and posterolateral.
Clinical Pearl: Always maintain a high index of suspicion for a spontaneously reduced knee dislocation in any patient presenting with a grossly unstable "floppy" knee, multidirectional instability, or high-energy lower extremity trauma. A normal radiograph does not rule out a catastrophic multiligamentous knee injury.
Initial Evaluation and the Irreducible Dislocation
The immediate priority in any suspected knee dislocation is a diligent neurovascular evaluation. The popliteal artery is tethered proximally at the adductor hiatus and distally at the soleus arch, making it highly susceptible to intimal tear, transection, or thrombosis during extreme tibial displacement.
While most knee dislocations can be managed with closed reduction under conscious sedation in the emergency department, closed reduction may be impossible in certain rotary variants, especially when the dislocation is posterolateral.
Blocking of concentric reduction by the interposition of the joint capsule has been classically described by Watson-Jones and Anderson. Furthermore, the "buttonholing" of the medial femoral condyle through a longitudinal tear in the medial joint capsule has been well-documented by Brennan et al., as well as by Quinlan and Sharrard. Shields et al. further noted that a torn tibial collateral ligament (MCL) and the pes anserinus tendons can also invaginate into the joint space, physically blocking reduction.
Surgical Warning: A classic clinical sign of an irreducible posterolateral knee dislocation is the "dimple sign"—a transverse skin furrow or puckering over the medial joint line caused by the medial femoral condyle buttonholing through the medial capsule. Attempting forceful closed reduction in the presence of a dimple sign is contraindicated and may cause iatrogenic skin necrosis or further chondral damage.
When an irreducible dislocation is encountered, emergent open reduction is necessary. The surgical approach depends on the type of dislocation, but a standard medial approach is most frequently utilized for posterolateral dislocations.
Step-by-Step Open Reduction (Medial Approach):
* Incision: A longitudinal incision is made over the medial aspect of the knee, centered over the palpable prominence of the medial femoral condyle.
* Dissection: The subcutaneous tissues are divided to expose the medial fascia. The saphenous nerve and vein must be identified and protected.
* Release: The entrapping structures (usually the medial capsule, MCL, or pes anserinus) are carefully identified. The capsular slit through which the condyle has buttonholed is extended longitudinally to release the strangulated condyle.
* Reduction: Gentle traction and internal rotation of the tibia are applied to achieve concentric reduction.
* Repair: The torn structures are anatomically repaired, and the aftertreatment follows standard multiligamentous injury protocols.
Temporary Stabilization Techniques
Following successful reduction (closed or open), the knee must be stabilized. If the knee redislocates in a splint, or if the patient requires vascular repair (e.g., reverse saphenous vein grafting by a vascular surgeon), immediate rigid stability is paramount to protect the vascular anastomosis.
Historically, transarticular pins were driven from the anterior eminence of the tibia into the femur to provide immediate stability.
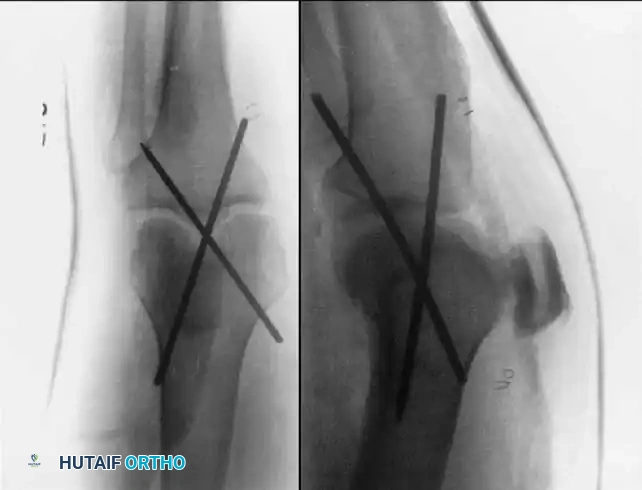
While effective for rigid immobilization, transarticular pins have been associated with significant complications, including pin track infection, septic arthritis, and pin breakage. Therefore, they should be used with extreme caution. We have found a transarticular pin to be uniquely useful when the posterior capsule is completely disrupted, preventing concentric reduction in full extension. In such specific cases, the pin is left in place for 4 to 6 weeks, after which it is removed, and range of motion is initiated.
Modern Alternative: Knee-Spanning External Fixation
A knee-spanning external fixator is now the preferred method for temporary stabilization in open knee dislocations with extensive soft-tissue injury, or in highly unstable knees following vascular repair.
* Femoral Pins: Two 5.0 mm half-pins are placed in the anterior or anterolateral femur, well proximal to the suprapatellar pouch.
* Tibial Pins: Two 5.0 mm half-pins are placed in the anterior tibial crest, distal to the joint capsule.
* Frame Assembly: Carbon fiber rods are used to bridge the joint, locking the knee in 10 to 15 degrees of flexion to reduce tension on the popliteal neurovascular bundle.
Principles of Ligamentous Repair and Reconstruction
In complete knee dislocations, both the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) are usually torn. In addition, either the tibial collateral ligament (MCL) or fibular collateral ligament (LCL) is completely disrupted.
The decision to repair or reconstruct the ligaments surgically is dictated by the presence of other skeletal injuries, vascular deficits, open wounds, and the patient's physiological status. If possible, however, the ligaments should be repaired or reconstructed early. In the landmark series by Sisk and King, early ligament repair produced significantly more satisfactory long-term results (88%) compared to cast immobilization alone (64%).
Several surgeons have advocated for the early repair of all injured structures. Kennedy concluded that early repair of major ligamentous disruptions resulted in satisfactory knees. Shields et al. found that 11 of 12 knees treated by early repair of the ligaments had satisfactory function, whereas 9 of 11 treated without repair had unsatisfactory results. Meyers et al. corroborated this, finding that in 16 patients treated by early repair, 13 had excellent or good results, whereas closed methods yielded predominantly fair or poor results.
Preoperative Imaging and Surgical Timing
MRI is an invaluable tool in preoperative planning. Twaddle et al., in a study of 17 knee dislocations in polytrauma patients, found that MRI was more accurate in diagnosing the extent of ligamentous injury than clinical examination alone. Conversely, Lonner et al. found clinical examination under anesthesia to be highly accurate, noting that the most common error was an MRI-indicated LCL injury that was not clinically significant.
Surgical Pitfall: Many dislocations result in bony avulsions rather than midsubstance tears of the collateral or cruciate ligaments. Primary repair of midsubstance cruciate tears is biomechanically inferior to reconstruction. However, replacement of avulsed bone fragments with secure fixation (e.g., suture anchors or screws) can lead to excellent outcomes.
Posterolateral corner (PLC) injuries are particularly worrisome. They should be treated early (within 2 to 3 weeks) to avoid having to perform less rewarding, complex reconstructive procedures that become necessary once chronic scar tissue forms and tissue planes are obliterated. After stabilization of the patient and diligent neurovascular evaluation, we prefer to operate on these injuries within the first 3 weeks. Knees without PLC involvement can be treated in a delayed fashion once a range of motion of 0 to 90 degrees is restored.
If surgical repair is impossible—such as in injuries requiring extensive vascular repair, massive open wounds, or in elderly, low-demand patients—satisfactory results can sometimes be obtained by nonsurgical management. A long leg splint is applied for approximately 2 weeks, followed by protected range of motion in a hinged brace. These patients typically develop stiffness rather than gross instability as their primary long-term problem.
The Proximal Tibiofibular Joint (PTFJ)
Anatomy and Biomechanics
Acute dislocation of the proximal tibiofibular joint is a rare entity. It is usually the result of a twisting trauma to the flexed knee and may be seen in association with other injuries to the same extremity, such as tibial shaft fractures or multiligamentous knee injuries. Because of its rarity and the subtle clinical findings, injuries of the proximal tibiofibular joint are frequently overlooked in the acute setting.
According to Ogden (1974), the articular configuration of the proximal tibiofibular joint can be classified into two basic types: oblique or horizontal.
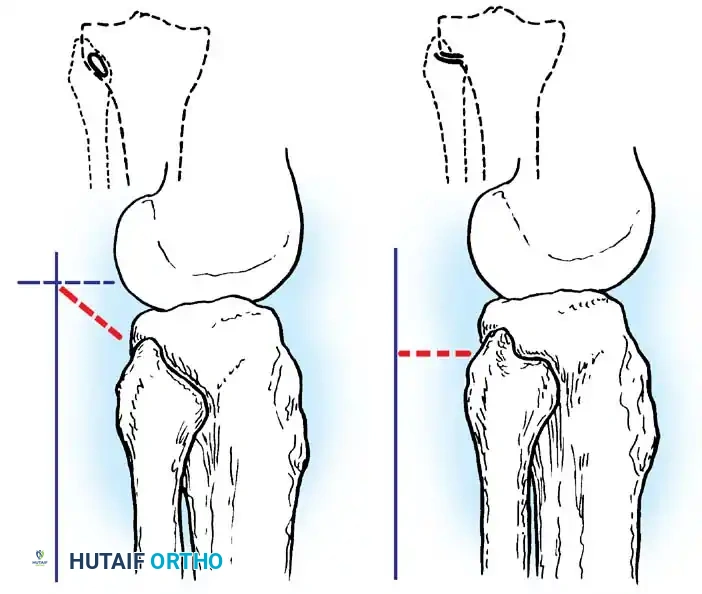
- Horizontal Joints: Feature a larger surface area and allow for more physiologic motion (rotation and translation) to accommodate ankle dorsiflexion and plantarflexion.
- Oblique Joints: Feature a steeper articular inclination with relative restriction of motion. This restricted mobility is presumably the reason why most traumatic dislocations occur in oblique joints (accounting for 70% of injuries in Ogden’s series).
Clinical Presentation and Diagnosis
Patients with acute PTFJ dislocations usually present with localized lateral knee pain, a visible or palpable prominence in the lateral aspect of the knee, and pain exacerbated by ankle motion. Patients with chronic dislocations or subluxation complain of popping, snapping, and lateral instability, which can easily be confused with a lateral meniscus tear or snapping biceps femoris tendon. Rarely, transient or permanent peroneal nerve deficits are present due to traction on the common peroneal nerve as it wraps around the fibular neck.
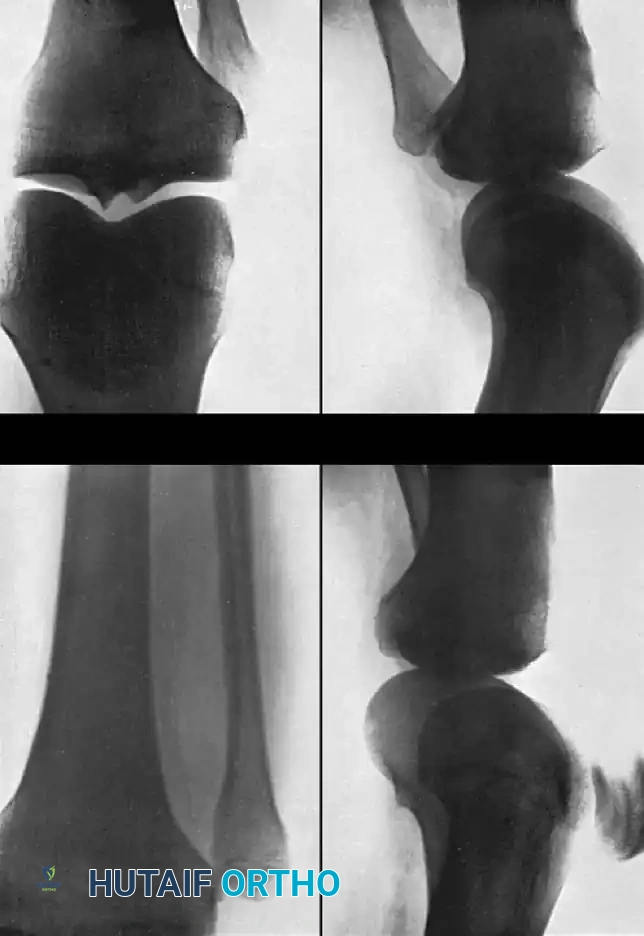
Standard anteroposterior and lateral radiographs may show subtle asymmetry or overlap of the fibular head relative to the lateral tibial condyle. However, Keogh et al. concluded after a comprehensive cadaver study that the diagnosis of suspected dislocations of the proximal tibiofibular joint is best determined with an axial CT scan, which definitively demonstrates the loss of articular congruity.
Classification of PTFJ Dislocations
Ogden classified tibiofibular subluxations and dislocations into four distinct types:
1. Subluxation: Excessive symptomatic translation without complete dislocation.
2. Anterolateral Dislocation: The most common type. The fibular head is displaced anteriorly and laterally.
3. Posteromedial Dislocation: Less common, usually high-energy, and often associated with peroneal nerve injury.
4. Superior Dislocation: Rare, typically associated with a concomitant fracture of the fibula or proximal dislocation of the lateral malleolus (e.g., variant of a Maisonneuve injury).
Surgical Approaches and Treatment Protocols
Management of Subluxation:
Subluxation of the proximal tibiofibular joint is a recurring problem often associated with generalized joint hypermobility. Initial treatment consists of cylinder cast immobilization. If symptoms fail to respond to conservative measures, resection of the fibular head is recommended.
* Crucial Biomechanical Note: Arthrodesis (fusion) of the proximal tibiofibular joint is strictly discouraged. Because the fibula must migrate proximally and rotate externally during ankle dorsiflexion, fusing the proximal joint severely restricts ankle motion and predictably leads to late, painful complaints referable to the ankle and distal tibiofibular syndesmosis.
Management of Anterolateral Dislocations:
Anterolateral dislocations were the most common in Ogden’s series. They are usually treated successfully by closed reduction. The knee is flexed to 90 degrees to relax the biceps femoris tendon and LCL, and direct posteromedial pressure is applied to the fibular head until an audible "clunk" is felt. Post-reduction, the knee is immobilized in a hinged brace.
Management of Posteromedial Dislocations:
Posteromedial proximal tibiofibular dislocations are relatively uncommon and notoriously difficult to reduce closed. They are usually associated with severe disruptions of the tibiofibular capsular ligaments and the fibular collateral ligament.
* Operative Technique: When the dislocation is acute, open reduction is recommended. A lateral approach is utilized, carefully isolating and protecting the common peroneal nerve. The joint is reduced under direct vision. Temporary extra-articular fixation is achieved with two smooth Kirschner wires driven from the fibular head into the lateral tibial plateau. The torn capsular ligaments are then repaired primarily.
Management of Superior Dislocations:
Superior dislocations frequently require open reduction. Following surgical reduction and K-wire stabilization, the leg must be immobilized in a long leg cast to prevent ankle motion, as ankle dorsiflexion forces the fibula proximally, which can cause loosening or breakage of the pin fixation.
* Postoperative Protocol: Immobilization of the knee in slight flexion (15 to 20 degrees) is utilized to relax the proximal pull of the biceps femoris on the fibular head. The patient is strictly non-weight-bearing on crutches until the long leg cast is removed at 3 weeks. A short leg walking cast is then applied for an additional 3 weeks. The K-wires are removed in the clinic 6 weeks after surgery, and progressive range of motion and strengthening exercises are instituted.
📚 Medical References
- knee dislocation: a review of nineteen knees, Clin Orthop Relat Res 216:136, 1987.
- Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee, J Pediatr Orthop 7:194, 1987.
- Katz MP, Grogono BJ, Soper KC: The etiology and treatment of congenital dislocation of the knee, J Bone Joint Surg 49B:112, 1967.
- Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee, J Pediatr Orthop 19:252, 1999.
- Lenke LG, Schoenecker PL, Gilula LA: Imaging rounds no. 105, Orthop Rev 20:295, 1991.
- Muhammad KS, Koman LA, Mooney JF III, et al: Congenital dislocation of the knee: overview of management options, J South Orthop Assoc 8:93, 1999.
- Niebauer JJ, King DE: Congenital dislocation of the knee, J Bone Joint Surg 42A:207, 1960.
- Nogi J, MacEwen GD: Congenital dislocation of the knee, J Pediatr Orthop 2:509, 1982.
- Roach JW, Richards BS: Instructional case: congenital dislocation of the knee, J Pediatr Orthop 8:226, 1988.
- Congenital Dislocation of the Patella Eilert RE: Congenital dislocation of the patella, Clin Orthop Relat Res 389:22, 2001.
- Gao GX, Lee EH, Bose K: Surgical management of congenital and habitual dislocation of the patella, J Pediatr Orthop 10:255, 1990.
- Ghanem I, Wattincourt L, Sering R: Congenital dislocation of the patella, I: pathologic anatomy, J Pediatr Orthop 20:812, 2000.
- Ghanem I, Wattincourt L, Sering R: Congenital dislocation of the patella, II: orthopaedic management, J Pediatr Orthop 20:817, 2000.
- Gordon JE, Schoenecker PL: Surgical treatment of congenital dislocation of the patella, J Pediatr Orthop 19:260, 1999.
- Green JP, Waugh W: Congenital lateral dislocation of the patella, J Bone Joint Surg 50B:285, 1968.
- Langenskiöld A, Ritsilä V: Congenital dislocation of the patella and its operative treatment, J Pediatr Orthop 12:315, 1992.
- Lenke LG, Schoenecker PL, Gilula LA: Imaging rounds no. 104, Orthop Rev 19:919, 1990.
- McCall RE, Lessenberry HB: Case report: bilateral congenital dislocation of the patella, J Pediatr Orthop 7:100, 1987.
- Stanisavljevic S, Zemenick G, Miller D: Congenital, irreducible, permanent lateral dislocation of the patella, Clin Orthop Relat Res 116:190, 1975.
- [Congenital Long Bone Defi ciencies
General Aitken GT: Amputation as a treatment for certain lowerextremity congenital anomalies, J Bone Joint Surg 41A:1267, 1959.](https://pubmed.ncbi.nlm.nih.gov/?term=Congenital%20Long%20Bone%20De%EF%AC%81%20ciencies%0A%0AGeneral%20Aitken%20GT%3A%20Amputation%20as%20a%20treatment%20for%20certain%20lowerextremity%20congenital%20anomalies%2C%20J%20Bone%20Joint%20Surg%2041A%3A1267%2C%201959.)
- Day HJB: Nomenclature and classifi cation in congenital limb defi ciency. In Murdoch G, Donovan RG, eds:
You Might Also Like

