INTRAPELVIC PROTRUSIO ACETABULI (OTTO PELVIS OR ARTHROKATADYSIS)
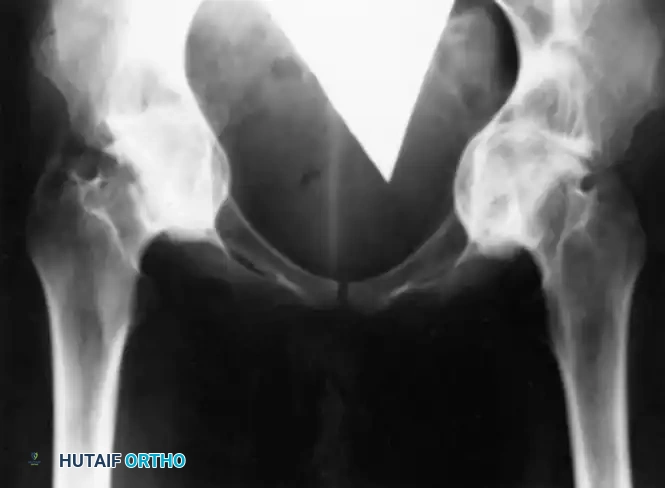
Intrapelvic protrusio acetabuli, historically referred to as Otto pelvis or arthrokatadysis, is a complex morphological deformity characterized by the chronic, progressive protrusion of the femoral head into the acetabulum and the true pelvis. Radiographically, it is defined by the medialization of the acetabular line past the ilioischial line (Kohler’s line).
Approximately two-thirds of these lesions present unilaterally. While the condition most frequently manifests in middle-aged individuals, it can develop during adolescence, particularly in the context of genetic or metabolic predispositions. The etiology is broadly categorized into primary (idiopathic) and secondary forms. Secondary protrusio acetabuli is frequently causally related to metabolic bone diseases such as osteomalacia, Paget's disease, or severe inflammatory arthropathies, most notably rheumatoid arthritis.
Biomechanics and Pathophysiology
The biomechanical consequences of protrusio acetabuli are profound. As the femoral head migrates medially, the center of rotation (COR) of the hip joint is displaced medially and superiorly. This medialization shortens the abductor moment arm, leading to significant abductor weakness, a pronounced Trendelenburg gait, and increased joint reactive forces that further accelerate medial bone loss. The femoral neck may eventually impinge on the ischium or the anterior acetabular rim, severely restricting the range of motion.
Clinical Pearl: The primary biomechanical goal in the surgical reconstruction of protrusio acetabuli is the lateralization and inferiorization of the hip's center of rotation to its anatomic origin. Failure to restore the COR will result in persistent abductor weakness, impingement, and premature component failure.
Clinical Presentation and Radiographic Evaluation
Patients typically present with an insidious onset of deep groin pain, a progressive limp, and a marked limitation in hip range of motion—particularly in abduction and rotation. Pain and functional incapacitation are the primary indications for surgical intervention.
Standard anteroposterior (AP) pelvis and lateral hip radiographs are essential. The diagnosis is confirmed when the acetabular teardrop is obliterated or when the medial wall of the acetabulum projects medial to Kohler's line.
Cross-sectional imaging (CT scanning) is highly recommended for preoperative templating. A 3D CT reconstruction allows the surgeon to accurately quantify the volumetric bone loss of the medial wall, assess the integrity of the anterior and posterior columns, and determine the required volume of bone graft.
Surgical Management: Total Hip Arthroplasty (THA)
Total hip arthroplasty is the preferred and definitive treatment for protrusio acetabuli. Historically, bipolar socket hemiarthroplasty combined with bone grafting to the medial wall defect yielded acceptable results (as reported by Wilson and Scott, who noted good outcomes in 21 of 22 hips at an average of 54 months). However, modern tribology and advanced uncemented fixation have made THA the gold standard.
Ebert et al. and Gates et al. have heavily emphasized the absolute necessity of medial bone grafting when performing THA in these patients. In a long-term follow-up study averaging 12.8 years, Gates et al. demonstrated that THA combined with medial bone grafting was effective in arresting the progression of protrusio acetabuli in 90% of patients.
Step-by-Step Surgical Technique for THA in Protrusio
- Surgical Approach and Exposure:
A standard posterior or direct anterior approach may be utilized. However, the surgeon must be prepared for a challenging dislocation. Because the femoral head is "captured" within the deep acetabular socket, forceful dislocation maneuvers can easily result in iatrogenic fractures of the posterior wall or the femoral shaft. - In Situ Femoral Neck Osteotomy:
If the head cannot be safely dislocated, an in situ osteotomy of the femoral neck is mandatory. The femoral neck is cut at the templated level, and the femoral head is subsequently extracted from the acetabulum using a corkscrew. In severe cases of arthrokatadysis, the head may need to be sectioned into quadrants (pie-crusting) for safe removal. - Acetabular Preparation:
The fundamental principle of acetabular reaming in protrusio is to ream the periphery, not the medial wall. The medial wall is often paper-thin or entirely deficient. Reaming should be directed laterally and inferiorly to create a bleeding peripheral rim that will support the hemispherical shell. - Medial Bone Grafting:
The medial defect must be grafted to lateralize the component. Morselized cancellous autograft (often harvested from the extracted femoral head) or allograft is packed tightly into the medial defect. Reverse reaming (running the reamer in reverse) can be used to impact the graft into a dense, supportive layer. - Component Implantation:
A multi-hole, uncemented hemispherical titanium shell is impacted into the prepared peripheral rim. The shell must achieve rigid peripheral press-fit stability. Supplemental screw fixation into the safe zones (posterosuperior quadrant) is highly recommended. If the peripheral rim is incompetent, an anti-protrusio cage (e.g., Burch-Schneider cage) or a custom triflange component may be required to span the defect and transfer loads to the intact ilium and ischium.
Surgical Warning: Never accept a medialized cup position. Placing the acetabular component directly against the thin medial wall without grafting will inevitably lead to intrapelvic migration of the prosthesis.
Alternative: Arthrodesis
While THA is the treatment of choice, hip arthrodesis should be considered in a very specific subset of patients: young, active individuals with unilateral disease who are engaged in heavy, demanding physical labor. Arthrodesis provides a stable, painless joint that can withstand extreme loading, though it sacrifices mobility and places increased stress on the lumbar spine and contralateral hip over time.
OSTEITIS PUBIS
Osteitis pubis is a painful, noninfectious, inflammatory condition involving the pubic bone, the pubic symphysis, and the surrounding myofascial structures. It represents a spectrum of anterior pelvic ring overload and instability.
Etiology and Demographics
The condition is frequently triggered by repetitive microtrauma and biomechanical overload. It is highly prevalent in athletes whose sports require repetitive kicking, pivoting, or extreme exertion, ranging from long-distance runners and soccer players to powerlifters.
Additionally, osteitis pubis has a well-documented iatrogenic etiology. It has been reported following various urological and gynecological procedures (e.g., prostatectomy, bladder suspension) where the retropubic space of Retzius is violated, leading to localized periostitis or altered symphyseal biomechanics.
Clinical Presentation and Diagnostics
The primary symptom is the gradual onset of sharp or aching pain in the pubic region. The pain frequently radiates into the groin, along the medial aspect of the thighs (following the adductor origin), or superiorly into the lower abdomen (following the rectus abdominis insertion).
As the inflammatory process progresses, increasing pain may make ambulation exceedingly difficult. Patients often develop a characteristic antalgic or waddling gait to minimize shear forces across the symphysis pubis.
Imaging Modalities:
* Radiographs: Plain radiographic changes may lag behind clinical symptoms by 2 to 3 weeks. Characteristic findings include symmetrical bone resorption at the medial ends of the pubic bones, widening or irregularity of the pubic symphysis, and reactive rarefaction or sclerosis along the pubic rami.
* Bone Scintigraphy (Technetium-99m): Bone scans are highly sensitive and will show diffuse, intense uptake in the pubis much earlier than plain radiographs.
* Magnetic Resonance Imaging (MRI): MRI is the gold standard for differentiating osteitis pubis from other causes of groin pain, such as athletic pubalgia (sports hernia), adductor tendinopathy, iliopsoas bursitis, and pubic ramus stress fractures. MRI typically reveals subchondral bone marrow edema extending from the symphysis into the pubic rami.
Nonoperative Management
Because osteitis pubis is generally a self-limiting condition, the first line of treatment is strictly nonoperative.
* Rest and Modification: Complete cessation of the offending activity is paramount.
* Pharmacotherapy: Aggressive use of nonsteroidal anti-inflammatory drugs (NSAIDs) to modulate the inflammatory cascade.
* Physical Therapy: Core stabilization and progressive adductor stretching/strengthening once acute pain subsides.
* Injections: If symptoms persist despite oral medications and rest, fluoroscopically or ultrasound-guided corticosteroid injections directly into the symphysis pubis can provide significant diagnostic and therapeutic benefit.
Operative Management
Operative treatment is rarely indicated and is reserved for patients with recalcitrant symptoms that have failed a minimum of 6 to 12 months of exhaustive nonoperative management.
Wedge Resection of the Symphysis (Historical Context)
Historically, wedge resection of the symphysis pubis was utilized. Grace et al. reported on 10 patients who underwent wedge resections for recalcitrant osteitis pubis. At an average of 14 months postoperatively, all patients showed marked improvement. However, the long-term follow-up (average 92 months) revealed a high failure rate, with three of the 10 patients dissatisfied.
Pitfall: Resection of the symphysis pubis destroys the anterior tension band of the pelvic ring. This can lead to catastrophic posterior pelvic instability. One patient in the Grace et al. series required bilateral sacroiliac arthrodeses for severe pain caused by secondary pelvic instability. Similarly, Moore, Stover, and Matta reported patients developing bilateral sacroiliac instability after wedge resection, necessitating complex posterior arthrodesis.
Symphyseal Arthrodesis (Preferred Technique)
Due to the high risk of posterior pelvic destabilization associated with resection, symphyseal arthrodesis (fusion) is now the preferred operative intervention for refractory cases. Williams, Thomas, and Downes reported excellent results after symphysis fusion in patients with osteitis pubis and documented anterior pelvic instability.
Surgical Technique for Symphyseal Arthrodesis:
1. Approach: A Pfannenstiel incision is utilized to expose the anterior pelvic ring. The rectus abdominis insertions are carefully mobilized.
2. Preparation: The fibrocartilaginous disc of the symphysis is radically excised. The hyaline cartilage endplates of the pubic bones are decorticated down to bleeding subchondral bone using curettes and a high-speed burr.
3. Grafting: Autologous cancellous bone graft, typically harvested from the anterior iliac crest, is packed tightly into the symphyseal defect.
4. Fixation: Rigid internal fixation is achieved using a multi-hole reconstruction plate (often a 3.5mm or 4.5mm pelvic plate) contoured to the superior aspect of the pubic rami. In cases of severe instability, orthogonal dual-plating (superior and anterior) may be employed to neutralize shear forces until arthrodesis is achieved.
PATHOPHYSIOLOGICAL CONSIDERATIONS IN RHEUMATOID SYNOVITIS
Given that rheumatoid arthritis (RA) is a primary driver of secondary protrusio acetabuli, a deep understanding of rheumatoid synovitis is essential for the reconstructive surgeon.
As detailed by Bondeson et al., the pathophysiology of rheumatoid joint destruction is driven by synovial macrophages and macrophage-produced cytokines (such as TNF-alpha and IL-1). These cytokines upregulate aggrecanases and matrix metalloproteinases (MMPs), leading to rapid degradation of articular cartilage and subchondral bone. This aggressive osteolysis is what permits the femoral head to migrate medially through the acetabular floor.
Synovectomy and Arthroplasty in the Rheumatoid Patient
While early arthroscopic or open synovectomy (as discussed by Krebs, Limbird, and Triantafyllou) can temporarily halt the inflammatory cascade and provide symptomatic relief in early-stage rheumatoid joints, it does not permanently prevent joint deterioration. Doets et al. demonstrated that synovectomy of the rheumatoid knee does not prevent long-term radiographic progression.
Therefore, in the setting of advanced rheumatoid arthritis with protrusio acetabuli, total joint arthroplasty remains the definitive solution. Modern literature (Creighton et al., Lachiewicz) supports the use of uncemented, porous-coated components in rheumatoid patients, provided that bone stock is adequately restored via the impaction grafting techniques described above. The surgeon must also be highly cognizant of perioperative medical management, particularly the coordination of disease-modifying antirheumatic drugs (DMARDs) and biologic agents, to balance the risks of postoperative infection against the risk of a systemic rheumatoid flare (Howe et al.). Furthermore, preoperative evaluation of the cervical spine is mandatory in all RA patients undergoing THA to rule out atlantoaxial instability prior to intubation (Collins et al.).
📚 Medical References
- protrusio acetabuli, loose stems, Orthop Rev 14:27, 1985.
- Giliberty RP, Trenkle WA, Licon O: A retrospective study of the bipolar hip endoprosthesis, Orthop Rev 7:27, 1978.
- Goodnough LT, Shafron D, Marcus RE: Utilization and effectiveness of autologous blood donation for arthroplastic surgery, J Arthroplasty 5(suppl):89, 1990.
- Gottschalk FA, Morein G, Weber F: Effect of the position of the greater trochanter on the rate of union after trochanteric osteotomy for total hip arthroplasty, J Arthroplasty 3:235, 1988.
- Gross AE, Goodman S: The current role of structural grafts and cages in revision arthroplasty of the hip, Clin Orthop Relat Res 429:193, 2004.
- Harris WH: Advances in total hip arthroplasty: the metal-backed acetabular component, Clin Orthop Relat Res 183:4, 1984.
- Harris WH, Allen JR: The calcar replacement femoral component for total hip arthroplasty: design, uses and surgical technique, Clin Orthop Relat Res 157:215, 1981.
- Harris WH, Crothers OD: Reattachment of the greater trochanter in total hip-replacement arthroplasty: a new technique, J Bone Joint Surg 60A:211, 1978.
- Hashemi-Nejad A, Haddad FS, Tong KM, et al: Does Chiari osteotomy compromise subsequent total hip arthroplasty, J Arthroplasty 17:731, 2002.
- Head WC: Wagner surface replacement arthroplasty of the hip: analysis of fourteen failures in forty-one hips, J Bone Joint Surg 63A:420, 1981.
- Head WC, Mallory TH, Berklacich FM, et al: Extensile exposure of the hip for revision arthroplasty, J Arthroplasty 2:265, 1987.
- Head WC, Paradies LH: Ipsilateral hip and knee replacements as a single surgical procedure, J Bone Joint Surg 59A:352, 1977.
- Holmberg S: Life expectancy after total hip arthroplasty, J Arthroplasty 7:183, 1992.
- Judet R, Judet J: Technique and results with the acrylic femoral head prosthesis, J Bone Joint Surg 34B:173, 1952.
- Judet R, Siguier M, Brumpt B, et al: A noncemented total hip prosthesis, Clin Orthop Relat Res 137:76, 1978.
- Kavanagh BF, Fitzgerald RH Jr: Clinical and radiographic assessment of total hip arthroplasty: a new hip score, Clin Orthop Relat Res 193:133, 1985.
- Kostuik J, Alexander D: Arthrodesis for failed arthroplasty of the hip, Clin Orthop Relat Res 188:173, 1984.
- Lachiewicz PF, Anspach WE, DeMasi R: A prospective study of 100 consecutive Harris-Galante porous total hip arthroplasties: 2to 5-year results, J Arthroplasty 7:519, 1992.
- Larson CB: Rating scale for hip disabilities, Clin Orthop Relat Res 31:85, 1963.
- Mahomed NN, Barrett JA, Katz JN, et al: Rates and outcomes of primary and revision total hip replacement in the United States Medicare population, J Bone Joint Surg 85A:27, 2003.
- Mardones R, Pagnano NW, Nemanich JP, et al: The Frank Stinchfi eld Award: muscle damage after total hip arthroplasty done with the two-incision and mini-posterior techniques, Clin Orthop Relat Res 441:63, 2005.
- McBeath AA, Bahrke MS, Balke B: Walking effi ciency before and after total hip replacement as determined by oxygen consumption, J Bone Joint Surg 62A:807, 1980.
- McKee GK: Development of total prosthetic replacement of the hip, Clin Orthop Relat Res 72:85, 1970.
- McMurray MR, Birnbaum MA, Walter NE: Intraoperative autologous transfusion in primary and revision total hip arthroplasty, J Arthroplasty 5:61, 1990.
- McWilliams TG, Binns MS: The timing of femoral component insertion in cemented hip arthroplasty, J Arthroplasty 18:51, 2003.
- Mendes DG, Roffman M, Silbermann M: Reconstruction of the acetabular wall with bone graft in arthroplasty of the hip, Clin Orthop Relat Res 186:29, 1984.
- Miniaci A, Bailey WH, Bourne RB, et al: Analysis of radionuclide arthrograms, radiographic arthrograms, and sequential plain radiographs in the assessment of painful hip arthroplasty, J Arthroplasty 5:143, 1990.
- Moore AT: The self-locking metal hip prosthesis, J Bone Joint Surg 39A:811, 1957.
- Morscher EW: Cementless total hip arthroplasty, Clin Orthop Relat Res 181:76, 1983.
- Müller ME: Total hip prostheses, Clin Orthop Relat Res 72:46, 1970.
- Murray WR: Bipolar prosthesis salvage for acetabular insuffi ciency: a preliminary report, Orthop Trans 8:203, 1984.
- Ogonda L, Wilson R, Archbold P, et al: A minimal incision technique in total hip arthroplasty does not improve early postoperative outcomes: a prospective, randomized, controlled trial, J Bone Joint Surg 87A:701, 2005.
- Oh I, Bourne RB, Harris WH: The femoral cement compactor: an improvement in cementing technique in total hip replacement, J Bone Joint Surg 65A:1335, 1983.
- Oh I, Harris WH: A cement fi xation system for total hip arthroplasty, Clin Orthop Relat Res 164:221, 1982.
- Pagnano MW, Leone J, Lewallen DG, et al: Two-incision THA had modest outcomes and some substantial complications, Clin Orthop Relat Res 441:86, 2005.
- Parvizi J, Burmeister H, Ganz R: Previous Bernese periacetabular osteotomy does not compromise the results of total hip arthroplasty, Clin Orthop Relat Res 423:118, 2004.
- Pitto RP, Hamer H, Fabiani R, et al: Prophylaxis against fat and bone-marrow embolism during total hip arthroplasty reduces the incidence of postoperative deep-vein thrombosis: a controlled, randomized clinical trial, J Bone Joint Surg 84A:39, 2002.
- Poss R: Total joint replacement: optimizing patient expectations, J Am Acad Orthop Surg 1:18, 1993.
- Rao RR, Sharkey PF, Hozack WJ, et al: Immediate weightbearing after uncemented total hip arthroplasty, Clin Orthop Relat Res 349:156, 1998.
- Ries MD, Philbin EF, Groff GD, et al: Effect of total hip arthroplasty on cardiovascular fi tness, J Arthroplasty 12:84, 1997.
- Ritter MA, Vaughn BK, Frederick LD: Single-stage, bilateral, cementless total hip arthroplasty, J Arthroplasty 10:151, 1995.
- Roach JW, Paradies LH: Total hip arthroplasty performed during adolescence, J Pediatr Orthop 4:418, 1984.
- Rooker GD, Wilkinson JD: Metal sensitivity in patients undergoing hip replacement, J Bone Joint Surg 62B:502, 1980.
- Salvati EA, Hughes P, Lachiewicz P: Bilateral total hipreplacement arthroplasty in one stage, J Bone Joint Surg 60A:640, 1978.
- Salvati EA, Wilson PD Jr, Jolley MN, et al: A ten-year follow-up study of our fi rst one hundred consecutive Charnley total hip replacements, J Bone Joint Surg 63A:753, 1981.
- Schinsky MF, Nercessian OA, Arons RR, et al: Comparison of complications after transtrochanteric and posterolateral approaches for primary total hip arthroplasty, J Arthroplasty 18:430, 2003.
- Schulte KR, Callaghaan JJ, Kelley SS, et al: The outcome of Charnley total hip arthroplasty with cement after a minimum of twenty-year follow-up, J Bone Joint Surg 75A:961, 1993.
- Sharkey PF, Rao R, Hozack WJ, et al: Conversion of hemiarthroplasty to total hip arthroplasty, J Arthroplasty 13:627, 1998.
- Smith-Petersen MN: Evolution of mould arthroplasty of the hip joint, J Bone Joint Surg 30B:59, 1948.
- Sutherland CJ: Radiographic evaluation of acetabular bone stock in failed total hip arthroplasty, J Arthroplasty 3:73, 1988.
- Sutherland CJ, Wilde AH, Borden LS, et al: A ten-year follow-up of one hundred consecutive Müller curved-stem total hip-replacement arthroplasties, J Bone Joint Surg 64A:970, 1982.
- Swanson RL, Evarts CM: Dual-lock total hip arthroplasty: a preliminary experience, Clin Orthop Relat Res 191:224, 1984.
- Thompson FR: Two and a half years’ experience with a Vitallium intramedullary hip prosthesis, J Bone Joint Surg 36A:489, 1954.
- Thompson RC Jr, Culver JE: The role of trochanteric osteotomy in total hip replacement, Clin Orthop Relat Res 106:102, 1975.
- Thomson JD, Callaghan JJ, Savory CG, et al: Prior deposition of autologous blood in elective orthopaedic surgery, J Bone Joint Surg 69A:320, 1987.
- Tullos HS, McCaskill BL, Dickey R, et al: Total hip arthroplasty with a low-modulus porous-coated femoral component: progress report, J Bone Joint Surg 66A:888, 1984.
- Veberne GH: A femoral head prosthesis with a built-in joint: a radiological study of the movements of the two components, J Bone Joint Surg 65B:544, 1983.
- Weber BG: Total hip replacement with rotation-endoprosthesis (trunnion-bearing prosthesis), Clin Orthop Relat Res 72:79, 1970.
- Weeden SH, Paprosky WG, Bowling JW: The early dislocation rate in primary total hip arthroplasty following the posterior approach with posterior soft-tissue repair, J Arthroplasty 18:709, 2003.
- Wilson JN, Scales JT: The Stanmore metal on metal total hip prosthesis using a three pin type cup: a follow-up of 100 arthroplasties over nine years, Clin Orthop Relat Res 95:239, 1973.
- Wilson MG, Nikpoor N, Aliabadi P, et al: The fate of acetabular allografts after bipolar revision arthroplasty of the hip: a radiographic review, J Bone Joint Surg 71A:1469, 1989.
- Wilson PD Jr, Gordon SL, eds: NIH Consensus Development Conference: total hip joint replacement, Bethesda, Md, March 1982, J Orthop Res 1:189, 1983.
- Wilson WJ: Intraoperative autologous transfusion in revision total hip arthroplasty, J Bone Joint Surg 71A:8, 1989.
- Woolson ST, Marsh JS, Tanner JB: Transfusion of previously deposited autologous blood for patients undergoing hip replacement surgery, J Bone Joint Surg 69A:325, 1987.
- Wroblewski BM, Siney PD: Charnley low-friction arthroplasty of the hip: long-term results, Clin Orthop Relat Res 292:191, 1993.
- Yamaguchi MD, Naito M, Asayama I, et al: The effect of posterolateral reconstruction on range of motion and muscle strength in total hip arthroplasty, J Arthroplasty 18:347, 2003.
- Biomechanics and Materials Al-Saffar N: Early clinical failure of total joint replacement in association with follicular proliferation of B-lymphocytes: a report of two cases, J Bone Joint Surg 84A:2270, 2002.
- Amstutz HC, Lodwig RM, Schurman DJ, et al: Range-ofmotion studies for total hip replacements: a comparative study with a new experimental apparatus, Clin Orthop Relat Res 111:124, 1975.
- Asayama I, Akiyoshi Y, Naito M, et al: Intraoperative pelvic motion in total hip arthroplasty, J Arthroplasty 19:992, 2004.
- Bankston AB, Cates H, Ritter MA, et al: Polyethylene wear in total hip arthroplasty, Clin Orthop Relat Res 317:7, 1995.
- Barrack RL, Lavernia C, Ries M, et al: Virtual reality computer animation of the effect of component position and design on stability after total hip arthroplasty, Orthop Clin North Am 32:569, 2001.
- Barrack RL, Thornberry RL, Ries MD, et al: The effect of component design on range of motion to impingement in total hip arthroplasty, Instr Course Lect 50:275, 2001.
- Bartel DL, Burstein AH, Toda MD, et al: The effect of conformity and plastic thickness on contact stresses in metal-backed plastic implants, J Biomech Eng 107:193, 1985.
- Bednar JM, Friedenberg ZB, Turner ML: Bipolar femoral endoprosthesis: a study correlating component movement with clinical outcome, J Trauma 28:664, 1988.
- Bobyn JD, Mortimer ES, Glassman AH, et al: Producing and avoiding stress shielding: laboratory and clinical observations of noncemented total hip arthroplasty, Clin Orthop Relat Res 274:79, 1992.
- Bobyn JD, Pilliar RM, Cameron HU, et al: The effect of porous surface confi guration on the tensile strength of fi xation of implants by bone ingrowth, Clin Orthop Relat Res 149:291, 1980.
- Bobyn JD, Stackpool GJ, Hacking SA, et al: Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial, J Bone Joint Surg 81B:907, 1999.
- Bobyn JD, Tanzer M, Krygier JJ, et al: Concerns with modularity in total hip arthroplasty, Clin Orthop Relat Res 298:27, 1994.
- Bochner RM, Pellicci PM, Lyden JP: Bipolar hemiarthroplasty for fracture of the femoral neck, J Bone Joint Surg 70A:1001, 1988.
- Bono JV, Sanford L, Toussaint JT: Severe polyethylene wear in total hip arthroplasty: observations from retrieved AML PLUS hip implants with an ACS polyethylene liner, J Arthroplasty 9:119, 1994.
- Bragdon CR, Jasty M, Muratoglu OK, et al: Third-body wear of highly cross-linked polyethylene in a hip simulator, J Arthroplasty 18:553, 2003.
- Bragdon CR, O’Connor DO, Lowenstein JD: The importance of multidirectional motion on polyethylene wear. Paper presented at American Association of Hip and Knee Surgeons, Dallas, 1995.
- Brand RA, Pedersen DR, Davy DT, et al: Comparison of hip force calculations and measurements in the same patient, J Arthroplasty 9:45, 1994.
- Brodner W, Grohs JG, Bancher-Todesca D, et al: Does the placenta inhibit the passage of chromium and cobalt after metal-on-metal total hip arthroplasty, J Arthroplasty 19:102, 2004.
- Brodner W, Pitzan P, Meisinger V, et al: Serum cobalt levels after metal-on-metal total hip arthroplasty, J Bone Joint Surg 85A:2168, 2003.
- Burke DW, Gates EI, Harris WH: Centrifugation as a method of improving tensile and fatigue properties of acrylic bone cement, J Bone Joint Surg 66A:1265, 1984.
- Burroughs BR, Hallstrom B, Golladay GJ, et al: Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes: an in vitro study, J Arthroplasty 20:11, 2005.
- Burton P, Prieskorn D, Smith R, et al: Component motion in bipolar hip arthroplasty: an evaluation of reamed and nonreamed acetabula, Orthopedics 17:319, 1994.
- Cameron HU: Dissociation of a polyethylene liner from an acetabular cup, Orthop Rev 22:1160, 1993.
- Capello WN, D’Antonio JA, Feinberg JR, et al: Alternative bearing surfaces: alumina ceramic bearings for total hip arthroplasty, Instr Course Lect 54:171, 2005.
- Charnley J: A biomechanical analysis of the use of cement to anchor the femoral head prosthesis, J Bone Joint Surg 47B:354, 1965.
- Charnley J, Follacci FM, Hammond BT: The long-term reaction of bone to self-curing acrylic cement, J Bone Joint Surg 50B:822, 1968.
- Cheng SL, Davey JR, Inman RD, et al: The effect of the medial collar in total hip arthroplasty with porous-coated components inserted without cement, J Bone Joint Surg 77A:118, 1995.
- Cook SD, Barrack RL, Thomas KA, et al: Quantitative analysis of tissue growth into human porous
