Intramedullary Pinning of Metacarpal Shaft Fractures: A Master Surgical Guide

Key Takeaway
Intramedullary pinning is a minimally invasive, highly effective surgical technique for managing displaced or unstable metacarpal shaft and neck fractures. By utilizing a pre-bent Kirschner wire introduced through the metacarpal base, surgeons can achieve excellent axial and rotational stability while preserving the extensor mechanism. This guide details the precise indications, biomechanical principles, step-by-step operative execution, and postoperative rehabilitation protocols necessary to optimize functional outcomes and minimize complications.
Introduction to Metacarpal Shaft Fractures
Metacarpal shaft and neck fractures are among the most frequently encountered injuries in orthopedic hand trauma. While a significant proportion of these fractures can be managed non-operatively with appropriate immobilization, fractures exhibiting unacceptable angular deformity, shortening, or rotational malalignment necessitate surgical intervention to restore the functional cascade of the hand.
Historically, open reduction and internal fixation (ORIF) utilizing plates and screws has been employed for rigid osteosynthesis. However, the literature demonstrates that plate and screw fixation in acute metacarpal fractures carries a complication rate as high as 42%, primarily due to extensor tendon adhesions, hardware prominence, and subsequent joint stiffness. Consequently, intramedullary (IM) pinning has emerged as the gold standard for transverse, short oblique, and neck fractures of the metacarpals. This minimally invasive technique provides robust three-point biomechanical stability, preserves the fracture hematoma, minimizes soft tissue stripping, and allows for early mobilization.
Indications and Contraindications
Surgical Indications
- Displaced Metacarpal Neck Fractures: Angulation exceeding acceptable tolerances (e.g., >10–15 degrees for the index/long fingers; >30–40 degrees for the ring finger; >40–50 degrees for the small finger).
- Metacarpal Shaft Fractures: Transverse or short oblique fractures with >2 mm of shortening or any degree of rotational malalignment.
- Multiple Metacarpal Fractures: To restore the anatomical arch and stability of the hand.
- Open Fractures: Particularly those requiring soft tissue management where bulky hardware is contraindicated.
Contraindications
- Intra-articular Fractures: Fractures extending into the metacarpophalangeal (MCP) or carpometacarpal (CMC) joints with articular incongruity typically require precise open reduction and interfragmentary screw fixation.
- Severe Comminution: Highly comminuted shaft fractures may lack the cortical contact necessary for IM wire stability, risking secondary shortening. In such cases, bridging plates or external fixation may be required.
Clinical Pearl: Rotational deformity is the least tolerated malalignment in metacarpal fractures. Even 5 degrees of rotational malrotation at the metacarpal shaft can result in 1.5 cm of digital overlap at the fingertips during composite flexion. Always assess the digital cascade clinically before and after fixation.
Surgical Anatomy and Biomechanics
The metacarpal bones exhibit a natural dorsal convexity. The intramedullary pinning technique capitalizes on this anatomical bow. By introducing a pre-bent Kirschner (K-wire) through the proximal base and advancing it into the metacarpal head, the wire creates a dynamic three-point fixation system within the medullary canal.
The entry point is critical. It must be extra-articular to avoid damaging the CMC joint, yet perfectly aligned with the longitudinal axis of the medullary canal to prevent iatrogenic cortical breach during wire advancement. Furthermore, the dorsal sensory branches of the ulnar and radial nerves, as well as the extensor tendon apparatus, lie in close proximity to the proximal entry portals and must be meticulously protected during the initial dissection.
Preoperative Planning and Patient Positioning
- Anesthesia: The procedure is highly amenable to regional anesthesia (e.g., supraclavicular or axillary brachial plexus block). General anesthesia may be utilized based on patient preference or the presence of concomitant injuries.
- Positioning: The patient is placed supine with the affected extremity extended on a radiolucent hand table. A non-sterile tourniquet is applied to the upper arm.
- Imaging: A mini C-arm fluoroscopy unit is positioned parallel to the hand table, allowing for seamless transition between anteroposterior (AP), lateral, and oblique views without manipulating the fractured hand excessively.
Step-by-Step Surgical Technique
1. Localization and Incision
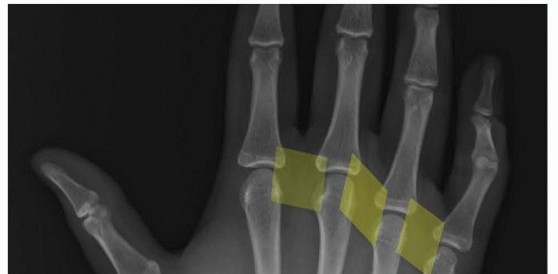
Begin by utilizing fluoroscopy to identify the exact center of the metacarpal base, both proximally and dorsally. Mark this precise location with a surgical skin marker.
FIGURE 67-38A: Skin marking indicating the middle of the metacarpal base as determined with fluoroscopy.
Make a 0.5-cm longitudinal incision beginning 1.0 to 1.5 cm proximal to the fluoroscopic mark. This proximal extension allows for a shallow trajectory angle when introducing the K-wire.

FIGURE 67-38B: Longitudinal incision placed proximal to the metacarpal base.
2. Soft Tissue Dissection and Portal Creation
Spread bluntly down through the subcutaneous tissues using a small hemostat. Meticulous blunt dissection is imperative to sweep away the dorsal sensory nerve branches and retract the extensor tendons safely.
Once the base of the fractured metacarpal is exposed, use a pair of sharp iris scissors (or a dedicated sharp awl) as a trocar. Create an entry portal in the proximal metacarpal base. The portal must be perfectly in line with the long axis of the metacarpal shaft to facilitate smooth wire passage.
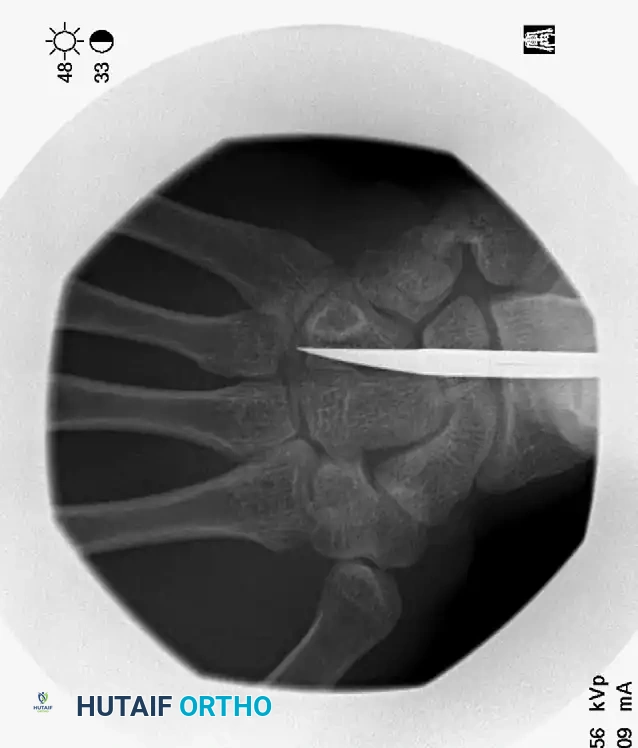
FIGURE 67-38C: Fluoroscopic view demonstrating the correct entry position and trajectory of the intramedullary wire.
3. Wire Preparation
Select a 0.062-inch (1.6 mm) Kirschner wire. Standard K-wires have sharp trocar tips that can inadvertently penetrate the articular surface of the metacarpal head. To prevent this:
* Cut the pointed end off the K-wire using heavy wire cutters to create a blunt tip.
* Gently curve the distal 5 to 10 mm of the wire (approximately 15 to 20 degrees). This pre-bend allows the wire to bounce off the endosteal cortex and assists the surgeon in "steering" the wire down the medullary canal.
4. Fracture Reduction and Wire Advancement
Before passing the wire across the fracture site, the fracture must be reduced. For metacarpal neck fractures, the Jahss maneuver is highly effective: flex the MCP joint to 90 degrees and apply dorsally directed pressure through the proximal phalanx to correct the apex-dorsal angulation.
Review the preoperative deformity carefully to understand the required reduction vectors.

FIGURE 67-35A: Preoperative AP radiograph of a fifth metacarpal neck fracture.

FIGURE 67-35B: Preoperative oblique radiograph demonstrating displacement.

FIGURE 67-35C: Preoperative lateral radiograph showing 80-degree apex dorsal angulation and rotational deformity.
Mount the unbent proximal end of the K-wire into a T-handle chuck (manual insertion provides superior tactile feedback compared to power driving). Advance the wire down the canal until it reaches the fracture site. Confirm the reduction fluoroscopically, then pass the wire across the fracture into the distal fragment.
Use live fluoroscopy to ensure intramedullary containment of the wire, especially as it crosses the fracture site. The blunt, curved tip should be advanced until it sits securely in the dense subchondral bone of the metacarpal head, stopping just short of the articular cartilage.

FIGURE 67-35D: Postoperative AP radiograph after reduction to acceptable angulation using a single intramedullary pin.

FIGURE 67-35E: Postoperative oblique radiograph confirming alignment.

FIGURE 67-35F: Postoperative lateral radiograph demonstrating restoration of the volar cortex.
This technique is equally effective for mid-shaft fractures, as demonstrated in the fourth metacarpal example below:

FIGURE 67-37A: Preoperative AP radiograph of a fourth metacarpal shaft fracture.

FIGURE 67-37B: Preoperative lateral radiograph of the fourth metacarpal fracture.

FIGURE 67-37C: Postoperative AP radiograph showing intramedullary fixation with a Kirschner wire.
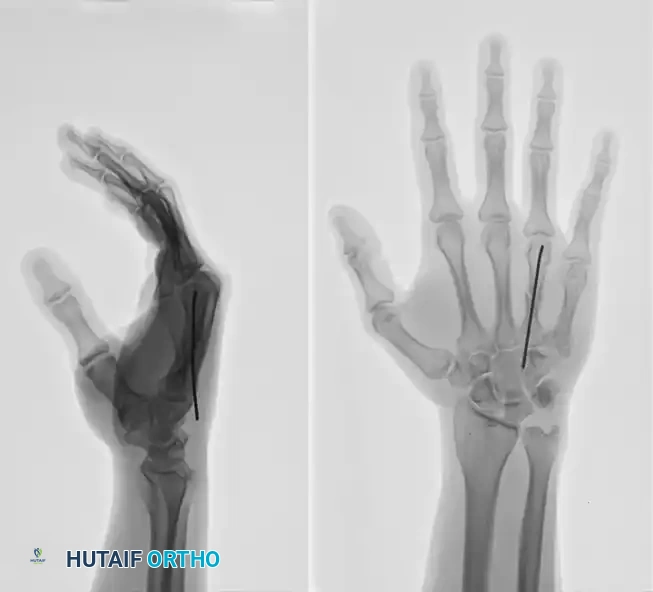
FIGURE 67-37D: Postoperative lateral radiograph confirming anatomic restoration.
5. Limited Open Reduction (If Required)
Occasionally, closed reduction is impossible due to soft tissue interposition (e.g., periosteum, intrinsic muscle fascia) or severe cortical buttonholing. If the wire is not easily passed across the fracture site after multiple attempts, do not force it, as this risks iatrogenic comminution or cortical blowout.
Instead, make a limited dorsal longitudinal incision directly over the fracture site. Gently retract the extensor mechanism, clear the interposed tissue, and anatomically reduce the fracture under direct vision. Once reduced, pass the intramedullary wire across the fracture site as previously described.
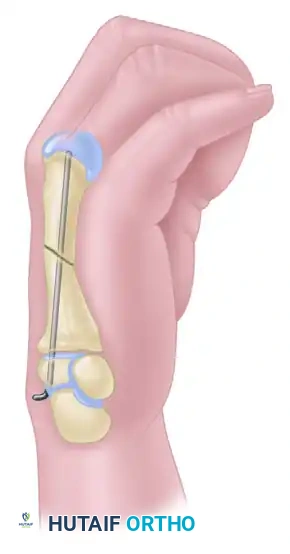
FIGURE 67-36A: Diagram illustrating an irreducible metacarpal shaft fracture requiring open reduction.

FIGURE 67-36B: Introduction of the intramedullary wire through the proximal fragment.
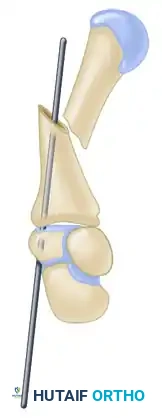
FIGURE 67-36C: Direct open reduction of the fracture fragments.

FIGURE 67-36D: Final seating of the intramedullary wire across the reduced fracture site.
6. Final Seating and Closure
After the fracture is anatomically reduced and the wire is confirmed to be in the subchondral bone of the metacarpal head, the proximal end of the wire must be managed.
Tamp the curved portion of the Kirschner wire slightly deeper if necessary, then cut the wire squarely at the proximal cortex. It is imperative to bury the cut end of the wire deep below the skin and subcutaneous tissue. A prominent wire will cause severe irritation to the overlying extensor tendons, potentially leading to tenosynovitis or tendon rupture. Close the skin with non-absorbable sutures (e.g., 4-0 Nylon).
Surgical Warning: Never leave the proximal K-wire proud in the subcutaneous tissue. The constant gliding of the extensor tendons over a sharp wire end will cause debilitating pain and restrict postoperative digital motion.
Special Considerations: Human Bites (Fight Bites)
Metacarpal neck fractures (particularly of the 3rd, 4th, and 5th digits) are frequently sustained by striking an opponent’s teeth in a fistfight. These "fight bites" are compound (open) injuries and carry a massive risk of deep space infection and septic arthritis due to virulent oral flora (e.g., Eikenella corrodens, Staphylococcus aureus, Streptococcus species).
If a human bite is suspected:
1. Aggressive Irrigation: The wound must be formally extended and aggressively irrigated in the operating room.
2. Arthrotomy: If the MCP joint capsule is breached, a formal arthrotomy and washout are mandatory.
3. Delayed Closure: The traumatic wound must never be closed primarily. It should be left open to heal by secondary intention.
4. Antibiotics: Initiate broad-spectrum intravenous antibiotics immediately, transitioning to targeted oral therapy based on intraoperative cultures.
You Might Also Like