PRINCIPLES OF NONUNION MANAGEMENT
The successful treatment of fracture nonunions remains one of the most formidable challenges in operative orthopedics. A nonunion is classically defined as a fracture that has not healed within nine months and has shown no radiographic progression of healing for three consecutive months. The etiology of nonunion is multifactorial, typically stemming from a failure of the biological environment (atrophic nonunion), a failure of mechanical stability (hypertrophic nonunion), or a combination of both, often complicated by infection.
To achieve osseous union, the surgeon must meticulously address the "diamond concept" of fracture healing: ensuring the presence of osteogenic cells, an osteoconductive scaffold, osteoinductive growth factors, and an optimized mechanical environment. As in fresh fractures, physical forces play a critical role in the success or failure of treatment. Although absolute rigid fixation is not universally necessary—and in some cases, relative stability is preferred to promote secondary bone healing via callus formation—shearing, rotary, and distracting forces must be minimized postoperatively.
INTRAMEDULLARY FIBULAR ALLOGRAFTS
Vascularized and non-vascularized fibular grafts have been utilized extensively and successfully to treat large segmental bone defects. In the upper extremity, particularly in the humerus, atrophic nonunions associated with severe osteopenia or significant bone loss present a unique biomechanical dilemma. Standard plating techniques frequently fail due to screw pull-out from poor-quality cortical bone.
To counteract this, excellent clinical and radiographic results have been obtained in humeral nonunions using a dual-construct technique: intramedullary grafting of the humerus with a structural allograft fibula, augmented with extramedullary plating using a 4.5-mm dynamic compression plate (DCP). This "tube-in-a-tube" construct, popularized by Crosby et al., significantly increases the pull-out strength of the screws, enhances bending and torsional stiffness, and provides a robust osteoconductive scaffold across the pseudarthrosis.
💡 Clinical Pearl: The Biomechanics of the Fibular Strut
When treating osteopenic humeral nonunions, the intramedullary fibular allograft acts as an internal dowel. As the screws from the 4.5-mm compression plate pass through the near cortex of the humerus, traverse the fibular allograft, and engage the far cortex of the humerus, they achieve up to four cortices of purchase per screw. This dramatically reduces the risk of hardware failure in osteoporotic bone.
Surgical Technique: Humeral Nonunion with Fibular Allograft
1. Patient Positioning and Preparation
The patient is positioned either in the beach-chair or supine position, depending on the exact location of the nonunion and surgeon preference. A radiolucent arm board is utilized to allow unimpeded fluoroscopic imaging in orthogonal planes. The entire upper extremity, from the neck to the fingertips, is prepped and draped to allow full manipulation of the arm.
2. Surgical Approach
Approach the humeral shaft anterolaterally. The incision is made along the lateral border of the biceps muscle.
* Proximally, the internervous plane lies between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves).
* Distally, the brachialis muscle is split longitudinally. Because the brachialis has dual innervation (musculocutaneous nerve medially and radial nerve laterally), splitting the muscle longitudinally avoids denervation of either half.
* Critical Step: The radial nerve must be meticulously identified, mobilized, and protected with vessel loops as it spirals across the posterior aspect of the humerus and pierces the lateral intermuscular septum.
3. Preparation of the Nonunion Site
Radically resect all intervening fibrous tissue, pseudarthrosis cartilage, and necrotic bone until punctate bleeding (the "paprika sign") is observed from the cortical ends. Expose the medullary canal proximally and distally. Ream the medullary canal sequentially to accommodate the fibular strut. The reamings should be preserved as they provide excellent autogenous bone graft material.
4. Graft Preparation and Insertion
Select an appropriately sized structural fibular allograft. The graft is contoured and cut to a length that allows it to span the nonunion site adequately, typically extending at least 4 to 5 centimeters into both the proximal and distal medullary canals. Place the contoured allograft fibula into the canal, bridging the defect, and reduce the fracture over the graft.
5. Plate Fixation
Apply a heavy-duty 4.5-mm dynamic compression plate (or locking compression plate, depending on bone quality) to the anterolateral surface of the humerus. Ensure a minimum of 12 cortices of screw fixation (6 cortices proximal, 6 cortices distal to the nonunion). The screws must pass through the humeral cortex, fully engage the intramedullary fibular allograft, and purchase the opposite humeral cortex.
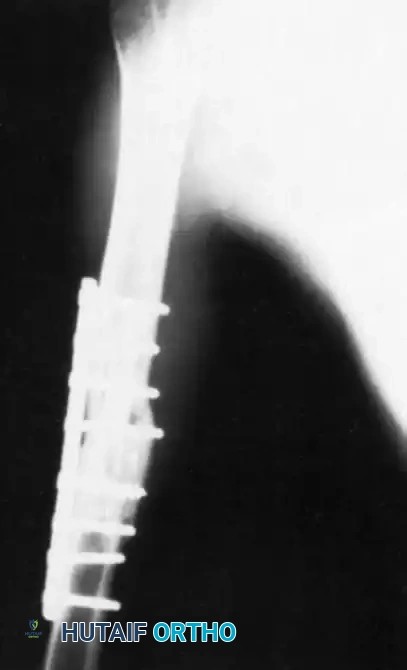
FIGURE 59-9: Anteroposterior radiograph of the humerus 5 months after insertion of a fibular allograft and compression plating with a 4.5-mm dynamic compression plate, revealing evidence of bridging callus formation and incorporation of the allograft. (From Crosby LA, Norris BL, Dao KD, et al: Humeral shaft nonunions treated with fibular allograft and compression plating, Am J Orthop 29:45, 2000.)
Postoperative Protocol
The arm is immobilized in a sling for 6 weeks to protect the construct during the initial phases of soft tissue healing and early graft incorporation. Following this period, the patient is transitioned to a functional cast brace, at which time active and active-assisted range-of-motion exercises for the shoulder and elbow are initiated. Progressive resistance exercises are delayed until radiographic evidence of union is confirmed.
STABILIZATION OF FRAGMENTS: INTERNAL AND EXTERNAL FIXATION
Adequate stabilization is the cornerstone of nonunion surgery. The choice of fixation depends heavily on the classification of the nonunion (hypertrophic vs. atrophic), the condition of the surrounding soft tissue envelope, the presence of active or latent infection, the size of the bone fragments, and the magnitude of any segmental bony defect.
Internal Fixation Strategies
Internal fixation should provide sufficient stability to allow for early mobilization while promoting bone healing without excessive rigidity that might lead to stress shielding.
Plate and Screw Fixation:
Plate fixation, often without the need for supplemental bone grafting, is usually adequate for hypertrophic nonunions. In these cases, the biological potential for healing is robust, but the mechanical environment is too unstable. A compression plate provides absolute stability, shutting down the micromotion that perpetuates the nonunion, allowing the hypertrophic callus to consolidate. This is contingent upon the bone not being severely osteoporotic and the fragments being large enough to afford secure screw fixation.
Intramedullary Nailing:
Intramedullary nailing, particularly statically interlocked nailing, is highly effective in the management of nonunions of the long bones, such as the tibia, femur, and humerus.
⚠️ Surgical Warning: Intramedullary Nailing in Nonunions
A relative contraindication for intramedullary nailing is a current, active intramedullary infection. However, in highly selected cases, intramedullary nailing is frequently successful as a salvage operation even for previously infected nonunions, provided aggressive debridement and appropriate antibiotic therapies are employed.
If alignment is acceptable or if a closed reduction can be obtained, the procedure can be performed without opening the fracture site, thereby preserving the periosteal blood supply. Bone grafting is usually not required in these closed procedures. The act of long-bone intramedullary reaming generates a large volume of corticocancellous autograft material at the fracture site. This material can also be easily harvested using a Reamer-Irrigator-Aspirator (RIA) system, providing voluminous, high-quality graft with minimal donor-site morbidity compared to traditional iliac crest bone grafting.
Intramedullary nails offer load-sharing biomechanics, allowing for early weight-bearing in lower extremity nonunions, and they mitigate the late effects of stress shielding commonly seen with rigid plating.
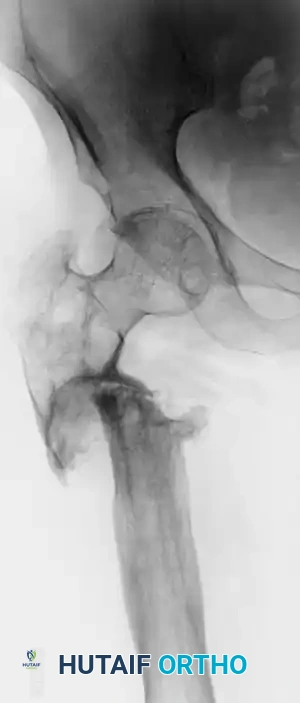
FIGURE 59-10A: Preoperative radiograph of a patient with a recalcitrant subtrochanteric nonunion persisting for 22 years, demonstrating severe sclerosis, deformity, and hardware failure.

FIGURE 59-10B: Postoperative appearance of the same patient treated with a locked second-generation cephalomedullary femoral nail, achieving robust mechanical alignment and stabilization.
External Fixation
External fixation is a powerful, albeit labor-intensive, tool in the treatment of complex nonunions. It is especially indicated for nonunions complicated by active infection, massive segmental bone defects, limb shortening, and complex multi-planar deformities.
The Ilizarov circular external fixator utilizes the principles of distraction osteogenesis. By applying tension-stress to the bone, the Ilizarov method stimulates the formation of new bone tissue. Hybrid circular frames attached to uniplanar external fixators have decreased some of the technical difficulties associated with traditional full-circular frames.
Advantages of external fixation include:
* Minimal Invasiveness: It does not disturb the delicate soft tissues and periosteal blood supply surrounding the nonunion site.
* Adjustability: It allows for the gradual correction of angular deformities and limb-length discrepancies postoperatively.
* Infection Control: It provides stable fixation without placing foreign hardware directly into an infected medullary canal.
MANAGEMENT OF INFECTED NONUNIONS
Infected nonunions represent a limb-threatening pathology. The classification system developed by Cierny et al. is indispensable for preoperative planning. This system categorizes osteomyelitis based on the anatomic status of bone involvement (Type 1: Medullary, Type 2: Superficial, Type 3: Localized, Type 4: Diffuse) and the physiological competency of the host (Class A: Normal, Class B: Compromised, Class C: Treatment worse than the disease).
Accurate diagnosis relies on multiple direct deep tissue cultures taken from the fracture site during surgery; superficial swab cultures of the skin or sinus tracts are notoriously unreliable and often reflect colonizing flora rather than the true pathogen.
Conventional Treatment Protocol
The primary objective of the conventional method is to convert an actively infected, draining nonunion into a sterile, non-draining environment, followed by secondary procedures to promote osseous union. This staged approach often requires a year or more to complete.
- Radical Debridement (Saucerization): The first and most critical operation involves thorough saucerization. All foreign material, loose hardware, infected granulation tissue, and devitalized sequestrum must be radically excised until healthy, bleeding bone is reached. This converts a necrotic environment into a vascularized bed capable of supporting an immune response and subsequent grafting.
- Dead Space Management: The resulting bony defect is typically managed with antibiotic-impregnated polymethylmethacrylate (PMMA) spacers, which provide high local concentrations of antibiotics while inducing a vascularized pseudomembrane (the Masquelet technique).
- Stabilization: While internal fixation has biomechanical advantages, placing permanent foreign materials into an actively infected bed is generally contraindicated. External fixation is the preferred method of stabilization during the eradication phase. With rare exceptions, an intramedullary nail should not be used in the presence of active, purulent medullary infection.
- Reconstruction: Once infection is eradicated (evidenced by normalized inflammatory markers and negative repeat cultures), the PMMA spacer is removed, and the defect is reconstructed using autogenous bone grafting, vascularized fibular grafts, or bone transport techniques.
BIOPHYSICAL ADJUNCTS TO FRACTURE HEALING
When surgical intervention is contraindicated, or as an adjunct to operative stabilization, biophysical stimulation has proven highly effective in accelerating bone regeneration and treating delayed unions and nonunions.
Low-Intensity Pulsed Ultrasound (LIPUS)
Xavier and Duarte in Brazil first reported the successful use of low-intensity pulsed ultrasound (30 mW/cm²) to heal nonunions in humans in 1983. The mechanism of action is rooted in mechanotransduction. Ultrasound waves create micro-mechanical strains within the fracture callus, which stimulates the genes involved in inflammation and bone regeneration.
Furthermore, LIPUS increases local blood flow through the dilation of capillaries and the enhancement of angiogenesis, thereby increasing the delivery of essential nutrients and osteoprogenitor cells to the fracture site. Studies also indicate that LIPUS enhances chondrocyte proliferation and differentiation, accelerating endochondral ossification.
- Clinical Efficacy: The overall success rate of LIPUS for nonunions and delayed unions in the United States ranges from 70% to 93%.
- Protocol: The standard protocol requires the patient to apply the ultrasound transducer to the skin overlying the fracture site for 20 minutes once daily.
- Economic Impact: Rubin et al. (2001) demonstrated in double-blind prospective clinical trials that LIPUS can reduce the healing time of fresh fractures by 40%. They estimated a significant cost savings of $15,000 per case when used early in high-risk fresh fractures by preventing the progression to nonunion. A systematic review and meta-analysis by Busse et al. further corroborated the significant benefit of LIPUS in fracture management.
Electrical and Electromagnetic Stimulation
Improvements in electrical and electromagnetic bone growth stimulators have expanded the non-operative armamentarium for nonunion management. These devices are typically used in conjunction with cast immobilization and protected weight-bearing. They are particularly advantageous in the management of infected nonunions where further surgical intervention carries high morbidity.
Three primary modalities exist:
1. Invasive: Requires surgical implantation of a cathode directly into the nonunion site, with an anode placed in the adjacent soft tissue (Direct Current).
2. Semi-invasive: Involves the percutaneous insertion of multiple Kirschner-wire electrodes into the bone.
3. Non-invasive (Pulsed Electromagnetic Fields - PEMF): Developed by Bassett et al., this method utilizes inductive coupling via external coils. It is highly effective and can be used safely in the presence of active infection.
Devices utilizing inductive coupling vary in configuration, employing either a Helmholtz coil design or a U-shaped coil. U-shaped coils applied for 3 or more hours per day have successfully healed nonunions of both long and short bones, open and closed fractures, long-standing recalcitrant nonunions, infected nonunions, and defects with fracture gaps up to 1 cm.
Various waveforms, including direct current, square-wave generators, and pulsed bursts, have proven beneficial. For instance, square-wave signals are highly effective for tibial delayed unions; however, the prolonged immobilization required can pose rehabilitation challenges. DeHaas et al. recommended that true pseudarthroses (nonunions with a distinct fluid-filled gap and synovial lining) be treated with surgical debridement, bone grafting, and internal fixation prior to the application of electrical stimulation, as stimulation alone cannot bridge a true synovial pseudarthrosis.
Extracorporeal Shock-Wave Therapy (ESWT)
Extracorporeal shock-wave therapy remains a popular non-invasive modality in Europe and is gaining traction in the United States. ESWT utilizes high-energy acoustic waves to induce microtrauma at the nonunion site, theoretically stripping away sclerotic fibrous tissue and stimulating a fresh inflammatory response and neovascularization. While it shows promise, its use is still being optimized as the orthopedic community awaits more conclusive Level I evidence regarding standardized dosing and specific indications.
