ADVANCED FOREFOOT AND MIDFOOT RECONSTRUCTION: NEUROMA EXCISION AND CAVUS DEFORMITY
The surgical management of forefoot and midfoot pathologies requires a profound understanding of both peripheral nerve anatomy and complex structural biomechanics. This comprehensive academic guide details the operative execution of interdigital neuroma excision utilizing a longitudinal plantar approach—specifically indicated for recurrent neuromas—and provides a foundational biomechanical analysis of the cavus foot deformity.
Designed for orthopedic residents, fellows, and practicing consultants, this text strictly adheres to evidence-based principles, outlining precise surgical steps, anatomical considerations, and postoperative protocols to optimize patient outcomes and minimize iatrogenic complications.
INTERDIGITAL NEUROMA EXCISION USING LONGITUDINAL PLANTAR INCISION
Interdigital neuromas (commonly referred to as Morton’s neuromas) represent a symptomatic perineural fibrosis of the common digital nerve, most frequently occurring in the third intermetatarsal space. While primary neuromas are traditionally approached via a dorsal incision to avoid plantar scarring, the longitudinal plantar approach is the gold standard for recurrent interdigital neuromas.
When a neuroma recurs, the previously resected nerve stump retracts proximally into the plantar vault, tethered by scar tissue. A dorsal approach in the revision setting is fraught with difficulty, poor visualization, and a high risk of incomplete resection. The plantar approach provides direct, unhindered anatomical access to the proximal nerve stump, allowing for adequate proximal resection without the need to violate the deep transverse intermetatarsal ligament (DTIML).
Pathoanatomy and Biomechanics
The common digital nerve travels plantarly to the DTIML. During the terminal stance phase of gait, the toes dorsiflex, pulling the digital nerves distally against the unyielding distal edge of the DTIML. This repetitive mechanical microtrauma, combined with ischemic changes and bursal inflammation, leads to endoneurial edema, axonal degeneration, and extensive perineural fibrosis.
Clinical Pearl: True interdigital neuromas are not neoplastic. Histologically, they demonstrate severe perineural fibrosis, demyelination, and the presence of Renaut bodies (subperineurial hyalinized structures indicative of chronic nerve compression).
Indications for the Plantar Approach
- Recurrent Interdigital Neuroma: The primary indication. The proximal stump is easily identified in virgin tissue proximal to the previous dorsal surgical bed.
- Concomitant Plantar Pathology: When simultaneous access to plantar structures (e.g., plantar plate repair) is required.
- Proximal Lesions: Unusually proximal primary neuromas that cannot be adequately accessed dorsally.
Preoperative Preparation and Positioning
- Anesthesia: The procedure is typically performed under regional anesthesia (ankle block or popliteal block) combined with monitored anesthesia care (MAC) or general anesthesia, depending on patient preference and comorbidities.
- Positioning: The patient is placed in the supine position.
- Tourniquet: A well-padded calf or thigh tourniquet is applied. The limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated (typically 250–300 mmHg) to ensure a bloodless surgical field, which is critical for identifying delicate neural structures amidst plantar fat.
- Assistant Role: An assistant is positioned to dorsiflex the ankle to a neutral position, which places the plantar aponeurosis under tension, facilitating precise dissection.
Surgical Technique: Step-by-Step (Technique 86-4)
1. Incision and Superficial Dissection
Begin by identifying the affected web space. With the ankle held in neutral dorsiflexion, initiate a 3- to 4-cm longitudinal plantar incision. The incision should begin just proximal to the web space (avoiding the weight-bearing pad of the metatarsal heads if possible) and extend in a proximal direction.
Surgical Warning: Never use a transverse plantar incision for neuroma excision. Transverse incisions transect the longitudinal fibers of the plantar aponeurosis and are highly prone to painful, hypertrophic scarring during weight-bearing.
Deepen the incision through the skin and subcutaneous tissue. The plantar fat pad is highly lobulated and dense. At this stage, the introduction of a small, self-retaining retractor (such as a Weitlaner or Gelpi) is an excellent aid to maintain exposure through the thick adipose layer overlying the plantar aponeurosis.
2. Deep Dissection and Aponeurotic Release
Identify the glistening, longitudinal fibers of the plantar aponeurosis. Make a longitudinal incision directly in line with the skin incision through the aponeurosis. Retract the aponeurotic edges to expose the underlying intrinsic musculature and the neurovascular bundles.
3. Nerve Isolation and Neuroma Identification
Utilizing blunt dissection in a longitudinal plane (often with a small hemostat or dissecting scissors), carefully separate the adipose tissue to identify the common digital nerve proximally, in an area of unscarred tissue.
Once the healthy proximal nerve is identified, trace it distally toward the web space. You will encounter the neuromatous enlargement (or the bulbous recurrent stump) just proximal to the emergence of the proper digital branches that supply the adjacent sides of the toes.
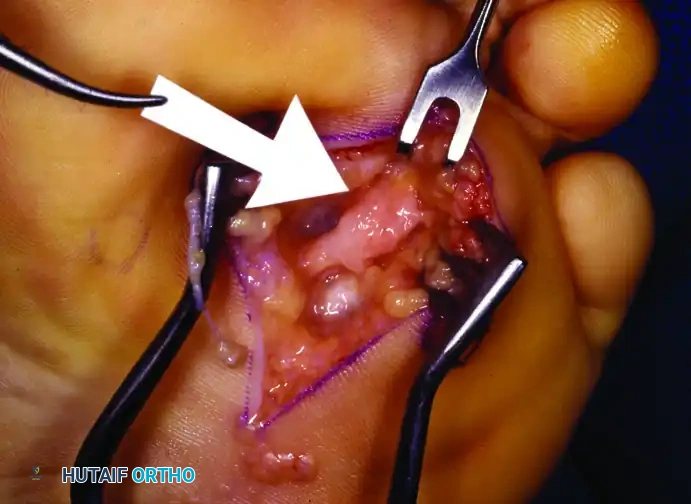
Figure 86-12A: Plantar incision for “recurrent” interdigital neuroma with communicating nerve entering the neuroma (arrow).
4. Resection of the Neuroma
The critical step in preventing further recurrence is ensuring the nerve is resected far enough proximally so that the new stump retracts deep into the intrinsic muscles of the foot, away from weight-bearing pressure and the DTIML.
- Carefully dissect the neuroma free from surrounding adhesions.
- Resect the nerve 2 to 3 cm proximal to the deep transverse intermetatarsal ligament.
- Crucial Anatomical Note: When utilizing the plantar approach, incising the deep transverse intermetatarsal ligament that lies dorsal to the neuroma is unnecessary. Preserving the DTIML maintains the structural integrity of the transverse metatarsal arch and prevents splaying of the forefoot.
5. Hemostasis and Closure
Prior to closure, deflate the tourniquet. Achieving meticulous hemostasis is paramount, as a postoperative plantar hematoma can lead to severe fibrosis, delayed wound healing, and a painful plantar scar. Use bipolar electrocautery for precise hemostasis.
Close the skin using interrupted nonabsorbable sutures (e.g., 3-0 or 4-0 nylon).
Pitfall Avoidance: During closure, be meticulously careful not to inadvertently include any small dorsal or plantar sensory nerve branches within the suture loop, as this will create a painful iatrogenic entrapment neuropathy.

Figure 86-12B: Final skin closure after neuroma excision using interrupted nonabsorbable sutures.
Postoperative Care Protocol
The success of a plantar approach relies heavily on strict adherence to postoperative offloading to ensure the plantar scar heals without hypertrophy or dehiscence.
- Immediate Postoperative Phase (0-48 Hours): A slightly bulky "sandwich" compression dressing is applied over a petroleum jelly–impregnated gauze pad, wrapped with an elastic bandage providing mild compression. The patient must rest with maximal elevation of the extremity. Strict bathroom privileges only are enforced to minimize dependent edema and hematoma formation.
- Early Ambulation (2 Days - 2 Weeks): Walking is allowed as tolerated, but strictly in a postoperative wooden-soled shoe. The patient is explicitly instructed to walk on the heel of the affected foot, completely offloading the forefoot.
- Note: Wound complications from early weight-bearing are exceedingly rare if the wooden-soled shoe is used correctly and heel-weight-bearing is maintained. If patient compliance is questionable, crutch walking with non-weight-bearing status is strongly encouraged.
- Suture Removal (2 to 3 Weeks): Sutures are removed between 14 and 21 days, depending on the clinical appearance of the wound. Following removal, adhesive plastic strips (Steri-Strips) are placed across the wound for an additional week to reduce tension on the healing scar.
- Transition Phase (3 to 7 Weeks): The wooden-soled shoe is maintained for a total of 2 to 3 weeks. Following this, the patient transitions to a wide toe box, soft-vamp shoe for an additional 3 to 4 weeks to accommodate residual swelling and prevent mediolateral compression of the metatarsal heads.
Controversies: Endoscopic Decompression
While endoscopic release of the transverse metatarsal ligament has gained popularity in some circles as a minimally invasive alternative for neuroma management, current academic consensus remains cautious. We currently do not routinely utilize endoscopy for decompression or excision of an interdigital neuroma due to a lack of high-level, long-term evidence regarding its efficacy and safety compared to open excision. Although encouraging short-term results have been reported in isolated studies, the risk of incomplete release, iatrogenic nerve injury, and failure to address the underlying perineural fibrosis makes open excision the definitive standard of care.
THE CAVUS FOOT DEFORMITY: BIOMECHANICS AND CLINICAL RECOGNITION
Transitioning from isolated forefoot nerve pathology to global foot biomechanics, the cavus foot represents one of the most challenging structural deformities encountered by the orthopedic surgeon. In its simplest definition, a cavus foot is one with an abnormally high longitudinal arch. However, this simplistic definition belies a highly complex, multi-planar spectrum of deformities that profoundly alter lower extremity biomechanics.
As the classic orthopedic adage states: Although pes cavus with multiple deformities is difficult to define, it is easily recognized; however, it is definitely not easy to treat operatively or nonoperatively.
The Spectrum of Deformities
A true cavus foot is rarely an isolated high arch; it is a synergistic cascade of contractures and bony malalignments. The classic presentation includes:
- Digital Deformities (Claw Toes): Hyperextension of the toes at the metatarsophalangeal (MTP) joints combined with hyperflexion at the proximal and distal interphalangeal (IP) joints. This is driven by an imbalance between the strong extrinsic extensors/flexors and the weak intrinsic muscles (lumbricals and interossei).
- Forefoot Pronation and Adduction (Forefoot Valgus): The first ray is rigidly plantarflexed. This plantarflexed first ray acts as a kickstand, driving the forefoot into a valgus position relative to the midfoot.
- Midfoot Architecture: A prominent, "bony" dorsum of the midfoot is visible, often leading to shoe-wear difficulties and dorsal osteophyte formation. Conversely, the medial plantar aspect of the foot often exhibits deep, wrinkled skin folds due to the chronic contracture of the medial column.
- Column Length Discrepancy: The deformity results in a functionally lengthened lateral border of the foot and a shortened, contracted medial border.
- Plantar Keratoses: Due to the rigid plantarflexion of the metatarsals and the loss of the shock-absorbing capacity of the arch, severe, painful calluses develop beneath the metatarsal heads (particularly the first and fifth).
- Hindfoot Varus: The heel is driven into a varus deformity. Initially, this varus may be flexible—a compensatory mechanism driven by the rigid plantarflexed first ray (the tripod effect). Over time, due to adaptive shortening of the subtalar joint capsule and ligaments, this varus deformity becomes rigid and fixed.
- Equinus Contracture: Tightness of the Achilles tendon or gastrocnemius-soleus complex is nearly universal, presenting with or without a clinical equinus contracture.
Biomechanical Pathogenesis: The Tripod Concept
Understanding the cavus foot requires mastering the "tripod concept" of foot biomechanics. The foot rests on three points: the heel, the first metatarsal head, and the fifth metatarsal head.
In a neurologically driven cavus foot (such as in Charcot-Marie-Tooth disease), the peroneus longus overpowers a weak tibialis anterior, rigidly plantarflexing the first ray. When the patient bears weight, this rigid first ray hits the ground prematurely. To allow the lateral side of the foot (the fifth metatarsal) to contact the ground, the entire hindfoot must tilt into varus.
Clinical Pearl: The Coleman Block Test
To determine if the hindfoot varus is flexible (driven by the forefoot) or fixed (rigid subtalar joint), the Coleman block test is mandatory. The patient stands with their heel and lateral border of the foot on a 1-inch wooden block, allowing the first metatarsal to drop off the edge. If the hindfoot varus corrects to neutral, the deformity is flexible and driven entirely by the plantarflexed first ray. If the varus persists, the subtalar joint is rigidly contracted. This distinction dictates the entire surgical reconstructive algorithm.
Diagnostic Evaluation and Treatment Philosophy
Because bilateral cavus feet are highly associated with underlying neurological disorders (e.g., Charcot-Marie-Tooth disease, Friedreich's ataxia, spinal dysraphism, or tethered cord), a thorough neurological workup, including electromyography (EMG), nerve conduction studies (NCS), and potentially spinal MRI, is mandatory before any surgical intervention.
Treatment is notoriously difficult. Nonoperative management focuses on accommodating the deformity with custom orthotics featuring lateral wedges, first ray cutouts, and deep heel cups, alongside extra-depth shoes to accommodate claw toes.
Operative intervention is reserved for progressive deformities, intractable pain, or recurrent lateral ankle instability. Surgical reconstruction is highly individualized but generally follows a stepwise approach:
1. Soft Tissue Releases: Plantar fascia release (Steindler stripping) and Achilles tendon lengthening.
2. Osseous Correction of the Forefoot: Dorsiflexion osteotomy of the first metatarsal to eliminate the forefoot valgus drive.
3. Osseous Correction of the Hindfoot: Lateralizing calcaneal osteotomy for flexible varus, or triple arthrodesis for rigid, arthritic deformities.
4. Tendon Transfers: Transferring the peroneus longus to the peroneus brevis, or the Jones transfer (EHL to the first metatarsal neck) to restore dynamic muscle balance and prevent recurrence.
In conclusion, whether addressing the localized perineural fibrosis of a recurrent interdigital neuroma via a meticulous plantar approach, or deconstructing the multi-planar biomechanical collapse of a cavus foot, the orthopedic surgeon must rely on a foundation of precise anatomical knowledge, rigorous clinical evaluation, and flawless surgical execution.
