INTRODUCTION TO AMPUTATION SURGERY
Historically viewed as a failure of medical or surgical intervention, amputation is now universally recognized by orthopaedic surgeons as a definitive, reconstructive, and often life-saving procedure. The primary goal of amputation surgery is not merely the resection of diseased or non-viable tissue, but the creation of a dynamic, functional residual limb (stump) optimized for prosthetic fitting and maximal patient rehabilitation.
The National Center for Health Statistics estimates that more than 300,000 patients with amputations live in the United States. The incidence of amputations performed annually continues to rise, driven predominantly by an aging population and the global epidemic of diabetes mellitus. In the Western world, greater than 90% of amputations are secondary to peripheral vascular disease (PVD). Conversely, in younger demographics, high-energy trauma remains the leading cause, followed by primary musculoskeletal malignancies.
The only absolute indication for amputation is irreversible ischemia in a diseased or traumatized limb. However, amputation may also be urgently required to preserve life in patients with uncontrollable, ascending infections, or it may represent the most oncologically sound option for specific aggressive tumors—though modern advances in orthopaedic oncology now facilitate limb salvage in the majority of cases.
PERIPHERAL VASCULAR DISEASE AND DIABETES
Peripheral vascular disease, with or without concomitant diabetes mellitus, is the most frequent indication for amputation, typically presenting in individuals aged 50 to 75 years.
Systemic Considerations and Preoperative Optimization
The orthopaedic surgeon must approach the dysvascular patient holistically. If vascular disease has progressed to the point of requiring major limb amputation, the microvascular and macrovascular pathology is rarely confined to the involved extremity. These patients invariably suffer from concomitant atherosclerotic disease processes affecting the cerebral vasculature, coronary arteries, and renal systems.
Clinical Pearl: A multidisciplinary approach is mandatory. Prior to any elective or semi-elective amputation for PVD, a formal vascular surgery consultation is indicated. Advanced endovascular and open bypass techniques now allow for the revascularization of limbs that were historically deemed unsalvageable.
Approximately 50% of amputations for PVD are performed on diabetic patients. The most significant predictor of eventual amputation in the diabetic population is peripheral neuropathy, clinically quantified by insensitivity to the Semmes-Weinstein 5.07 monofilament. Additional documented risk factors include:
* Prior cerebrovascular accident (stroke).
* Prior major or minor contralateral amputation.
* Decreased transcutaneous oxygen tension (TcPO2 < 30 mm Hg indicates poor healing potential).
* Decreased ankle-brachial index (ABI < 0.45 is associated with high failure rates).
Nutritional and Immunological Parameters
Surgical site healing in the dysvascular patient is highly dependent on baseline nutritional and immunological status.
Surgical Warning: The risk of catastrophic wound complications and dehiscence is exponentially increased in patients presenting with a serum albumin level of less than 3.5 g/dL or a total lymphocyte count (TLC) of less than 1,500 cells/mL. Aggressive nutritional supplementation is required preoperatively when feasible.
Perioperative mortality rates for amputation in the setting of severe PVD are historically reported at up to 30%, with a staggering 40% of patients succumbing to systemic cardiovascular events within 2 years postoperatively. Furthermore, critical ischemia will develop in the contralateral lower extremity in 30% of surviving patients.
Biomechanics and Level Selection
Determining the appropriate level of amputation requires a delicate balance between ensuring adequate vascularity for wound healing and preserving maximal limb length for biomechanical efficiency. The metabolic energy required for ambulation is inversely proportional to the length of the remaining limb.
* Transtibial Amputation (Below Knee): Increases baseline metabolic demand by approximately 25%.
* Transfemoral Amputation (Above Knee): Increases baseline metabolic demand by 65% or more.
In an elderly patient with significant cardiopulmonary comorbidities, the energy reserves may not permit ambulation if a proximal (transfemoral) amputation is performed. If the patient possesses sufficient cognitive function, balance, and upper extremity strength, amputation should be performed at the most distal level that guarantees healing. Conversely, a non-ambulatory, bedbound patient with a severe knee flexion contracture should undergo a transfemoral amputation or knee disarticulation to improve bed mobility, simplify nursing care, and eliminate the risk of proximal tibial skin breakdown.
TRAUMA AND THE MANGLED EXTREMITY
Trauma remains the leading indication for amputation in the younger, active population, with a higher prevalence in males due to vocational and avocational hazards. Because these patients are typically healthy, the loss of a limb has profound psychological, functional, and economic implications.
Indications for Primary Amputation in Trauma
The only absolute indication for primary amputation in the trauma setting is an irreparable vascular injury resulting in a prolonged ischemic limb. However, with modern advancements in prehospital resuscitation, microvascular free tissue transfer, and Ilizarov bone transport techniques, orthopaedic surgeons frequently face complex dilemmas regarding limb salvage versus primary amputation.
Lange’s criteria provide a widely accepted framework for decision-making in severe lower extremity trauma.
Absolute Indications for Amputation (Lange):
* Type III-C open tibial fractures with complete, anatomically verified disruption of the posterior tibial nerve.
* Crush injuries with a warm ischemia time exceeding 6 hours.
Relative Indications for Amputation:
* Polytrauma with serious associated life-threatening injuries.
* Severe ipsilateral foot and ankle crush injuries.
* Anticipated protracted surgical course requiring multiple free flaps and massive tibial bone reconstruction.
The Mangled Extremity Severity Score (MESS)
To introduce objectivity into the highly subjective realm of limb salvage, several scoring systems have been developed. The Mangled Extremity Severity Score (MESS) remains the most clinically utilized tool. It evaluates four distinct parameters:
1. Skeletal / Soft-Tissue Injury:
* Low energy (Stab wounds, simple closed fractures): 1 point
* Medium energy (Open/multiple-level fractures, dislocations): 2 points
* High energy (Close-range shotgun, high-velocity gunshot): 3 points
* Massive crush (Logging, railroad, oil rig accidents): 4 points
2. Limb Ischemia: (Points doubled if ischemia exceeds 6 hours)
* None (Pulsatile limb): 0 points
* Mild (Diminished pulses, no signs of ischemia): 1 point
* Moderate (No Doppler pulse, sluggish refill, paresthesia): 2 points
* Advanced (Pulseless, cool, paralyzed, numb): 3 points
3. Shock (Hemodynamics):
* Normotensive (Stable in field and OR): 0 points
* Transiently hypotensive (Responsive to IV fluids): 1 point
* Prolonged hypotension (Systolic BP < 90 mm Hg in field, responsive only in OR): 2 points
4. Patient Age:
* < 30 years: 0 points
* 30 to 50 years: 1 point
* > 50 years: 2 points
Clinical Pearl: A MESS score of 6 or less is generally consistent with a salvageable limb. A score of 7 or greater is highly predictive of eventual amputation. While not a substitute for clinical judgment, calculating and documenting the MESS score is a critical medicolegal and clinical step.
Life Over Limb: The Polytrauma Patient
Amputation of a severely mangled extremity is often necessary to preserve the patient's life. Heroic attempts to salvage a dying limb can precipitate a systemic inflammatory response syndrome (SIRS), metabolic overload, myoglobinuric renal failure, and secondary multi-organ dysfunction syndrome (MODS). An Injury Severity Score (ISS) greater than 50 is widely considered an absolute contraindication to protracted limb salvage attempts.
Psychological and Functional Trade-offs
The surgeon must engage in extensive, transparent shared decision-making with the patient and their family. Patients initially fixate on "saving the limb" without comprehending the grueling reality of limb salvage: years of external fixation, multiple free flaps, chronic osteomyelitis, opioid dependency, and severe social isolation.
Modern prosthetics often provide superior functional outcomes compared to a stiff, painful, and insensate "salvaged" limb. Early amputation and prosthetic fitting correlate with decreased morbidity, fewer total operations, reduced hospital costs, and a significantly faster return to the workforce.
THERMAL INJURIES: BURNS AND FROSTBITE
Burns and Electrical Injuries
Severe thermal or high-voltage electrical injuries to an extremity frequently necessitate amputation. Electrical injuries are particularly deceptive, as deep muscle necrosis often extends far proximally to the visible cutaneous burn. Management mandates aggressive, early surgical debridement, prophylactic fasciotomies to prevent compartment syndrome, and serial evaluations in the operating room.
Delayed amputation of an unsalvageable burned limb drastically increases the risk of invasive local sepsis, systemic bacteremia, myoglobin-induced acute kidney injury, and mortality.
Frostbite
Frostbite involves the actual crystallization of intra- and extracellular fluid within the extremities, commonly affecting high-altitude climbers, winter sports enthusiasts, and vulnerable populations such as the homeless or those with severe psychiatric disorders.
Tissue necrosis in frostbite occurs via two distinct mechanisms:
1. Direct Cellular Toxicity: Formation of ice crystals disrupts cellular membranes.
2. Microvascular Ischemia: Endothelial damage leads to profound localized vasoconstriction, microvascular thrombosis, and subsequent gangrene.
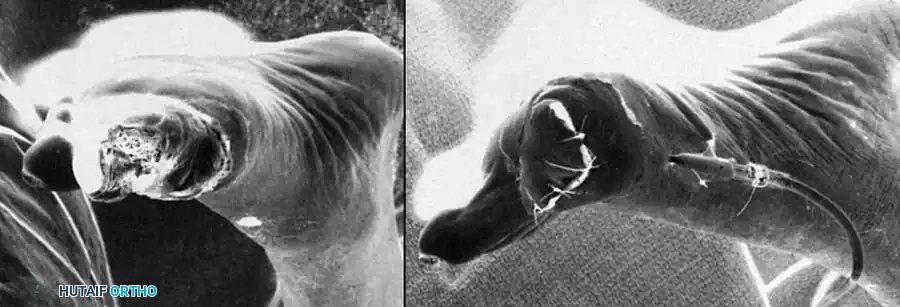
Clinical presentation of severe frostbite progressing to dry gangrene of the forefoot. Note the clear demarcation line separating viable tissue from mummified, necrotic tissue, which dictates the eventual level of amputation.
Acute Management of Frostbite:
* Rapid Rewarming: The cornerstone of acute treatment is rapid rewarming in a circulating water bath at 40ºC to 44ºC. This process is exquisitely painful and requires aggressive parenteral opioid analgesia.
* Thrombolytic Therapy: If digital perfusion is absent post-rewarming, the administration of tissue plasminogen activator (tPA) or the use of regional sympathetic blockade may salvage at-risk tissue.
* Wound Care: Tetanus prophylaxis is mandatory. Clear blebs may be aspirated or treated with topical aloe vera to inhibit thromboxane production. Hemorrhagic blebs should be left intact or treated with silver sulfadiazine (Silvadene).
* Surgical Timing: "Freeze in January, amputate in July." Unless wet gangrene or systemic sepsis develops, surgical amputation should be delayed for weeks to months to allow for complete auto-demarcation of the necrotic tissue, thereby preserving maximal limb length.
INFECTION, ONCOLOGIC RESECTION, AND LIMB SALVAGE
In cases of chronic osteomyelitis, infected arthroplasty, or massive oncologic resections, amputation may be required after multiple failed limb salvage attempts. In staged procedures where local infection control is paramount before final closure or targeted osseointegration, orthopaedic surgeons frequently utilize antibiotic-impregnated polymethylmethacrylate (PMMA) cement spacers.

A custom-molded, antibiotic-impregnated PMMA cement spacer fashioned over a metallic endosteal stem. This construct provides high local concentrations of antibiotics while maintaining soft-tissue tension and dead-space management.
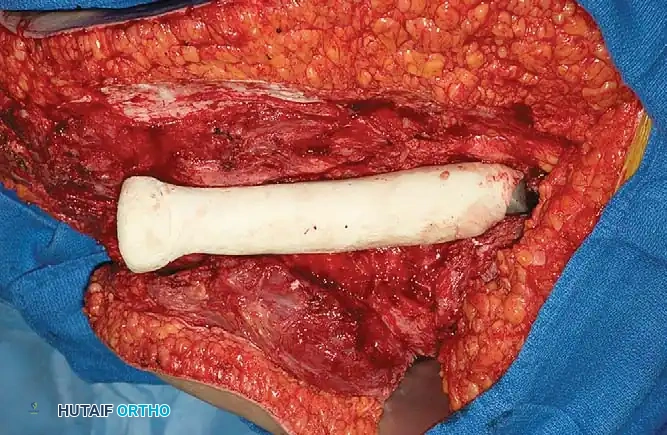
Intraoperative view demonstrating the insertion of the antibiotic cement spacer into the femoral canal. This technique is critical in staged revisions or when preparing a heavily contaminated amputation stump for delayed primary closure.
SURGICAL PRINCIPLES OF AMPUTATION
Regardless of the indication, meticulous surgical technique is paramount to creating a durable, painless residual limb capable of withstanding the shear and compressive forces of a prosthetic socket.
1. Positioning and Preparation
- The patient is positioned supine on a radiolucent operating table.
- A pneumatic tourniquet is applied proximally; however, tourniquet inflation is strictly contraindicated in patients with severe peripheral vascular disease, as it may induce further ischemic injury to the compromised skin flaps.
- The entire limb is prepped and draped free to allow for intraoperative assessment of joint range of motion and flap mobility.
2. Surgical Approach and Flap Design
- Transtibial Amputation: The standard approach utilizes a long posterior myocutaneous flap (Burgess technique). The posterior flap, supplied by the sural artery, provides robust, well-vascularized gastrocnemius muscle to pad the distal tibia.
- Transfemoral Amputation: Equal anterior and posterior fish-mouth flaps are typically utilized, ensuring the scar does not lie directly over the distal femur.
3. Bone and Nerve Management
- Osteotomy: The bone is transected using an oscillating saw under continuous saline irrigation to prevent thermal necrosis. In a transtibial amputation, the anterior cortex of the tibia must be meticulously beveled at a 45-degree angle, and all sharp edges rasped smooth to prevent skin ulceration. The fibula is cut 1 to 2 cm shorter than the tibia.
- Nerve Handling: Prevention of symptomatic neuromas is critical. Major nerves (e.g., tibial, common peroneal, sciatic) are isolated, gently distracted distally, ligated, and sharply transected with a scalpel. They are then allowed to retract deep into healthy muscle beds, well away from the surgical scar and weight-bearing surfaces.
4. Myodesis and Closure
- Myodesis: To maintain physiological muscle tension and provide a dynamic distal cushion, the muscle fascia is sutured directly to the bone via drill holes (myodesis). In a transfemoral amputation, securing the adductor magnus to the lateral femur is critical to prevent the limb from resting in an abducted position, which severely compromises prosthetic gait.
- Closure: The wound is closed in multiple layers over a closed-suction drain. Skin edges must be approximated without tension using non-reactive sutures or staples.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative phase is as critical as the surgical execution. The immediate goals are edema control, joint contracture prevention, and psychological support.
- Rigid Removable Dressings (RRD): Application of a cast or RRD in the operating room protects the vulnerable stump from trauma, significantly reduces postoperative edema, and accelerates wound healing.
- Contracture Prevention: Patients must be educated to avoid placing pillows under the knee (transtibial) or prolonged sitting (transfemoral) to prevent debilitating flexion contractures.
- Prosthetic Fitting: Once the surgical wound is fully healed and edema has stabilized (typically 4 to 8 weeks postoperatively), the patient is fitted with a preparatory prosthesis.
- Pain Management: Multimodal analgesia, including gabapentinoids and regional nerve blocks, is utilized to manage acute surgical pain and mitigate the development of phantom limb pain, a complex neuropathic phenomenon experienced by the majority of amputees.
