Operative Management of the Proximal Tibiofibular Joint and Chronic Knee Dislocations

Key Takeaway
The proximal tibiofibular joint is a complex articulation essential for ankle and knee biomechanics. Subluxations are classified as idiopathic or posttraumatic. While idiopathic cases often resolve nonoperatively, chronic posttraumatic instability may require proximal fibular resection. Similarly, chronic knee dislocations demand meticulous open reduction, balancing soft tissue releases with the potential need for delayed arthroplasty or arthrodesis to restore functional stability and alignment in the severely compromised joint.
PROXIMAL TIBIOFIBULAR JOINT SUBLUXATION AND DISLOCATION
The proximal tibiofibular joint (PTFJ) is a highly constrained synovial articulation that plays a critical, albeit often underappreciated, role in the biomechanics of the lower extremity. It serves to dissipate torsional stresses applied at the ankle, provides lateral stability to the knee via its ligamentous attachments, and acts as a strut for the origin of the musculature of the lateral and anterior compartments of the leg.
Ogden classically described two primary etiologic classifications of proximal tibiofibular subluxations or dislocations: idiopathic and posttraumatic.
Idiopathic Subluxation
The idiopathic variant occurs predominantly in preadolescent or adolescent children, with a higher predilection in females. It may also manifest in patients in their late fourth and fifth decades who exhibit generalized ligamentous laxity (e.g., Ehlers-Danlos or Marfan syndrome).
Idiopathic subluxation is generally a self-limiting condition and is overwhelmingly treated nonoperatively. If the condition becomes acutely symptomatic, initial management should consist of cast immobilization or bracing to allow capsular inflammation to subside. Surgical intervention in the young, idiopathic patient is strongly discouraged due to the high rate of spontaneous resolution as skeletal maturity is reached. However, in older patients where the subluxation becomes chronic, painful, and refractory to prolonged immobilization, surgical intervention may be warranted.
Posttraumatic Chronic Subluxation
Posttraumatic, chronic subluxation of the proximal fibula typically follows high-energy trauma or severe twisting injuries that disrupt the anterior and posterior capsular ligaments of the PTFJ, often in conjunction with injury to the fibular collateral ligament (FCL) of the knee.
An old, unreduced dislocation of the proximal fibula may not inherently impair function enough to necessitate surgical treatment. Observation is the standard of care unless specific clinical criteria are met.
Surgical Indications for Posttraumatic PTFJ Instability:
* The old injury places abnormal biomechanical strain on the knee joint, resulting in chronic lateral-sided pain and posterolateral instability.
* The dislocated head of the fibula remains excessively prominent, subjecting it to repeated direct microtrauma.
* Clinical signs and symptoms of common peroneal nerve irritation or compression neuropathy are present.
Biomechanics and the Rationale for Resection over Fusion
When surgical treatment is definitively indicated for chronic, symptomatic subluxation of the PTFJ, resection of the proximal fibula is considered the gold-standard procedure.
Historically, arthrodesis (fusion) of the PTFJ was attempted; however, Ogden’s biomechanical studies demonstrated the inherent flaws of this approach. During dorsiflexion of the ankle, the wider anterior dome of the talus engages the ankle mortise, forcing the lateral malleolus outward. To accommodate this lateral plane rotation of the talus and the expansion of the ankle joint, the entire fibula must migrate proximally and rotate externally around its longitudinal axis.
If the PTFJ is fused, this essential rotary function is eliminated. In Ogden’s clinical series of four patients who underwent PTFJ fusion, three developed severe pain, discomfort, and secondary instability of the ankle joint due to the rigid constraint of the fibula. Two of these patients subsequently required resection of the proximal fibula, which successfully restored fibular rotation and relieved their ankle symptoms. Therefore, arthrodesis of the PTFJ is contraindicated in the management of isolated PTFJ instability.
SURGICAL TECHNIQUE: RESECTION OF THE PROXIMAL FIBULA
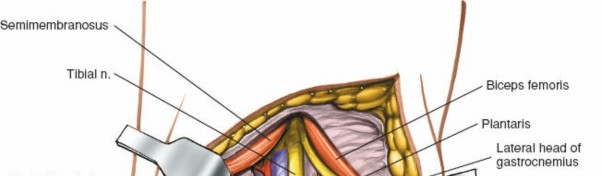
The primary goal of this procedure is to excise the unstable articulation while meticulously preserving the lateral supporting structures of the knee, specifically the insertion of the fibular collateral ligament (FCL) and the biceps femoris tendon.
Preoperative Preparation and Positioning
- Anesthesia: General or regional anesthesia.
- Positioning: The patient is placed supine on the operating table. A sandbag or bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral aspect of the knee into clear view. A sterile tourniquet is applied to the proximal thigh.
- Landmarks: The fibular head, fibular neck, lateral epicondyle of the femur, and the course of the common peroneal nerve are palpated and marked.
Surgical Approach and Dissection
- Incision: Make a longitudinal or slightly curved incision over the lateral aspect of the knee, centered over the fibular head and extending distally along the line of the fibula for approximately 7 to 10 cm.
- Superficial Dissection: Incise the subcutaneous tissue and deep fascia in line with the skin incision. Identify the interval between the biceps femoris tendon posteriorly and the iliotibial band anteriorly.
- Peroneal Nerve Identification: The common peroneal nerve must be identified early in the procedure. It is located posterior to the biceps femoris tendon and wraps around the fibular neck from posterior to anterior.
> 🚨 SURGICAL WARNING: The common peroneal nerve is highly susceptible to traction neuropraxia and direct transection. Dissection around the fibular neck must be strictly subperiosteal. Isolate the nerve with a vessel loop, but avoid excessive traction. - Ligamentous Preservation: It is paramount that the lateral supporting structures of the knee joint be reconstructed. This is accomplished by performing a careful osteotomy that preserves the proximal fibular styloid process. The FCL and the biceps femoris tendon insert onto this styloid process.
- Fibular Resection:
- Incise the periosteum of the fibula distal to the styloid process.
- Using a periosteal elevator, strip the soft tissues subperiosteally from the proximal fibula, working distally to proximally, carefully protecting the peroneal nerve.
- Perform an osteotomy of the fibula approximately 2 to 3 cm distal to the joint line, removing the articular portion of the fibular head while leaving the styloid process intact.
- Excise the remaining articular cartilage and capsule of the PTFJ.
- Reconstruction: The preserved fibular styloid process, with its attached FCL and biceps femoris, must now be securely anchored to the lateral metaphysis of the tibia to prevent posterolateral rotatory instability (PLRI) of the knee. Prepare a bleeding bone bed on the lateral tibia. Secure the styloid process to the tibia using heavy nonabsorbable transosseous sutures, suture anchors, or a cancellous screw with a spiked washer, depending on bone quality.
- Closure: Deflate the tourniquet and achieve meticulous hemostasis. Close the deep fascia, subcutaneous tissue, and skin in layers.
Postoperative Protocol
- Immobilization: A long leg, bent-knee cast (flexed to 30 degrees to relax the biceps femoris and FCL) or a locked hinged knee brace is applied immediately postoperatively.
- Weight-Bearing: The patient is kept non-weight-bearing for 6 weeks to allow for osseous integration of the styloid process to the tibia.
- Rehabilitation: After 6 weeks, the cast or brace is removed, and treatment proceeds as described for acute injuries of the lateral knee ligaments. Progressive range of motion (ROM) and strengthening exercises are initiated, focusing on quadriceps and hamstring rehabilitation.
CHRONIC AND UNREDUCED KNEE DISLOCATIONS
Acute dislocation of the knee is a true orthopedic emergency, primarily due to the high incidence of associated popliteal artery injuries and common peroneal nerve palsies. Because acute dislocations demand immediate reduction and vascular assessment, old, unreduced dislocations of the knee are exceedingly rare in modern orthopedic practice.
When encountered, chronic knee dislocations present a formidable surgical challenge. The joint capsule becomes severely contracted, the collateral and cruciate ligaments are scarred in non-anatomic positions, and the articular cartilage undergoes rapid degeneration due to lack of normal synovial fluid circulation and abnormal mechanical pressure.
Clinical Outcomes of Open Reduction
A useful, functional range of motion is seldom fully restored after the open reduction of a chronic knee dislocation. Even if the articular cartilage appears macroscopically normal at the time of surgery, dense intra-articular adhesions inevitably develop between the articular surfaces during the postoperative healing phase.
Despite these limitations, functional salvage is possible. Henshaw et al. reported a case of open reduction of a knee performed 24 weeks after the initial injury. At the 22-month postoperative follow-up, the patient had achieved a painless range of motion from 5 to 40 degrees and experienced no pain during weight-bearing. While the patient ambulated independently, running was precluded due to the restricted arc of motion. Nevertheless, the overall result was considered highly satisfactory given the severity of the chronic deformity.
Decision Making: Reduction vs. Arthroplasty vs. Arthrodesis
The surgical strategy for a chronic knee dislocation depends heavily on the condition of the articular cartilage, the extent of soft tissue contracture, and the patient's functional demands.
* Open Reduction: Indicated if the articular cartilage is preserved and the joint can be mobilized without catastrophic damage to the neurovascular bundle.
* Arthrodesis (Fusion): Indicated if the articular cartilage is irreversibly destroyed, or if open reduction alone would require such extensive soft tissue dissection that the viability of the limb is threatened.
* Total Knee Arthroplasty (TKA): Petrie et al. reported their experience with chronic knee dislocations treated with TKA. They noted profound technical difficulties in obtaining a well-balanced and well-aligned knee due to the complete absence of normal ligamentous tension. If arthroplasty is indicated, a staged approach is often preferred: first, perform an open reduction to resolve severe contractures and realign the mechanical axis; second, allow the soft tissues to heal and rehabilitate the extremity; finally, perform the TKA at a later date when the soft tissue envelope is more compliant.
Fig. 58-2: Seventeen-year-old girl with a history of neurofibromatosis and a 6-week history of acute knee dislocation and inability to walk. (A and B) Anteroposterior and lateral radiographs of the knee showing posteromedial dislocation of the tibia with medial dislocation of the patella. (C and D) Anteroposterior and lateral radiographs at the time of open reduction and internal fixation utilizing a smooth Steinmann pin driven through the quadriceps mechanism, femur, and tibia to maintain temporary alignment. (E and F) Postoperative anteroposterior and lateral radiographs demonstrating mild persistent lateral subluxation but an overall good reduction of the knee and patellar dislocation.
SURGICAL TECHNIQUE: OPEN REDUCTION OF CHRONIC KNEE DISLOCATION
Preoperative Planning
Advanced imaging, including MRI and CT angiography, is mandatory to assess the exact position of the popliteal vessels, which are often encased in dense scar tissue and tethered to the posterior capsule.
Surgical Approach and Exposure
- Incision: Utilize an extensile anteromedial approach to expose the knee joint. If the patella has been chronically displaced either medially or laterally (as seen in Fig. 58-2), the skin incision must be modified to correspond with the normal anatomical location of the medial borders of the quadriceps tendon, patella, and patellar tendon to allow for proper realignment of the extensor mechanism.
- Deep Dissection: Perform a medial parapatellar arthrotomy. Evert or laterally subluxate the patella to expose the tibiofemoral articulation.
- Soft Tissue Release: In a chronic dislocation, the joint space will be obliterated by dense fibrous tissue. Meticulously excise enough fibrous tissue from the intercondylar notch and the medial and lateral gutters to expose the articular surfaces completely.
- Posterior Capsular Release: If the tibia is chronically subluxated or dislocated (often posteriorly or posteromedially), the posterior capsule will be severely contracted.
> Clinical Pearl: Dissect the soft structures subperiosteally from the posterior aspect of the femur and tibia. This subperiosteal plane is crucial to protect the popliteal artery and vein, which lie immediately posterior to the capsule.
Joint Reduction and Fixation
- Assessment of Cartilage: Once the joint is mobilized, inspect the articular cartilage.
- If the cartilage appears undamaged or salvageable: Proceed with reduction of the dislocation. Gentle traction and manipulation are required. Avoid excessive leverage that could cause iatrogenic fractures of the osteopenic bone.
- If the cartilage has been irreversibly damaged: Abandon open reduction and proceed directly with an arthrodesis of the knee, utilizing an intramedullary nail or dual-plate construct.
- Temporary Fixation: Due to the complete incompetence of the cruciate and collateral ligaments, the reduced joint will be grossly unstable. Temporary transarticular fixation is often required. As demonstrated in Figure 58-2, a heavy, smooth Steinmann pin can be driven antegrade through the quadriceps mechanism and distal femur, across the joint line, and into the proximal tibia to hold the reduction.
- Extensor Mechanism Realignment: If the patella was chronically dislocated, a lateral retinacular release and medial reefing (or medial patellofemoral ligament reconstruction) may be necessary to centralize the extensor mechanism.
Staged Arthroplasty Considerations
If the ultimate goal is a total knee arthroplasty, it is often safer and more effective to use the open reduction as a preliminary, soft-tissue balancing procedure. Reduce the joint, pin it temporarily if necessary, and close the wound. Proceed with rehabilitation to allow the severe capsular contractures to resolve and the skin envelope to heal. The definitive arthroplasty can then be performed in a delayed fashion under more favorable anatomical conditions.
Postoperative Management
- For Open Reduction (Staged for Arthroplasty): Immobilize the extremity in a long leg cast or a locked hinged brace. The transarticular Steinmann pin is typically removed at 4 to 6 weeks. Once the pin is removed, gentle, protected range of motion is initiated to stretch the soft tissues in preparation for future arthroplasty.
-
For Arthrodesis: If an arthrodesis was performed at the time of the open reduction, the patient is kept strictly non-weight-bearing or touch-down weight-bearing in a cylinder cast or brace until radiographic evidence of bony consolidation is observed, typically at 10 to 12 weeks.
You Might Also Like