Extraarticular Ankylosis of the Knee: Comprehensive Surgical Management

Key Takeaway
Extraarticular ankylosis of the knee presents a complex reconstructive challenge, often resulting from severe trauma, prolonged immobilization, or extensive soft-tissue scarring. Unlike intraarticular arthrofibrosis, the joint space may remain preserved. Management requires meticulous preoperative planning and precise surgical execution. Soft-tissue releases, including the Thompson, Judet, and mini-invasive quadricepsplasty techniques, aim to restore functional range of motion. This guide details the pathoanatomy, biomechanics, step-by-step surgical approaches, and rigorous postoperative rehabilitation protocols essential for optimizing patient outcomes.
Pathoanatomy and Biomechanics of Extraarticular Ankylosis
Ankylosis of the knee, whether intraarticular or extraarticular, is a profoundly debilitating condition that severely compromises lower extremity biomechanics, gait kinematics, and overall patient quality of life. The deformity may present with the knee locked in complete extension, in isolated flexion, or in a complex multiplanar deformity characterized by flexion, external rotation, and valgus malalignment.
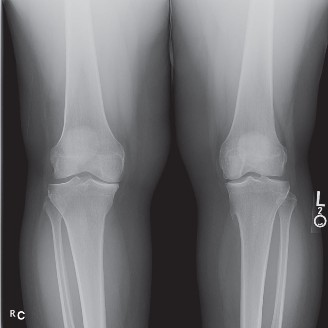
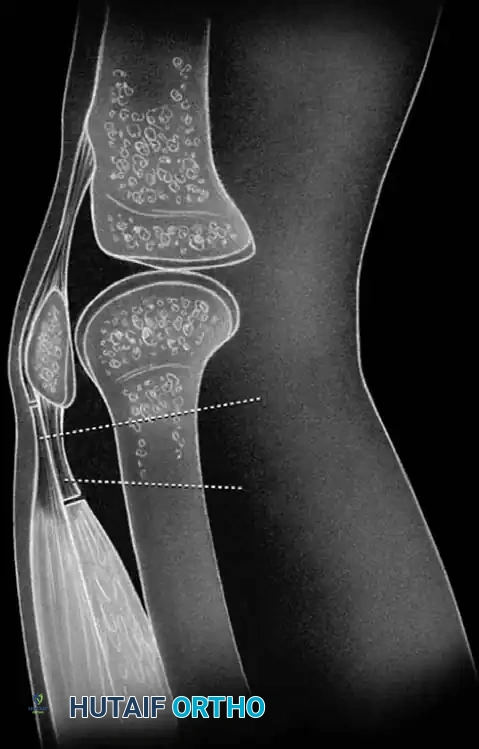
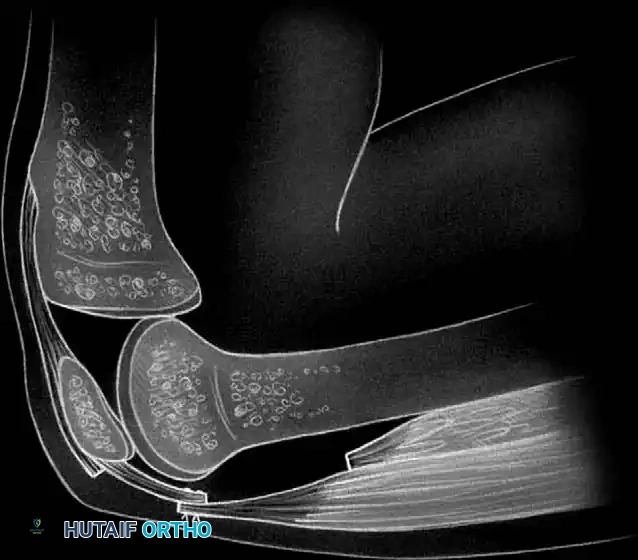
When the ankylosis is strictly extraarticular, the intrinsic articular cartilage and meniscal structures may remain relatively pristine. Radiographic evaluation often reveals an apparently normal joint space, distinguishing this pathology from end-stage osteoarthritis or inflammatory arthropathies. The primary mechanical block to motion arises from the profound contracture, fibrosis, and tethering of the periarticular soft-tissue envelope.
When extraarticular ankylosis and contracture limit mobility to a non-functional arc, a comprehensive soft-tissue release procedure—such as a quadricepsplasty or radical capsulotomy—is generally indicated.
💡 Clinical Pearl: Soft-Tissue Envelope Optimization
Adequate soft-tissue augmentation is paramount to the success of release procedures performed for posttraumatic ankylosis. Ulusal et al. demonstrated that combining free-flap coverage with release procedures (typically quadricepsplasty and capsulotomy) significantly improves outcomes in patients with posttraumatic knee joint stiffness following open fractures.
In patients ranging from 11 to 38 years of age, the utilization of transferred free flaps provided a pliable, well-vascularized contour match. The integration of free tissue transfers for soft-tissue augmentation minimizes catastrophic wound complications—such as wound edge necrosis, dehiscence, and deep infection. Crucially, a robust soft-tissue envelope permits the early initiation of aggressive postoperative continuous passive motion (CPM) and physical therapy, which are the ultimate determinants of functional success.
Extraarticular Ankylosis in Extension
Extraarticular ankylosis in extension is most frequently encountered following high-energy fractures of the femoral shaft or extensive soft-tissue avulsion injuries to the anterior aspect of the thigh. The resulting hematoma, subsequent organization, and profound scarring or fibrosis of all or part of the quadriceps mechanism tether the extensor apparatus, obliterating normal excursion.
Nicoll classically emphasized that this rigid extension deformity is multifactorial and can be driven by one or more of the following pathoanatomical changes:
1. Vastus Intermedius Fibrosis: Profound scarring of the vastus intermedius muscle, which tethers the rectus femoris directly to the anterior cortex of the femur, obliterating the suprapatellar pouch.
2. Patellofemoral Adhesions: Dense, fibrous adhesions binding the deep surface of the patella to the femoral trochlea and condyles.
3. Retinacular Contracture: Fibrosis and structural shortening of the lateral and medial expansions of the vasti, rigidly adhering them to the femoral condyles.
4. Rectus Femoris Shortening: Actual myostatic contracture and absolute shortening of the rectus femoris muscle belly itself.
To systematically address these deforming forces, several surgical techniques have been developed, ranging from the traditional open Thompson quadricepsplasty to the sequential Judet release, and more recently, mini-invasive endoscopic techniques.
The Thompson Quadricepsplasty
The Thompson quadricepsplasty is a powerful, albeit extensive, open procedure designed to systematically liberate the extensor mechanism. Its ultimate functional success is heavily dependent on three critical factors:
1. The degree to which the rectus femoris muscle has escaped the initial traumatic injury.
2. The surgeon's ability to meticulously isolate the rectus femoris from the densely scarred components of the surrounding quadriceps mechanism.
3. The patient's capacity to actively rehabilitate and hypertrophy the isolated muscle postoperatively.
🔪 Surgical Technique: Thompson Quadricepsplasty
- Incision and Exposure: Utilize an electrocoagulation unit throughout the operation to maintain meticulous hemostasis. Make an anterior longitudinal incision through the skin and superficial fascia, extending from the proximal third of the thigh down to the distal pole of the patella. The exact trajectory should incorporate or bypass previous traumatic scars to optimize skin viability.
- Fascial Release: Divide the deep fascia along both the medial and lateral borders of the rectus femoris muscle, extending from the proximal apex of the incision down to the patella. Carefully develop the planes to separate the rectus femoris from the vastus medialis and vastus lateralis.
- Capsular and Retinacular Release: Divide the anterior portion of the knee capsule. This must include the lateral and medial expansions of the vasti on both sides of the patella. The release must be carried far enough posteriorly and distally to completely overcome their fibrotic contracture.
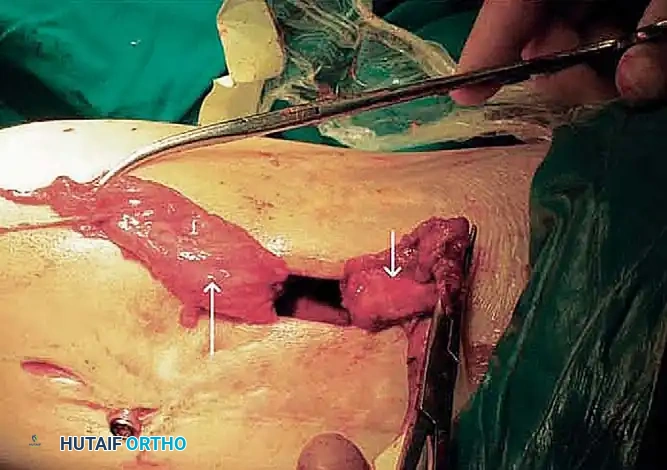
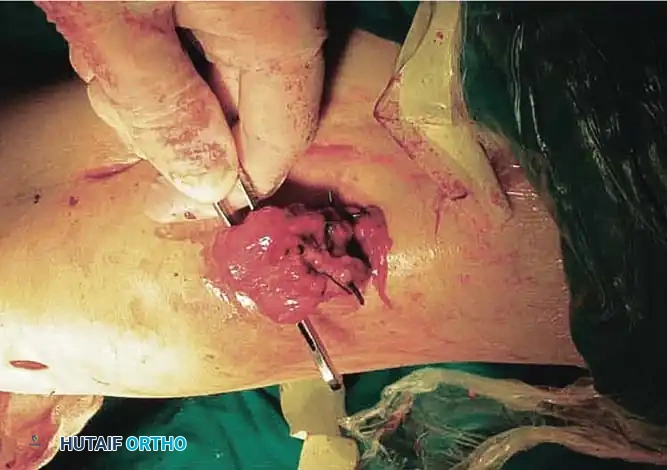
- Excision of the Vastus Intermedius: This is a critical step. The vastus intermedius is typically found as a dense, scarred fibrotic band binding the posterior surface of the rectus femoris and the patella directly to the anterior femur. Excise this fibrotic mass completely. Surgical Warning: Leave a thin fibrous or periosteal covering on the anterior surface of the femur to prevent subsequent bony overgrowth or massive hematoma adherence.
- Tendon Reconstruction (If Necessary): If the tendon of the rectus femoris was destroyed by the initial injury, a neo-tendon must be created by making longitudinal incisions through the organized scar tissue in the distal third of the thigh.
- Joint Mobilization: At this juncture, slowly and gently flex the knee to 110 degrees. This maneuver will audibly and palpably release any remaining intraarticular adhesions within the gutters and intercondylar notch.
- Muscle Interposition and Closure: If the vastus medialis and lateralis are severely scarred, interpose viable subcutaneous tissue and fat between them and the newly isolated rectus femoris to prevent readherence. If these muscles remain relatively healthy, suture them to the rectus femoris as far distally as the distal third of the thigh. Deflate the tourniquet, achieve absolute hemostasis, insert a deep suction drain, and close the wound in layers.
🚨 Surgical Pitfall: Over-Manipulation
Never forcefully manipulate the knee past 110 degrees if extreme resistance is met, as this can result in an iatrogenic patellar tendon avulsion, transverse patellar fracture, or supracondylar femur fracture. If flexion is not achieved, re-evaluate the proximal releases.
Postoperative Rehabilitation Protocol
The extremity is immobilized in a splint at approximately 50 degrees less than the maximal flexion obtained intraoperatively. This position is maintained for 48 to 72 hours to allow initial hemostasis and reduce dead space hematoma.
Following this brief immobilization, the extremity is placed in a Continuous Passive Motion (CPM) machine. Range of motion is aggressively pursued until 90 degrees of passive flexion is achieved. Passive, active-assisted, and active exercises for both the quadriceps and hamstrings are initiated immediately; these are of critical importance to the success of the procedure.
The knee should be maintained in full extension during the night using a rigid splint to prevent secondary flexion contractures, while daytime hours are dedicated to active mobilization. If 90 degrees of flexion is not obtained by 3 months postoperatively, a gentle manipulation under anesthesia (MUA) may be required. Patients must be counseled preoperatively to expect a very slow return of active quadriceps extension, often enduring severe quadriceps weakness for many months. In skeletally immature patients, some of the intraoperative improvement in flexion may be lost as longitudinal bone growth outpaces soft-tissue stretch.
The Judet Sequential Quadricepsplasty
As an alternative designed to minimize collateral damage to the quadriceps mechanism and preserve extensor power, Judet described a proximal-based, staged, sequential release of the intrinsic and extrinsic structures limiting knee flexion.
The Judet technique is executed in three distinct phases, progressing only if the desired flexion is not achieved:
1. Phase 1: Release of the medial and lateral retinacula, combined with the release of adhesions in the suprapatellar gutter and between the patella and femoral condyles. This is typically performed through a longitudinal or medial parapatellar incision.
2. Phase 2: Release of the vastus intermedius through a long posterolateral incision extending from the superior pole of the patella to the greater trochanter. The muscle is elevated off the linea aspera and anterior femur.
3. Phase 3: Detachment of the rectus femoris from its proximal insertion at the anterior inferior iliac spine (AIIS) through a proximal anterolateral extension of the posterolateral incision.
The final phase is utilized only if flexion remains unacceptably limited after manipulation subsequent to the first two phases. Literature reports indicate excellent or good results in approximately 81% of patients, with fair results in 19%, noting superior preservation of active extension compared to the Thompson technique.
Mini-Invasive Quadricepsplasty
Endoscopically and arthroscopically assisted percutaneous techniques have revolutionized the approach to extraarticular ankylosis, significantly reducing the morbidity associated with massive open exposures. Wang, Zhao, and He described a highly effective extraarticular "mini-invasive" quadricepsplasty followed by intraarticular arthroscopic lysis of adhesions.
This procedure is meticulously executed in five stages. The range of flexion is measured after each stage of release, and the procedure is immediately terminated when the desired degree of flexion (ideally 120 degrees) is obtained. This step-wise approach prevents unnecessary destabilization of the extensor mechanism.
🔪 Surgical Technique: Mini-Invasive 5-Stage Release
STAGE 1: Lateral Retinacular Release
* Utilizing an inside-out technique, create a percutaneous parapatellar lateral arthrotomy. Incise the lateral retinaculum from the patella along its lateral border, extending from the superolateral corner of the patella down to the lateral aspect of its lower pole.
* To fully restore the lateral recess, free the lateral retinaculum from the lateral femoral condyle, and meticulously release the vastus lateralis tendon and the iliotibial band from their scarred attachments to the distal third of the femur.
STAGE 2: Anterior Interval and Suprapatellar Mobilization
* Mobilize the suprapatellar pouch, the patellofemoral compartment, and the anterior interval by sharply dividing the dense adhesions within these spaces. The anterior interval—defined as the region posterior to the infrapatellar fat pad and anterior to the anterosuperior aspect of the tibial plateau—must be completely liberated to allow patellar descent during flexion.
- Separate the tendinous tissue of the vastus intermedius from that of the rectus femoris and the anterior surface of the femur, recreating the gliding planes of the extensor apparatus.
STAGE 3: Medial Retinacular Release
* With a percutaneous inside-out technique, release the medial patellar retinaculum through the suprapatellar pouch, patellofemoral compartment, and anterior interval that were reestablished in the second stage.
* Surgical Warning: Take extreme care to delineate the medial arthrotomy margin, which starts from the medial epicondyle of the femur and slants laterally to the tibial tubercle. This precise trajectory avoids the catastrophic detachment of the vastus medialis obliquus (VMO) from its dynamic insertion at the superomedial corner of the patella.
* Free the medial retinaculum from the medial femoral condyle, and release the vastus medialis from the distal third of the femur to fully restore the medial recess.
STAGE 4: Vastus Intermedius Transection
* If flexion remains inadequate, proceed to transect the previously mobilized vastus intermedius at a level near its musculotendinous junction. This eliminates the primary tethering force binding the extensor mechanism to the femoral shaft.
STAGE 5: Quadriceps Tendon Lengthening
* The fifth and final stage consists of a formal lengthening of the quadriceps tendon.
* Transect the rectus femoris at a more distal level than the vastus intermedius, adjacent to its patellar insertion.
* Deliver the free tendinous ends of the vastus intermedius and rectus femoris through the percutaneous wound.
- Gently manipulate the knee in flexion repeatedly until maximal flexion is achieved. The proximal portion of the vastus intermedius tendon and the distal portion of the rectus femoris tendon are then sutured together with the knee held in 90 degrees of flexion to set the new resting length of the extensor mechanism.
This mini-invasive approach represents a highly reasonable alternative to open quadricepsplasty, producing a superior cosmetic result, minimizing wound necrosis, and allowing for immediate, aggressive postoperative rehabilitation.
Salvage Procedures: Patellectomy
Historically, instead of patellaplasty or complex soft-tissue releases, authors such as West and Soto-Hall recommended total patellectomy. In contemporary orthopedic practice, patellectomy is rarely utilized and is strictly reserved as a salvage procedure for end-stage, recalcitrant arthrofibrosis with severe patellofemoral osteoarthritis. The procedure is associated with poor functional results, a 30% reduction in extensor mechanism mechanical advantage, and exceedingly difficult postoperative rehabilitation.
🔪 Surgical Technique: Salvage Patellectomy
- Through a transverse incision at the level of the inferior third of the patella, incise the quadriceps expansion in line with the incision. This ensures that the final suture line in the tendon will lie at the level of the infrapatellar fat pad rather than directly over the abrasive femoral condyles.
- By careful, sharp dissection, enucleate and excise the patella from its tendinous envelope.
- Because the removal of the patella produces a relative lengthening of the quadriceps mechanism (loss of the fulcrum effect), proper resting tension must be restored. Achieve this by overlapping the cut edges of the tendon by approximately 1.5 cm and suturing them together with heavy, non-absorbable sutures (e.g., #5 Krackow stitch). According to Soto-Hall, this imbrication allows complete active extension to be regained more rapidly after surgery.
- If the quadriceps mechanism is in a valgus position and lateral instability of the patella was demonstrated prior to surgery, extend the medial arm of the incision proximally. Remove or plicate a V-shaped section of the medial capsule to restore the balance between the medial and lateral dynamic stabilizers, effectively transferring part of the insertion of the vastus medialis distally.
Extraarticular Ankylosis in Flexion
Flexion contracture of the knee is significantly more common than extension contracture. It is frequently seen in patients subjected to prolonged wheelchair use, severe hamstring spasticity, or chronic inflammatory arthropathies.
The pathoanatomy of flexion ankylosis is complex. It is often complicated by posterior subluxation and external rotation of the tibia on the femur. This triplanar deformity occurs because the hamstring muscles exert a constant posterior translational force on the tibia, while the biceps femoris muscle and the iliotibial band act as powerful external rotators. Consequently, all of the neurovascular and soft-tissue structures within the popliteal space become severely contracted.
Management Strategies
Flexion contractures can usually be at least partially corrected through conservative, non-operative modalities. The amount of correction possible is directly proportional to the severity and chronicity of the deformity.
- Conservative Management: Modalities include traction with balanced suspension, Buck extension, and the application of static or dynamic progressive splints, serial casts, or hinged braces designed to extend the knee gradually. These measures exploit the viscoelastic creep of the posterior soft tissues.
- Surgical Management: If conservative measures fail, surgical intervention is required. This typically involves a radical posterior capsulotomy, fractional lengthening or Z-plasty of the hamstring tendons (biceps femoris, semimembranosus, semitendinosus), and release of the iliotibial band.
🚨 Surgical Warning: Neurovascular Compromise
During the surgical correction of severe flexion ankylosis, the peroneal and tibial nerves, as well as the popliteal artery, are at extreme risk of traction injury. Correction must be gradual. If the knee is acutely extended intraoperatively, the surgeon must palpate distal pulses and monitor for signs of nerve ischemia. Prophylactic peroneal nerve decompression at the fibular head is often warranted in contractures exceeding 45 degrees.
In conclusion, the management of extraarticular knee ankylosis demands a profound understanding of periarticular anatomy and biomechanics. Whether employing the extensive Thompson release, the sequential Judet approach, or modern mini-invasive techniques, the surgeon must balance the need for maximal soft-tissue release with the preservation of extensor mechanism continuity. Meticulous surgical execution, combined with an unwavering commitment to postoperative rehabilitation, remains
You Might Also Like