Recurrent Patellar Instability: Clinical Evaluation & Surgical Management
Key Takeaway
Recurrent patellar instability presents a complex biomechanical challenge requiring meticulous clinical and radiographic evaluation. Diagnosis relies on identifying malalignment, trochlear dysplasia, and ligamentous laxity. Surgical management is dictated by specific anatomic deficits, utilizing procedures such as Medial Patellofemoral Ligament (MPFL) reconstruction or Tibial Tubercle Osteotomy (TTO) to restore patellofemoral kinematics. This guide details the diagnostic framework, imaging indices, and step-by-step operative interventions for optimal patient outcomes.
Introduction to Patellofemoral Instability
Patellofemoral instability is a multifactorial orthopedic condition characterized by recurrent subluxation or dislocation of the patella from the femoral trochlea. The stability of the patellofemoral joint relies on a delicate interplay between static restraints (osseous architecture of the trochlea, medial patellofemoral ligament [MPFL]) and dynamic stabilizers (quadriceps musculature, specifically the vastus medialis obliquus [VMO]). Disruption of this biomechanical harmony—whether through acute trauma, chronic ligamentous attenuation, or underlying anatomic dysplasia—results in recurrent instability, progressive cartilage degradation, and profound functional impairment.
Successful management demands a rigorous, evidence-based approach to clinical evaluation, precise radiographic quantification of anatomic risk factors, and targeted surgical intervention.
Clinical Features and Patient History
In patients presenting with recurrent dislocation or subluxation of the patella, an accurate and exhaustive history remains one of the most critical diagnostic tools. Patellar problems can frequently mimic various "internal derangements" of the knee, such as meniscal tears or anterior cruciate ligament (ACL) injuries.
An accurate history detailing the exact mechanism of injury, as well as the character and localization of pain, is paramount. Patients suffering from recurrent dislocation frequently report diffuse, poorly localized pain around the anterior aspect of the knee. This discomfort is classically exacerbated by activities that increase patellofemoral joint reaction forces, such as ascending or descending stairs, squatting, or walking on inclined surfaces.
The pain is typically located anteriorly and is often described as a chronic, dull ache punctuated by intermittent episodes of sharp, severe pain. A pervasive feeling of insecurity in the knee is a hallmark symptom; patients frequently describe the knee as "giving way," "buckling," or "going out." Furthermore, mechanical symptoms such as patellar crepitation and recurrent effusions are common clinical features that warrant thorough investigation.
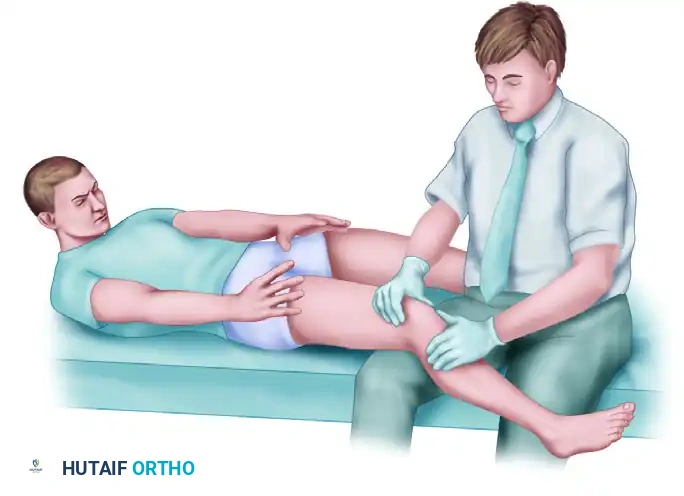
Comprehensive Physical Examination
The physical examination of the patellofemoral joint must be systematic, evaluating the patient in standing, seated, and supine positions to capture dynamic and static abnormalities.
Standing Examination
The examination begins with the patient standing to assess global lower extremity alignment. The clinician must observe for multi-planar malalignment, including:
* Femoral Anteversion: Often presenting as "squinting patellae."
* Genu Valgum: Increases the lateral vector force on the patella.
* External Tibial Torsion: Contributes to an increased Q-angle.
* Pes Planus: Pronation of the foot leads to obligatory internal tibial rotation, exacerbating patellofemoral maltracking.
Seated Examination
With the patient seated and the knees flexed to 90 degrees, the clinician observes patellar height and tracking. A lateral or superior position of the patella (patella alta) may be immediately visible. As the patient actively extends the knee, the examiner should watch for the "J-sign"—a sudden lateral deviation of the patella as it exits the trochlear groove near full extension, indicative of maltracking and MPFL incompetence.
Supine Examination
In the supine position, the knee is evaluated for effusions and palpable abnormalities. Patellofemoral crepitus may be palpable during active and passive range of motion.
The Q-Angle:
The Quadriceps (Q) angle is a fundamental measurement of the lateralizing vector acting on the patella. It is formed by the intersection of two lines: one drawn from the anterior superior iliac spine (ASIS) to the center of the patella, and a second drawn from the center of the patella to the tibial tuberosity. Physical findings often include factors that contribute to an abnormally increased Q-angle (normal is typically <15 degrees in males and <18 degrees in females).
Palpation and Apprehension:
Tenderness along the medial or lateral facets of the patella may be noted with direct palpation. This is best achieved by manually subluxing the patella medially or laterally and rotating it to expose the articular surfaces. Such tenderness strongly indicates underlying chondral pathology or osteochondral lesions.
The Patellar Apprehension Test is highly sensitive for prior dislocation. With the knee relaxed in 20 to 30 degrees of flexion (to engage the patella in the trochlea), the examiner applies a laterally directed force to the medial border of the patella. A positive test occurs when the patient experiences a sensation of impending dislocation, often accompanied by reflex quadriceps contraction to halt the lateral translation.
Assessment of Ligamentous Laxity and Muscle Atrophy
Thigh circumferences, measured at a standardized distance proximal to the superior pole of the patella, frequently reveal quadriceps (specifically VMO) atrophy on the involved side.
After careful examination of the injured knee, the contralateral knee and other joints must be assessed for generalized hyperlaxity (Beighton criteria). Indicators of generalized ligamentous laxity include:
* Hyperextension of the knees or elbows past 10 degrees.
* Ability to passively touch the thumb to the volar aspect of the forearm.
* Hyperextension of the metacarpophalangeal (MCP) joint of the index finger past 90 degrees.
* Multidirectional laxity of the shoulder joint.
Clinical Pearl: Patients with generalized ligamentous laxity frequently exhibit fewer acute osteochondral shear lesions following a dislocation event compared to patients with normal collagen tension, as the joint subluxes with less applied force and lower energy.
Finally, the thigh-foot angle is measured with the patient prone and the knee flexed to 90 degrees. An angle exceeding 30 degrees indicates a significant rotational deformity of the lower extremity (excessive external tibial torsion), which must be factored into surgical decision-making.
Radiographic Measurements and Imaging Analysis
Accurate radiographic quantification of patellofemoral anatomy is mandatory. A standard series includes weight-bearing anteroposterior (AP), true lateral (at 30 degrees of flexion), and axial (Merchant or sunrise) views. Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) is essential for advanced surgical planning.
Assessment of Patellar Height
Patella alta (an abnormally high-riding patella) delays the engagement of the patella into the stabilizing trochlear groove during early flexion, predisposing the joint to instability.
Blumensaat Line:
Evaluated on a true lateral radiograph with the knee flexed to 30 degrees. A line is drawn through the roof of the intercondylar notch (Blumensaat's line) and extended anteriorly. In a normal knee, this line should closely approximate the inferior pole of the patella. If the patella is significantly proximal to this line, patella alta is diagnosed.

Standardized Indices for Patellar Height:
* Insall-Salvati Index: Measured on a lateral radiograph. It is the ratio of the patellar tendon length (LT) to the greatest diagonal length of the patella (LP). A normal ratio is 1.0. Patella alta is defined as a ratio ≥ 1.2, and patella infera as ≤ 0.8.
* Caton-Deschamps Index: The ratio between the distance from the inferior articular margin of the patella to the anterior corner of the superior tibial epiphysis (AT) and the length of the patellar articular surface (AP). Normal is 0.6 to 1.3. Patella alta is > 1.3.
* Blackburne-Peel Ratio: The perpendicular distance from the inferior articular pole of the patella to the tibial plateau articular surface, divided by the length of the patellar articular surface. Normal ranges from 0.54 to 1.06.
Assessment of Trochlear Dysplasia and Alignment
Trochlear dysplasia flattens the bony constraint of the anterior femur, removing the primary static stabilizer against lateral patellar translation.
- Trochlear Depth (Dejour): Measured on a true lateral radiograph 1 cm distal to the superior margin of the trochlear groove. A normal depth is ≥ 5 mm. Shallower measurements indicate dysplasia.
- Crossing Sign: On a lateral radiograph, if the anterior cortical outline of the femoral condyles intersects the outline of the trochlear floor, a dysplastic, flattened sulcus is present.
- Trochlear Bump: If the trochlear floor line extends anterior to the anterior femoral cortex, it indicates a supratrochlear spur or bump, highly correlative with severe dysplasia.
- Patellar Tilt (CT Scan): Measured on an axial CT slice at 20 degrees of knee flexion. It is the angle formed by the intersection of a line tangent to the posterior femoral condyles and the major transverse axis of the patella. A normal angle is < 20 degrees. Angles > 20 degrees indicate significant dysplasia and lateral tightness.
- TT-TG Distance (CT or MRI): The Tibial Tubercle-Trochlear Groove distance is the gold standard for quantifying lateralization of the extensor mechanism. Two parallel lines are drawn perpendicular to the posterior bicondylar axis: one bisecting the deepest point of the trochlear groove, and the other bisecting the center of the tibial tubercle.
- Normal: < 15 mm.
- Borderline: 15 - 20 mm.
- Pathologic Malalignment: > 20 mm (Strong indication for tibial tubercle osteotomy).
Surgical Indications
Surgical intervention is indicated in patients who have failed a comprehensive non-operative rehabilitation program (focused on VMO strengthening and core/gluteal stabilization) and continue to experience recurrent instability.
Absolute indications for early surgery include:
1. Acute dislocation associated with a displaced osteochondral fracture (requiring excision or fixation).
2. Major disruption of the MPFL with a high-demand athletic profile.
3. Recurrent instability with progressive chondral damage.
Surgical decision-making is an "a la carte" process dictated by the patient's specific anatomic deficits identified during the radiographic evaluation.
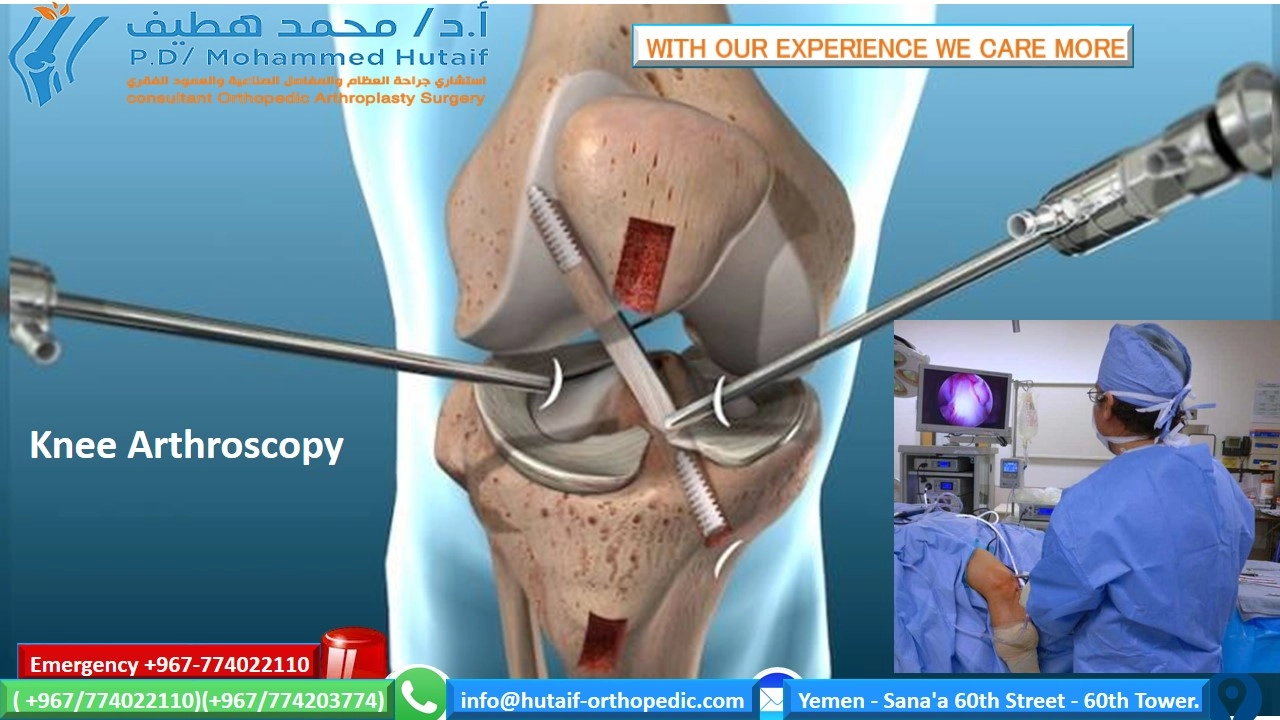
Operative Techniques
1. Medial Patellofemoral Ligament (MPFL) Reconstruction
The MPFL is the primary soft-tissue restraint to lateral patellar translation from 0 to 30 degrees of flexion. Reconstruction is the workhorse procedure for recurrent instability without severe bony malalignment.
Positioning and Preparation:
The patient is positioned supine. A tourniquet is applied to the proximal thigh. Diagnostic arthroscopy is routinely performed first to evaluate and treat any intra-articular chondral lesions and to assess patellar tracking dynamically.
Graft Selection and Preparation:
Autograft (gracilis or semitendinosus) or allograft may be utilized. The graft is whipstitched at both ends. If a double-bundle technique is chosen, the graft is folded to create a loop.
Patellar Fixation:
A 2-cm longitudinal incision is made over the medial border of the patella. The medial capsule is exposed. Two transverse sockets (or a single longitudinal trough, depending on the technique) are drilled into the upper half of the medial patellar margin, taking care not to breach the anterior cortex or articular surface. The graft ends are secured into the patella using suture anchors or interference screws.
Femoral Attachment (Schöttle's Point):
Accurate femoral tunnel placement is the most critical step to ensure graft isometry. Schöttle's point is identified fluoroscopically on a true lateral radiograph:
1. 1 mm anterior to the posterior cortical line of the femur.
2. 2.5 mm distal to the posterior origin of the medial femoral condyle.
3. Proximal to the level of the posterior point of Blumensaat's line.
A guide pin is placed at this isometric point, and a tunnel is reamed. The looped end of the graft is passed between the capsule and the vastus medialis fascia and shuttled into the femoral tunnel.
Tensioning and Fixation:
Surgical Warning: Over-tensioning the MPFL graft is a catastrophic error that leads to medial patellofemoral overload, severe pain, iatrogenic medial subluxation, and rapid cartilage wear.
The graft must be tensioned with the knee at 30 degrees of flexion. The patella should be able to be manually translated laterally by 1 to 2 quadrants (approximately 10 mm). Once appropriate tension is confirmed, the graft is secured in the femur with an interference screw.
2. Tibial Tubercle Osteotomy (TTO)
A TTO is indicated when there is significant lateralization of the extensor mechanism (TT-TG > 20 mm) or severe patella alta (Caton-Deschamps > 1.3). The Fulkerson anteromedialization osteotomy is commonly employed to simultaneously medialize and anteriorize the tubercle, correcting the Q-angle and unloading the distal/lateral patellar facets.
Surgical Approach:
A longitudinal incision is made just lateral to the tibial crest. The anterior compartment musculature is elevated off the lateral aspect of the tibia.
Osteotomy:
Using an oscillating saw, an osteotomy is initiated proximal to the tibial tubercle and directed distally. For an anteromedialization (Fulkerson), the cut is made at an oblique angle (typically 45 to 60 degrees to the coronal plane) from anteromedial to posterolateral. The distal periosteal hinge is preserved to prevent proximal migration.
Translation and Fixation:
The osteotomized bone block is translated medially (to reduce the TT-TG to approximately 10-12 mm) and anteriorly. It is temporarily pinned with Kirschner wires. Patellar tracking is assessed. Once optimal tracking is achieved, the osteotomy is rigidly fixed with two or three 4.5 mm cortical lag screws placed from anterior to posterior.
Postoperative Protocol and Rehabilitation
Rehabilitation must balance the protection of the surgical repair with the prevention of arthrofibrosis.
- Phase I (Weeks 0-2): The knee is locked in full extension in a hinged brace for weight-bearing. Passive range of motion (ROM) is initiated from 0 to 90 degrees. Quadriceps activation (isometric sets) is emphasized immediately.
- Phase II (Weeks 2-6): Weight-bearing is progressed to full as tolerated with the brace locked in extension. ROM is gradually advanced to full flexion. The brace is unlocked for ambulation once straight-leg raises can be performed without an extensor lag.
- Phase III (Weeks 6-12): The brace is discontinued. Focus shifts to closed-kinetic-chain strengthening (leg presses, mini-squats), core stability, and proprioceptive training.
- Phase IV (Months 3-6): Progression to sport-specific activities, plyometrics, and agility drills. Return to play is typically permitted at 5 to 6 months postoperatively, contingent upon achieving >90% limb symmetry index on functional testing.
Complications and Pitfalls
- Recurrent Instability: Often due to failure to recognize and address underlying bony malalignment (e.g., performing an isolated MPFL reconstruction in a patient with a TT-TG of 25 mm).
- Stiffness and Arthrofibrosis: The most common complication following MPFL reconstruction, usually secondary to graft over-tensioning or non-isometric femoral tunnel placement.
- Patellar Fracture: Can occur due to aggressive drilling of the patellar sockets or placement of tunnels too close to the articular surface.
- Tibial Tubercle Fracture: A risk following TTO if the distal hinge is violated or if the patient falls before radiographic union is achieved. Strict adherence to weight-bearing precautions is mandatory.
📚 Medical References
- Patellar instability after total knee arthroplasty, Clin Orthop Relat Res 237:184, 1988.
- Haas SB, Tribus CB, Insall JN, et al: The signifi cance of calf thrombi after total knee arthroplasty, J Bone Joint Surg 74B:799, 1992.
- Haddad FS, Masri BA, Campbell D, et al: The PROSTALAC functional spacer in two-stage revision for infected knee replacements, J Bone Joint Surg 82B:807, 2000.
- Hanssen AD, Rand JA: Evaluation and treatment of infection at the site of a total hip or knee arthroplasty, Instr Course Lect 48:111, 1999.
- Hanssen AD, Rand JA, Osmon DR: Treatment of the infected total knee arthroplasty with insertion of another prosthesis: the effect of antibiotic-impregnated bone cement, Clin Orthop Relat Res 309:44, 1994.
- Hanssen AD, Trousdale RT, Osmon DR: Patient outcome with reinfection following reimplantation for the infected total knee arthroplasty, Clin Orthop Relat Res 321:55, 1995.
- Healy WL, Siliski JM, Incavo SJ: Operative treatment of distal femoral fractures proximal to total knee replacements, J Bone Joint Surg 75A:27, 1993.
- Henry SL: Management of supracondylar fractures proximal to total knee arthroplasty with the GSH supracondylar nail, Contemp Orthop 31:231, 1995.
- Hofmann AA, Goldberg T, Tanner AM, et al: Treatment of infected total knee arthroplasty using an articulating spacer: 2to 12-year experience, Clin Orthop Relat Res 430:125, 2005.
- Hofmann AA, Tkach TK, Evanich CJ, et al: Patellar component medialization in total knee arthroplasty, J Arthroplasty 12:155, 1997.
- Hozack WJ, Goll SR, Lotke PA, et al: The treatment of
You Might Also Like