Guyon's Canal Syndrome: Volar Approach for Ulnar Nerve Decompression & Exploration
Key Takeaway
Guyon's Canal Syndrome (GCS) is ulnar nerve compression at the wrist, distinct from cubital tunnel syndrome, causing sensory/motor deficits. It stems from trauma, cysts, or repetitive microtrauma. Diagnosis involves electrodiagnostic studies and imaging. The definitive treatment for GCS unresponsive to conservative care is the volar surgical approach for direct nerve decompression and exploration within Guyon's canal.
Introduction & Epidemiology
Compression of the ulnar nerve at the wrist, specifically within Guyon's canal, constitutes a clinically significant neuropathy distinct from more proximal entrapment sites like the cubital tunnel. Often referred to as Guyon's canal syndrome (GCS) or ulnar tunnel syndrome, this condition can lead to debilitating sensory and/or motor deficits in the hand. The volar approach to the ulnar nerve is the definitive surgical technique for direct decompression, neurolysis, and exploration of the ulnar nerve and its branches within this confined space. This approach is also invaluable for addressing traumatic injuries or excising space-occupying lesions affecting the nerve at the wrist. Its extensile nature allows for seamless proximal extension into the distal forearm, if warranted by the pathology.
The epidemiology of Guyon's canal syndrome highlights a diverse etiology. While idiopathic cases exist, identifiable causes include:
*
Traumatic:
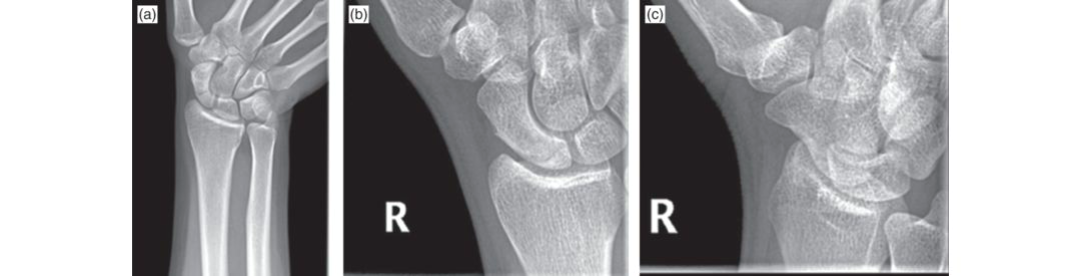
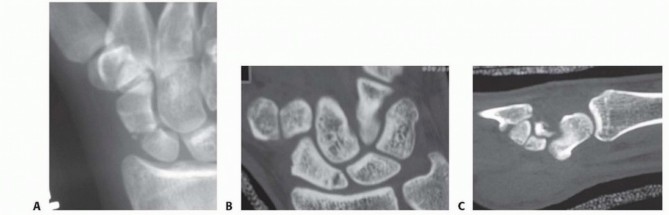
Fractures (e.g., hook of hamate, distal radius, metacarpal base), wrist dislocations, repetitive microtrauma (e.g., occupational vibration, cycling – "cyclist's palsy" from handlebar pressure).
*
Space-Occupying Lesions:
Ganglion cysts (most common, often originating from pisotriquetral joint), lipomas, anomalous muscles (e.g., accessory abductor digiti minimi), vascular anomalies (ulnar artery aneurysm or thrombosis), soft tissue tumors.
*
Inflammatory/Degenerative:
Synovitis, tenosynovitis, or arthritic changes in adjacent joints.
Clinical diagnosis is characterized by pain, paresthesia, and/or weakness in the ulnar nerve distribution distal to the wrist, with specific symptom patterns often correlating to the zone of compression within Guyon's canal. Electrodiagnostic studies (NCS/EMG) are paramount for confirming the diagnosis, localizing the level of compression, and ruling out more proximal ulnar neuropathies or cervical radiculopathy. Imaging modalities such as high-resolution ultrasound and MRI are increasingly utilized to identify specific compressive lesions, particularly space-occupying masses or vascular pathology. When conservative measures fail, or in the presence of progressive neurological deficits, surgical intervention via the volar approach provides a reliable means to alleviate nerve compression and restore function.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy of Guyon's canal and the branching patterns of the ulnar nerve at the wrist is foundational for effective and safe surgical intervention. Guyon's canal is a fibro-osseous tunnel that serves as a crucial passageway for the ulnar nerve and artery into the hand.
Boundaries of Guyon's Canal
The canal is a dynamic anatomical structure with well-defined borders:
*
Proximal:
The distal edge of the volar carpal ligament, which is continuous with the more substantial flexor retinaculum.
*
Distal:
The fibrous arch formed by the origins of the hypothenar muscles (specifically the abductor digiti minimi and flexor digiti minimi brevis) and the deep palmar aponeurosis.
*
Radial:
The hook of the hamate and the transverse carpal ligament.
*
Ulnar:
The pisiform bone and the abductor digiti minimi muscle.
*
Floor:
Primarily formed by the flexor retinaculum and the deep origins of the hypothenar musculature.
*
Roof:
Composed of the volar carpal ligament, superficial to which lies the palmaris brevis muscle (if present) and the palmar aponeurosis.
Contents of Guyon's Canal
The principal neurovascular structures within the canal are the ulnar nerve and the ulnar artery, typically accompanied by its venae comitantes. The ulnar nerve usually enters the canal just ulnar and slightly superficial to the ulnar artery.
Ulnar Nerve Branching and Zones of Compression
Within or immediately distal to Guyon's canal, the ulnar nerve typically trifurcates into its terminal branches. A clinically relevant classification, often attributed to Denis Browne, divides the canal into three zones based on the nerve's branching pattern and common sites of compression:
- Zone 1 (Proximal to Bifurcation): This zone encompasses the common ulnar nerve trunk before its division into the superficial sensory and deep motor branches. Compression here results in a mixed motor and sensory deficit, affecting all intrinsic hand muscles supplied by the ulnar nerve and sensation to the ulnar half of the ring finger and the entire little finger. Common etiologies include proximal ganglion cysts, ulnar artery thrombosis/aneurysm, or diffuse space-occupying lesions.
- Zone 2 (Deep Motor Branch): This is the most common site of compression, affecting only the deep motor branch distal to the superficial sensory branch origin. Patients present with pure motor deficits (weakness and atrophy of the interossei, adductor pollicis, and hypothenar muscles) with preserved sensation. Common causes include ganglion cysts arising from the pisotriquetral joint, hook of hamate fractures (which can impinge the nerve as it curves around the hook), or anomalous muscles.
- Zone 3 (Superficial Sensory Branch): Compression in this zone affects only the superficial sensory branch. Patients present with pure sensory deficits in the ulnar nerve distribution without motor weakness. This is the least common zone of compression and may be associated with direct trauma or superficial lesions.
Biomechanics of Compression
The confined, relatively unyielding fibro-osseous architecture of Guyon's canal renders the ulnar nerve highly susceptible to extrinsic or intrinsic compression. Any process that reduces the volume of the canal or increases the volume of its contents can lead to nerve impingement. Examples include:
*
Extrinsic Compression:
Direct external pressure (e.g., handlebars, tools), fracture callus, ligamentous thickening, or osteophytes.
*
Intrinsic Compression:
Space-occupying lesions mentioned above, or dynamic compression where specific wrist positions (e.g., sustained extension, ulnar deviation) stretch the nerve over rigid structures or exacerbate existing pathologies.
Understanding these biomechanical factors guides both the pre-operative diagnostic workup and the intra-operative strategy for complete decompression.
Indications & Contraindications
The decision for a volar approach to the ulnar nerve at the wrist is made after careful consideration of a patient's clinical presentation, objective findings, and response to non-operative management.
Indications for Volar Ulnar Nerve Decompression/Exploration
- Persistent Symptoms Refractory to Conservative Treatment: Chronic or recurrent ulnar nerve symptoms (pain, paresthesia, numbness, weakness) that have not improved after an adequate trial (typically 3-6 months) of non-operative measures, including activity modification, ergonomic adjustments, splinting, and physiotherapy.
- Progressive Neurological Deficit: Objective evidence of worsening motor weakness (e.g., increasing intrinsic muscle atrophy, progressive decrease in grip or pinch strength) or sensory loss confirmed by serial clinical examinations and/or electrodiagnostic studies.
- Acute Traumatic Injury: Suspected or confirmed ulnar nerve laceration, severe contusion, or acute compression secondary to wrist trauma (e.g., displaced hook of hamate fracture, severe crush injury) requiring exploration, neurolysis, or primary repair.
- Space-Occupying Lesion: Identification of a clearly defined compressive mass within Guyon's canal on imaging (e.g., symptomatic ganglion cyst, lipoma, ulnar artery aneurysm/thrombosis, anomalous muscle) that correlates with the patient's symptoms.
- Diagnostic Exploration: In rare circumstances where clinical suspicion of Guyon's canal syndrome is high, but electrodiagnostic studies are inconclusive, and conservative treatment has failed, surgical exploration may be undertaken to confirm the diagnosis and treat any underlying pathology.
- Recurrent Symptoms After Prior Decompression: Re-exploration for persistent or recurrent symptoms following an inadequate previous decompression or due to new pathology or significant scar formation.
Contraindications
- Active Local Infection: Any active cellulitis, abscess, or purulent infection in the surgical field.
- Uncontrolled Systemic Comorbidities: Severe, unoptimized medical conditions (e.g., unstable angina, uncontrolled diabetes, severe coagulopathy) that pose an unacceptably high anesthetic or surgical risk. These should be managed and optimized prior to surgery.
- Unrealistic Patient Expectations: Patients who have unrealistic expectations regarding the potential outcomes of the surgery, especially concerning complete symptom resolution or recovery of long-standing severe deficits.
- Resolving Symptoms: Ulnar neuropathy symptoms that are demonstrably improving with non-operative management.
- Primary Pathology Proximal to the Wrist: If the primary source of ulnar nerve compression is definitively localized more proximally (e.g., cubital tunnel syndrome, C8/T1 radiculopathy) and there is no concomitant Guyon's canal involvement requiring intervention.
- Poor Surgical Candidate: Patients unwilling or unable to participate in necessary post-operative rehabilitation protocols.
Summary of Operative vs. Non-Operative Indications
| Indication Type | Operative Management | Non-Operative Management |
| **** | | |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning and meticulous patient positioning are paramount to ensure optimal surgical access, nerve visualization, patient safety, and minimize potential complications during the volar approach to the ulnar nerve.
Pre-Operative Planning
- Clinical Review: Re-evaluate all clinical notes, electrodiagnostic reports (NCS/EMG), and imaging studies (ultrasound, MRI) to precisely confirm the diagnosis, the suspected zone of compression, and identify any anomalous anatomy or specific mass lesions. This informs the extent of planned decompression and potential need for mass excision.
- Anesthesia Consultation: Discuss anesthetic options. Regional anesthesia (e.g., axillary block) often combined with intravenous sedation, provides excellent intraoperative pain control, allows for patient cooperation if motor testing is desired, and offers prolonged post-operative analgesia. General anesthesia is also a viable option.
- Tourniquet Placement: A pneumatic tourniquet should be applied to the proximal arm. Its proper application should be confirmed with the anesthesia team.
-
Surgical Site Marking:
Pre-operatively, identify and mark key anatomical landmarks on the skin:
- Pisiform: A prominent landmark on the ulnar aspect of the proximal wrist.
- Hook of Hamate: Palpate approximately 1.5-2 cm distal and radial to the pisiform. This is crucial for navigating the deep motor branch.
- Hypothenar Eminence: Mark its radial border as a guide for the incision.
- Proximal Wrist Crease: A transverse line used as a general reference for the proximal limit of the wrist joint.
- Planned Incision Line: Draw the curved incision line based on these landmarks.
-
Equipment Check:
Ensure all necessary surgical instruments are readily available, including:
- Standard small hand surgery set.
- Surgical loupes (2.5x to 4.5x magnification) are essential for precise nerve dissection.
- Fine nerve hooks, blunt dissectors.
- Bipolar cautery.
- Vessel loops or fine silastic slings for nerve retraction.
- Small malleable retractors.
- Micro-surgical instruments if primary nerve repair is anticipated.
Patient Positioning
-
Supine Position:
The patient is placed supine on the operating table.
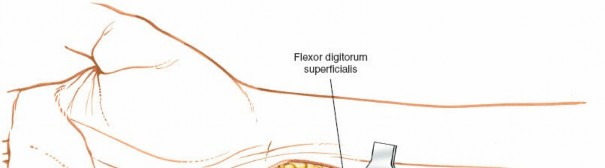
Figure 5-15: Patient positioned supine on the operating table, with the affected arm extended on a hand table. - Arm on Hand Table: The affected upper extremity is positioned on a dedicated hand table, ensuring it is stable and provides unrestricted access for the surgical team.
-
Supinated Position:
The hand is placed in a fully supinated position, with the palm facing upwards. This optimal positioning allows direct visualization of the volar aspect of the wrist and hand, facilitating the intended dissection.
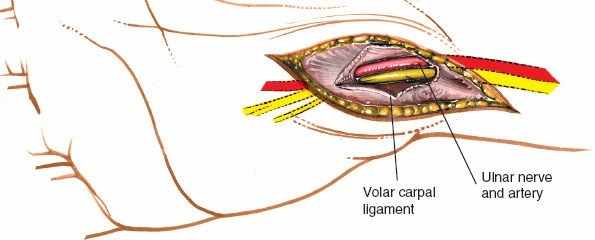
Figure depicting the hand positioned in supination on the hand table for volar access. -
Exsanguination and Tourniquet Inflation:
- After sterile preparation and draping of the limb, the extremity is exsanguinated using a soft Esmarch bandage from distal to proximal.
-
The pneumatic tourniquet, previously applied to the proximal arm, is then inflated to a pressure typically 100-120 mmHg above the patient's systolic blood pressure. This creates a bloodless surgical field, which is critical for meticulous nerve dissection and minimizing the risk of neurovascular injury.

Figure illustrating the technique of exsanguination using an Esmarch bandage, followed by tourniquet inflation.
Detailed Surgical Approach / Technique
The volar approach to the ulnar nerve at the wrist provides direct and extensile access for decompression and exploration of Guyon's canal. Precision and meticulous dissection are paramount due to the close proximity of neurovascular structures.
Landmarks and Incision
-
Re-identify Landmarks:
Once the limb is prepped and draped, reconfirm the anatomical landmarks marked pre-operatively:
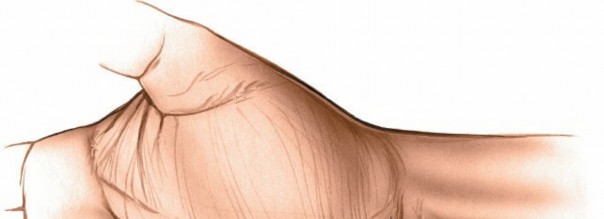
- Hypothenar Eminence: The muscular bulk on the ulnar side of the palm.
- Pisiform: Proximal ulnar wrist bone.
-
Proximal Transverse Skin Crease:
Overlies the wrist joint.

Figure 5-31: Surface anatomy of the wrist, highlighting the hypothenar eminence and wrist creases.
-
Incision:
- Make a curved incision, initiating approximately 2-3 cm proximal to the proximal wrist crease.
- The incision proceeds distally, following the radial border of the hypothenar eminence.
- It crosses the proximal transverse wrist crease obliquely, typically at an angle of about 60 degrees.
- Extend the incision onto the volar aspect of the distal forearm proximally and distally into the mid-palm, along the ulnar border of the thenar crease.
-
The incision length is typically 5 to 6 cm but can be extended proximally along the ulnar aspect of the forearm for more extensive exposure or distally into the palm for wider access to the deep motor branch. This curvilinear design aids in achieving broad exposure while minimizing scar contracture across flexion creases.

Figure 5-31: Proposed curved incision line for the volar approach to the ulnar nerve at the wrist.
Dissection
-
Skin and Subcutaneous Layers:
- Incise the skin with a No. 15 surgical blade.
- Carefully dissect through the subcutaneous tissue. Identify and protect any superficial veins (which may be ligated if necessary) and the palmar cutaneous branch of the ulnar nerve if encountered (though typically more ulnar to this incision).
-
The palmaris brevis muscle, a thin superficial muscle, may be encountered ulnarly within the subcutaneous tissue. It can be incised or retracted ulnarly.

Initial skin incision and subcutaneous fat dissection, demonstrating exposure of superficial structures.
-
Exposure of Guyon's Canal Roof:
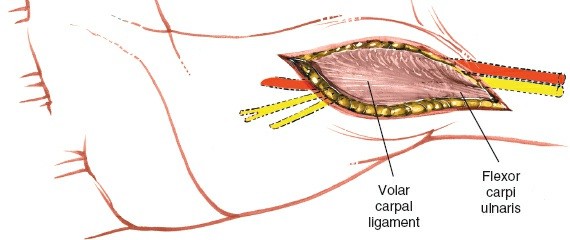
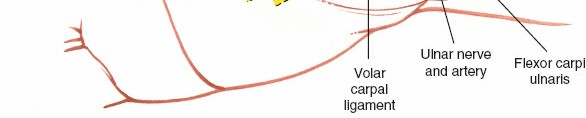
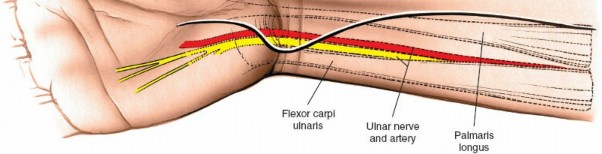
- Deep to the subcutaneous tissue, the roof of Guyon's canal is formed by the volar carpal ligament (a thickening of the antebrachial fascia). This ligament lies superficial to the ulnar nerve and artery.
-
Carefully incise the volar carpal ligament longitudinally along its ulnar aspect. Use fine scissors or a small scalpel, elevating the ligament with fine forceps to protect underlying neurovascular structures. The incision should extend proximally to release any fascial constriction in the forearm and distally to fully open the canal.

Incision of the volar carpal ligament (roof of Guyon's canal) to expose the underlying ulnar nerve and artery.
-
Identification of Ulnar Nerve and Artery:
- Once the roof is opened, the ulnar nerve and artery will be visualized within Guyon's canal. The ulnar artery typically lies radial to the ulnar nerve.
- Gently clear any overlying fatty tissue or loose connective tissue using fine blunt dissection.
- Carefully identify the ulnar nerve. It is often pale yellow and glistening. Identify the ulnar artery, which pulsates if the tourniquet is not inflated. If the tourniquet is inflated, the artery can be distinguished by its appearance and consistency.
-
Use fine nerve hooks or vessel loops to gently elevate and isolate the ulnar nerve and artery for protection and to facilitate further dissection.

Identification of the ulnar nerve and artery within Guyon's canal, with careful dissection to separate them from surrounding tissues.
-
Decompression and Exploration:
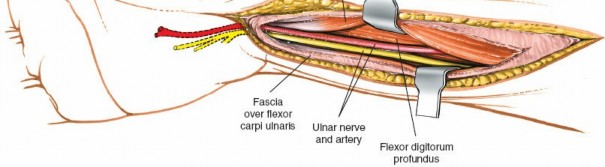
- Proximal Extension: Trace the ulnar nerve proximally into the forearm. Ensure that the distal edge of the flexor carpi ulnaris aponeurosis and any other fascial bands in the forearm are completely released to decompress the nerve fully.
-
Distal Exploration and Branching:
This is the critical step. Follow the ulnar nerve distally into the hand to identify its bifurcation into the superficial sensory branch and the deep motor branch.
- Superficial Sensory Branch: This branch continues distally, typically superficial to the hook of the hamate, supplying sensation to the little finger and the ulnar side of the ring finger.
- Deep Motor Branch: This branch characteristically dives radially and deeply, passing under the fibrous arch of the hypothenar muscles (origins of abductor digiti minimi and flexor digiti minimi brevis) and then curves around the hook of the hamate. It then courses across the palm, supplying the intrinsic muscles.
-
Release Compressive Arches:
The most common sites of compression for the deep motor branch are:
- The fibrous arch of the hypothenar muscles: Meticulously incise this arch with fine scissors or a scalpel, carefully elevating the arch away from the underlying nerve to prevent iatrogenic injury.
-
Around the hook of the hamate: Thoroughly explore this area. If a hook of hamate fracture (healed or non-united) or significant scarring is present, these structures must be addressed.
Detailed view of the ulnar nerve bifurcating into its superficial sensory and deep motor branches within the distal part of Guyon's canal.
Further distal dissection, showing the deep motor branch of the ulnar nerve as it dives radially and often curves around the hook of the hamate.

Surgical release of the fibrous arch of the hypothenar muscles, a common site of compression for the deep motor branch.
A wider view illustrating complete decompression of the ulnar nerve and its branches, ensuring free mobility and absence of constricting bands.
-
Excision of Lesions (if present):
- If a space-occupying lesion (e.g., ganglion, lipoma, anomalous muscle) is identified as the cause of compression, it should be carefully excised. For ganglion cysts, ensure the stalk is traced to its origin (e.g., pisotriquetral joint) and excised to minimize recurrence.
- If ulnar artery pathology (aneurysm, thrombosis) is discovered, appropriate vascular surgical management (e.g., resection, thrombectomy, bypass) should be considered, potentially requiring consultation.
- Neurolysis: In cases of significant scarring or nerve adherence to surrounding tissues, careful external neurolysis may be performed using fine instruments to free the nerve sheath. Internal neurolysis is rarely indicated and generally carries a higher risk of iatrogenic injury.
Internervous Plane
The volar approach to the ulnar nerve at the wrist, as described, does not follow a true internervous plane. Instead, it is an anatomical dissection directly into the structures of Guyon's canal. The initial dissection is through skin and subcutaneous tissue, then directly incising the volar carpal ligament (the roof of Guyon's canal) to expose the ulnar nerve and artery. Subsequently, dissection focuses on isolating and decompressing the nerve from all surrounding compressive structures, including fibrous arches and anomalous muscles. This direct anatomical approach underscores the critical need for precise knowledge of regional anatomy and careful surgical technique under magnification to protect the delicate neurovascular structures.
Closure
- Hemostasis: Before closure, deflate the tourniquet and ensure meticulous hemostasis using bipolar cautery. This prevents post-operative hematoma formation, which can itself cause recurrent compression or scarring.
- Subcutaneous Layer: Close the subcutaneous tissue using fine absorbable sutures (e.g., 4-0 Vicryl), taking care to avoid placing sutures too close to the decompressed nerve.
- Skin Closure: Close the skin with non-absorbable sutures (e.g., 4-0 or 5-0 nylon) or surgical staples. The curvilinear incision typically allows for a tension-free closure.
- Dressing: Apply a sterile, non-adherent dressing directly to the wound, followed by a soft compressive bandage. A volar splint may be applied in a neutral wrist position for comfort and protection for 1-2 weeks, particularly if extensive neurolysis or mass excision was performed.
Complications & Management
While the volar approach to the ulnar nerve is generally safe and effective, surgeons must be aware of potential complications and have strategies for their prevention and management.
Common Complications and Management Strategies
| Complication | Incidence (Approximate) | Salvage Strategies / Management |
Post-Operative Rehabilitation Protocols
Following surgical decompression of the ulnar nerve at the wrist, a structured rehabilitation protocol is essential for optimizing recovery, restoring function, preventing stiffness, and minimizing scar formation. The specific progression will depend on the extent of surgical intervention (e.g., simple decompression vs. nerve repair or mass excision) and individual patient factors.
Phase 1: Immediate Post-Operative (Days 0-7)
- Goals: Control pain and edema, protect the surgical site, maintain mobility of uninvolved joints.
- Pain Management: Administer oral analgesics as prescribed.
- Wound Care: Maintain a clean, dry, sterile dressing. Follow surgeon's instructions for dressing changes. Monitor for signs of infection.
- Edema Control: Encourage constant elevation of the hand above heart level (e.g., resting on pillows).
-
Immobilization:
- For simple decompression without nerve repair or extensive neurolysis , a soft compressive dressing is typically applied. A volar wrist splint in a neutral position may be used for comfort and protection, usually for 1-2 weeks, or even omitted if the patient is comfortable and compliant with gentle movements.
- If nerve repair or extensive neurolysis was performed, a volar wrist splint maintaining a neutral or slightly flexed wrist position, and often IP joints in slight flexion, is recommended for 3-4 weeks to protect the repair site.
- Early Motion (for simple decompression): Gentle, active range of motion (AROM) of the uninvolved fingers (MCP, PIP, DIP joints) should be initiated immediately to minimize stiffness and promote fluid circulation.
- Gentle Nerve Gliding (for simple decompression): Initiate very gentle ulnar nerve gliding exercises if tolerated and explicitly approved by the surgeon. These help prevent adhesion formation without stressing the nerve.
Phase 2: Early Mobilization & Light Strengthening (Weeks 1-4)
- Goals: Restore wrist and forearm range of motion, initiate gentle strengthening, continue nerve gliding.
- Splint Weaning: If a splint was used for simple decompression, it is typically discontinued around week 2, transitioning to night-time use only as needed for comfort or protection. For nerve repair, the protective splint remains for 3-4 weeks.
-
Active Range of Motion (AROM):
- Wrist: Gradually introduce active wrist flexion, extension, radial deviation, and ulnar deviation.
- Forearm: Encourage full active pronation and supination.
- Fingers: Progress full AROM of all finger joints.
-
Nerve Gliding Exercises:
Progress ulnar nerve gliding exercises:
- Level 1: "Waiter's tip" position (wrist extended, forearm pronated, fingers extended) gently moving towards shoulder.
- Level 2: "Hand-to-ear" with head tilt away.
- These exercises should be pain-free and performed gently, focusing on smooth movement rather than stretching.
- Light Strengthening: Begin isometric exercises for intrinsic hand muscles (e.g., gentle resistance with finger abduction/adduction, thumb opposition). Avoid heavy gripping or lifting.
- Scar Management: Once the incision is well-healed (typically 2-3 weeks post-op), initiate gentle scar massage to desensitize the area and prevent hypertrophic scarring. Silicone gel sheeting or scar strips may be considered.
Phase 3: Progressive Strengthening & Functional Integration (Weeks 4-12+)
- Goals: Maximize strength, dexterity, and endurance; facilitate return to full activity.
-
Progressive Strengthening:
Advance to isotonic strengthening exercises for the wrist and hand using therapeutic putty, light weights, and resistance bands. Focus on improving:
- Grip strength (e.g., towel squeeze, putty squeeze).
- Pinch strength (e.g., coin pinch, clothespin squeeze).
- Intrinsic muscle strength (e.g., resisted finger abduction/adduction).
-
Dexterity and Fine Motor Skills:
Incorporate activities that challenge fine motor coordination:
- Picking up small objects (e.g., beads, pins).
- Buttoning, zippering.
- Writing, typing.
- Sensory Re-education: If significant pre-operative sensory deficits exist, initiate sensory re-education techniques (e.g., discrimination training, texture stimulation).
- Return to Activity: Gradually progress to functional activities. Light work duties and hobbies may resume. Avoid heavy lifting, repetitive gripping, or direct pressure on the operated area. Return to more strenuous activities and sports is typically permitted after 8-12 weeks, contingent on pain levels, strength recovery, and individual progression.
- Ergonomic Assessment: Advise patients on ergonomic modifications at home and in the workplace to prevent recurrence of symptoms.
Specific Considerations for Nerve Repair
- If primary nerve repair was performed, the initial immobilization period is crucial (typically 3-4 weeks in a protected, slightly flexed wrist position).
- Rehabilitation will be significantly slower and highly individualized, dictated by the surgeon and hand therapist.
- Gentle, controlled AROM is introduced gradually after the immobilization period, strictly avoiding tension on the repair site.
- Focus will be on protecting the repair, preventing stiffness, and supporting nerve regeneration. Sensory and motor re-education will be prolonged.
Hand Therapy Involvement
Close collaboration with a certified hand therapist (CHT) is strongly recommended. The CHT provides expert guidance, individualized exercise programs, manual therapy techniques, custom splinting as needed, and patient education on precautions and self-management strategies.
Summary of Key Literature / Guidelines
The surgical management of ulnar nerve compression at the wrist, primarily Guyon's canal syndrome, is supported by a consistent body of literature and clinical consensus, though it is less common than cubital tunnel syndrome. Current guidelines emphasize a systematic approach to diagnosis and treatment.
Diagnostic Approach
- Clinical Examination: The initial diagnostic cornerstone involves a detailed history and physical examination to identify symptoms (pain, paresthesia, numbness, weakness) localized to the ulnar nerve distribution distal to the wrist. The specific presentation helps differentiate between Denis Browne's Zones of compression.
-
Electrodiagnostic Studies (NCS/EMG):
Widely regarded as the gold standard for objective confirmation.
- NCS helps localize the site of compression by demonstrating slowed conduction velocities or prolonged latencies across the wrist segment.
- EMG assesses for denervation and reinnervation changes in ulnar-innervated intrinsic hand muscles, providing prognostic information regarding axonal integrity.
- Studies (e.g., Uncini et al., 1989; Murata et al., 2005) have refined electrodiagnostic criteria for GCS.
-
Imaging Modalities:
- High-resolution Ultrasound: Increasingly recognized as a valuable, non-invasive tool. It can directly visualize the ulnar nerve within Guyon's canal, identify nerve swelling, and detect space-occupying lesions (ganglion cysts, lipomas, anomalous muscles, ulnar artery thrombosis/aneurysm) with high sensitivity and specificity (Jung et al., 2008).
- Magnetic Resonance Imaging (MRI): Provides excellent soft tissue contrast, particularly useful for characterizing complex mass lesions, subtle bone pathologies (e.g., hook of hamate stress fractures), or evaluating nerve integrity in traumatic cases.
Surgical Efficacy and Outcomes
- High Success Rates: Surgical decompression of Guyon's canal generally yields favorable outcomes, with reported success rates (defined as improvement or resolution of symptoms) ranging from 70% to over 90% (e.g., Gross and Watson, 1993; Middleton and Anakwe, 2012).
- Etiology-Specific Outcomes: Outcomes tend to be superior when a clear, treatable compressive lesion (e.g., ganglion cyst, anomalous muscle) is identified and excised, compared to idiopathic cases or those associated with diffuse conditions.
- Prognostic Factors: Factors influencing outcomes include the duration and severity of pre-operative symptoms, presence of axonal degeneration on EMG, and the specific etiology. Earlier intervention for progressive motor weakness tends to correlate with better recovery.
- Return to Function: Most patients experience significant improvement in pain and paresthesia relatively quickly. Recovery of motor strength and intrinsic muscle function can take several months, particularly in cases with significant pre-operative atrophy or axonal loss.
Operative Technique Principles
- Volar Approach as Standard: The volar approach, as detailed, is the universally accepted standard for surgical access to Guyon's canal, offering direct visualization and extensibility.
- Magnification: The use of surgical loupes (2.5x to 4.5x) is strongly recommended to facilitate meticulous dissection, minimize iatrogenic injury to the delicate nerve and its branches, and identify subtle compressive structures.
- Thorough Decompression: Guidelines emphasize the importance of complete release of all potential compressive structures. This includes not only the roof of Guyon's canal (volar carpal ligament) but also thorough exploration and release of the fibrous arch of the hypothenar muscles (for the deep motor branch) and the area around the hook of the hamate. Proximal extension into the forearm to release fascial bands (e.g., distal flexor carpi ulnaris aponeurosis) should be performed if indicated.
- Meticulous Hemostasis: Due to the proximity of the ulnar artery and venae comitantes, stringent hemostasis is crucial to prevent post-operative hematoma formation, which can create recurrent compression or significant scar tissue.
Post-Operative Management and Rehabilitation
- Early Mobilization: Modern rehabilitation protocols advocate for early, gentle active range of motion of the wrist and fingers, especially in uncomplicated decompressions, to prevent stiffness and promote nerve gliding.
- Hand Therapy: Referral to an experienced hand therapist is highly beneficial for structured exercise progression, scar management, sensory re-education, and guidance on functional return.
- Nerve Gliding: Specific nerve gliding exercises are incorporated to prevent adhesions and promote nerve mobility.
In summary, the current literature and established surgical guidelines underscore that the volar approach to the ulnar nerve offers a predictable and effective treatment for Guyon's canal syndrome when non-operative measures fail or specific indications are met. Adherence to meticulous surgical technique, combined with targeted pre-operative diagnostics and structured post-operative rehabilitation, are key determinants of successful patient outcomes.
Clinical & Radiographic Imaging
You Might Also Like