Comprehensive Guide to the Volar Approach: Carpal Tunnel & Wrist Surgical Anatomy
Key Takeaway
The volar approach is a foundational surgical technique for conditions like carpal tunnel syndrome and wrist injuries. It provides unparalleled anatomical access, critical for addressing complex pathologies. Meticulous understanding of carpal tunnel boundaries, median nerve branches (palmar cutaneous and thenar motor), and wrist structures is paramount to prevent iatrogenic injury and ensure successful outcomes.
Introduction & Epidemiology
The volar approach to the carpal tunnel and wrist represents a foundational technique in hand and wrist surgery, addressing a spectrum of pathologies from compressive neuropathies to complex traumatic injuries. Decompression of the median nerve within the carpal tunnel, most commonly for carpal tunnel syndrome (CTS), is among the most frequent procedures performed by hand surgeons globally. Epidemiologically, CTS affects 3-6% of the adult population, with a higher prevalence in females and individuals engaged in repetitive wrist movements or specific occupational tasks. Beyond CTS, the volar wrist approach is indispensable for the management of distal radius fractures, carpal instability, tumors, infections, and reconstructive procedures involving tendons and nerves.
The inherent complexity of the wrist's neurovascular and tendinous anatomy necessitates a meticulous, visually guided surgical approach. Variances in the anatomical course of critical structures, particularly the thenar motor branch and the palmar cutaneous branch of the median nerve, underscore the imperative for direct visualization, thereby mitigating iatrogenic injury. While minimally invasive techniques exist for specific indications, the open volar approach provides unparalleled anatomical access and control, particularly in cases of severe median nerve compression, recurrent CTS, revision surgery, or when concomitant pathology such as tenosynovitis, tumors, or fractures must be addressed. This comprehensive guide outlines the anatomical underpinnings, indications, surgical technique, and post-operative management associated with the volar approach to the carpal tunnel and wrist, emphasizing an evidence-based perspective.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for successful and safe execution of the volar approach.
Carpal Tunnel Anatomy
The carpal tunnel is an osteofibrous canal located at the wrist, serving as a critical conduit for the median nerve and nine flexor tendons.
*
Boundaries
:
*
Floor
: Composed of the carpal bones arranged in a U-shape. From radial to ulnar, the bones forming the floor are the scaphoid tubercle, trapezium, capitate, and hamate.
*
Roof
: Formed by the transverse carpal ligament (flexor retinaculum), a strong fibrous band stretching between the radial (scaphoid tubercle and trapezium crest) and ulnar (pisiform and hook of hamate) carpal eminences.
*
Proximal Boundary
: Defined by the distal wrist crease.
*
Distal Boundary
: Varies but is generally defined by the Kaplan's cardinal line.
*
Contents
:
*
Median Nerve
: Positioned most superficially beneath the transverse carpal ligament, on the radial side. This is the primary structure of concern in CTS.
*
Flexor Tendons
: Four flexor digitorum superficialis (FDS), four flexor digitorum profundus (FDP), and one flexor pollicis longus (FPL) tendons, all contained within their respective synovial sheaths.
*
Median Artery (Persistent)
: Rarely present but can be a source of bleeding or a space-occupying lesion.
*
Key Relationships
: The ulnar nerve and artery pass superficial to the transverse carpal ligament, within Guyon's canal. The radial artery courses laterally.
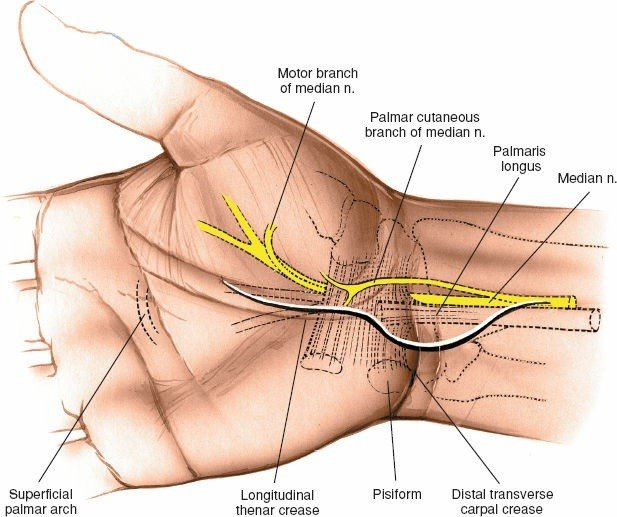
Median Nerve Branches
Two specific branches of the median nerve are critically vulnerable during a volar approach:
*
Palmar Cutaneous Branch
: This sensory branch typically originates from the median nerve approximately 5-7 cm proximal to the wrist crease, penetrating the deep fascia proximal to the transverse carpal ligament. It travels superficially and radial to the main median nerve trunk, providing sensation to the thenar eminence. Its course is highly variable; it can pass through, over, or under the transverse carpal ligament, or even pierce the FCR tendon sheath, making its protection challenging but essential.
*
Thenar Motor Branch (Recurrent Motor Branch)
: This branch supplies the thenar musculature (abductor pollicis brevis, opponens pollicis, superficial head of flexor pollicis brevis). Its origin from the median nerve and its course are notoriously variable:
*
Extraligamentous (most common, ~50%)
: Arises distal to the transverse carpal ligament, curves proximally and radially to enter the thenar muscles.
*
Subligamentous (transligamentous, ~30%)
: Pierces the transverse carpal ligament.
*
Intraligamentous (anomalous, ~20%)
: Arises within the confines of the ligament, passing through it.
*
*
This variability mandates direct visualization during ligament release to prevent iatrogenic injury.
Wrist Anatomy for Extended Volar Approaches
When addressing fractures or other extensive pathologies, the volar approach necessitates a deeper understanding of the wrist's structural components.
*
Distal Radius
: The volar surface of the distal radius is characterized by the pronator quadratus fossa and the "watershed line" (often described as the volar rim of the distal radius), which represents the insertion of the volar radiocarpal ligaments and the pronator quadratus muscle. Careful subperiosteal elevation distal to this line is crucial to preserve the ligamentous attachments and blood supply. The anterior interosseous artery and nerve lie on the interosseous membrane, deep to the pronator quadratus.
*
Flexor Tendons and Sheaths
: The FCR tendon lies radially, separating the median nerve from the radial artery more proximally. The FPL tendon runs radially within the carpal tunnel. The FDS and FDP tendons are central.
*
Neurovascular Structures
: The radial artery runs laterally to the FCR tendon, while the ulnar artery and nerve run in Guyon's canal on the ulnar side. The median nerve is central.
*
*

*
*
Biomechanics
- Carpal Tunnel : Pressure within the carpal tunnel increases with wrist flexion and extension, particularly if carpal tunnel volume is compromised (e.g., tenosynovitis, tumors). Decompression aims to reduce this pressure, restoring axoplasmic flow to the median nerve.
- Distal Radius : The volar surface of the distal radius is critical for maintaining stability, especially against dorsal displacement forces. Volar plate fixation provides rigid support, counteracting these forces and allowing early motion. The volar radiocarpal ligaments are essential static stabilizers of the carpus.
Indications & Contraindications
The volar approach is versatile, indicated for a broad range of conditions affecting the carpal tunnel and wrist.
Operative Indications (Volar Approach)
-
Median Nerve Decompression
:
- Carpal Tunnel Syndrome (CTS) : Refractory to conservative management (splinting, NSAIDs, steroid injections), objective signs of nerve compression (EMG/NCS abnormalities, thenar atrophy), severe or progressive symptoms, acute CTS (e.g., secondary to trauma, hemorrhage, infection).
- Recurrent Carpal Tunnel Syndrome : Typically requiring neurolysis and potentially flap coverage.
-
Flexor Tendon Pathology
:
- Synovectomy : For inflammatory conditions (e.g., rheumatoid arthritis, gout), chronic tenosynovitis, or infections (septic tenosynovitis).
- Tendon Repair/Reconstruction : Lacerations, ruptures, or complex reconstructions within the carpal tunnel or flexor compartments.
-
Space-Occupying Lesions
:
- Excision of Tumors : Ganglion cysts, lipomas, nerve sheath tumors (schwannomas, neurofibromas), hemangiomas, or other benign tumors compressing the median nerve or other structures.
-
Infections
:
- Drainage of Sepsis : Tracking from the midpalmar space or intrinsic to the carpal tunnel (e.g., acute flexor tenosynovitis with pus).
-
Trauma and Fractures
:
- Open Reduction and Internal Fixation (ORIF) of Distal Radius Fractures : Unstable, displaced, intra-articular, comminuted, or osteoporotic fractures, particularly those with volar displacement or significant metaphyseal comminution requiring volar plate fixation. Examples include AO/OTA Type A2, A3, B1, B2, C1, C2, C3 fractures.
- Volar Lip Fractures of the Distal Radius : Articular fragments that destabilize the radiocarpal joint.
- ORIF of Carpal Fractures/Dislocations : Examples include displaced scaphoid fractures (e.g., through an FCR approach), transscaphoid perilunate dislocations (volar component), lunate dislocations, or other carpal instabilities requiring ligament repair or reconstruction.
- Nerve/Tendon Lacerations : Acute repair of median nerve, flexor tendon, or associated vascular injuries within the carpal tunnel or wrist.
- Debridement and Fasciotomy : For compartment syndrome of the forearm/hand in select cases.
Contraindications
-
Absolute Contraindications
:
- Active local infection at the proposed surgical site (relative, requires treatment prior to elective surgery).
- Uncontrolled systemic infection.
- Severe uncorrectable coagulopathy.
- Patient refusal or inability to comply with post-operative rehabilitation.
-
Relative Contraindications
:
- Severe medical comorbidities that significantly increase surgical risk (e.g., severe cardiac, pulmonary, or renal disease) where risks outweigh potential benefits.
- Poor skin quality or scarring from previous surgeries that might compromise wound healing or tissue viability.
Table: Operative vs. Non-Operative Indications
| Indication Type | Condition | Operative Considerations | Non-Operative Considerations |
|---|---|---|---|
| Carpal Tunnel Syndrome | Mild to Moderate Symptoms, No Atrophy |
- Failed conservative management (3-6 months)
- EMG/NCS evidence of moderate-to-severe compression - Thenar atrophy or persistent motor weakness - Acute onset with rapid neurological deterioration (e.g., hemorrhage, infection) - Recurrent CTS |
- Night splinting (neutral wrist position)
- Activity modification - NSAIDs - Corticosteroid injections (limited to 1-2, spaced apart) - Physical therapy modalities (nerve gliding exercises) |
| Distal Radius Fractures | Unstable, Displaced, Intra-Articular, Open |
- Significant articular displacement (>2mm)
- Volar comminution/displacement - Shortening (>3-5mm) - Dorsal tilt (>10-20 degrees) - Significant metaphyseal comminution - Associated carpal instability - Open fractures - Irreducible fractures |
- Minimally displaced, stable extra-articular fractures
- Acceptable alignment after closed reduction - Elderly, low-demand patients with reasonable tolerance for malunion - Casting or splinting with serial radiographs for monitoring - External fixation (as a temporary measure or definitive for highly comminuted/open fractures not amenable to internal fixation, often bridging). |
| Tenosynovitis / Tumors | Symptomatic, Space-Occupying |
- Persistent pain/swelling
- Mechanical symptoms (locking, triggering) - Mass effect on neurovascular structures - Biopsy for suspected malignancy - Failed conservative management for chronic tenosynovitis |
- Rest, splinting
- NSAIDs - Steroid injections (for inflammatory tenosynovitis) - Observation (for asymptomatic or very small, benign lesions) |
| Lacerations / Infections | Acute Lacerations, Abscesses |
- Nerve/tendon/vascular lacerations
- Deep space infection, abscess formation |
- Superficial lacerations without deep structure involvement
- Cellulitis without abscess formation (responds to antibiotics) |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning and meticulous patient positioning are crucial for successful outcomes and to minimize complications.
Pre-Operative Planning
-
History and Physical Examination
:
- Thorough medical history to identify comorbidities, medications (especially anticoagulants), and allergies.
- Detailed neurovascular examination of the hand and wrist, assessing motor and sensory function of the median, ulnar, and radial nerves.
- Specific tests for CTS (Phalen's, Tinel's, Durkan's compression test) and evaluation of thenar atrophy.
- Assessment of range of motion, grip strength, and pain characteristics.
- For fractures, evaluate skin integrity, open wounds, and associated soft tissue injuries.
-
Imaging Studies
:
- Carpal Tunnel Syndrome : Often clinical diagnosis, but EMG/NCS confirms diagnosis and severity. MRI may be useful for identifying space-occupying lesions or inflammatory tenosynovitis.
- Fractures/Tumors : Standard wrist radiographs (PA, lateral, oblique views) are essential. CT scans are invaluable for assessing articular involvement, comminution, and fragment orientation for distal radius fractures and complex carpal injuries. MRI is useful for soft tissue tumors, ligamentous injuries, and occult fractures.
- Anesthesia Consultation : Discuss options with the patient and anesthesiologist (regional block such as axillary or supraclavicular, versus general anesthesia). Regional anesthesia can provide excellent post-operative analgesia.
- Informed Consent : Comprehensive discussion of the procedure, potential benefits, risks (including specific nerve injuries, infection, scar pain, recurrence), and alternatives.
Patient Positioning
- Operating Table : Place the patient supine on the operating table.
- Arm Position : The affected extremity is placed on a dedicated hand table.
-
Forearm Orientation
: The forearm is positioned in the supinated position so that the palm faces upward. This ensures optimal exposure of the volar aspect of the wrist and hand.
 - Tourniquet : An upper arm pneumatic tourniquet is routinely applied and inflated after exsanguination with an Esmarch bandage. This provides a bloodless field, which is critical for identifying delicate neurovascular structures. The duration of tourniquet use should be monitored.
- Preparation and Drape : Standard sterile preparation and draping of the hand, wrist, and forearm, allowing full visualization and manipulation.
Detailed Surgical Approach / Technique
1. Carpal Tunnel Release (Open Volar Approach)
a. Landmarks and Incision
-
Key Landmarks
:
- Thenar crease (origin of seed content).
- Distal wrist crease.
- Hook of the hamate (palpated just ulnar to the midline at the distal palm).
- Pisiform (palpated at the ulnar side of the wrist crease).
- Kaplan's cardinal line (between the hook of the hamate and the web space between thumb and index finger, indicating the approximate distal border of the transverse carpal ligament).
-
Incision Options
:
- Longitudinal Incision : Extends from the distal wrist crease (or just proximal to it) across the thenar crease into the palm, staying along the radial border of the thenar eminence. This is a common and versatile incision, providing excellent exposure while minimizing crossing of flexion creases at right angles. It should be slightly curvilinear or "zigzag" to avoid contracture.
- Short Transverse Incision : Made at the distal wrist crease. Historically used, but offers limited exposure, higher risk of incomplete release, and increased risk to the palmar cutaneous branch. Generally not recommended for primary open releases.
-
Modified Longitudinal Incision
: A longitudinal incision primarily in the palm, proximal to the thenar crease, extending approximately 3-4 cm.

For primary open release, a longitudinal incision starting just ulnar to the thenar crease, extending proximally into the wrist crease is preferred. The proximal extent should be carefully planned to avoid injury to the palmar cutaneous branch and to allow full release of the TCL.
b. Dissection and Ligament Release
- Skin Incision : The skin is incised with a No. 15 blade, approximately 3-4 cm long.
- Subcutaneous Dissection : Careful dissection through the subcutaneous fat, identifying and protecting the palmar cutaneous branch of the median nerve. This branch typically lies radial and superficial to the incision in the palm; its course is unpredictable and must be diligently sought out and preserved if encountered.
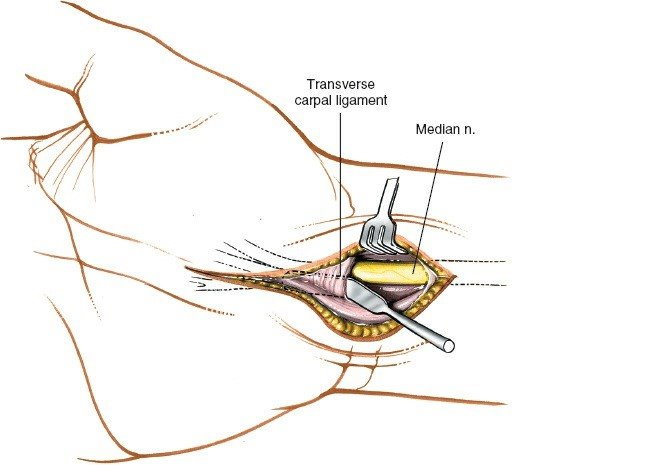
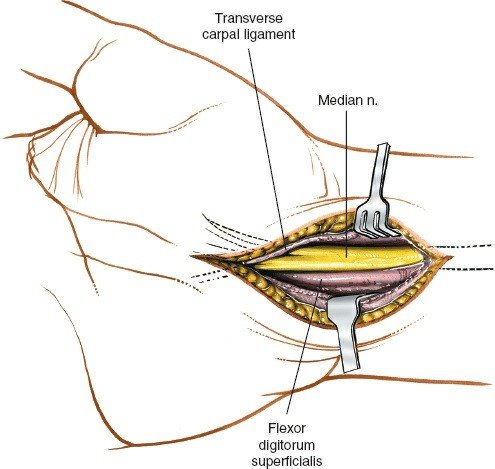
- Deep Fascia : Incise the deep fascia longitudinally. The underlying transverse carpal ligament (TCL) will be visible as a distinct, pearly-white, transversely oriented fibrous band.
- Ligament Identification : The TCL is identified, extending from the thenar eminence ulnarly towards the hypothenar eminence. Ensure clear identification of its proximal and distal margins.
-
Ligament Release
:
- Safe Zone : The release is typically initiated at the ulnar border of the TCL to protect the thenar motor branch, which usually originates from the radial aspect of the median nerve.
- Technique : A small incision is made in the TCL proximally, taking care not to injure underlying structures. A small curved blunt scissor (e.g., tenotomy scissors, "iris" scissors) or a specialized ligament knife is then introduced deep to the ligament.
- Proximal to Distal Release : The ligament is carefully divided from proximal to distal under direct vision, ensuring the entire ligament is cut, including any distal thickening. The median nerve and flexor tendons are visualized beneath the ligament.
- Protection of Thenar Motor Branch : As the dissection proceeds distally, meticulous attention is paid to identifying the thenar motor branch. If encountered, its course must be defined, and the remaining ligament released away from it. The variability of this branch (extraligamentous, subligamentous, intraligamentous) necessitates this careful approach.
- Completion : Ensure complete release of the entire transverse carpal ligament and any constricting fascia proximally and distally. The median nerve should be seen to "bowstring" or relax.
-

- Inspection : Once the ligament is completely released, the median nerve is inspected for any signs of compression, external impingement, or tumor. If significant tenosynovitis is present, a limited synovectomy of the flexor tendons may be performed.
- Hemostasis : Achieve meticulous hemostasis.
- Closure : The skin and subcutaneous tissues are closed in layers using absorbable sutures for subcutaneous tissue and non-absorbable sutures for skin. The TCL is left open to decompress the carpal tunnel. A soft compressive dressing is applied.
2. Extended Volar Approach for Distal Radius Fractures (Henry Approach)
This approach provides excellent exposure to the volar aspect of the distal radius and is commonly utilized for ORIF with volar locking plates.
a. Incision and Initial Dissection
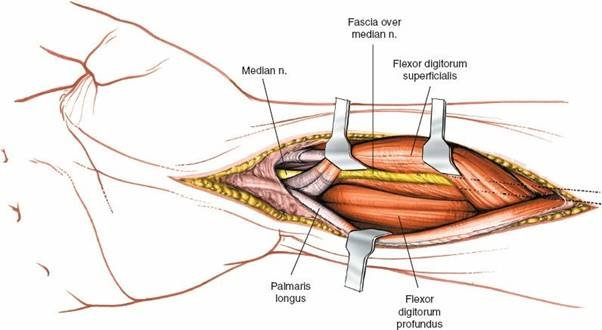
- Incision : A longitudinal incision is made on the volar aspect of the distal forearm, typically 5-8 cm in length, centered between the flexor carpi radialis (FCR) and palmaris longus (PL) tendons. It should extend proximally enough to allow for plate application and distally to the wrist crease.
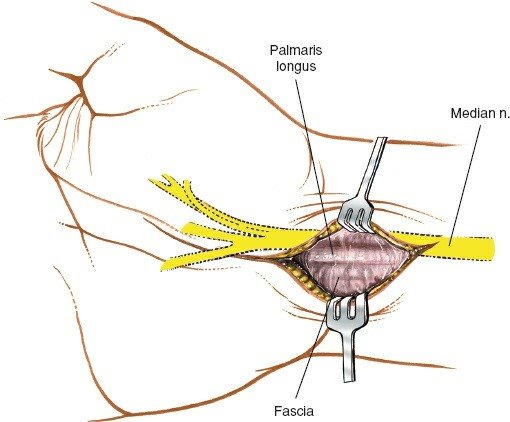
- Subcutaneous Dissection : Careful dissection through the subcutaneous tissue. Identify and protect superficial nerves (e.g., lateral antebrachial cutaneous nerve radially, palmar cutaneous branch of the median nerve ulnarly).
- Identification of FCR Tendon : The FCR tendon is identified. The incision often follows its ulnar border. The FCR sheath is incised longitudinally.
b. Internervous Plane
- The Henry approach utilizes the interval between the FCR tendon (and its associated muscle belly proximally) and the radial artery (which lies radially). More commonly, the approach proceeds ulnar to the FCR tendon , creating an interval between the FCR and the median nerve/FPL tendon. This internervous plane is between the FCR (innervated by median nerve) and the flexor digitorum superficialis (FDS) or flexor pollicis longus (FPL) (also median nerve) or more proximally between the brachioradialis (radial nerve) and FCR.
- The approach essentially exposes the deep layer of the flexor compartment.
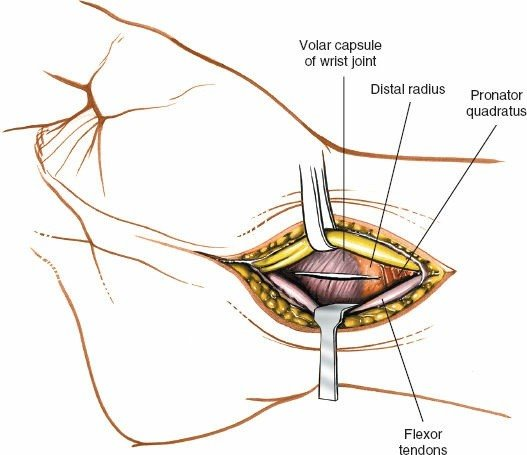
c. Deep Dissection and Pronator Quadratus Exposure
- Retraction : The FCR tendon is retracted radially. The median nerve and FPL tendon are retracted ulnarly. The radial artery must be carefully protected and may be retracted radially or ulnarly depending on its course and the need for exposure.
- Pronator Quadratus (PQ) : The pronator quadratus muscle becomes visible, running transversely across the volar aspect of the distal radius. This is the anatomical landmark for the fracture site.
-
Subperiosteal Elevation
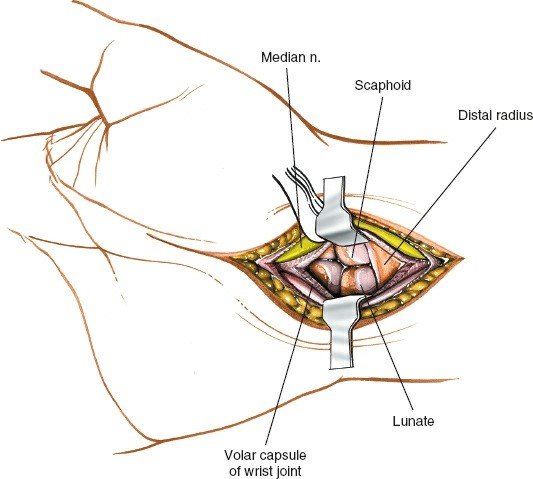
: The pronator quadratus is carefully elevated subperiosteally from its insertion on the distal radius. This is typically initiated at its ulnar border and reflected radially. Great care must be taken to stay just distal to the watershed line to preserve the volar radiocarpal ligaments and avoid devascularization of the critical volar wrist capsule structures.
 - Fracture Exposure : With the PQ elevated, the fracture site on the volar aspect of the distal radius is fully exposed. The fracture hematoma is evacuated.
d. Reduction and Fixation
- Indirect Reduction : Often achieved through ligamentotaxis using a finger trap traction device on a tower, allowing longitudinal traction to restore length and alignment.
- Direct Reduction : Fragments are manipulated directly using elevators, bone hooks, or K-wires as joysticks. Intra-articular fragments are reduced first. A ball-tipped probe or Freer elevator can be used to reduce articular fragments from the dorsal aspect, if necessary, to ensure a smooth joint surface.
- Temporary Fixation : K-wires are often used to provisionally hold reduced fragments.
- Plate Application : A volar locking plate is selected. The plate is positioned on the volar surface of the distal radius, typically distal to the watershed line, ensuring that the most distal screws provide subchondral support without penetrating the joint. The plate should contour to the natural curvature of the radius.
-
Screw Insertion
:
- Proximal Screws : Cortical screws are inserted into the proximal shaft, engaging both cortices.
- Distal Screws : Locking screws are inserted into the distal fragments, providing fixed-angle support to the articular and metaphyseal fragments. Intra-operative fluoroscopy is essential to verify screw length and avoid joint penetration. Dynamic compression screws may be used for compression across the fracture gap if appropriate.
-
Final Assessment
: Perform intra-operative fluoroscopy in multiple planes (PA, lateral, oblique) to confirm reduction, plate position, and screw length. Assess wrist and forearm range of motion to ensure no impingement or restriction.


e. Closure
- Pronator Quadratus Repair : The elevated pronator quadratus is meticulously repaired back to its origin or reapproximated over the plate, if possible, using absorbable sutures. This protects the flexor tendons from hardware irritation and aids in re-establishing anatomy.
- Sheath Closure : The FCR tendon sheath is closed.
- Layered Closure : Subcutaneous tissues and skin are closed in layers.
- Dressing : A sterile dressing is applied, often incorporating a volar splint for initial protection (particularly for fractures).
3. Volar Approach for Transscaphoid Perilunate Dislocation/Fracture-Dislocation
The volar approach is crucial for addressing the volar component of these complex injuries, including reduction of the lunate and repair of torn volar ligaments (e.g., radioscaphocapitate). This approach usually involves an extension of the FCR approach, careful identification of disrupted volar ligaments, reduction of dislocated carpal bones, and often temporary K-wire fixation before definitive reconstruction.
Complications & Management
Despite meticulous technique, complications can arise following volar wrist and carpal tunnel surgery. Proactive identification and appropriate management are essential.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Nerve Injury | ||
| - Median Nerve (main trunk) | <1% (rare) |
- Immediate re-exploration if suspected intraoperatively.
- Primary repair (direct or nerve graft) depending on defect. - Neurolysis if compressive scar. - Long-term occupational therapy, splinting. |
| - Thenar Motor Branch | 1-5% (CTS release) |
- Immediate exploration and repair if identified.
- If delayed, observation for 3-6 months. - Thenar motor reconstruction (tendon transfer, nerve transfer) for persistent paralysis (e.g., EIP to APB). |
| - Palmar Cutaneous Branch | 5-10% (CTS release) |
- Reassurance for sensory changes; usually resolves.
- Desensitization therapy. - Local anesthetic injections, neuropathic pain medication. - Excision of painful neuroma or nerve repair in rare, debilitating cases. |
| - Radial Digital Nerve | <1% (rare, especially during incision) |
- Similar to palmar cutaneous nerve injury, but often more debilitating if affecting crucial pinch.
- Surgical repair or neuroma excision if severe. |
| Infection | 1-3% |
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical debridement, intravenous antibiotics, wound culture, hardware removal (if applicable and fracture stable). - For septic tenosynovitis: Emergency drainage and irrigation. |
| Hematoma | 2-5% |
- Small: Observation, compression.
- Large/expanding: Surgical evacuation, meticulous hemostasis. |
| Scar Tenderness/Hypertrophy | 10-20% |
- Scar massage, silicone gel sheets, topical steroids.
- Desensitization exercises. - Z-plasty or scar revision in severe, persistent cases after 6-12 months. |
| Recurrence of CTS | 5-15% (long-term) |
- Non-operative management (splinting, injections) if mild.
- Revision carpal tunnel release, often with neurolysis. - Adjuvant procedures: Synovectomy, hyperextension block splinting, flap coverage (e.g., hypothenar fat pad flap) to prevent re-adhesion. |
| Pillar Pain | 20-30% (CTS release) |
- Reassurance, physical therapy, NSAIDs, local injections.
- Usually self-limiting, resolving within 6-12 months. - Rarely, surgical intervention for specific causes (e.g., neuroma in hamate region). |
| Tendon Adhesion/Rupture | <1% (more common with hardware prominence) |
- Adhesions: Aggressive physical therapy, tenolysis if severe and persistent functional deficit.
- Rupture: Tendon repair or reconstruction (graft, transfer) depending on defect and tendon involved. Hardware removal if related. |
| Vascular Injury | <1% (radial artery) |
- Direct repair or interposition graft.
- Ligation if non-dominant artery and robust collateral flow. |
| Complex Regional Pain Syndrome (CRPS) | 2-5% |
- Early diagnosis, aggressive multidisciplinary management (physical therapy, occupational therapy, pain management specialists, psychological support).
- Pharmacotherapy (gabapentin, amitriptyline, bisphosphonates). - Sympathetic blocks. |
| Fracture-Specific Complications | (for distal radius ORIF) | |
| - Nonunion/Malunion | 1-5% |
- Nonunion: Revision ORIF with bone grafting.
- Symptomatic malunion: Corrective osteotomy. - Asymptomatic malunion: Observation. |
| - Hardware-related complications | 5-10% (tendon irritation/rupture, prominent hardware) |
- Hardware removal, often delayed until fracture healing is complete.
- Repositioning of plate if screws are intra-articular and causing symptoms. - Tendon repair/reconstruction if rupture occurs. |
| - Loss of Reduction | 2-5% |
- Re-operation for revision fixation.
- External fixation, casting, or splinting. |
| - Stiffness/Loss of ROM | Common, varies by injury |
- Aggressive physical and occupational therapy.
- Dynamic splinting. - Release of adhesions (tenolysis, capsulotomy) if non-operative measures fail after sufficient time. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional outcomes, minimizing stiffness, and preventing complications following volar wrist and carpal tunnel surgery. Protocols vary based on the specific procedure performed.
Carpal Tunnel Release (Open)
-
Immediate Post-operative (Day 0-3)
:
- Immobilization : A soft bulky dressing or light wrist splint (neutral position) for comfort and protection. Some surgeons prefer no immobilization immediately post-op.
- Elevation : Hand elevation above heart level to minimize edema.
- Early Motion : Encouragement of gentle active range of motion (AROM) of digits (finger flexion and extension) immediately to prevent tendon adhesions.
- Pain Management : Standard analgesics.
-
Early Rehabilitation (Week 1-3)
:
- Wound Care : Incision inspection, suture removal (typically 10-14 days).
- Scar Management : Gentle scar massage (after wound closure) to desensitize and prevent hypertrophic scarring. Silicone sheeting or gel may be used.
- Edema Control : Continued elevation, gentle compression, retrograde massage.
- Progressive Mobilization : Full AROM of the wrist and fingers. Gentle nerve gliding exercises ("median nerve glides") to facilitate nerve mobility and prevent adhesions.
- Avoidance : Avoid excessive grip or pinch activities initially. Avoid heavy lifting.
-
Intermediate Rehabilitation (Week 4-6)
:
- Strengthening : Progressive gentle strengthening exercises for grip, pinch, and wrist muscles, gradually increasing resistance.
- Return to Activity : Gradual return to light functional activities.
- Desensitization : Continued desensitization for any residual pillar pain or scar tenderness.
-
Advanced Rehabilitation (Week 7-12 and beyond)
:
- Full Strength and Endurance : Progress to full strengthening and endurance exercises.
- Activity Modification : Advice on ergonomics and activity modification to prevent recurrence.
- Return to Work/Sport : Gradual return to full work and sports activities as tolerated, typically 2-3 months post-op, with full recovery often taking 6 months to a year.
Distal Radius Fracture (Volar Plating)
-
Immediate Post-operative (Day 0-7)
:
- Immobilization : A sugar-tong or volar splint is typically applied for initial comfort and protection, holding the wrist in a neutral to slight extension position. Some surgeons allow early motion.
- Elevation & Edema Control : Crucial for pain management and wound healing.
- Finger Motion : Immediate active range of motion of digits and elbow/shoulder to prevent stiffness.
- Pain Management : Standard analgesics, potentially regional blocks.
-
Early Rehabilitation (Week 1-6)
:
- Splinting : The splint may be removed at 1-2 weeks, and a removable wrist brace or dynamic splint initiated. Some protocols allow immediate controlled wrist motion.
- Wound Care & Suture Removal : Incision care, suture removal around 10-14 days.
- Active Range of Motion (AROM) : Gentle, controlled AROM of the wrist (flexion/extension, radial/ulnar deviation, pronation/supination) as permitted by fracture stability and surgeon preference. Focus on restoring pain-free motion.
- Passive Range of Motion (PROM) : Initiated carefully once appropriate stability is confirmed, typically under therapist guidance.
- Edema & Scar Management : As described for CTR.
-
Intermediate Rehabilitation (Week 6-12)
:
- Radiographic Assessment : Confirm fracture healing.
- Progressive Strengthening : Once radiographic healing is evident, progressive strengthening exercises for the wrist and forearm are initiated (grip, pinch, wrist flexor/extensor strengthening).
- Increased Activity : Gradual return to light functional activities, incorporating the hand and wrist.
-
Advanced Rehabilitation (Week 12 and beyond)
:
- Full Strengthening : Maximal resistance exercises.
- Proprioception and Coordination : Advanced exercises for fine motor skills and balance.
- Return to Work/Sport : Gradual return to full duty and sports, often taking 4-6 months, with continued improvement for up to a year. Regular follow-up to assess for hardware irritation.
Summary of Key Literature / Guidelines
The volar approach remains the gold standard for many hand and wrist pathologies, supported by extensive literature.
Carpal Tunnel Syndrome
- Open vs. Endoscopic Carpal Tunnel Release : Meta-analyses consistently demonstrate comparable long-term outcomes regarding symptom relief and functional recovery between open and endoscopic techniques. Endoscopic release typically offers a faster return to work and less post-operative pain in the immediate term, but may have a slightly higher, albeit still low, risk of major nerve injury in some studies. The open volar approach, as described, remains highly effective, particularly advantageous in cases with anatomical variants, revision surgery, or concomitant pathology, offering direct visualization and safety. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines provide evidence-based recommendations, endorsing surgical release for CTS refractory to conservative management.
- Recurrence : Recurrence rates are generally low after successful primary release but can be challenging. Management often involves revision decompression with meticulous neurolysis, sometimes supplemented with vascularized or non-vascularized fat pad interposition flaps to prevent re-adhesion.
Distal Radius Fractures
- Volar Locking Plates : The advent of volar locking plates has revolutionized the treatment of unstable distal radius fractures, allowing for stable fixation, restoration of anatomical alignment, and early mobilization. Numerous studies highlight their efficacy in improving functional outcomes, particularly for complex and intra-articular fractures. The AO Foundation principles for fracture management guide the use of these plates, emphasizing stable fixation and preservation of biology.
- Complication Profile : While effective, volar plating is associated with potential complications such as flexor tendon irritation/rupture (especially FPL), median nerve irritation, and hardware prominence, particularly with plates extending too distally or not adequately covered by the pronator quadratus. Careful surgical technique, including proper plate positioning distal to the watershed line and meticulous repair of the pronator quadratus, is crucial to minimize these risks.
- Comparison to Dorsal Plating/External Fixation : For appropriate fracture patterns, volar locking plates generally outperform dorsal plating in terms of reducing complication rates (especially extensor tendon issues) and external fixation in achieving superior functional outcomes and earlier return to activity, although external fixation remains valuable for highly comminuted or open fractures.
In summary, the volar approach, whether for carpal tunnel decompression or complex wrist trauma, remains a cornerstone of hand surgery. A comprehensive understanding of anatomy, meticulous surgical technique, and structured post-operative rehabilitation are key to achieving optimal patient outcomes. Continuous adherence to established guidelines and a critical appraisal of evolving literature ensure the highest standard of care.
You Might Also Like