Thumb Carpometacarpal Joint Implant and Resurfacing Arthroplasty

DEFINITION
Trapeziometacarpal joint (basal joint) arthritis is a debilitating condition that most commonly affects women in their 50s and 60s.21,22 The stage of arthritis dictates the treatment for this disorder.6,7,23Ligament reconstruction and tendon interposition (LRTI) arthroplasty, fusion, and nonbiologic reconstruction of this joint are common techniques to treat this condition.11,12,24,25This chapter will discuss the role of resurfacing arthroplasty and total joint replacement.
ANATOMY
The anatomy of the thumb metacarpal (TM) joint is extremely complex and has been well studied.3,19 The deepanterior oblique ligament (dAOL) (“beak ligament”) is the primary stabilizer of the TM joint.10,11 More recently, 16 ligaments have been described that stabilize the TM joint. Seven of these ligaments, including the superficial anterior oblique ligament (sAOL), dAOL, dorsoradial, posterior oblique, ulnar collateral, intermetacarpal, and dorsal intermetacarpal, directly stabilize the TM joint. The other 9 ligaments indirectly stabilize the TM joint bydirectly stabilizing the trapezium.3,18The TM joint is the most complex joint in the hand.8 It is a biconcave-convex saddle joint with minimal bony constraints. This joint allows flexion-extension, abduction-adduction, and pronation-supination of the thumbray.14 For optimal treatment outcomes with joint replacement, normal kinematics—six degrees of freedom— should be restored as closely as possible.
PATHOGENESIS
Degeneration of the AOL of the TM joint has been linked to the development of osteoarthritis.Pathologic laxity, abnormal translation of the metacarpal on the trapezium, and generation of abnormally high shear forces within the TM joint, especially on the palmar aspect of the joint during pinch and grip motions, occur when the AOL becomes incompetent.The base of the metacarpal tends to sublux dorsally with AOL detachment, emphasizing the importance of the AOL. In advanced osteoarthritis, adduction and flexion contractures tend to develop, producing further functional impairment and joint overload.
NATURAL HISTORY
The vast number of described operations to treat osteoarthritis of the TM joint demonstrates the lack of consensus among treating surgeons as to the best way to approach this disorder. This chapter details the role of resurfacing and implant arthroplasty for the treatment of osteoarthritis of the TM joint.Various materials, techniques, and prostheses have been used in the past. Hemiarthroplasty and total jointarthroplasty of the TM joint have largely failed, with mediocre long-term results compared with soft tissue arthroplasty.1,2,7,9,17,23 However, the appeal of a replacement may lie with quicker recovery, more normal kinematics, immediate stability, and the avoidance of metacarpal subsidence.Obviously, the perils of prosthetic alternatives revolve around durability, survivability, and complication rate. Joint resurfacing with the Artelon implant (Small Bone Innovations, Inc., Morrisville, PA) was touted to have the most potential, in terms of a biologic resurfacing. This procedure avoids the use of a semiconstrained device— which has been associated with trapezial component loosening and failure, but long-term follow-up has been characterized by a significant complication rate and poor satisfaction.
PATIENT HISTORY AND PHYSICAL FINDINGS
Arthritis of the TM joint often presents with pain at the base of the thumb during pinch and grip (stressful activities for the TM joint). Women are 10 to 15 times more likely than men to develop this disorder. Asian and Caucasian populations have an increased prevalence as well.Common offending activities include brushing teeth, opening a jar, picking up a book, or turning a key. All of these activities involve increasing the breadth of grasp or forceful lateral pinch. Usually, the pain is localized at the base of the thumb on the dorsal or volar radial aspect of the thenar cone. Patients often feel the joint slipping or subluxing radially.A “shoulder sign” is an enlarging prominence (the result of a dorsally subluxing proximal metacarpal on the trapezium and metacarpal adduction) that develops with progressive disease.Other causes of pain in the hand should be evaluated (see Differential Diagnosis list) as well. This is important because any concomitant disease, such as a trigger thumb, may hamper the postoperative therapy regimen and negatively affect the patient's final outcome.The treating physician should also keep the diagnosis of carpal tunnel syndrome in mind, as it coexists in about 44% of patients with TM joint arthritis. Furthermore, the postoperative swelling from a basal joint arthroplasty may exacerbate even mild cases of carpal tunnel syndrome.The Allen test should be performed on every patient who is undergoing surgery for basal joint arthroplasty, as the radial artery will be near or in the operative field and mayP.1078need to be mobilized depending on the exact procedure performed. Any injury to the radial artery should be repaired immediately.The stability of the metacarpophalangeal (MCP) joint of the thumb is also critical, as this is a source of postoperative stress on the reconstructed beak ligament from either ligament reconstruction or suspensionplasty procedures.MCP joint fusion or volar plate capsulodesis should be performed when the MCP joint hyperextends to greater than 20 degrees.15Methods for examining the carpometacarpal (CMC) joint of the thumb include the following:CMC grind test: A positive test is suggestive of degenerative disease.CMC instability test: Laxity of the TM joint is common in early stages of degeneration, but as the joint degenerates, it usually becomes stiffer.MCP joint stability test: If the MCP joint is actively hyperextending, this could put undue stress on a reconstructed TM joint and lead to failure. This hyperextendable MCP joint should be stabilized.Metacarpal base compression test: Glickel13 believed that this is more commonly painful in advanced stages rather than milder stages of TM joint disease.Distraction test: A positive result from this maneuver is thought to be caused by traction on an inflamed TM joint capsule.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Imaging of the TM joint includes a true anteroposterior (AP) view of the TM joint (called aRobert view or pronated AP), lateral, and posteroanterior 30-degree oblique stress view (with thumb tips pressing against each other).The most common staging system was originally described by Eaton and Littler11,12: stage 1 shows slight widening of the joint, possibly from synovitis; stage 2 demonstrates some joint space narrowing and osteophytes smaller than 2 mm; stage 3, osteophytes larger than 2 mm; and stage 4 disease, scaphotrapezial joint space involvement along with TM joint narrowing.The senior author of this chapter has described a “fifth stage” in which the disease process is pantrapezial and there is TM, scaphotrapezial, and scaphotrapezoidal joint degeneration. Scaphotrapezoidal arthritis can be a source of continued pain and this joint should be evaluated intraoperatively in every patient because, unfortunately, preoperative radiographs are only 44% sensitive and 86% specific for diagnosing arthritis at thisjoint.26
DIFFERENTIAL DIAGNOSIS
Scaphotrapezial arthritis Scaphotrapezoidal arthritis Thumb sesamoid arthritis Carpal tunnel syndrome De Quervain tenosynovitisStenosing flexor tenosynovitis (trigger finger)
NONOPERATIVE MANAGEMENT
Initial management of TM joint arthritis is nonoperative and includes anti-inflammatory medication, thenar cone muscle isometric strengthening exercises, hand- or forearm-based thumb spica splint immobilization, steroid injections, and activity modification.These measures may not alleviate any or all of the patient's symptoms, but they may help enough to provide temporary relief, allowing the patient ample time to educate himself or herself and to contemplate the treatment alternatives.The time afforded by the nonoperative measures may also allow the patient to schedule the operation at a more convenient time.
SURGICAL MANAGEMENT
There are several options for surgical treatment of TM joint arthritis. LRTI, suspensionplasty, and CMC joint fusion are discussed in other chapters. This chapter focuses on the role of resurfacing and implant arthroplasty. Resurfacing is an increasingly attractive option in younger, more active patients in whom one might prefer toavoid trapeziectomy to eliminate the risk of metacarpal subsidence with time. Subsidence can result in recurrent pain and weakness.The Artelon (Small Bone Innovations) spacer is a bioabsorbable implant (FIG 1A) that degrades and is replaced with scar tissue that protects the base of the TM and the distal aspect of the trapezium. This implant is ideal for a younger laborer with TM arthritis in whom grip and pinch strength are of critical importance. The attraction of this alternative is that it is a potentially definitive procedure that does not “burn the bridge” of resectionarthroplasty in the future.20Pyrocarbon resurfacing using the “saddle” implant (Ascension Orthopedics, Austin, TX; FIG 1B) is an alternative to Artelon. Its design mimics the articular shape of the metacarpal articular surface, which may more closely restore CMC joint kinematics compared to Artelon implant use. Little information exists in the literature, however, regarding outcomes; in 2009, Mayo Clinic investigators reported on the use of pyrolytic carbon hemiarthroplastyfor the treatment of CMC arthritis and 49 patients.16 This investigation showed that its use was an acceptable option, although a high complication rate was observed in the early cohort, with many cases of subluxation attributed to the creation of a too shallow trapezial cup.Total joint arthroplasty, such as with the Avanta CMC implant (FIG 1C), is another option. Implant arthroplasty options may require less immobilization, lead to quicker return of functional abilities, obviate metacarpalsubsidence, and provide immediate stability.5 In 2006, the outcomes following 26 procedures in 25 patientswere reported.2 This series intimated that this option was efficacious and feasible for the osteoarthritic thumb. Indeed, a review of implant options published in 2013 acknowledges that a variety of metal total joint prostheseshave been developed and that favorable short-term outcomes have been reported.27 However, the literature is full of articles describing failures of innumerable prosthetic implants for the TM joint, thus appropriate patient selection remains critical.
PREOPERATIVE PLANNING
Many other hand pathologies can coexist with TM joint arthritis. These other diagnoses should be evaluated before the day of surgery.P.1079If an Allen test had not been performed previously, it should be performed before the surgery.
POSITIONING

FIG 1 • A. Artelon implant demonstrating T shape with two dorsal wings. B. Pyrocarbon saddle implant. C. Avanta CMC implant. (C: Courtesy of Small Bone Innovations, Inc., Morrisville, PA.)
APPROACH
There are several different approaches for soft tissue arthroplasties, but for resurfacing or implant arthroplasties, a dorsal approach seems to work the best and to offer the best visualization.
TECHNIQUES
Artelon Resurfacing Arthroplasty
ARTELON RESURFACING ARTHROPLASTY
EXPOSURE


TECH FIG 1 • Dorsal approach to the TM joint after reflecting the joint capsule.
JOINT PREPARATION
Use a high-speed sagittal saw to remove the distal facet of the trapezium. Take care not to injure the flexor carpi radialis (FCR) or flexor pollicis longus (FPL) tendons, which lie on the volar side of the bony cut.Alternatively, a burr can be used to decorticate the trapezial surface while maintaining its native contour.Use a high-speed burr to slightly decorticate the dorsum of the proximal metacarpal to stimulate healing but not enough to affect the suture anchor fixation (TECH FIG 2).
IMPLANT PLACEMENT


TECH FIG 2 • Appearance of the TM joint after bone cuts on trapezium, burring of proximal TM, and

TECH FIG 3 • Appearance of the resurfacing arthroplasty after stabilization of the Artelon implant with suture anchors.
Pyrocarbon Resurfacing Arthroplasty
PYROCARBON RESURFACING ARTHROPLASTY
EXPOSURE
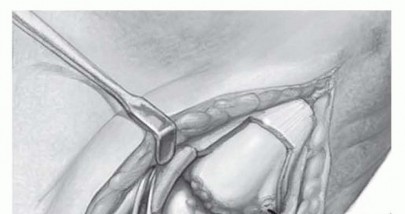
Make a dorsal longitudinal incision centered over the CMC joint. Identify and protect the branches of the superficial radial nerve throughout the procedure, along with the EPL and EPB.After mobilizing and protecting the radial artery, mobilize the EPL and EPB tendons enough to facilitate a longitudinal incision through the capsule. Reflect the capsule enough to completely visualize the joint.Subperiosteal release allows the base of the metacarpal to be dislocated dorsal to the trapezium. Place a Hohmann retractor beneath the palmar surface to maintain exposure.
JOINT PREPARATION

TECH FIG 4 • Extramedullary guide to plan placement of saddle implant.
IMPLANT PLACEMENT

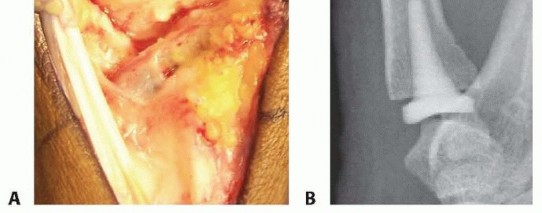
TECH FIG 5 • A. Saddle implant in place. B. Postoperative lateral radiograph showing implant in place. P.10812. Total Joint Replacement
EXPOSURE
We use a technique and surgical approach similar to that described by Badia and Sambandam2 for implanting a Braun-Cutter trapeziometacarpal joint prosthesis (or Avanta CMC implant; Small Bone Innovations; see FIG 1C) using bone cement.Make a 4-cm longitudinal incision over the dorsal aspect of the base of the thumb. Identify and protect branches of the superficial sensory radial nerve. Perform further dissection between the EPL and EPB tendons, isolating and protecting the dorsal branch of the radial artery.Open the dorsal capsule of the trapeziometacarpal joint longitudinally. Reflect the periosteum and the dorsal capsule radially and ulnarly as a single flap to be repaired later (TECH FIG 6).
JOINT PREPARATION
TECH FIG 6 • The first compartment is opened from the volar side and the strands of the abductor pollicis longus (APL) are inspected. A strand of the APL that inserts on the base of the metacarpal in the bone area that will be resected should be freed from its insertion and tagged for later repair. (Courtesy of Small Bone Innovations, Inc., Morrisville, PA.)



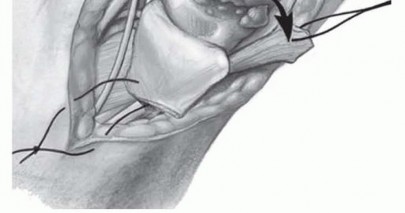
TECH FIG 7 • The capsule of the trapeziometacarpal joint is excised (A) and the joint is exposed (B). C. The alignment of the metacarpal component is parallel to the axis of the metacarpal shaft, with slight volar inclination. The trapezial joint surface is evaluated. If the surface is fairly intact, blocking volar, ulnar, and radial osteophytes are removed and the hole is burred for the trapezium component. D. The metacarpal canal is reamed and prepared for prosthetic insertion. (A,C,D: Courtesy of Small Bone Innovations, Inc., Morrisville, PA.) P.1082
IMPLANT PLACEMENT
Place the implant and perform a trial reduction so that motion and fluoroscopic images can be assessed. If there is any bony impingement at the periphery of the residual trapezium, this can be addressed before placing the permanent prosthesis.For final placement, first cement the trapezial cup in the trapezium, taking care to impact the cement beneath the subcortical bone.Once the cup has been inserted but before the cement has cured, insert the TM component with bone cement (TECH FIG 8A). TECH FIG 8 • A,B. The components are cemented into place, the trapezium first and the metacarpal second. Compression should be maintained until the bone cement has completely set. C. Postoperative lateral radiograph showing implant in place. (A: Courtesy of Small Bone Innovations, Inc., Morrisville, PA.)


|Preoperative ▪ Always do an Allen test before surgery.1. Always evaluate the thumb MCP joint for active instability-hyperextension.Intraoperative ▪ Use extreme caution mobilizing the radial artery. Often, bipolar electrocautery facilitates mobilization, especially of the deep perforators at the volar base of the TM joint.2. Evaluate the scaphotrapezoidal joint, as preoperative radiographs are not good at predicting disease.3. Be careful when sawing or drilling not to injure structures deep to the bone.4. After making the bone cuts on the trapezium and burring the proximal metacarpal, drill and place the suture anchors far enough away from the prepared bone to avoid inadvertent breakout in the fresh cancellous bone surfaces.5. Once the implant has been secured and the capsule repaired, do not manipulate by the thumb, as this may put undue stress on the soft tissue repair.6. After the procedure, before contaminating the sterile field, release the tourniquetand observe the reperfusion of the hand to ensure that no unexpected arterial|Postoperative ▪ Have a postoperative therapy protocol for patients to follow.injury occurred.
POSTOPERATIVE CARE
P.1083At the end of the surgery, the patient is placed into a thumb spica splint to keep the thumb in opposition. At 2 weeks postoperatively, the sutures are removed and placement into a thumb spica cast continues for 2 more weeks.The cast immobilization is discontinued at 6 weeks postoperatively if Artelon resurfacing has been used and at 2 weeks if CMC replacement has been performed. A custom Orthoplast thumb-based spica splint (Johnson & Johnson, New Brunswick, NJ) is worn full time for protection, except during showers and therapy.Formal therapy is usually not required after total joint replacement. In the case of resurfacing, therapy will focus on range-of-motion exercises only for postoperative weeks 4 to 6, advancing to thenar isometrics for weeks 6 to8. At 8 weeks postoperatively, the patient will start grip and pinch strengthening exercises; the splint is also discontinued at this point.
OUTCOMES
Several long-term studies have shown better than 90% satisfaction and pain relief with soft tissue arthroplasties, but favorable long-term outcome studies in support of the Artelon implant or for total joint arthroplasty are infrequent. In 2013, a retrospective review was published of 38 patients who received anArtelon implant.4 Twelve of 32 patients (37%) required revision surgery with removal of implant and salvage arthroplasty. Twenty patients with non-revised Artelon implants were compared with 10 patients who received 13 LRTI procedures; patients with Artelon has significantly less pain improvement compared to those receiving the LRTI procedure. In addition, satisfaction was significantly decreased. As was theconclusion of the arteries of this study,4 the authors have abandoned the use of Artelon in the treatment of thumb CMC joint osteoarthritis.Although the literature supports the use of pyrolytic carbon hemiarthroplasty16 and total joint arthroplasty2 in the treatment of thumb CMC joint arthritis, patient selection remains very important because nonimplant options provide favorable outcomes.
COMPLICATIONS
Superficial branch of the radial nerve injury Damage to flexor tendons during saw use Radial artery injuryDislocation or subsidence of total joint implant Subluxation of TM jointContinued pain or discomfortFailure to recognize other sources of pathology in the hand and wrist
REFERENCES
- Athwal GS, Chenkin J, King GJ, et al. Early failures with a spheric interposition arthroplasty of the thumb basal joint. J Hand Surg Am 2004;29(6):1080-1084.
- Badia A, Sambandam SN. Total joint arthroplasty in the treatment of advanced stages of thumb carpometacarpal joint osteoarthritis. J Hand Surg Am 2006;31(10):1605-1614.
- Bettinger PC, Linscheid RL, Berger RA, et al. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg Am 1999;24(4):786-798.
- Blount AL, Armstrong SD, Yuan F, et al. Porous polyurethaneurea (Artelon) joint spacer compared to trapezium resection and ligament reconstruction. J Hand Surg Am 2013;38(9):1741-1745.
- Bozentka DJ. Implant arthroplasty of the carpometacarpal joint of the thumb. Hand Clin 2010;26:327-337.
- Burton RI, Pellegrini VD Jr. Basal joint arthritis of thumb. J Hand Surg Am 1987;12(4):645.
- Burton RI, Pellegrini VD Jr. Surgical management of basal joint arthritis of the thumb. Part II. Ligament reconstruction with tendon interposition arthroplasty. J Hand Surg Am 1986;11(3):324-332.
- Cooney WP III, Chao EY. Biomechanical analysis of static forces in the thumb during hand function. J Bone Joint Surg Am 1977;59(1): 27-36.
- De Smet L, Sioen W, Spaepen D, et al. Total joint arthroplasty for osteoarthritis of the thumb basal joint. Acta Orthop Belg 2004;70: 19-24.
- Doerschuk SH, Hicks DG, Chinchilli VM, et al. Histopathology of the palmar beak ligament in trapeziometacarpal osteoarthritis. J Hand Surg Am 1999;24(3):496-504.
- Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am 1973;55(8):1655-1666.
- Eaton RG, Littler JW. A study of the basal joint of the thumb: treatment of its disabilities by fusion. J Bone Joint Surg Am 1969;51(4):661-668.
- Glickel SZ. Clinical assessment of the thumb trapeziometacarpal joint. Hand Clin 2001;17:185-195.
- Haines RW. The mechanism of rotation at the first carpometacarpal joint. J Anat 1944;78:44-46.
- Lourie GM. The role and implementation of metacarpophalangeal joint fusion and capsulodesis: indications and treatment alternatives. Hand Clin 2001;17:255-260.
- Martinez de Aragon JS, Moran SL, Rizzo M, et al. Early outcomes of pyrolytic carbon hemiarthroplasty forthe treatment of trapezialmetacarpal arthritis. J Hand Surg Am 2009;34:205-212.
- Naidu SH, Kulkarni N, Saunders M. Titanium basal joint arthroplasty: a finite element analysis and clinical study. J Hand Surg Am 2006;31(5):760-765.
- Nanno M, Buford WL Jr, Patterson RM, et al. Three-dimensional analysis of the ligamentous attachments of the first carpometacarpal joint. J Hand Surg Am 2006;31(7):1160-1170.
- Napier JR. The form and function of the carpometacarpal joint of the thumb. J Anat 1955;89:362-369.
- Nilsson A, Liljensten E, Bergström C, et al. Results from a degradable TMC joint spacer (Artelon) compared with tendon arthroplasty. J Hand Surg Am 2005;30(2):380-389.
- Pellegrini VD Jr. Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration. I. Anatomy and pathology of the aging joint. J Hand Surg Am 1991;16(6):967-974.
- Pellegrini VD Jr. Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration. II. Articular wear patterns in the osteoarthritic joint. J Hand Surg Am 1991;16(6): 975-982.
- Pellegrini VD Jr, Burton RI. Surgical management of basal joint arthritis of the thumb. Part I. Long-term results of silicone implant arthroplasty. J Hand Surg Am 1986;11(3):309-324.
- Tomaino MM. Suspensionplasty for basal joint arthritis: why and how. Hand Clin 2006;22:171-175.
- Tomaino MM, Pellegrini VD Jr, Burton RI. Arthroplasty of the basal joint of the thumb. Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77(3):346-355.
- Tomaino MM, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am 1999;24:1220-1224.
- Vitale MA, Taylor F, Ross M, et al. Trapezium prosthetic arthroplasty (silicone, Artelon, metal, and pyrocarbon). Hand Clin 2013;29:37-55.
