Tendon Transfers for Ulnar Nerve Palsy

DEFINITION
Ulnar nerve palsy refers to loss of sensory and motor function after injury to the ulnar nerve above or below the wrist (high vs. low ulnar nerve palsy).
ANATOMY
The ulnar nerve is the terminal branch of the medial cord (C8 and T1).The ulnar nerve consists of motor and sensory fibers. There are no muscles innervated by the ulnar nerve in the arm. In the forearm, the flexor carpi ulnaris receives its nerve branches after the ulnar nerve passes through the cubital tunnel. The other muscles innervated in the forearm are the flexor digitorum profundus of the ring and small fingers.The muscles innervated in the hand (by order of innervation) are the following:Hypothenar musclesAbductor digiti minimi Flexor digiti minimi Opponens digiti minimiRing and small lumbricalsDorsal and palmar interosseous muscles Adductor pollicisDeep head of flexor pollicis brevisFirst dorsal interosseous (last muscle innervated by the ulnar nerve)The sensory fibers of the ulnar nerve supply the small finger and the ulnar half of ring finger over the entire palmar surface and the dorsal surface distal to the proximal interphalangeal (PIP) joint. The dorsal surface proximal to the PIP joint of the small finger and the ulnar half of the ring finger and ulnar dorsum of the hand are innervated via the dorsal sensory branch of the ulnar nerve, which arises from the ulnar nerve 7 cm proximal to the wrist. The sensory branch crosses from volar to dorsal at the level of the ulnar styloid.
PATHOGENESIS
Ulnar nerve palsy can arise from a laceration anywhere along its course. Proximal injuries to the medial cord may present with additional sensory loss in the distribution of the medial brachial or antebrachial cutaneous nerves. Nerve compression typically occurs either at the cubital tunnel at the elbow or the canal of Guyon at the wrist.A variety of systemic conditions may mimic ulnar neuropathy, including Charcot-Marie-Tooth disease, syringomyelia, and leprosy. In Charcot-Marie-Tooth disease and syringomyelia, there is weakness involvingother nerves. In leprosy, there is a profound loss of sensation in the ulnar nerve distribution in addition to the claw deformity of the fingers.
NATURAL HISTORY
The severity of the nerve palsy depends on the degree of the nerve lesion and the presence of anomalous innervation patterns (Martin-Gruber, Riche-Cannieu) in determining the number of muscles involved and the extent of palsy. Anomalous innervation patterns can confuse the examiner.Martin-Gruber anastomosis patterns are divided into four types:Type I (60%): Motor branches from the median nerve are sent to the ulnar nerve to innervate “median” muscles.Type II (35%): Motor branches from the median nerve are sent to the ulnar nerve to innervate “ulnar” muscles.Type III (3%): Motor branches from the ulnar nerve are sent to the median nerve to innervate “ulnar” muscles.Type IV (1%): Motor branches from the ulnar nerve are sent to the median nerve to innervate “median” muscles.With prolonged nerve palsy, secondary abnormalities of the hand occur, such as stretching of the central slip of the extensor mechanism at the PIP joint or fixed joint flexion contractures.
PATIENT HISTORY AND PHYSICAL FINDINGS

FIG 1 • A. With lateral pinch, the thumb interphalangeal joint flexes (Froment sign) and the thumb MCP joint hyperextends (Jeanne sign). B. With finger extension, the ring and small fingers hyperextend at the MCP joints and flex at the proximal and distal interphalangeal joints (Duchenne sign). Flattening of the metacarpal arch with loss of the hypothenar muscles produces loss of the small finger to oppose through the carpometacarpal joint (Masse sign). C. Clawing of the ring and small fingers when the MCP joints are allowed to extend. This worsens as the patient flexes the wrist to try to aid finger extension (Andre-Thomas sign). D. Full extension of ring and small finger PIP joints when MCP hyperextension is blocked indicates a competent central slip (Bouvier maneuver). Bouvier maneuver: inability to actively extend PIP joint when MCP joints are hyperextended and ability to actively extend PIP joint when MCP joints are blocked from hyperextension (FIG 1C,D). When active PIP joint extension is possible with the MCP joints blocked, this indicates competence of the central slip (positive test). When PIP joints cannot actively extend (negative test), this implies central slip attenuation. In this case, tendon transfers will need to block MCP joint hyperextension and provide PIP joint extension.Andre-Thomas sign: clawing of ring and small fingers, hyperextension of MCP joints and flexion of PIP joints, flexion of wrist (FIG 1C). An increase in the claw deformity as the patient tries to extend the fingers by flexing the wrist indicates a poor prognosis for tendon transfer surgery.Masse sign: flattening of the metacarpal arch (see FIG 1B); inability to oppose the small finger carpometacarpal jointPollack sign: inability to flex the distal interphalangeal joint of the ring and small fingers; used to differentiate high from low ulnar nerve palsyIn assessing for tendon transfers in ulnar nerve palsy, the primary functional concerns are the following:Lack of thumb adduction and lateral pinchClaw deformity of fingers that impairs object acquisition and grip Loss of ring and small finger flexion (high palsy)
IMAGING AND OTHER DIAGNOSTIC STUDIES
Electromyographic and nerve conduction velocity studies are used to isolate the ulnar nerve pathology and rule out other diagnoses. Serial studies may demonstrate the potential for recovery.
DIFFERENTIAL DIAGNOSIS
Cervical radiculopathy Lower brachial plexopathyCharcot-Marie-Tooth disease SyringomyeliaLeprosy
NONOPERATIVE MANAGEMENT
When the Bouvier test is positive (active PIP joint extension is possible when MCP joint hyperextension is prevented), a dorsal MCP blocking splint for the ring and small fingers is fabricated to preserve the integrity of the PIP joint central slips.If a fixed flexion contracture of more than 45 degrees occurs at the PIP joint, a supervised hand therapy program consisting of serial casting is required.If the fixed flexion contracture does not respond to therapy, preliminary surgical joint release is necessary before tendon transfers.
SURGICAL MANAGEMENT
Tendon transfers address the primary functional concerns listed earlier9:Lack of thumb adduction and lateral pinchClaw deformity of the fingers that impairs object acquisition and grip Loss of ring and small finger flexion (high palsy)
CONSIDERATIONS
Restoring Thumb AdductionThe first factor to consider in performing a transfer to restore thumb adduction is what donor muscle to use.The extensor carpi radialis brevis (ECRB)10 and the flexor digitorum superficialis (FDS)5 are the most commonly used.The FDS of the ring finger can be used in low ulnar nerve palsy when the flexor digitorum profundus of the ring finger is functioning.3In high ulnar nerve palsy, the FDS of the middle finger can be used instead of the FDS of the ring finger. The brachioradialis can be used if the ECRB is required for an intrinsic reconstruction of the fingers.Alternatively, the extensor indicis proprius or abductor pollicis longus can be used.P.857The second factor to consider is placement of the pulley.For transfers coming from the dorsum of the hand, the pulley is either the index or middle finger metacarpal. Passing the transfer through the third web space, using the middle metacarpal as the pulley, allows thetransferred tendon to lie palmar to the adductor pollicis but dorsal to the flexor tendons and neurovascular bundles.For transfers originating from the palm of the hand (FDS), the vertical septum of the palmar fascia attached to the third metacarpal forms the pulley.The third factor is attachment of the transfer to the thumb.The transfer can be inserted directly into the thumb metacarpal, into the adductor pollicis tendon, or into the abductor pollicis brevis tendon.This last technique, favored by Omer,6 allows the tendon to be sewn to the strong fascia abductor pollicis longus tendon and improves pronation of the thumb to aid in pinch.The last factor to address is stability of the MCP and interphalangeal joints.For patients with a persistent Froment sign and mild hyperextension of the MCP joint, the split FPL to extensor pollicis longus tenodesis will stabilize the interphalangeal joint without fusion.When the MCP joint shows substantial instability or arthritic changes, it should be fused.Correcting Claw Deformity of FingersProcedures to correct MCP hyperextension may be either static or dynamic.A static procedure prevents hyperextension of the MCP joint, improving extension of the fingers. The Bouvier maneuver must be positive. The disadvantage of static procedures, either the MCP volar capsulodesis or tenodesis procedure, is that they tend to stretch with time.A dynamic transfer uses the FDS, extensor carpi radialis longus, ECRB, or flexor carpi radialis as a donor muscle.If the Bouvier maneuver is positive, there is no need to restore PIP joint extension.If the Bouvier maneuver is negative, the procedure must address both MCP joint flexion and PIP joint extension. The insertion site of the tendon transfer determines which joints are affected by the transfer.FDS transfers for finger clawing7AdvantagesNo need for tendon graftNot passing tendon through interosseous spaces or through carpal tunnel DisadvantagesDoes not increase grip strengthHigh incidence of swan-neck deformitiesCannot use FDS of ring and small fingers in high ulnar nerve palsyWrist motors for transfers for finger clawing4Advantage: increases grip strength DisadvantagesRequires tendon graft, either palmaris longus, plantaris, fascia lata, or toe extensorPasses tendon through interosseous spaces or through carpal tunnelRestoring Ring and Small Finger Extrinsic Muscle FunctionIn patients with high ulnar nerve palsy, it is important to restore extrinsic flexion power before performing intrinsic transfers.Claw deformity of the ring and small fingers will worsen after these transfers.
PREOPERATIVE PLANNING
Tendon transfers are indicated when no further nerve recovery is anticipated.In evaluating a patient for tendon transfer procedures, the examiner assesses the number of functions lost, determines the number of muscles available for transfer, and assesses the strength and excursion of each ofthe donor and recipient muscles.2When there are insufficient donor muscles to substitute for all functions that are lost, tenodesis and arthrodesis procedures may partially substitute for the lost function.There should be no fixed flexion contractures of the joints affected by the transfers. The transferred tendons need to be placed in a smooth, scarfree bed to glide.The principle of “one muscle and one function” should apply to each tendon transfer.
POSITIONING
The patient is supine with the arm abducted on an arm table.
APPROACH
All transfers for thumb adduction must pass distal to the pisiform.All transfers for intrinsic reconstruction must pass palmar to the axis of rotation of the MCP joint and dorsal to the axis of the PIP joint.P.858
TECHNIQUES
Transfers to Restore Thumb Adduction
TRANSFERS TO RESTORE THUMB ADDUCTION
Brachioradialis Extended with Tendon Graft, through Third Web Space, Inserted into Abductor Pollicis Brevis Tendon


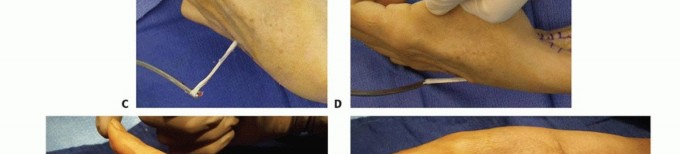
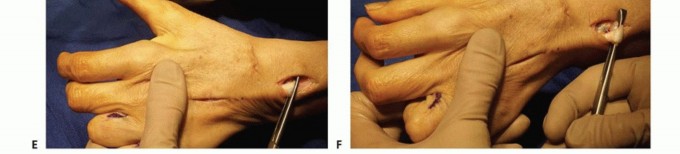
TECH FIG 1 • A. The brachioradialis muscle is freed into the proximal third of the forearm. The tendon is lengthened with a palmaris longus graft via a three-pass Pulvertaft method. B. Tendon graft taken from a slip of the abductor pollicis longus is sewn into the insertion of the abductor pollicis brevis tendon. The graft is passed palmar to the adductor pollicis muscle. The tendon is shown through the palmar incision before being passed dorsally through the third web space. C. Abductor pollicis longus tendon graft passed dorsally through the third web space. D. Brachioradialis with tendon graft passed into the incision over the dorsal hand. E. Tensioning of tendon transfer. With the wrist in neutral and no tension on the graft, the thumb should fully extend. F. Tensioning of tendon transfer. With the wrist in neutral and moderate tension on the tendon, the thumb strongly adducts to the index finger.


TECH FIG 2 • A. The FPL tendon is split into radial and ulnar halves at its insertion into the distal phalanx. The radial half is transected at the level of the interphalangeal joint. B. The radial half of the FPL tendon is woven into the radial half of the extensor pollicis longus tendon. A pin is placed across the interphalangeal joint in full extension. C. FPL split tenodesis sewn into place. Split Flexor Pollicis Longus to Extensor Pollicis Longus Tenodesis Make an incision along the radial proximal phalanx of the thumb. Identify the FPL and extensor pollicis longus tendons. Take care to preserve the oblique pulley.Identify the natural cleft between the radial and ulnar fibers of the FPL and split the tendon (TECH FIG 2A).Weave the radial half of the FPL tendon into the extensor pollicis longus tendon (TECH FIG 2B,C). Pin the interphalangeal joint in extension with a 0.045-inch smooth pin.1. Tendon Transfers for Claw Deformity of Fingers
ZANCOLLI LASSO
This operation is indicated when there is a positive Bouvier maneuver. Make a midpalm Bruner zigzag incision.Incise the tendon sheath between the A1 and A2 pulleys. Identify the FDS tendon and transect it just proximal to the bifurcation. Leaving the bifurcation intact will decrease the incidence of PIP hyperextension.Zancolli11 recommends using the FDS of each finger, but Anderson1 recommends using the FDS of the middle finger, split into four tails, to control MCP flexion of all four fingers.Pull the FDS tendon out of the tendon sheath distal to the A1 pulley, bring it palmar to the A1 pulley, and sew it to itself proximal to the A1 pulley. If insufficient MCP flexion is attained, the tendon exits the pulley sheath in the middle of the A2 pulley to improve the lever arm of the transfer.Set tension so the MCP joint is in 40 to 50 degrees of flexion with the wrist in neutral.When one FDS tendon is used for all four fingers, transect the FDS middle tendon distal to the A2 pulley through an oblique incision on the finger.Make a transverse midpalm incision, retrieve the tendon, and split it into four tails.Pass each tail down the lumbrical canal, palmar to the deep transverse metacarpal ligament, and into the flexor sheath proximal to the A1 pulley. Pass the tendon around the pulley and sew the distal end of the tendon back to itself proximal to the A1 pulley, tensioning it while the MCP joint is in 40 to 50 degrees of flexion with the wrist in neutral.For either the Zancolli or Anderson technique, the tendon may be sewn to the proximal metaphyseal-diaphyseal junction of the proximal phalanx via suture anchors or pullout drill holes.
STILES-BUNNELL TRANSFER
This technique is indicated when the Bouvier maneuver is negative.One FDS tendon is used to motor two digits. Make radial midaxial incisions over the proximal phalanges of the digits. Make a midpalmar incision to retrieve the tendon. Cut the FDS ring tendon just proximal to its bifurcation between the A1 and A2 pulleys.Split the tendon and pass each half down the lumbrical canal. Pass the tendon passer from distally to proximally, going palmar to the deep transverse intermetacarpal ligament.Sew the tendon to the lateral band to restore PIP extension. Set tension with the MCP joint in 40 to 50 degrees of flexion and the PIP joints in full extension with the wrist in neutral. Excessive tension will cause PIP hyperextension.P.860 Dorsal Route Transfer of Extensor Carpi Radialis Brevis


TECH FIG 3 • A. Tendon graft is passed from the dorsum of the hand over the fourth web space, palmar to the deep transverse intermetacarpal ligament, and through the lumbrical canals of the ring and small fingers to exit over the radial lateral bands of the fingers. B. Tendon grafts have been sewn to the proximal phalanges by suture anchors. Tension on the tendon grafts causes MCP flexion.If the Bouvier maneuver is negative, attach the graft to the radial lateral band of the middle, ring, and small fingers and the ulnar lateral band of the index finger.Retrieve the ECRB tendon through a dorsal incision. Bring the tendon grafts through the same wound. First, sew the grafts to each other, synchronized to obtain even pull-through the grafts. Then, sew the grafts to the ECRB tendon with the wrist in 30 degrees of extension and the MCP joints in 60 degrees of flexion.1. Transfer of Flexor Digitorum Profundus Ring and Small to Flexor Digitorum Profundus Middle (High Ulnar Nerve Palsy)Make a longitudinal incision over the distal third of the forearm. Identify the flexor digitorum profundus tendons.After synchronizing the long, ring, and small tendons, place two rows of horizontal sutures between the three tendons.
PEARLS AND PITFALLS
Evaluation ▪ Differentiate high from low ulnar nerve palsy.1. Determine the potential for nerve and muscle recovery.2. Critically assess the strength of the donor muscles.3. Determine the integrity of the PIP central slip (Bouvier maneuver).4. Have the patient prioritize functional impairment.Adductorplasty ▪ Assess both adduction and opposition.5. Dorsal transfers passed through the third web space allow for strong adduction using a wrist extensor or the brachioradialis muscle.6. Hyperextension of the MCP joint and hyperflexion of the interphalangeal joint must be addressed with either a capsulodesis and fusion of the MCP joint or a split FPL tenodesis. Both the MCP and interphalangeal joints should not be fused.Claw finger deformities1. Determine the integrity of the PIP central slip (Bouvier maneuver).2. When the Bouvier maneuver shows that the PIP central slip is competent, the tendon transfer should be sewn to the proximal phalanx or the pulleys. If the central slip is not competent, the tendon transfer is sewn into the lateral band.3. Transfers need to pass palmar to the axis of rotation of the MCP joints.
POSTOPERATIVE CARE
P.861A knowledgeable hand therapist plays an important role in the postoperative care of tendon transfers for ulnar nerve palsy. Protecting the transfers with well-made splints while mobilizing uninvolved joints requires strictadherence to postoperative protocols.8For most procedures, the hand is immobilized for 3 weeks, followed by a blocking splint to allow motion within the restraints of the splint for the next 3 weeks.Passive exercises are begun at 6 weeks and strengthening at 8 weeks for the adductorplasty and at 10 to 12 weeks for the intrinsic tendon transfers.
OUTCOMES
After tendon transfers for thumb adduction, pinch strength usually improves from 25% to 50% of normal.Tendon transfers to improve intrinsic function maintain good to excellent correction of the claw deformity in 80% to 90% of patients.Only the ECRB transfer improves grip strength.
COMPLICATIONS
More complications occur after intrinsic muscle transfers than adductorplasty because of the delicate balance of the extensor hood mechanism.Transfer not strong enoughProblems include choice of a muscle with insufficient strength or excursion, use of a soft tissue pulley that stretched, or elongation at the tendon transfer site.Elongation is a particular problem with sewing the transfer into the lateral bands of the extensor hood. Patients with this transfer must be instructed on not hyperextending the MCP joints.Transfers that are not strong enough can be treated with a therapy program to strengthen the muscle but often require surgical revision.Transfer too strongProblems include choice of a muscle that is too strong or with too short of an excursion or sewing the transfer in with too much tension.When the transfer is sewn too tightly into the lateral band, it can produce a swan-neck deformity of the digit.Transfers that are too tight can be treated with passive range of motion in therapy, trying to stretch the transfer.
REFERENCES
- Anderson GA. Ulnar nerve palsy. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Elsevier, 2005:1161-1196.
- Brand PW, Beach RB, Thompson DE. Relative tension and potential excursion of muscles in the forearm and hand. J Hand Surg Am 1981;6(3):209-219.
- Hamlin C, Littler JW. Restoration of power pinch. J Hand Surg Am 1980;5(4):396-401.
- Hastings H II, Davidson S. Tendon transfers for ulnar nerve palsy. Evaluation of results and practical treatment considerations. Hand Clin 1988;4:167-178.
- Hastings H II, McCollam SM. Flexor digitorum superficialis lasso tendon transfer in isolated ulnar nerve palsy: a functional evaluation. J Hand Surg Am 1994;19(2):275-280.
- Omer G. Tendon transfers for combined traumatic nerve palsies of the forearm and hand. J Hand Surg Br 1992;17(6):603-610.
- Ozkan T, Ozer K, Gülgönen A. Three tendon transfer methods in reconstruction of ulnar nerve palsy. J Hand Surg Am 2003;28(1): 35-43.
- Rath S. Immediate postoperative active mobilization versus immobilization following tendon transfer for claw deformity correction in the hand. J Hand Surg Am 2008;33(2):232-240.
- Sachar K. Reconstruction for ulnar nerve palsy. In: Berger RA, Weiss APC, eds. Hand Surgery. Philadelphia: Lippincott Williams & Wilkins, 2004:979-990.
- Smith RJ. Extensor carpi radialis brevis tendon transfer for thumb adduction—a study of power pinch. J Hand Surg Am 1983;8(1): 4-15.
- Zancolli EA. Claw-hand caused by paralysis of the intrinsic muscles: a simple surgical procedure for its correction. J Bone Joint Surg Am 1957;37-A(5):1076-1080.
