Surgical Treatment of Deep Space Infections of the Hand

Surgical Treatment of Deep Space Infections of the Hand
Introduction & Epidemiology
Deep space infections of the hand represent a critical and potentially devastating condition requiring prompt diagnosis and aggressive management to preserve hand function. These infections occur within the anatomically defined potential spaces of the hand, delimited by fibrous septa and fascial layers. Untreated or inadequately treated infections can lead to significant morbidity, including widespread tissue necrosis, osteomyelitis, septic arthritis, tenosynovitis, chronic pain, and profound functional impairment. In severe cases, systemic sepsis and limb loss are possible sequelae.
The most commonly encountered deep space infections involve the thenar, midpalmar, and hypothenar spaces, the interdigital subfacial web space, and Parona’s space in the distal forearm, which communicates with hand structures. Thenar space infections are statistically the most frequent of these entities, while midpalmar and hypothenar space infections are comparatively less common.
The etiology of deep space infections typically involves direct penetrating trauma, such as puncture wounds or lacerations, which introduce pathogens directly into these compartments. Alternatively, infection may spread contiguously from adjacent infected sites, such as superficial abscesses, felon, paronychia, or critically, from pyogenic flexor tenosynovitis (PFT). The latter is particularly relevant for thenar and midpalmar space involvement due to the communication of the radial and ulnar bursae with these deep spaces.
The microbiology of these infections is often polymicrobial, reflecting the complex microflora of the skin and the environment. Staphylococcus aureus remains the single most common causative organism, including Methicillin-Sensitive Staphylococcus aureus (MSSA) and increasingly, Methicillin-Resistant Staphylococcus aureus (MRSA). Other frequently isolated pathogens include various species of Streptococcus and Gram-negative bacilli, such as coliforms, especially in cases related to human or animal bites, immunocompromised hosts, or specific environmental exposures. Early empirical antibiotic therapy must account for these prevalent organisms, with definitive treatment guided by culture and sensitivity results obtained intraoperatively.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy of the hand’s fascial planes, synovial sheaths, and neurovascular structures is paramount for the successful surgical management of deep space infections. The hand's complex architecture compartmentalizes potential spaces, dictating the spread of infection and guiding surgical approaches.
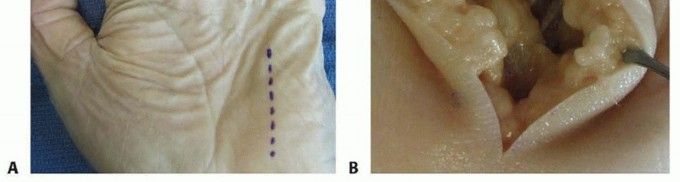
The images provided illustrate key anatomical considerations for these infections:

These diagrams likely depict the intricate fascial layers and potential spaces within the hand, highlighting the critical boundaries that define these compartments.
Deep Palmar Fascial Spaces
The palmar aponeurosis and the thenar and hypothenar eminences form key anatomical landmarks that define the deep fascial spaces.
-
Thenar Space:
-
Boundaries:
- Anterior: Flexor tendons of the index finger and their lumbrical.
- Posterior: Adductor pollicis muscle.
- Radial: Web space of the thumb.
- Ulnar: Midpalmar septum separating it from the midpalmar space.
- Contents: Primarily the first lumbrical muscle.
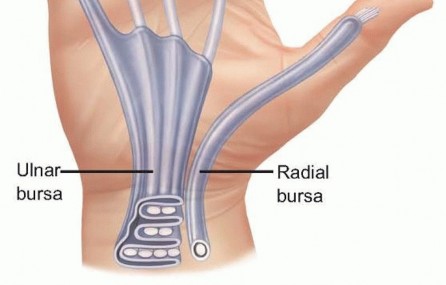
- Communication: Can communicate with the radial bursa, making it susceptible to spread from flexor pollicis longus tenosynovitis.
-
Significance:
Infections often present with thumb abduction and flexion contracture due to adductor pollicis spasm.
-
Boundaries:
-
Midpalmar Space:
-
Boundaries:
- Anterior: Flexor tendons of the middle, ring, and small fingers, and their lumbricals, dorsal to the palmar aponeurosis.
- Posterior: Interosseous muscles and metacarpals.
- Radial: Midpalmar septum, separating it from the thenar space.
- Ulnar: Hypothenar septum, separating it from the hypothenar eminence.
- Contents: Flexor tendons (middle, ring, small fingers) and their lumbricals.
- Communication: Directly communicates with the carpal canal and the ulnar bursa, making it vulnerable to spread from flexor tenosynovitis of the small finger and sometimes the ring finger. It can also communicate with the interdigital web spaces.
-
Significance:
Infections often lead to loss of the normal palmar concavity and tenderness over the space.
-
Boundaries:
-
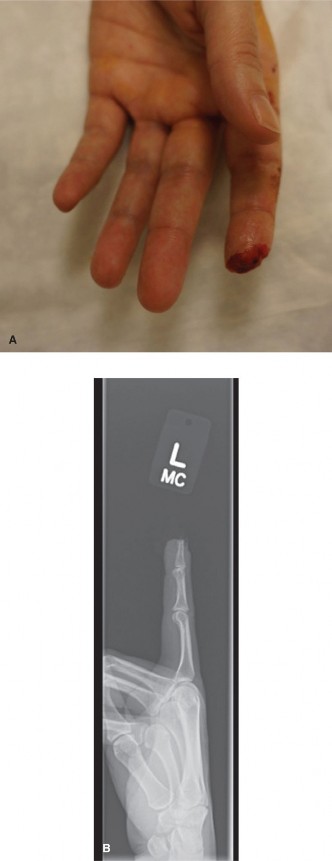
Hypothenar Space:
- Boundaries: The muscles of the hypothenar eminence. It is less a distinct deep space and more a collection of muscles separated by fascial planes.
- Contents: Hypothenar muscles (abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi).
-
Significance:
Less commonly involved in isolated deep space infections; more frequently affected by direct trauma or spread from the small finger, as seen in this image.

Interdigital Subfacial Web Space (Collar Button Abscess)
- Location: Between the metacarpal heads, distal to the deep transverse metacarpal ligament.
- Anatomy: Characterized by superficial and deep collections of pus separated by the deep transverse metacarpal ligament.
- Communication: Communicates dorsally with the dorsal subcutaneous space and volarly with the midpalmar space.
-
Significance:
Often presents with significant swelling and pain, with pus pointing both dorsally and volarly (hence "collar button").

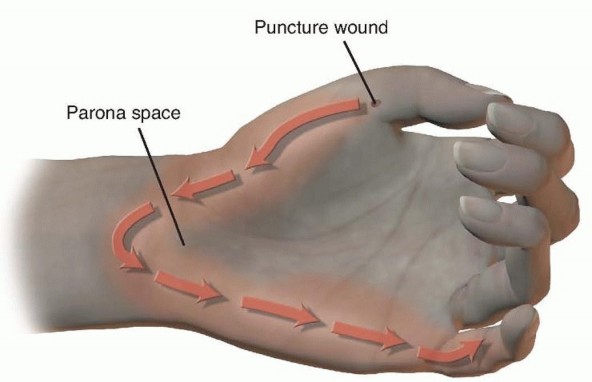
Parona's Space
- Location: A potential space in the distal forearm, volar to the pronator quadratus and deep to the flexor digitorum profundus and flexor pollicis longus tendons.
- Communication: Crucially, Parona's space communicates directly with the radial and ulnar bursae (flexor tendon sheaths) within the carpal canal.
-
Significance:
Infection in Parona's space typically signifies extensive flexor tenosynovitis of either the radial bursa (thumb) or ulnar bursa (small finger, often communicating with ring and middle finger sheaths), requiring aggressive drainage both in the hand and distal forearm.

The biomechanical implications of these spaces relate to the path of least resistance for purulent exudate. The tough fascial septa prevent direct circumferential spread, forcing pus to track along neurovascular bundles, tendon sheaths, or into adjacent communicating spaces. This compartmentalization, while protective in some respects, can also lead to increased pressure within a closed space, compromising blood supply and facilitating rapid tissue destruction if not promptly decompressed.
Indications & Contraindications
The decision for surgical intervention in deep space hand infections is critical and often time-sensitive.
Indications for Operative Management
- Clinical Evidence of Pus: Fluctuance on examination, despite initial antibiotic therapy.
- Failure of Non-Operative Treatment: Persistence or worsening of symptoms (pain, swelling, erythema, limited range of motion) after 24-48 hours of appropriate intravenous antibiotics.
- Systemic Signs of Sepsis: Fever, tachycardia, hypotension, leukocytosis with a left shift, requiring emergent source control.
- Progressive Local Signs: Rapidly expanding erythema, lymphangitis, or lymphadenopathy.
- Signs of Impending Tissue Necrosis: Blanching, dusky skin, severe pain out of proportion to exam.
- Suspicion of Pyogenic Flexor Tenosynovitis (PFT): Kanavel's signs (uniform swelling of the digit, semi-flexed posture, tenderness along the flexor sheath, pain with passive extension), often precedes or coexists with deep space infections.
- Imaging Confirmation: Ultrasound or MRI demonstrating a localized fluid collection suggestive of an abscess.
- Presence of Foreign Body: Particularly if infected or thought to be contributing to the infection.
- Immunocompromised Patient: Lower threshold for surgical intervention due to increased risk of rapid progression and severe complications.
Contraindications for Operative Management
True contraindications are rare in the setting of deep space hand infections, given the urgency of source control. However, relative contraindications or factors requiring stabilization prior to surgery include:
- Early Cellulitis Without Abscess Formation: In the absence of a distinct fluid collection or fluctuance, empirical broad-spectrum intravenous antibiotics and close observation may be sufficient.
- Patient Instability: Uncontrolled comorbidities (e.g., severe cardiac disease, respiratory failure) that preclude safe anesthesia or surgery. In such cases, emergent stabilization and resuscitation are paramount, often followed by surgical drainage once stable enough.
- Lack of Surgical Expertise: Referral to a specialist hand surgeon is indicated if the local team lacks experience in complex hand anatomy and deep space drainage.
Operative vs. Non-Operative Indications
| Feature/Condition | Non-Operative Management | Operative Management |
|---|---|---|
| Diagnosis | Cellulitis without fluctuance or clear abscess formation. | Deep space abscess confirmed by clinical exam (fluctuance), aspiration of pus, or imaging (US/MRI). |
| Clinical Course | Stable or improving symptoms (pain, swelling, erythema) after 24-48 hours of IV antibiotics. | Worsening symptoms, spread of erythema, development of fluctuance, or systemic signs of sepsis despite appropriate IV antibiotics. |
| Infection Type | Superficial cellulitis, early stages of infection without pus collection. | Deep space infection, pyogenic flexor tenosynovitis (Kanavel's signs), suspected osteomyelitis, septic arthritis, necrotizing fasciitis. |
| Systemic Symptoms | Afebrile or low-grade fever, no signs of sepsis. | High fever, tachycardia, hypotension, signs of systemic inflammatory response (SIRS) or sepsis. |
| Imaging Findings | Negative for abscess, foreign body, or bony involvement. | Ultrasound showing fluid collection >1 cm, MRI showing deep space abscess, X-ray showing foreign body or early osteomyelitis. |
| Pathogen | Non-specific or responsive to empirical broad-spectrum antibiotics (e.g., uncomplicated cellulitis). | Suspected resistant organisms, polymicrobial infection, or failure to respond to initial antibiotics. |
| Patient Status | Immunocompetent, good overall health. | Immunocompromised, diabetic, vascular compromise, or other high-risk factors increasing infection severity. |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is essential for a successful outcome.
Diagnostic Workup
- History and Physical Examination: Thorough history including mechanism of injury, time of onset, previous hand infections, and comorbidities. Detailed hand examination focusing on swelling, erythema, tenderness, fluctuance, digital posture, and neurovascular status. Assessment for Kanavel's signs is critical.
- Laboratory Studies: Complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) to assess inflammation. Blood cultures should be drawn, especially if systemic signs of infection are present.
-
Imaging:
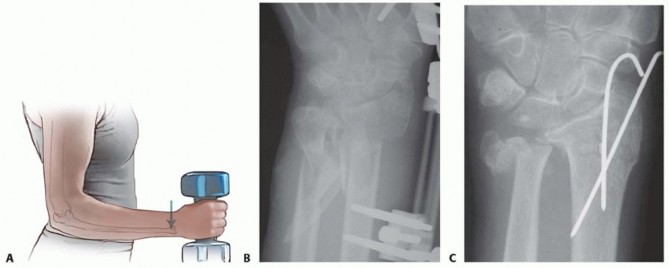
- Plain Radiographs: Anteroposterior, lateral, and oblique views to rule out foreign bodies, osteomyelitis, or septic arthritis.
- Ultrasound: Can be highly effective in identifying and localizing fluid collections, guiding aspiration, and differentiating cellulitis from abscess.
-
Magnetic Resonance Imaging (MRI):
Reserved for complex, diffuse, or chronic infections, or when osteomyelitis/septic arthritis is suspected and cannot be adequately assessed by plain films or ultrasound. It provides excellent soft tissue detail.

Antibiotic Prophylaxis/Therapy
- Empirical Broad-Spectrum Antibiotics: Initiate immediately upon diagnosis, tailored to likely pathogens (e.g., Gram-positive coverage for S. aureus , consideration for Gram-negative and anaerobic coverage based on mechanism of injury or patient factors). Vancomycin or linezolid for MRSA coverage, combined with a beta-lactamase inhibitor or cephalosporin for Gram-negative coverage, is a common initial regimen.
- Definitive Therapy: Adjust antibiotics based on intraoperative Gram stain, culture, and sensitivity results.
Anesthesia
- Regional Anesthesia: Axillary or supraclavicular block is often preferred as it provides excellent analgesia and muscle relaxation, minimizing tourniquet pain, and allowing the patient to remain awake.
- General Anesthesia: May be necessary for anxious patients, extensive infections, or those unable to tolerate regional anesthesia.
Patient Positioning and Preparation
- Positioning: Supine position with the affected arm abducted and pronated on a hand table. This allows for optimal access to both volar and dorsal aspects of the hand.
- Tourniquet: A pneumatic tourniquet applied to the upper arm is essential to achieve a bloodless surgical field, allowing for precise identification of anatomical structures and thorough debridement.
-
Sterile Prep and Drape:
Standard sterile preparation of the entire limb, from fingertips to above the tourniquet.

Detailed Surgical Approach / Technique
The primary surgical objectives are drainage of pus, debridement of necrotic tissue, acquisition of tissue for culture, and thorough irrigation. Incisions must provide adequate access while respecting vital neurovascular structures and future hand function.
General Principles of Drainage
- Longitudinal Incisions: Whenever possible, incisions should be longitudinal in relation to the hand's long axis, typically volar for deep palmar spaces and dorsal for web spaces/superficial infections.
- Avoid Transverse Incisions: Transverse incisions across flexion creases should generally be avoided to prevent contractures.
- Protect Neurovascular Structures: Meticulous blunt dissection should be employed, especially near known neurovascular bundles.
- Adequate Exposure: Incisions must be sufficient to allow complete exploration and drainage of all compartments involved.
- Thorough Debridement: All necrotic tissue, devitalized fat, and foreign bodies must be removed.
- Irrigation: Copious irrigation with saline.
- Drainage: Placement of soft rubber drains (e.g., Penrose or small suction drains) is often necessary to prevent re-accumulation of pus and allow continued egress of exudate.
- Delayed Primary Closure (DPC) or Secondary Intention: Wounds are typically left open or packed loosely to allow for continued drainage and to monitor for further infection. DPC may be considered after 3-5 days if the infection is controlled and the wound is clean.
Specific Surgical Approaches
1. Thenar Space Infection
- Incision: A longitudinal incision centered over the thenar crease on the palmar aspect, extending from the distal thumb crease towards the wrist. This incision should be carefully placed to avoid injury to the recurrent motor branch of the median nerve (which innervates thenar muscles) and the radial digital nerve to the thumb.
-
Technique:
- Incise skin and subcutaneous tissue.
- Bluntly dissect through the thenar muscles, carefully spreading tissue longitudinally.
- The space lies deep to the flexor tendons of the index finger and superficial to the adductor pollicis muscle.
- Once the abscess cavity is entered, perform thorough digital exploration, debridement, and irrigation.
-
Place a Penrose drain and leave the wound open or loosely packed.

2. Midpalmar Space Infection
-
Incision:
- Transverse Incision: A transverse incision in the distal palmar crease, extending from the second to the fifth metacarpal, can be used for broad access. This incision should stay within the skin crease to minimize contracture.
- Longitudinal Incisions: Individual longitudinal incisions over the affected metacarpal shafts (usually between the metacarpals) or in the interdigital web spaces are also viable, especially if the infection is more localized.
-
Technique:
- Incise skin and subcutaneous tissue.
- For a transverse incision, divide the palmar aponeurosis.
- Bluntly dissect between the flexor tendons and the deep palmar fascia. The space is situated between the flexor tendons (anteriorly) and the interosseous muscles/metacarpals (posteriorly).
- Carefully avoid the digital neurovascular bundles lying volar to the flexor tendons.
- Explore, debride, and irrigate thoroughly.
-
Place Penrose drains into the deepest recesses of the space and leave the wound open.

3. Hypothenar Space Infection
- Incision: A longitudinal incision along the ulnar border of the hand, over the hypothenar eminence.
-
Technique:
- Incise skin and subcutaneous tissue.
- Bluntly dissect through the hypothenar muscles. The space is less defined than the thenar or midpalmar spaces.
- Debride and irrigate.
-
Place a drain if necessary and leave the wound open.

4. Interdigital Web Space (Collar Button Abscess)
-
Incision:
Often requires both dorsal and volar incisions to adequately drain the superficial and deep collections.
- Volar: A short, transverse incision in the distal palmar crease, centered over the web space.
- Dorsal: A longitudinal incision over the affected web space on the dorsum of the hand.
-
Technique:
- After incising the skin, blunt dissection through the superficial palmar fascia and then through the deep transverse metacarpal ligament is often necessary to connect the volar and dorsal abscess cavities.
- Crucial: Thoroughly explore both dorsal and volar collections.
-
Debride, irrigate, and pass a Penrose drain through the web space, connecting the dorsal and volar aspects to ensure continuous drainage.

5. Parona's Space Infection (often with Pyogenic Flexor Tenosynovitis)
- Incision: A longitudinal incision on the ulnar border of the distal forearm, approximately 2-3 cm proximal to the wrist crease, carefully avoiding the ulnar nerve and artery. An additional volar wrist incision (Carpi Ulnaris approach) may be utilized for wider access to the flexor tendons and ulnar bursa, extending distally into the palm.
-
Technique:
- Incise skin and subcutaneous tissue.
- Bluntly dissect between the flexor carpi ulnaris (FCU) and the neurovascular bundle, or between the flexor digitorum superficialis and profundus muscles.
- The space lies deep to the flexor tendons and superficial to the pronator quadratus.
- A common finding is diffuse pus surrounding the flexor tendons, requiring thorough exploration, debridement of necrotic synovium, and copious irrigation.
- If associated with tenosynovitis, the entire flexor tendon sheath (radial or ulnar bursa, and digital sheath) must be drained. Mid-axial digital incisions are used for digital tenosynovitis.
-
Place large bore drains (e.g., irrigation and suction catheters) for continuous lavage, or Penrose drains. Wounds are left open.


Complications & Management
Despite optimal surgical intervention, deep space hand infections can be associated with significant complications, necessitating vigilant post-operative care and, at times, further surgical intervention.
Common Complications
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Recurrent Infection | Varies (5-15%), higher in immunocompromised patients or with incomplete debridement. | Re-exploration and drainage, repeat cultures, adjusted antibiotics, removal of any remaining foreign bodies or devitalized tissue. Consider alternative drainage techniques or more extensive debridement. |
| Stiffness / Contracture | Very common (20-40%), especially in prolonged infections or delayed treatment. | Aggressive early hand therapy, dynamic splinting, static progressive splinting, serial casting. Surgical release of contractures (e.g., capsulotomy, tenolysis) once infection is completely resolved and tissues are quiescent. |
| Tendon Adhesions / Rupture | 10-20%, higher with flexor tenosynovitis or prolonged inflammation. | Early protected motion during rehabilitation. Tenolysis (surgical release of adhesions) after infection is cleared. Tendon reconstruction (grafting or transfer) for rupture, typically in a delayed fashion. |
| Nerve Damage (Neurapraxia/Axonotmesis/Neurotmesis) | <5%, primarily from direct surgical injury or compressive edema. | Intraoperative identification and protection. Post-operative nerve gliding exercises. Nerve repair/grafting for transection, typically in a delayed manner after infection resolution. Symptomatic management for neuropathic pain. |
| Vascular Compromise | Rare, but limb-threatening (<1%). | Immediate re-exploration, release of compressive hematoma/edema, assessment of vessel patency. Microvascular repair if indicated, but often not feasible in an infected field. Amputation in extreme cases. |
| Osteomyelitis | 5-10%, higher in open fractures or prolonged untreated infections. | Prolonged targeted antibiotic therapy (often 6 weeks IV). Surgical debridement of infected bone, sometimes requiring bone resection and reconstruction. Sequestrectomy. |
| Septic Arthritis | 5-10%, if infection spreads to a joint. | Immediate surgical drainage and irrigation of the joint. Prolonged antibiotics. Joint splinting followed by protected motion. Salvage options include arthrodesis or excision arthroplasty for severe joint destruction. |
| Chronic Pain | 15-25%, multifactorial (nerve injury, stiffness, scar tissue). | Multimodal pain management, including physical therapy, neuropathic medications, judicious use of analgesics. Psychological support. Consideration of nerve blocks or neuromodulation. |
| Systemic Sepsis / MODS | Rare but life-threatening (<1%). | Aggressive resuscitation in ICU, broad-spectrum antibiotics, source control (surgical drainage). Support of organ systems. |
| Scar Contracture / Hypertrophic Scarring | Common with open wounds and secondary intention healing. | Scar massage, silicone sheeting, compression garments. Z-plasty or other reconstructive scar revision techniques in selected cases after wound maturation. |
Management Principles
- Early Recognition: Prompt identification of complications is key.
- Serial Examinations: Regular assessment of the wound, hand function, and systemic status.
- Imaging: Repeat imaging (X-rays, ultrasound, MRI) if new concerns arise.
- Multidisciplinary Approach: Collaboration with infectious disease specialists, physical/occupational therapists, and pain management teams.
- Patient Education: Inform patients about potential complications and the importance of adherence to rehabilitation protocols.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical intervention itself in achieving optimal functional outcomes and preventing long-term disability. The hand therapy regimen must be tailored to the specific infection, surgical approach, and individual patient factors, often requiring a delicate balance between protecting the healing tissues and initiating early motion.
Immediate Post-Operative Phase (Days 0-7)
- Elevation: Strict hand elevation above heart level (on pillows or in a sling) to minimize edema.
- Pain Management: Aggressive pain control to facilitate comfort and early participation in therapy.
- Wound Care: Regular wound checks. Drains are typically removed once drainage significantly diminishes (e.g., <10-20 mL/day) and the purulent discharge has resolved, usually within 2-5 days. Wounds are packed lightly with sterile gauze or moist dressings.
-
Splinting:
- Initial resting splinting in the "intrinsic plus" or "position of safety" (wrist in 20-30 degrees extension, MCPs in 70-90 degrees flexion, IPs in full extension, thumb abducted and extended) to prevent contractures and joint stiffness.
- This position maintains collateral ligament length at the MCP joints and prevents intrinsic muscle shortening.
- Antibiotics: Continue intravenous antibiotics, transitioning to oral antibiotics based on culture sensitivities and clinical improvement. The total duration of antibiotics varies but often extends for 1-4 weeks post-drainage, depending on the severity and resolution of infection.
- Early Motion (as tolerated): Gentle, protected passive range of motion (PROM) for non-involved joints. Active range of motion (AROM) for involved digits may be initiated once the acute inflammatory phase subsides and stability allows, typically under direct therapist supervision. The specific timing depends on the extent of debridement and proximity to tendons.
Intermediate Post-Operative Phase (Weeks 1-4)
-
Hand Therapy Progression:
- Active Range of Motion (AROM): Gradually increase active flexion and extension of all digits and the wrist. Focus on composite fist and full extension.
- Passive Range of Motion (PROM): Continued PROM, especially for stiff joints, performed gently to avoid tissue trauma.
- Edema Control: Continued elevation, light compression wraps (e.g., Coban), retrograde massage.
- Scar Management: Once wounds are closed or stable, begin scar massage, silicone gel sheeting, or compression garments to minimize hypertrophic scarring and contracture.
- Light Strengthening: Initiate very gentle isometric exercises or light resistance exercises as pain allows and wound integrity is assured.
- Splinting: Static progressive splinting or dynamic splinting may be introduced to address specific joint contractures.
Advanced Post-Operative Phase (Weeks 4-12+)
- Strengthening: Progressive resistive exercises for grip, pinch, and individual finger strength.
- Functional Activities: Incorporate activities of daily living (ADLs) and work-related tasks to restore functional independence.
- Endurance: Exercises to improve hand and arm endurance.
- Return to Activity: Gradually progress towards full return to normal activities, sports, or work, guided by functional assessment and patient tolerance.
- Monitoring: Continued monitoring for signs of residual infection, stiffness, or other complications.
Key Considerations for Rehabilitation
- Individualized Approach: Protocols must be tailored to the patient’s specific needs, motivation, and the unique challenges posed by their infection.
- Patient Compliance: Education and motivation are paramount for adherence to home exercise programs and splint wear.
- Communication: Close communication between the surgeon and hand therapist is essential for adjusting the protocol based on patient progress and surgical findings.
- Psychological Support: Address potential psychological impact of hand injury and prolonged recovery.
Summary of Key Literature / Guidelines
The management of deep space hand infections is guided by long-standing surgical principles and contemporary understanding of microbiology and antibiotic stewardship. While specific, universally endorsed clinical guidelines analogous to those for major joint reconstruction may not exist, consensus within the orthopedic and hand surgery community emphasizes several critical points:
- Early Diagnosis is Paramount: The literature consistently highlights that delayed diagnosis and intervention are the most significant factors contributing to poor outcomes, including permanent functional impairment and systemic complications. Clinical vigilance, particularly for subtle signs in immunocompromised patients, is crucial.
- Aggressive Surgical Debridement and Drainage: This is the cornerstone of treatment for all deep space hand infections with abscess formation. Studies reinforce the necessity of thorough debridement of necrotic tissue, copious irrigation, and ensuring adequate drainage pathways (often leaving wounds open or with drains). Inadequate drainage is a major risk factor for recurrence and prolonged morbidity.
- Targeted Antibiotic Therapy: Initial broad-spectrum empirical intravenous antibiotics, informed by local resistance patterns and patient risk factors, are critical. Prompt adjustment of the antibiotic regimen based on intraoperative Gram stain, culture, and sensitivity results is essential for effective pathogen eradication. The emergence of MRSA necessitates its consideration in initial empirical coverage.
- Importance of Hand Therapy: Early, protected, and progressive hand rehabilitation is indispensable for restoring function, preventing stiffness, and minimizing long-term sequelae. Literature supports the role of early mobilization strategies, balanced with wound healing and infection control, to optimize range of motion and functional return.
- Understanding Anatomy: A profound knowledge of hand anatomy—the fascial planes, tendon sheaths, and neurovascular bundles—is repeatedly cited as foundational for safe and effective surgical access and drainage, minimizing iatrogenic injury.
- Management of Pyogenic Flexor Tenosynovitis (PFT): PFT often coexists with or precedes deep space infections. The specific approach to PFT, involving tendon sheath irrigation and potential open debridement, is critical and directly impacts outcomes in related deep space infections (e.g., Parona's space, thenar, midpalmar).
- Multidisciplinary Care: The complexity of these infections often benefits from a collaborative approach involving hand surgeons, infectious disease specialists, and hand therapists to optimize patient care from diagnosis through rehabilitation.
While specific randomized controlled trials on surgical techniques for deep space infections are scarce due to the emergent nature and variability of presentation, the body of literature primarily consists of cohort studies, case series, and expert consensus, all converging on these established principles for successful management. Future research may focus on optimizing antibiotic regimens for emerging resistant organisms and refining rehabilitation protocols for specific infection types.
Clinical & Radiographic Imaging


You Might Also Like