Acute Triceps Tendon Ruptures: Epidemiology, Diagnosis, Surgical Anatomy & Biomechanics

Key Takeaway
A triceps tendon rupture is a significant elbow extensor injury, often presenting with a sudden 'pop,' acute pain, and a palpable defect. Common in active middle-aged males, it's diagnosed via history, physical exam (inability to extend elbow), and imaging. MRI is the gold standard, confirming diagnosis, assessing tear severity, and guiding treatment.
Introduction & Epidemiology
Acute triceps tendon ruptures, while less common than their biceps, quadriceps, or Achilles counterparts, represent a significant injury to the elbow extensor mechanism. These injuries typically manifest as a sudden "pop" followed by acute pain and functional impairment, often leaving a palpable defect superior to the olecranon. While relatively rare, accounting for approximately 1% of all major tendon ruptures, their incidence may be underreported or increasing due to greater participation in strength-training activities and contact sports, as well as an aging, active population.
Epidemiologically, triceps tendon ruptures frequently occur in active, middle-aged males, often associated with weightlifting, contact sports, or falls onto an outstretched arm. The mechanism is predominantly eccentric loading of the triceps while the elbow is in a flexed position, such as attempting to block a fall or resisting a sudden external force. Direct trauma to the posterior elbow is a less common etiology. Predisposing factors can include anabolic steroid use, chronic tendinopathy, systemic conditions (e.g., renal failure, hyperparathyroidism, rheumatoid arthritis, diabetes mellitus), local steroid injections, and specific medications (e.g., fluoroquinolones). These factors can compromise tendon vascularity and collagen integrity, rendering the tendon more susceptible to rupture.
Clinical diagnosis is primarily established through a thorough history and physical examination. Patients typically report an acute, sharp pain and a sensation of tearing or "pop" at the posterior elbow. Objective findings include swelling, ecchymosis extending distally, and a palpable defect proximal to the olecranon. The inability to actively extend the elbow against gravity or resistance, or a demonstrable extensor lag, is pathognomonic for a complete rupture. Pain with resisted extension and tenderness at the triceps insertion are also common.
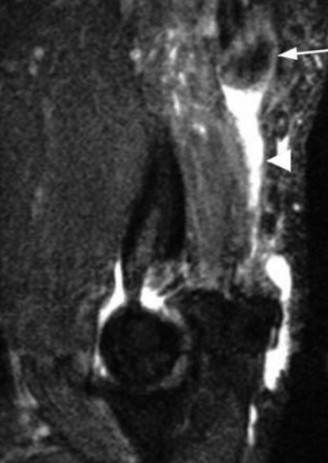
Radiographic evaluation is essential. Plain radiographs (AP, lateral, oblique views of the elbow) can reveal an avulsion fracture of the olecranon, often termed a "fleck sign," representing a bony fragment pulled off with the tendon insertion. While a negative radiograph does not exclude rupture, it helps rule out other bony injuries. Ultrasound can be a useful, dynamic, and cost-effective initial imaging modality, demonstrating tendon discontinuity and retraction, though its accuracy is operator-dependent. Magnetic resonance imaging (MRI) remains the gold standard for confirming the diagnosis, precisely localizing the rupture, quantifying the degree of retraction, differentiating between partial and complete tears, assessing tendon quality, and identifying associated soft tissue or bony pathology. Early and accurate diagnosis is critical, as delayed treatment can lead to significant tendon retraction, scar tissue formation, muscle atrophy, and increased surgical complexity, ultimately compromising functional outcomes.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the surgical anatomy and biomechanics of the triceps brachii muscle and its distal tendon is paramount for successful surgical repair. The triceps brachii is the primary extensor of the elbow and contributes significantly to shoulder stability, particularly the long head. It is composed of three distinct heads:
- Long Head: Originates from the infraglenoid tubercle of the scapula. It is the only bi-articular head, crossing both the shoulder and elbow joints, contributing to shoulder extension and adduction.
- Lateral Head: Originates from the posterior surface of the humerus, superior to the radial groove.
- Medial Head: Originates from the posterior surface of the humerus, inferior to the radial groove and intermuscular septa. This head lies deepest and is often the first to contract during elbow extension.
Distally, these three heads converge to form a robust, broad, and flattened common tendon that inserts onto the olecranon process of the ulna. The precise insertion site is crucial: the superficial fibers insert onto the posterior and superior aspects of the olecranon, while the deeper fibers blend with the periosteum and often insert more medially on the olecranon's tip. There is also a fascial expansion, the triceps aponeurosis, which extends distally over the anconeus muscle, contributing to the overall extensor mechanism. This broad insertion provides a large footprint for load distribution during extension.
The blood supply to the triceps muscle and tendon is primarily from branches of the profunda brachii artery and the ulnar collateral arteries. Venous drainage follows arterial supply. The primary innervation is via the radial nerve (C7, C8, T1), which courses intimately with the humerus in the spiral groove. Proximity of the radial nerve to the posterior aspect of the humerus necessitates meticulous surgical dissection to avoid iatrogenic injury, particularly during distal humeral exposure or when managing chronic ruptures with significant scarring. The posterior cutaneous nerve of the forearm, a branch of the radial nerve, also crosses the surgical field and is vulnerable during skin incision and subcutaneous dissection.
Biomechanically, the triceps brachii functions as a powerful elbow extensor. Its maximum moment arm for extension is typically observed at approximately 90 degrees of elbow flexion. Rupture of the triceps tendon severely compromises this extensor capability, leading to an inability to actively extend the elbow against gravity or resistance, thus impairing activities of daily living and athletic performance. The integrity of the triceps tendon is critical for pushing, lifting, and stabilizing the arm. A complete rupture results in a significant functional deficit, with patients typically unable to perform tasks requiring elbow extension, such as pushing oneself up from a chair or lifting objects overhead. Partial ruptures may present with pain and weakness but maintain some degree of active extension, depending on the percentage of torn fibers and the remaining intact fascial attachments.
Indications & Contraindications
The decision-making process for managing triceps tendon ruptures hinges on several factors, including the type and extent of rupture, patient activity level, medical comorbidities, and chronicity of the injury. While acute, complete ruptures in active individuals are typically managed operatively, a spectrum of presentations allows for non-operative considerations.
Indications for Operative Management:
- Acute Complete Ruptures: These are the most common indication. Surgical repair should ideally be performed within 2-3 weeks of injury to prevent significant tendon retraction, muscle atrophy, and scar tissue formation, which complicate primary repair.
- Acute Partial Ruptures with Significant Functional Deficit: Tears involving greater than 50% of the tendon's cross-sectional area, particularly if associated with a demonstrable extensor lag or significant weakness on resisted extension despite non-operative management.
- Avulsion Fractures of the Olecranon: If the bony fragment is displaced and compromises the extensor mechanism, or if it represents a significant portion of the triceps insertion.
- Chronic Ruptures: While more challenging, surgical intervention may still be indicated for chronic ruptures (typically >3-4 weeks post-injury) in symptomatic, active individuals to restore function, though these often require augmentation.
- Active, High-Demand Individuals: Patients whose profession or recreational activities demand full, robust elbow extension.
Indications for Non-Operative Management:
- Acute Partial Ruptures with Intact Extensor Mechanism: Tears involving less than 50% of the tendon's cross-sectional area, with minimal or no extensor lag, and satisfactory strength on resisted extension.
- Medically Unfit Patients: Individuals with significant medical comorbidities that preclude safe surgical intervention and anesthesia.
- Low-Demand, Sedentary Patients: Elderly patients or those with very low functional requirements who can tolerate some degree of extensor weakness.
- Patients Refusing Surgery: After comprehensive counseling on the risks and benefits of both operative and non-operative approaches.
Contraindications for Operative Management:
-
Absolute Contraindications:
- Active local or systemic infection.
- Uncontrolled severe medical comorbidities precluding anesthesia or surgical stress.
-
Relative Contraindications:
- Poor skin quality or compromised soft tissue envelope over the posterior elbow.
- Active substance abuse or non-compliance with post-operative protocols.
- Significant chronic psychiatric illness affecting rehabilitation compliance.
The following table summarizes the indications:
| Indication Category | Operative Management
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical to anticipating potential intraoperative challenges and ensuring optimal patient outcomes. This begins with a thorough review of the patient's medical history, including comorbidities, medications, and previous surgical history. A comprehensive physical examination should confirm the diagnosis and rule out concurrent injuries or neurological deficits. Particular attention should be paid to the skin and soft tissue envelope over the posterior elbow, documenting any signs of infection, atrophy, or poor vascularity.
Imaging studies, especially MRI, are indispensable. The MRI confirms the extent of the rupture (partial vs. complete), the degree of tendon retraction, the quality of the remaining tendon tissue, and the presence of any associated bony avulsions. It also helps identify any chronic changes such as tendinosis or muscle atrophy that might influence the repair strategy. For chronic ruptures, the MRI can assess the amount of tendon gap and muscle scarring, which often dictates the need for augmentation.
Prior to surgery, appropriate prophylactic antibiotics should be administered. The choice of anesthesia can vary, with general anesthesia being most common, often supplemented with a regional block (e.g., interscalene or supraclavicular block) to aid in post-operative pain control.
Patient positioning is critical for optimal surgical exposure and to allow for appropriate intraoperative manipulation of the elbow. The two most common positions are prone and lateral decubitus.
-
Prone Position:
- Advantages: Provides excellent posterior access to the elbow, allowing the arm to be fully free-draped. This facilitates the ability to flex and extend the elbow through a full arc of motion, which is crucial for tensioning the repair and assessing joint stability. The unaffected arm is typically tucked at the side.
-
Setup:
The patient is placed prone on the operating table. Care must be taken to pad all pressure points to prevent nerve injury (e.g., ulnar nerve at the elbow, peroneal nerve at the fibular head). The head should be supported and protected. The ipsilateral arm is allowed to hang free off the side of the table or is supported by a padded arm board, allowing full range of motion of the shoulder and elbow. A tourniquet is applied to the upper arm. The entire arm, from shoulder to fingertips, is prepped and draped to allow sterile manipulation.
- Considerations: Requires careful patient turning and positioning. Ventilation may be slightly more challenging than supine, but generally well-tolerated.
-
Lateral Decubitus Position:
- Advantages: Also provides excellent posterior access to the elbow. It can be more comfortable for some patients and may be preferred if there are concerns with prone ventilation. Similar to prone, the arm can be free-draped for full range of motion.
- Setup: The patient is positioned on their side, with the affected arm superior. Axillary roll should be placed to protect the neurovascular structures of the dependent arm. The affected arm is typically supported on a padded arm rest or overhead table, allowing for controlled manipulation. A tourniquet is applied to the upper arm.
- Considerations: Requires careful padding of the dependent side.
Regardless of the position chosen, careful attention to padding, nerve protection, and secure limb positioning is paramount to prevent iatrogenic injury. The application of a pneumatic tourniquet to the upper arm is standard practice to provide a bloodless field, which significantly aids in visualization and identification of delicate structures. The sterile field should be generous, encompassing the entire arm from the shoulder to the hand, to allow for intraoperative manipulation and access to potential graft harvest sites if augmentation is anticipated.
Detailed Surgical Approach / Technique
The goal of surgical repair is to restore the integrity of the triceps extensor mechanism, allowing for pain-free, full range of motion and strength. The approach typically involves a direct posterior incision.
Surgical Incision and Initial Dissection:
- Incision: A straight posterior longitudinal incision centered over the olecranon is preferred. The incision typically extends from approximately 5 cm proximal to the olecranon to 3-4 cm distal to it. For chronic repairs or those requiring augmentation, the incision may need to be longer. Care is taken to design the incision to avoid placing it directly over the ulnar nerve, though the nerve itself is not routinely exposed unless a concomitant pathology exists or if nerve transposition is planned for other reasons.
- Subcutaneous Dissection: Sharp dissection through the subcutaneous fat is performed. It is crucial to identify and protect the branches of the posterior cutaneous nerve of the forearm, which can be vulnerable to injury in this plane. These nerves course superficially and can be gently retracted to prevent neuropraxia or painful neuromas.
- Fascial Layer: The deep fascia overlying the triceps muscle is incised longitudinally. This exposes the underlying muscle belly and the retracted proximal tendon stump.
Identification and Preparation of Tendon Ends:
- Proximal Tendon Stump: The ruptured proximal end of the triceps tendon is identified. It is often retracted proximally, sometimes several centimeters. The edges of the tendon are typically frayed and thickened due to inflammatory response and scar tissue. The tendon end should be debrided back to healthy, robust tissue using a scalpel or scissors. Careful identification of the individual heads of the triceps can sometimes be made, but often a conjoined tendon is encountered.
- Distal Insertion Site (Olecranon): The distal aspect of the rupture involves the avulsed tendon from its insertion on the olecranon. Any remaining frayed tendon fibers or granulation tissue on the olecranon should be meticulously debrided to expose fresh, bleeding bone. A burr or osteotome can be used to lightly decorticate the olecranon's posterior facet, creating a raw bony bed for tendon reattachment, promoting tendon-to-bone healing. A small trough or gutters can also be fashioned if a transosseous technique is planned.
Repair Techniques:
The choice of repair technique depends on the quality of the tendon tissue, the degree of retraction, and surgeon preference.
A. Primary Repair (Acute Ruptures with Good Tissue Quality):
-
Transosseous Suture Repair (e.g., Krackow or Bunnell Stitch):
- This is a classic and reliable technique, particularly for acute ruptures with good tissue quality.
- Two or three non-absorbable, braided sutures (e.g., #5 Ethibond or FiberWire) are woven into the proximal triceps tendon in a locking stitch pattern (e.g., Krackow or Bunnell stitch). This provides a secure grip on the tendon fibers.
- Three convergent drill holes are created through the olecranon, exiting on its anterior cortex, typically just distal to the articular cartilage. These holes are usually 2.5 mm in diameter, spaced approximately 5-7 mm apart, forming a triangle. The drill holes should be angled slightly distally and anteriorly.
- Suture passers or long needles are used to retrieve the sutures through the drill holes. Each suture limb is passed through a separate hole.
- The elbow is then gently brought into 20-30 degrees of flexion, which is the position of maximal tension for the triceps. The sutures are then tensioned and tied securely over the anterior cortex of the ulna, often over a cortical bone bridge or through a button to prevent suture pull-through. This creates a strong compression of the tendon stump onto the prepared olecranon bed.
- The repair tension is checked by passively extending the elbow. It should be firm but allow for some flexion.
-
Suture Anchor Repair:
- Increasingly popular due to excellent fixation strength and less invasive bone preparation.
- Two to four non-absorbable suture anchors (e.g., 5.0-6.5 mm fully threaded or cannulated PEEK/titanium anchors) are placed into the prepared posterior olecranon. The number of anchors depends on the size of the footprint and the surgeon's preference. They are typically placed in a row just proximal to the insertion site.
- Each anchor has two or more limbs of high-strength suture. These sutures are then individually passed through the proximal triceps tendon using a suture passer in a locking or mattress fashion.
- The sutures are then tied, securing the tendon to the olecranon. Similar to transosseous repair, the elbow is typically positioned in 20-30 degrees of flexion during knot tying to achieve appropriate tension.
- This technique minimizes the need for extensive dissection on the anterior aspect of the ulna and is often quicker.
B. Augmentation (Chronic Ruptures, Poor Tissue Quality, or Re-ruptures):
When the tendon stump is severely retracted, atrophied, or of poor quality, primary repair alone may be insufficient. Augmentation with a graft becomes necessary.
-
Autograft Options:
- Semitendinosus/Gracilis: Harvested from the ipsilateral or contralateral thigh. Provides robust, long, and strong tissue. Requires a separate incision.
- Palmaris Longus: If present, can be used for smaller defects.
- Achilles Tendon Allograft: A common and excellent choice, especially if a large defect or poor host tissue is present. The calcaneal bone plug can be used to anchor one end into the olecranon, while the tendon body is woven into the host triceps.
- Fascia Lata: Harvested from the lateral thigh. Can be folded and woven into the repair.
-
Allograft Options:
- Achilles Tendon Allograft: Most commonly used. Can bridge large gaps and provide substantial strength. The bone block can be secured into the olecranon with screws or anchors, and the tendon body woven into the retracted triceps stump.
- Tibialis Anterior Allograft: Another viable option for augmentation.
-
Augmentation Technique:
- The chosen graft is prepared. If an Achilles tendon allograft with a bone plug is used, the bone plug is typically secured into a trough fashioned in the olecranon using cancellous screws or suture anchors. The tendinous portion is then woven into the proximal triceps stump using multiple locking sutures.
- If a free tendon graft (e.g., semitendinosus) is used, it can be passed through drill tunnels in the olecranon and then woven into the triceps tendon in a "pulvertaft" fashion, or secured with suture anchors to both the olecranon and the triceps stump.
- The goal is to create a strong composite repair that can withstand early rehabilitation stresses.
Closure:
- Repair Assessment: After the repair is complete, the tourniquet is deflated. Hemostasis is achieved. The elbow is gently brought through a range of motion to assess the stability and tension of the repair. There should be no gapping, and full extension should be achievable without undue stress on the repair.
- Layered Closure: The deep fascia is approximated if possible without tension. The subcutaneous tissues are closed with absorbable sutures. The skin is closed with staples or non-absorbable sutures.
- Post-Operative Dressing: A sterile dressing is applied, and the arm is typically placed in a hinged elbow brace or a posterior splint, often set at 30-45 degrees of flexion.
Throughout the procedure, constant vigilance for the radial nerve and its branches is maintained. The internervous plane for a posterior approach to the elbow is essentially absent as the triceps muscle is directly accessed. The key to preventing iatrogenic nerve injury is meticulous soft tissue handling, careful retraction, and a precise understanding of the anatomy, especially during dissection near the humerus.

Complications & Management
Despite careful surgical technique and adherence to rehabilitation protocols, triceps tendon repair is not without potential complications. Understanding these risks and having strategies for their management is crucial for academic orthopedic surgeons.
Common Complications:
-
Re-rupture:
- Incidence: Relatively low, generally reported between 2% and 5%. Higher in chronic repairs, those with poor tissue quality, or non-compliant patients.
- Causes: Inadequate initial repair, premature or aggressive rehabilitation, poor tendon quality, underlying systemic comorbidities, or new trauma.
- Management: Diagnosed similarly to the primary rupture. Requires revision surgery, often with augmentation using autograft (e.g., semitendinosus, quadriceps tendon) or allograft (e.g., Achilles tendon with bone block). The revision procedure is typically more complex due to scar tissue and further tendon retraction.
-
Elbow Stiffness / Loss of Range of Motion (ROM):
- Incidence: Can be significant, ranging from 10% to 20%, especially with prolonged immobilization or inadequate rehabilitation. Loss of terminal extension is more common than flexion loss.
- Causes: Post-operative scarring, capsular contracture, heterotopic ossification, prolonged immobilization, or patient non-compliance with therapy.
- Management: Aggressive post-operative physical therapy focusing on early controlled motion. Dynamic splinting may be beneficial. For established stiffness, manipulation under anesthesia (MUA) or open/arthroscopic capsular release may be necessary. Prophylaxis for heterotopic ossification (NSAIDs or radiation therapy) should be considered, particularly in high-risk patients.
-
Neurological Injury:
- Incidence: Radial nerve injury is the most concerning, although rare (1-3%). More common is injury to the posterior cutaneous nerve of the forearm, a sensory branch of the radial nerve.
- Causes: Direct laceration, stretch injury from retraction, or compression during surgery. The radial nerve is at risk if dissection extends too far laterally or distally along the humerus.
-
Management:
- Posterior Cutaneous Nerve: Sensory deficits are typically tolerated. Neuromas can be treated with local injections, surgical excision, or nerve capping.
- Radial Nerve: Immediate post-operative palsy requires careful assessment. Observation is often warranted for neuropraxia. EMG/NCS studies can assess severity and guide prognosis. If no recovery is observed within 3-6 months, neurolysis or, in rare cases of transection, nerve grafting may be indicated.
-
Infection:
- Incidence: Low, typically 1-5%, similar to other clean orthopedic procedures.
- Causes: Breach in sterile technique, prolonged surgical time, or compromised host immunity.
- Management: Superficial infections often respond to oral antibiotics and local wound care. Deep infections require surgical debridement, intravenous antibiotics, and potentially implant removal (if applicable and infection persists). For prosthetic augmentation, managing infection can be particularly challenging.
-
Persistent Weakness / Fatigue:
- Incidence: 5-10%. Some degree of residual weakness or fatigability may persist despite a successful anatomical repair.
- Causes: Muscle atrophy pre-operatively, incomplete recovery of muscle strength, scar tissue within the muscle belly, or residual tendon laxity.
- Management: Continued and progressive strengthening rehabilitation. Re-evaluation of repair integrity via imaging. In cases of significant persistent weakness due to mechanical failure, revision surgery or augmentation may be considered.
-
Heterotopic Ossification (HO):
- Incidence: Variable, reported from 5% to 15%. Risk factors include severe trauma, previous elbow surgery, or prolonged immobilization.
- Causes: Uncontrolled inflammatory response leading to abnormal bone formation in soft tissues around the joint.
- Management: Prophylaxis with non-steroidal anti-inflammatory drugs (NSAIDs) like indomethacin for 3-6 weeks post-operatively, or a single dose of post-operative radiation therapy, especially in high-risk patients. If symptomatic HO limits ROM, surgical excision may be required once the HO has matured (typically 6-12 months post-onset).
-
Hardware-Related Complications:
- Incidence: 5-10%, particularly with transosseous repairs where sutures are tied over a button or bone bridge, or with suture anchors.
- Causes: Suture pull-through, anchor failure, prominent or irritating knots, or irritation from bone buttons.
- Management: Symptomatic hardware may require removal once the tendon healing is considered robust (typically 6-12 months post-op). Revision fixation may be necessary for anchor failure or suture pull-through if the repair is compromised.
The following table summarizes common complications and their management:
| Complication | Incidence (Approx.) | Salvage Strategies ## Introduction & Epidemiology
Triceps tendon ruptures, while less frequently encountered than quadriceps or biceps ruptures, represent a critical injury to the elbow extensor mechanism. These injuries are characterized by the sudden onset of posterior elbow pain, often accompanied by an audible "pop," swelling, ecchymosis, and significant functional impairment. The annual incidence is challenging to ascertain precisely due to its rarity and potential for misdiagnosis, but a general estimation places it at approximately 0.8% of all major tendon ruptures. However, with increasing participation in strength-training, power sports, and an aging yet active population, anecdotal evidence suggests a possible rise in prevalence.
The typical demographic affected includes active individuals, predominantly males, within the fourth to sixth decades of life. Etiologically, the injury mechanism is most commonly an eccentric contraction of the triceps against a sudden forceful flexion of the elbow, such as occurs during a fall onto an outstretched arm, resisting a heavy load, or in collision sports. Direct trauma to the posterior aspect of the elbow is a less frequent cause. Predisposing factors significantly contribute to tendon vulnerability and include chronic tendinopathy, systemic conditions like chronic renal failure, hyperparathyroidism, rheumatoid arthritis, gout, and diabetes mellitus. Iatrogenic factors such as local corticosteroid injections into the tendon and certain systemic medications, notably fluoroquinolones, also weaken tendon integrity. Prior anabolic steroid use has also been correlated with an increased risk of triceps tendon rupture due to its effects on collagen synthesis and tendon structure.
Clinical presentation is usually acute and distinct. Patients typically report immediate pain and inability to extend the elbow against resistance. On physical examination, localized tenderness, swelling, and ecchymosis over the posterior aspect of the elbow are consistently observed. The hallmark finding in complete ruptures is a palpable defect or "divot" just proximal to the olecranon process. An extensor lag, characterized by the inability to actively extend the elbow to full terminal extension, or an inability to maintain passive full extension against gravity, is a strong indicator of a complete tear compromising the extensor mechanism.
Diagnostic imaging commences with plain radiographs (AP, lateral, and oblique views of the elbow), primarily to rule out associated bony injuries and to identify an avulsion fracture of the olecranon, often visible as a small bony fragment retracted proximally, known as the "fleck sign." A negative radiograph does not exclude a significant soft tissue injury. Ultrasonography can serve as a useful adjunct, offering a dynamic and non-invasive assessment of tendon continuity and retraction, though its diagnostic accuracy is highly operator-dependent. Magnetic resonance imaging (MRI) is considered the gold standard for definitive diagnosis, providing detailed visualization of the tendon architecture, precisely localizing the rupture site, quantifying the degree of tendon retraction, differentiating between partial and complete tears, assessing the quality of the remaining tendon and muscle tissue, and identifying any concomitant intra-articular or periarticular pathology. Timely and accurate diagnosis is paramount, as delayed surgical intervention (>3-4 weeks) can lead to substantial tendon retraction, muscle contracture and atrophy, formation of dense scar tissue, and increased surgical complexity, often necessitating augmentation and potentially compromising long-term functional outcomes.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the triceps brachii complex is indispensable for the successful management of its distal tendon ruptures. The triceps brachii, the largest muscle in the posterior compartment of the arm, is the primary and most powerful extensor of the elbow. Its intricate structure comprises three distinct heads, each originating from a different site and converging into a common distal tendon:
- Long Head (Caput Longum): Originates from the infraglenoid tubercle of the scapula and the adjacent glenoid labrum. As the only bi-articular head, it crosses both the glenohumeral and elbow joints, contributing to shoulder adduction and extension, in addition to elbow extension.
- Lateral Head (Caput Laterale): Arises from the posterior surface of the humerus, superior to the radial groove and the lateral intermuscular septum.
- Medial Head (Caput Mediale): Originates from the posterior surface of the humerus, inferior to the radial groove and the medial and lateral intermuscular septa. This head is typically deepest and lies directly on the periosteum of the humerus, forming a significant portion of the muscle belly.
Distally, these three heads coalesce into a robust, broad, and somewhat flattened common triceps tendon. This tendon has a complex, multi-layered insertion onto the olecranon process of the ulna. The superficial fibers predominantly insert onto the posterior and superior aspects of the olecranon, while deeper fibers may directly blend with the periosteum and insert more medially on the olecranon tip. A significant anatomical component is the broad aponeurotic expansion that extends distally over the anconeus muscle and contributes to the overall stability of the posterior elbow capsule and extensor mechanism. The average length of the tendinous portion is approximately 7-8 cm, with an insertion footprint typically 2.5-3 cm wide and 1.5-2 cm long.
The vascular supply to the triceps muscle is derived primarily from the profunda brachii artery (deep brachial artery) and its branches, as well as the superior and inferior ulnar collateral arteries. Venous drainage parallels arterial distribution. The innervation for all three heads of the triceps brachii is provided by the radial nerve (C7, C8, T1), which courses in the spiral groove of the humerus. During its course, the radial nerve is in close proximity to the posterior humeral shaft and the lateral intermuscular septum, making it vulnerable during surgical dissection, particularly when extensive exposure of the distal humerus is required or in cases of chronic ruptures with extensive scarring. A critical sensory nerve, the posterior cutaneous nerve of the forearm, a branch of the radial nerve, also crosses the posterior aspect of the elbow superficially, traversing the subcutaneous tissue, and is highly susceptible to iatrogenic injury during skin incision and superficial dissection.
From a biomechanical perspective, the triceps brachii acts as the principal antagonist to the biceps and brachialis muscles. Its primary action is elbow extension, generating maximal torque typically between 75 and 90 degrees of elbow flexion. This powerful extensor capacity is essential for myriad activities, including pushing, lifting, throwing, and maintaining upper extremity posture. The long head's bi-articular nature means it can also influence shoulder stability and motion, although its primary contribution is to elbow extension. A complete triceps tendon rupture fundamentally compromises the extensor mechanism, resulting in a profound functional deficit. Patients experience an inability to perform active elbow extension against gravity or resistance, significantly impairing activities of daily living that require pushing or stabilizing the arm. The integrity of the triceps tendon is indispensable for the effective transfer of force from the shoulder girdle through the arm to the forearm and hand. Partial ruptures, depending on their size and location, may result in varying degrees of weakness and pain but may retain some extensor function if sufficient intact fibers or fascial attachments remain.
Indications & Contraindications
The decision to proceed with operative versus non-operative management for triceps tendon ruptures is multi-factorial, requiring careful consideration of the injury pattern, patient demographics, functional demands, and medical comorbidities. While surgical repair is generally favored for most complete ruptures, there are specific scenarios where conservative treatment may be appropriate.
Indications for Operative Management
- Acute Complete Ruptures: The strongest indication for surgical intervention. This includes both pure tendon ruptures and avulsion fractures of the olecranon where the fragment significantly compromises the extensor mechanism. Surgical repair should ideally be performed within 2-3 weeks of injury. Early intervention is critical to facilitate primary repair due to less tendon retraction, better tissue quality, and reduced scar formation.
- Acute Partial Ruptures with Significant Functional Deficit: When conservative management fails or if the tear involves greater than 50% of the tendon's cross-sectional area, particularly in conjunction with an extensor lag or significant weakness on resisted extension.
- Chronic Ruptures (typically >3-4 weeks post-injury): While more technically demanding due to tendon retraction, muscle atrophy, and scarring, surgery is still indicated for symptomatic, active individuals to restore functional strength and ROM. These cases often necessitate augmentation.
- Avulsion Fractures of the Olecranon: If the bony fragment is displaced, comminuted, or causes mechanical blockage/instability of the elbow, or if it represents a significant portion of the triceps insertion.
- High-Demand Individuals: Athletes or patients whose occupation requires robust elbow extension and strength, irrespective of the chronicity of the injury (though acute repair is preferred).
Indications for Non-Operative Management
- Acute Partial Ruptures with Intact Extensor Mechanism: Tears involving less than 50% of the tendon's cross-sectional area, with minimal or no extensor lag, and satisfactory strength on resisted extension. These are typically managed with a period of immobilization followed by progressive rehabilitation.
- Elderly, Low-Demand, or Sedentary Patients: Individuals with minimal functional requirements who can tolerate some degree of extensor weakness and who may be at higher risk for surgical complications.
- Patients with Significant Medical Comorbidities: Those with uncontrolled systemic diseases (e.g., severe cardiovascular disease, poorly controlled diabetes) that pose an unacceptably high anesthetic or surgical risk.
- Patients Refusing Surgery: After comprehensive discussion of the risks, benefits, and potential functional limitations associated with non-operative treatment.
Contraindications for Operative Management
-
Absolute Contraindications:
- Active Local or Systemic Infection: Surgical repair in the presence of infection significantly increases the risk of implant-related infection and complications.
- Uncontrolled Severe Medical Comorbidities: Patients whose underlying health status makes them unfit for general anesthesia or the physiological stress of surgery.
-
Relative Contraindications:
- Compromised Soft Tissue Envelope: Poor skin quality, previous radiation, or severe scarring over the posterior elbow that may impede wound healing.
- Severe Osteoporosis: May compromise suture anchor fixation or transosseous suture pull-through.
- Patient Non-Compliance: Unreliable patients or those with active substance abuse issues who are unlikely to adhere to strict post-operative rehabilitation protocols.
- Undiagnosed or Unaddressed Neuropathies: Pre-existing radial nerve palsy affecting triceps function should be thoroughly investigated.
The following table summarizes the indications for operative versus non-operative management:
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Complete Rupture |
Acute: Primary repair (suture anchors, transosseous)
Chronic: Augmentation often required |
Generally contraindicated due to profound functional deficit and poor outcomes without repair |
| Partial Rupture | >50% tear, significant weakness/extensor lag, symptomatic, failed conservative management | <50% tear, intact extensor mechanism, minimal functional deficit, low-demand patients, medically unfit patients |
| Avulsion Fracture | Displaced fragment, fragment affecting extensor function, mechanical impingement | Non-displaced, stable, asymptomatic, minimal functional impact |
| Timing of Injury | Acute (ideally within 2-3 weeks post-injury) | Delayed presentation with minimal symptoms in select patients |
| Patient Factors | Active, high-demand individuals, good tissue quality, cooperative with rehab | Sedentary, low-demand individuals, significant medical comorbidities, poor tissue quality (may necessitate augmentation) |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is indispensable for anticipating potential intraoperative challenges, minimizing complications, and optimizing surgical outcomes. This phase begins well before the patient enters the operating room.
Pre-Operative Assessment:
-
Clinical Review:
- Detailed History: Including mechanism of injury, exact time of injury, prior elbow injuries, systemic comorbidities (e.g., diabetes, renal failure, rheumatoid arthritis, steroid use), and current medications (especially anticoagulants, steroids, fluoroquinolones).
- Physical Examination: Reconfirmation of the palpable defect, extensor lag, and assessment of distal neurovascular status. Documenting the range of motion (passive and active) and strength of other surrounding joints is crucial.
-
Imaging Review:
- Plain Radiographs: Re-evaluate AP, lateral, and oblique views for olecranon avulsion fractures or other bony pathology.
- MRI: Crucial for confirming diagnosis, delineating the extent of rupture (partial vs. complete), quantifying tendon retraction, assessing tendon quality, and identifying concomitant pathology (e.g., olecranon bursitis, concomitant ligamentous injury). For chronic ruptures, MRI helps gauge the gap length and degree of muscle atrophy, guiding the decision for augmentation.
-
Pre-operative Discussions:
- Informed Consent: Detailed discussion with the patient regarding the procedure, potential risks (re-rupture, infection, stiffness, nerve injury, persistent weakness), expected recovery course, and alternative treatments.
- Rehabilitation Protocol: Outline the general post-operative rehabilitation plan to the patient, setting realistic expectations for recovery.
- Anesthesia Consultation: Discussion with the anesthesiologist regarding patient comorbidities and optimal anesthetic plan (general anesthesia often combined with a regional nerve block, such as an interscalene or supraclavicular block, for post-operative pain management).
- Tourniquet Considerations: Standard pneumatic tourniquet application to the upper arm is planned to ensure a bloodless field, which significantly aids visualization.
Patient Positioning:
The choice of patient position is dictated by surgeon preference and facilitates optimal exposure, access to potential graft harvest sites, and intraoperative manipulation of the elbow. The two most commonly utilized positions are prone and lateral decubitus.
-
Prone Position:
- Setup: The patient is placed face-down on the operating table. All bony prominences (e.g., iliac crests, knees, feet, anterior shoulders) are meticulously padded to prevent pressure sores or nerve palsies. The head is supported in a neutral position with appropriate padding. The ipsilateral arm (operative arm) is typically free-draped, hanging off the side of the table or positioned on a specialized arm support, allowing unrestricted manipulation and full range of motion of the elbow and shoulder throughout the procedure. The contralateral arm is tucked at the patient's side, well-padded. A tourniquet is applied to the proximal aspect of the operative arm.
- Advantages: Provides excellent, unobstructed posterior access to the elbow. Allows for full visualization of the triceps muscle and tendon. Facilitates intraoperative assessment of repair tension through elbow flexion and extension.
-
Disadvantages:
Requires careful patient turning. May present challenges for airway management or for patients with specific cardiac or respiratory comorbidities.
-
Lateral Decubitus Position:
- Setup: The patient is positioned on their side, with the affected arm superior. An axillary roll is placed in the dependent axilla to protect neurovascular structures. The head is supported in neutral alignment. The affected arm is then supported on a padded arm board or Mayo stand, allowing for controlled positioning and movement of the elbow. The contralateral arm is positioned comfortably, typically across the patient's chest. A tourniquet is applied to the proximal aspect of the operative arm.
- Advantages: Offers good posterior access to the elbow, similar to the prone position. Potentially easier for airway management than prone for certain patients.
- Disadvantages: Requires meticulous padding of all dependent areas. The arm may be slightly less mobile than in the prone free-draped position.
Regardless of the chosen position, a wide sterile surgical field, extending from the shoulder to the hand, is crucial. This allows for elbow manipulation, access to potential autograft harvest sites (e.g., hamstring from the ipsilateral thigh), and management of unforeseen intraoperative events. Adequate lighting and clear visualization, often aided by loupe magnification, are essential.
Detailed Surgical Approach / Technique
The primary objective of surgical repair is the secure reattachment of the triceps tendon to its anatomical insertion on the olecranon, aiming to restore the robust extensor mechanism of the elbow. The approach is consistently posterior, focusing on minimizing soft tissue disruption while ensuring adequate exposure.
1. Surgical Incision and Initial Dissection:
- Skin Incision: A posterior longitudinal skin incision is made, centered directly over the olecranon. The incision typically extends approximately 6-8 cm proximal to the olecranon and 3-4 cm distal to its tip. For chronic ruptures or cases requiring extensive augmentation, a longer incision may be necessary. The incision can be slightly curved, with the concavity facing medially, to avoid scar contracture over the olecranon tip and to better protect the ulnar nerve region if it requires identification.
- Subcutaneous Dissection: Careful subcutaneous dissection is performed to elevate skin flaps. It is imperative to identify and protect branches of the posterior cutaneous nerve of the forearm, which arises from the radial nerve and courses superficially in this plane. These sensory nerves can be gently retracted with skin flaps to prevent iatrogenic injury, which could lead to dysesthesia or painful neuromas.
- Deep Fascia: The deep fascia overlying the triceps muscle is then incised longitudinally in line with the skin incision. This exposes the underlying muscle belly and the retracted proximal tendon stump.
2. Identification and Preparation of Tendon Ends:
- Proximal Triceps Tendon Stump: The retracted proximal end of the triceps tendon is located. In acute ruptures, it may be found just proximal to the olecranon. In chronic cases, it can be significantly retracted, sometimes several centimeters proximally, and may be encased in scar tissue. The frayed, devitalized, or scarred edges of the tendon should be sharply debrided back to healthy, robust, bleeding tissue. The three distinct heads of the triceps (long, lateral, and medial) coalesce here, often presenting as a conjoined tendinous structure.
- Olecranon Insertion Site: The distal aspect of the rupture involves the avulsed tendon from its insertion on the olecranon. Any remaining frayed tendon remnants, granulation tissue, or periosteum on the posterior olecranon should be meticulously debrided. A high-speed burr or osteotome is used to lightly decorticate the posterior and superior aspects of the olecranon, creating a fresh, bleeding bony bed. This decortication promotes robust tendon-to-bone healing and prepares the cancellous bone for suture anchor fixation or transosseous tunnel creation. A small transverse trough or gutters can also be fashioned across the olecranon if a transosseous suture technique is planned.
3. Repair Techniques:
The choice of repair technique is guided by the chronicity of the injury, the quality of the tendon tissue, the degree of retraction, and surgeon preference.
A. Primary Repair (Acute Ruptures with Good Tissue Quality):
-
Transosseous Suture Repair:
- This traditional and highly effective technique provides strong fixation.
- Two or three non-absorbable, high-strength braided sutures (e.g., #5 Ethibond, FiberWire) are woven into the proximal triceps tendon stump. A locking stitch pattern, such as the Krackow or Bunnell stitch, is utilized to maximize tendon purchase and minimize suture pull-through. Three to four passes are typically made through the tendon substance.
- Three convergent drill holes (typically 2.5 mm in diameter) are created through the olecranon. These holes originate on the posterior aspect of the prepared olecranon bed and exit on the anterior cortex of the ulna, distal to the articular cartilage. They are usually spaced 5-7 mm apart in a triangular or linear fashion.
- Each limb of the sutures is then passed individually through a separate drill hole using a specialized suture passer or long hypodermic needles.
- The elbow is gently brought into approximately 20-30 degrees of flexion, which places the triceps tendon in a physiologically appropriate position of tension. The sutures are then tensioned securely and tied over the anterior cortex of the ulna, often over a cortical bone bridge, a small bone button, or via mini-plate/screw construct to prevent suture cut-through or pressure necrosis of the bone. Knot tying is performed under appropriate tension, ensuring the tendon stump is firmly approximated to the decorticated olecranon.
-
Suture Anchor Repair:
- This technique is increasingly favored due to its strong, reproducible fixation and reduced need for extensive anterior ulnar dissection.
- Two to four non-absorbable suture anchors (e.g., 5.0-6.5 mm fully threaded or cannulated PEEK/titanium anchors) are implanted into the prepared posterior olecranon. They are typically placed in a straight line or slight curve, just proximal to the anatomical insertion footprint. The exact number and size depend on the size of the olecranon and the surgeon's preference.
- Each anchor has two or more limbs of high-strength suture. These sutures are then individually passed through the proximal triceps tendon stump using a suture passer. Various techniques can be employed, including simple sutures, mattress sutures, or locking stitches, to maximize tendon purchase. The goal is to create a broad area of compression of the tendon onto the bone.
- The sutures are then tied, securing the tendon to the olecranon. As with transosseous repair, the elbow is held in 20-30 degrees of flexion during knot tying to achieve optimal tension.
- This technique offers excellent pull-out strength and is technically less demanding for bone tunnel creation.
B. Augmentation (Chronic Ruptures, Poor Tissue Quality, or Re-ruptures):
When the triceps tendon stump is significantly retracted, atrophied, of poor quality, or in cases of re-rupture, primary repair alone is often insufficient. Augmentation with a graft is typically required.
-
Autograft Options:
- Ipsilateral Hamstring Tendons (Semitendinosus and/or Gracilis): A common choice due to sufficient length and strength. Requires a separate small incision in the medial thigh.
- Palmaris Longus Tendon: If present, can be used for smaller defects, but often insufficient for large gaps.
- Achilles Tendon Autograft: Can provide a substantial, robust graft with a bone block.
- Fascia Lata Autograft: Harvested from the lateral thigh. Can be folded and woven into the repair for reinforcement.
-
Allograft Options:
- Achilles Tendon Allograft: This is frequently used, particularly for chronic ruptures with large gaps or severely compromised host tissue. The calcaneal bone plug is ideal for fixation into the olecranon.
- Tibialis Anterior Allograft: Another viable allograft option, offering good length and strength.
-
Augmentation Technique (Example using Achilles Allograft with Bone Block):
- A trough or bone slot is created in the prepared olecranon to precisely match the size of the Achilles bone plug.
- The bone plug is then securely fixed into this trough using one or two cancellous screws or a heavy suture anchor system, ensuring solid bone-to-bone fixation.
- The tendinous portion of the Achilles allograft is then woven into the retracted proximal triceps tendon stump using multiple locking stitches (e.g., Pulvertaft weave), thereby bridging the gap and reinforcing the repair. Multiple non-absorbable sutures are used to secure the graft to the host tendon.
- The repair is tensioned with the elbow in 20-30 degrees of flexion.
- Other augmentation techniques involve passing free tendon grafts (e.g., hamstring) through drill tunnels in the olecranon and then weaving them into the triceps stump, creating a strong tension band effect.
4. Intraoperative Assessment and Closure:
- Repair Stability: After the repair is complete and the tourniquet deflated (achieving meticulous hemostasis), the elbow is gently brought through a controlled range of motion (typically from 20-30 degrees to 90 degrees of flexion). The repair should feel robust, with no gapping or excessive tension. The ability to achieve full extension passively without undue stress on the repair is confirmed.
- Layered Closure: The deep fascia is approximated with absorbable sutures, if possible, without placing tension on the repair. The subcutaneous tissues are closed with absorbable sutures. The skin is closed with staples or non-absorbable sutures, ensuring careful eversion of skin edges.
-
Post-Operative Dressing and Immobilization:
A sterile dressing is applied. The arm is then typically placed in a hinged elbow brace or a posterior splint, initially locked in approximately 30-45 degrees of flexion to protect the repair while allowing for some elbow joint "relaxation."
Throughout the entire procedure, continuous vigilance for the radial nerve and its cutaneous branches is paramount. Careful, sharp dissection, avoiding excessive blunt retraction, and maintaining a clear understanding of the anatomy are critical to minimizing iatrogenic nerve injury.
Complications & Management
Despite meticulous surgical technique and comprehensive post-operative care, triceps tendon repair can be associated with a range of complications. Awareness of these potential issues, their incidence, and effective salvage strategies is crucial for all orthopedic surgeons.
Specific Complications of Triceps Tendon Repair:
-
Re-rupture:
- Incidence: Ranges from 2% to 5%, but can be higher in chronic cases, repairs with poor tissue quality, or in non-compliant patients.
- Causes: Inadequate primary repair, premature or overly aggressive rehabilitation, inherent poor tendon quality (e.g., due to systemic disease), inadequate healing response, or re-traumatization.
- Management: Re-rupture is typically diagnosed with similar clinical signs to the initial injury. Revision surgery is almost always indicated. This often involves extensive debridement of scar tissue, identification of the re-ruptured ends, and almost invariably requires augmentation with a strong autograft (e.g., hamstring, quadriceps tendon) or allograft (e.g., Achilles tendon with bone block) to bridge the often larger defect and reinforce the repair.
-
Elbow Stiffness / Loss of Range of Motion (ROM):
- Incidence: A common complication, with reported rates between 10% and 20%. Loss of terminal extension is more frequently observed than flexion contracture.
- Causes: Prolonged immobilization, excessive post-operative scarring, heterotopic ossification, capsular contracture, or inadequate patient adherence to a strict rehabilitation protocol.
- Management: Prevention is key through early controlled mobilization. For established stiffness, a structured physical therapy program focusing on stretching, joint mobilization, and dynamic splinting is initiated. If non-operative measures fail, manipulation under anesthesia (MUA) may be considered. For persistent, recalcitrant stiffness, arthroscopic or open capsular release and adhesiolysis may be necessary. Prophylaxis against heterotopic ossification (NSAIDs or low-dose radiation) should be considered in high-risk patients.
-
Neurological Injury:
- Incidence: Radial nerve injury is rare (1-3%) but can be devastating. Injury to the posterior cutaneous nerve of the forearm (a sensory branch of the radial nerve) is more common (up to 5-10%).
- Causes: Direct laceration, stretch injury from vigorous retraction, or compression during surgery. The radial nerve's proximity to the humeral shaft in the spiral groove and the posterior cutaneous nerve's superficial course make them vulnerable.
-
Management:
- Posterior Cutaneous Nerve: Sensory deficits (numbness, dysesthesia) are often tolerated. Painful neuromas can be managed with local injections, surgical excision, or nerve capping.
- Radial Nerve: Immediate post-operative radial nerve palsy warrants prompt investigation (clinical exam, potentially EMG/NCS). For neuropraxia, observation is typically sufficient, with most cases resolving spontaneously within 3-6 months. Lack of recovery may necessitate neurolysis. Complete transection, though rare, would require primary repair or nerve grafting.
-
Infection:
- Incidence: Low, typically 1-5%, similar to other elective orthopedic procedures.
- Causes: Contamination during surgery, compromised host immunity, or poor wound healing.
- Management: Superficial infections may respond to targeted oral antibiotics and local wound care. Deep infections mandate urgent surgical debridement, tissue sampling for culture, intravenous antibiotic therapy tailored to sensitivities, and potentially removal of non-essential hardware. Prolonged antibiotic courses are often required.
-
Persistent Weakness / Fatigue:
- Incidence: Reported in 5-10% of patients, with some degree of residual strength deficit or fatigability often persisting despite an anatomically successful repair.
- Causes: Pre-existing muscle atrophy, incomplete re-innervation, scar tissue within the muscle, or subtle laxity of the repair.
- Management: Continuous, progressive strengthening and conditioning rehabilitation. Re-evaluation of the repair's integrity (clinical and imaging). In cases of significant, unrecoverable weakness due to mechanical failure, revision surgery with robust augmentation may be considered.
-
Heterotopic Ossification (HO):
- Incidence: Variable, ranging from 5% to 15%, particularly in cases of severe trauma, associated elbow fractures, or revision surgery.
- Causes: Uncontrolled inflammatory cascade leading to ectopic bone formation in the soft tissues surrounding the joint.
- Management: Prophylaxis with non-steroidal anti-inflammatory drugs (NSAIDs) such as indomethacin (e.g., 25 mg TID for 3-6 weeks post-op) or a single low dose of post-operative radiation therapy (e.g., 700-800 cGy within 72 hours of surgery) is recommended for high-risk patients. If symptomatic HO develops and limits ROM, surgical excision is performed after the HO has matured (typically 6-12 months post-onset), often combined with further HO prophylaxis.
-
Hardware-Related Complications:
- Incidence: Approximately 5-10%, particularly with suture anchors or transosseous sutures tied over buttons.
- Causes: Suture pull-through (especially in osteoporotic bone), anchor failure (rare), knot irritation, or prominence of buttons/hardware.
- Management: Symptomatic hardware may require removal once the tendon healing is robust (typically 6-12 months post-operatively). If hardware failure compromises the repair integrity before healing, revision fixation may be necessary.
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Re-rupture | 2-5% | Revision repair (often with autograft/allograft augmentation), repeat debridement |
| Elbow Stiffness/ROM Loss | 10-20% | Aggressive physical therapy, dynamic splinting, manipulation under anesthesia, capsulotomy/arthrolysis (open or arthroscopic) |
| Radial Nerve Injury (Motor) | 1-3% | Observation for neuropraxia (3-6 months), EMG/NCS, neurolysis, nerve grafting (rare) |
| Posterior Cutaneous N. Injury | 5-10% | Conservative management for sensory loss; local injection, surgical excision, or capping for painful neuroma |
| Infection | 1-5% | Debridement, targeted antibiotics, implant removal (if severe/persistent) |
| Persistent Weakness | 5-10% | Progressive strengthening rehabilitation, re-evaluation of repair, consider augmentation for mechanical failure |
| Heterotopic Ossification | 5-15% | Prophylaxis (NSAIDs/radiation), surgical excision (if symptomatic/mature HO) |
| Hardware Complications | 5-10% | Symptomatic hardware removal, revision fixation (if mechanical failure) |
| Chronic Pain | Variable | Multimodal pain management, nerve blocks, physical therapy, psychological support |
Post-Operative Rehabilitation Protocols
A structured, progressive post-operative rehabilitation protocol is paramount for optimizing functional outcomes, preventing complications, and facilitating a safe return to activity following triceps tendon repair. While specific protocols may vary based on surgeon preference, injury chronicity, quality of repair, and patient factors, the underlying principles remain consistent: protect the healing repair, restore full range of motion, and gradually regain strength and endurance.
Phase I: Immobilization & Protection (Weeks 0-2/3)
- Goal: Protect the repair, minimize pain and swelling, promote initial soft tissue healing.
- Immobilization: The elbow is typically immobilized in a hinged elbow brace or posterior splint, locked in 20-45 degrees of flexion. This position reduces tension on the triceps repair. Some surgeons may prefer a slightly greater flexion (e.g., 60-70 degrees) for the first week to further relax the repair, particularly for extensive or augmented repairs.
-
Activities:
- Strict avoidance of active elbow extension against gravity or resistance.
- Passive range of motion (PROM) for wrist and hand.
- Shoulder ROM exercises (flexion, extension, abduction, adduction) within pain limits, avoiding positions that place undue stress on the elbow.
- Ice, elevation, and pain management as needed.
- Wound care.
- Precautions: No active elbow extension. No lifting with the affected arm. Avoid weight-bearing through the arm.
Phase II: Controlled Early Motion (Weeks 2/3 - 6)
- Goal: Gradually restore passive and active-assisted range of motion while protecting the healing tendon.
- Brace Adjustment: The hinged elbow brace is maintained. At week 2 or 3, gentle passive and active-assisted elbow flexion is initiated, gradually increasing to 90-100 degrees by week 6, as tolerated. Extension is typically limited to 0-30 degrees initially, progressing gradually. The brace allows a controlled arc of motion.
-
Activities:
- Passive & Active-Assisted ROM: Gentle flexion and extension within the brace's allowed limits. Progression is slow and steady, guided by pain and tissue response.
- Gentle Isometric Exercises: Biceps curls (active-assisted with the unaffected arm or very light weight), forearm pronation/supination. Triceps isometrics (gentle contraction against resistance with the elbow flexed) may begin cautiously towards the end of this phase, only if cleared by the surgeon and therapist .
- Scar Massage: Once the wound is fully healed, gentle scar massage can begin to prevent adhesions.
- Precautions: Continue to avoid active resisted elbow extension. No lifting, pushing, or pulling. The brace is worn at all times, except for hygiene and specific exercises.
Phase III: Gradual Strengthening (Weeks 6-12)
- Goal: Progressively increase strength and endurance of the triceps and surrounding musculature.
- Brace Management: The hinged elbow brace can be weaned off, typically around week 8-10, as comfortable and directed by the surgeon.
-
Activities:
- Active ROM: Full active elbow flexion and extension should be achieved.
- Isometric Strengthening: Progress to submaximal triceps isometrics.
- Isotonic Strengthening: Begin with light resistance exercises for elbow flexion and extension, gradually increasing weight. Examples include dumbbell curls, triceps press-downs (light bands initially), and push-ups against a wall or incline.
- Forearm and Wrist Strengthening: Continue and advance exercises.
- Proprioceptive Exercises: Early balance and coordination drills for the upper extremity.
- Precautions: Avoid sudden, ballistic movements. Continue to avoid heavy lifting or high-impact activities. Progress resistance slowly and only with good form. Pain should be the guide.
Phase IV: Advanced Strengthening & Return to Activity (Months 3-6+)
- Goal: Maximize strength, power, and endurance; gradually integrate sport-specific or activity-specific training.
-
Activities:
- Progressive Resistance Training: Advance to heavier weights and more challenging exercises for triceps (e.g., overhead triceps extensions, close-grip bench press, dips).
- Plyometric Drills: Introduce sport-specific plyometrics (e.g., medicine ball throws) for athletes.
- Functional Training: Simulate occupational or recreational activities.
- Endurance Training: High-repetition, low-weight exercises.
- Return to Sport/Heavy Labor: Gradual, progressive return to full activity, typically between 6 to 12 months post-operatively, depending on the demands. Full recovery of pre-injury strength and power may take up to a year or longer, and some residual deficits may persist, especially with high-demand activities. A strength differential of no more than 10-15% compared to the contralateral arm is often a benchmark.
- Precautions: Emphasize proper technique to prevent re-injury. Continue warm-up and cool-down routines. Listen to the body for signs of overtraining or re-injury.
Patient education throughout all phases is paramount. Regular communication between the surgeon, physical therapist, and patient ensures adherence to the protocol and appropriate progression. Modifications may be necessary based on individual healing, pain levels, and any encountered complications. Chronic repairs or those requiring extensive augmentation may necessitate a more conservative, prolonged rehabilitation schedule.
Summary of Key Literature / Guidelines
The existing literature on triceps tendon ruptures, while less voluminous than for more common tendon injuries, consistently supports operative management for acute, complete tears in active individuals to achieve optimal functional recovery. Research has primarily focused on surgical techniques, graft augmentation strategies for chronic or complex cases, and rehabilitation outcomes.
1. Surgical Techniques: Transosseous vs. Suture Anchors
Historically,
transosseous suture repair
has been the gold standard, providing a robust, direct tendon-to-bone fixation. Studies by authors such as Sherman et al. (1995) and Cheema et al. (2009) have demonstrated excellent outcomes with this technique, reporting high rates of return to pre-injury activity and good strength recovery. The biomechanical advantage of broad tendon contact with a prepared bony bed and secure fixation through the bone contributes to its reliability.
More recently, suture anchor repair has gained popularity. Biomechanical studies (e.g., Morrey et al., 2000; Kim et al., 2010) have shown that modern suture anchors, particularly those with multiple suture limbs or fully threaded designs, provide comparable or even superior pull-out strength to transosseous techniques. Clinical series (e.g., Widmer and Clark, 2012) have reported excellent functional outcomes, reduced operative time, and potentially decreased soft tissue dissection associated with suture anchor techniques. The choice between transosseous and suture anchor repair often comes down to surgeon preference, bone quality, and the specific anatomy of the rupture. Both are considered acceptable and highly effective for acute tears with good tissue quality.
2. Augmentation Strategies for Chronic and Complex Ruptures
The literature consistently highlights the challenges of repairing
chronic triceps tendon ruptures
(typically >3-4 weeks post-injury) due to tendon retraction, scar tissue, and muscle atrophy. In these scenarios, primary repair alone is often insufficient, and
augmentation with autograft or allograft
is frequently necessary.
*
Autografts:
Common choices include semitendinosus, gracilis, quadriceps tendon, or fascia lata. The quadriceps tendon autograft, in particular, offers robust tissue and a bone block for secure olecranon fixation, analogous to its use in chronic rotator cuff or Achilles repairs. Authors like Hak and Giza (2006) and DeBeer and St. Pierre (2007) have reported successful outcomes with autogenous graft augmentation.
*
Allografts:
Achilles tendon allograft with a calcaneal bone block is a popular and effective option, especially for large defects or when autograft harvest is undesirable. It provides excellent mechanical strength and a bone-to-bone interface for secure distal fixation. Publications by Tarsuslugil et al. (2014) and Morrey (2017) discuss the utility and outcomes of allograft reconstruction for massive or chronic tears. While successful, augmentation introduces complexities such as graft harvest morbidity (for autografts) or potential for immune reaction and disease transmission (for allografts), along with higher costs.
3. Outcomes and Return to Activity
Overall, the literature demonstrates
favorable outcomes
following surgical repair of triceps tendon ruptures. Most series report high rates of successful tendon healing, restoration of elbow extension strength, and good functional scores. Return to pre-injury sports or occupational activities is common, especially in acute repairs. However, subtle deficits in strength or endurance, particularly with high-load activities, may persist in a minority of patients.
* A systematic review by Rose et al. (2016) noted that surgical repair leads to satisfactory functional outcomes in the majority of patients, with a low re-rupture rate.
* Studies have emphasized that early diagnosis and timely surgical intervention are critical prognostic factors, leading to less complex repairs and better functional recovery. Delayed repair is associated with increased surgical complexity and potentially diminished outcomes.
4. Complications and Rehabilitation
The reported complication rates are generally low, with re-rupture, infection, stiffness, and nerve injury being the most significant concerns, as detailed in the previous section.
Post-operative rehabilitation protocols
are universally recognized as critical for optimal outcomes. While specific timelines vary, the general consensus advocates for a period of initial immobilization (2-4 weeks) followed by a carefully controlled, progressive increase in range of motion and gradual strengthening. Protection against active resisted extension is paramount in the early phases to prevent repair failure. The emphasis is on early controlled passive and active-assisted motion, transitioning to gentle strengthening and eventually to sport-specific activities. Consensus statements and expert opinion articles (e.g., from the American Shoulder and Elbow Surgeons - ASES) recommend individualized, progressive protocols guided by clinical healing and patient tolerance.
5. Emerging Trends and Areas of Research
Current research continues to explore optimizing fixation strength, particularly in osteoporotic bone, and refining augmentation techniques. The role of biologics (e.g., PRP, bone marrow aspirate concentrate) to enhance tendon-to-bone healing is an evolving area of interest, though robust clinical evidence is still developing. Further investigation into the optimal rehabilitation protocols for augmented repairs and chronic cases is also ongoing. The importance of shared decision-making, accounting for patient-specific factors, remains a cornerstone of management.
Clinical & Radiographic Imaging