Unlocking the Coronoid: Posteromedial Approach to the Process of the Ulna

Key Takeaway
For anyone wondering about Unlocking the Coronoid: Posteromedial Approach to the Process of the Ulna, The posteromedial approach provides excellent exposure of the coronoid process of the ulna and medial aspect of the proximal ulna. It's used for open reduction of coronoid fractures, medial collateral ligament repair, and stabilization of sublime tubercle fractures. This approach, though not utilizing an internervous plane, risks the ulnar nerve due to its path through the nerve's bed.
Unlocking the Coronoid: Posteromedial Approach to the Process of the Ulna
Introduction & Epidemiology
Fractures of the coronoid process of the ulna, while often perceived as secondary injuries, are increasingly recognized as critical determinants of elbow stability. Their involvement significantly influences the management and prognosis of complex elbow dislocations, trans-olecranon fracture-dislocations, and various degrees of elbow instability. Historically, coronoid fractures were often overlooked, with treatment focusing primarily on associated injuries such as radial head fractures or olecranon fractures. However, contemporary understanding emphasizes the coronoid's fundamental role in providing anterior and medial buttressing against posterior and valgus displacement, respectively, making its integrity paramount for stable elbow function.
The incidence of coronoid fractures varies depending on the associated injury pattern. They are implicated in approximately 10-15% of all elbow fractures and dislocations. Notably, they are a hallmark component of the "terrible triad" injury, which comprises elbow dislocation, radial head fracture, and coronoid fracture, representing a complex and often challenging clinical scenario. Isolated coronoid fractures are rare, typically resulting from shear forces during hyperextension injuries or direct impaction. More commonly, they occur in conjunction with ligamentous injuries (e.g., medial collateral ligament (MCL) or lateral collateral ligament (LCL) ruptures) and other osseous injuries (e.g., radial head fractures, olecranon fractures). The anteromedial facet of the coronoid, which serves as the insertion site for the anterior bundle of the MCL (abMCL) and the anterior capsule, is particularly susceptible to avulsion fractures, often in valgus posteromedial rotatory instability patterns.
The posteromedial approach to the coronoid process of the ulna offers direct and comprehensive exposure of the anteromedial aspect of the coronoid, the sublime tubercle, and the anterior bundle of the MCL. This approach is particularly advantageous for addressing specific fracture morphologies, primarily those involving the anteromedial facet and larger coronoid fragments, especially in the context of valgus instability or concomitant MCL injuries. While providing excellent visualization and access for reduction and fixation, it necessitates meticulous dissection due to the intimate relationship with vital neurovascular structures, most notably the ulnar nerve.
Surgical Anatomy & Biomechanics
Surgical Anatomy
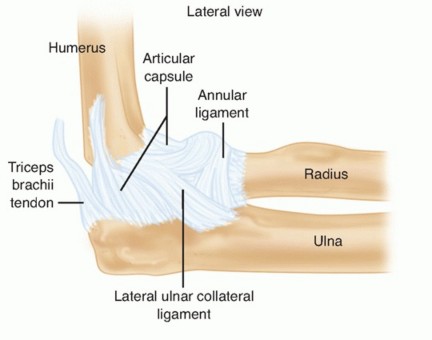
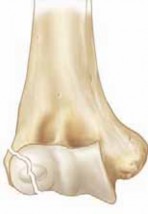
The coronoid process is an integral bony projection from the proximal ulna, comprising approximately 20% of the olecranon-coronoid complex. It articulates with the trochlea of the humerus, forming a crucial component of the ulnohumeral joint. From a surgical perspective, several key anatomical landmarks and structures are pertinent to the posteromedial approach:
- Coronoid Process: This structure can be broadly divided into an anterior facet (articular), an anterolateral facet, and an anteromedial facet. The anteromedial facet, specifically, provides insertion for the anterior bundle of the MCL and the anterior capsule. The sublime tubercle is a distinct prominence on the medial aspect of the coronoid, marking the primary attachment site for the anterior bundle of the MCL. The brachialis muscle inserts broadly onto the anterior and medial surfaces of the coronoid and the proximal ulna.
- Medial Collateral Ligament (MCL): Composed of anterior, posterior, and transverse bundles. The anterior bundle (abMCL) is the primary static stabilizer against valgus stress at all degrees of elbow flexion. Its fan-shaped origin is from the anterior inferior aspect of the medial epicondyle, inserting onto the sublime tubercle. Injuries to this ligament, often avulsion fractures of the sublime tubercle or mid-substance tears, are frequently associated with coronoid fractures, particularly anteromedial facet fractures.
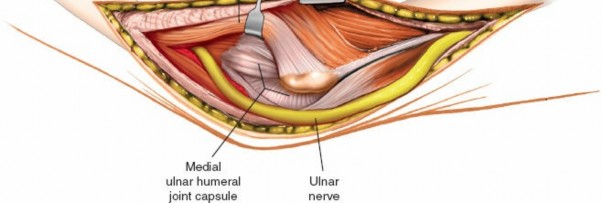
- Ulnar Nerve: This is the most critical neurovascular structure at risk during a posteromedial approach. The ulnar nerve passes posterior to the medial epicondyle within the cubital tunnel, then courses distally between the two heads of the flexor carpi ulnaris (FCU) muscle. The surgical trajectory of the posteromedial approach often lies directly in the "bed" of the ulnar nerve, necessitating its careful identification, mobilization, and protection.
- Medial Antebrachial Cutaneous Nerve (MACN): A sensory nerve that typically arises from the medial cord of the brachial plexus. It courses down the arm medial to the brachial artery, piercing the deep fascia proximal to the medial epicondyle. Its branches are superficial and vulnerable to injury during skin incision and subcutaneous dissection in this region, leading to sensory deficits in the medial forearm.
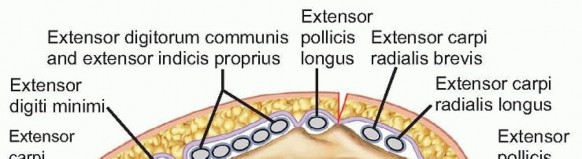
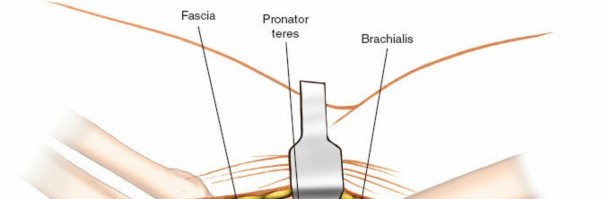
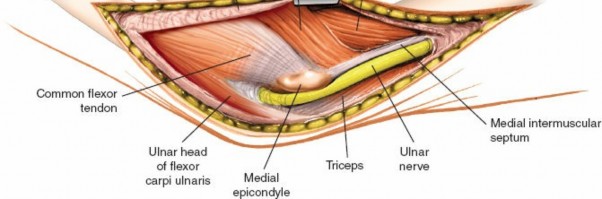
- Common Flexor-Pronator Mass: Originating from the medial epicondyle, this muscle group (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris) must be elevated or incised to access the deeper structures. The FCU is particularly relevant as it forms the roof of the cubital tunnel.
- Brachial Artery and Median Nerve: These structures lie anterior to the elbow joint capsule. While not directly in the primary dissection field, aggressive anterior retraction should be avoided to prevent injury.
- Internervous Plane: The posteromedial approach does not utilize a true internervous plane for deep dissection or extensibility in the conventional sense. The approach involves dissecting through the common flexor pronator origin and elevating it, or directly incising the FCU, within the territory of the ulnar nerve (for the FCU and medial aspect of FDS) or median nerve (for other flexors). This necessitates a careful, anatomical layer-by-layer dissection rather than following a specific fascial plane between distinct nerve territories, making the ulnar nerve vulnerable.
Biomechanics
The coronoid process plays a crucial biomechanical role in maintaining elbow stability:
- Anterior Buttress: The coronoid acts as a primary bony block against posterior displacement of the ulna relative to the humerus, especially in extension. Loss of this anterior buttress, particularly with larger coronoid fractures (Regan & Morrey Type II and III), significantly compromises posterior stability.
- Valgus Stability: The anteromedial facet, with its attachment of the abMCL, is critical for resisting valgus stress. Fractures involving this facet (e.g., O'Driscoll Type 1, 2, 3 anteromedial coronoid fractures) lead to medial column instability, often manifesting as posteromedial rotatory instability.
- Axial Load Transmission: The coronoid contributes to the articulation with the trochlea, distributing axial loads across the ulnohumeral joint.
- Overall Elbow Stability: In complex injuries like the terrible triad, the combination of coronoid fracture, radial head fracture, and LCL injury leads to gross instability. Repair of the coronoid process, often in conjunction with radial head fixation/replacement and LCL repair, is essential for restoring stability.
Indications & Contraindications
The posteromedial approach is tailored for specific elbow pathologies, primarily involving the anteromedial coronoid and medial soft tissue structures.
Indications
-
Coronoid Process Fractures:
- Anteromedial Coronoid Fractures (O'Driscoll Classification): This approach is ideal for O'Driscoll Type 1 (sublime tubercle avulsion), Type 2 (small osteochondral fragment), and Type 3 (large fragment including articular surface) anteromedial coronoid fractures, particularly when associated with valgus instability or MCL avulsion.
- Regan & Morrey Type II and III Coronoid Fractures: For larger fragments (involving >10-15% of articular surface) or comminuted fragments that are displaced and require direct visualization for reduction and buttress plating, especially when associated with medial instability.
- Fractures with Significant Displacement: Coronoid fractures that are displaced and block reduction of an elbow dislocation, or contribute to persistent instability after reduction.
- Fractures Associated with MCL Insufficiency: Often, fixation of the coronoid fragment and reattachment of the abMCL can be performed simultaneously via this approach.
-
Repair/Reconstruction of the Medial Collateral Ligament (MCL):
- Avulsion fractures of the sublime tubercle requiring reattachment.
- Mid-substance tears of the abMCL requiring direct repair, often in conjunction with coronoid fixation.
- Reconstruction of the abMCL using autograft or allograft, though a dedicated medial approach might be preferred for isolated reconstructions.
- Exposure of the Sublime Tubercle of the Ulna: For stabilization of avulsion fractures or reattachment of the abMCL.
- Complex Elbow Instability: In cases of chronic posteromedial rotatory instability or persistent instability after other stabilization procedures, especially when a primary medial deficiency is identified.
Contraindications
- Isolated Lateral Elbow Instability: Conditions like isolated LCL tears or purely lateral-sided radial head fractures are better addressed via lateral approaches (e.g., Kocher, Kaplan).
- Isolated Radial Head Fractures: Unless part of a terrible triad with significant medial instability or a large coronoid component requiring medial access.
- Anterolateral Coronoid Fractures: These are rare and might be better approached laterally if required.
- Significant Soft Tissue Compromise: Open fractures with extensive contamination or poor soft tissue envelope might preclude an immediate direct approach.
- Severe Medical Comorbidities: Patients unsuitable for general or regional anesthesia and prolonged surgery.
- Purely Non-Displaced, Stable Coronoid Fractures: Small, undisplaced fractures without associated instability are typically managed non-operatively.
Operative vs. Non-Operative Indications for Coronoid Fractures
| Feature | Non-Operative Management | Operative Management (Posteromedial Approach Preferred) |
|---|---|---|
| Fracture Type | Regan & Morrey Type I (tip avulsion), small <2mm fragment. | Regan & Morrey Type II/III (>10-15% of articular surface, displaced). O'Driscoll Anteromedial Type 1, 2, 3. |
| Displacement | Minimal or no displacement. | Displaced fragment (often >2mm), especially if blocking reduction. |
| Elbow Stability | Stable elbow after reduction (if dislocated) without obvious ligamentous laxity. | Gross instability after reduction, persistent subluxation, valgus instability. |
| Associated Injuries | Isolated minor coronoid fracture. | Medial collateral ligament avulsion/rupture, terrible triad, posteromedial rotatory instability. |
| Patient Factors | Low functional demand, significant comorbidities precluding surgery. | Active, functional patient, amenable to surgery and rehabilitation. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial for successful outcomes and minimizing complications.
Pre-Operative Planning
-
Imaging Review:
- Standard Radiographs: AP, lateral, and oblique views of the elbow provide initial assessment of fracture morphology, displacement, and associated dislocation.
- Computed Tomography (CT) Scan with 3D Reconstructions: Essential for detailed evaluation of coronoid fracture patterns (especially anteromedial facet involvement), fragment size, comminution, and articular involvement. 3D reconstructions are invaluable for understanding the complex spatial orientation of fragments and planning the reduction strategy. CT also helps identify associated radial head or olecranon fractures.
- Magnetic Resonance Imaging (MRI): May be indicated if significant ligamentous injuries (MCL, LCL) or occult osteochondral lesions are suspected, though often, the instability pattern on physical exam and plain films/CT is sufficient to guide MCL exploration.
-
Implant Selection:
Based on CT findings, appropriate implants are selected. This may include:
- Small fragment screws (2.0mm, 2.4mm, 2.7mm lag screws).
- Headless compression screws for smaller articular fragments.
- Anteromedial coronoid specific plates (e.g., pre-contoured buttress plates, often L-shaped or T-shaped).
- Suture anchors for ligamentous reattachment (e.g., abMCL to sublime tubercle).
- K-wires for temporary fixation.
- Arthroscopy Planning (Optional): In select cases, elbow arthroscopy may be performed prior to or in conjunction with open reduction to assess articular congruity, remove loose bodies, or address associated chondral injuries.
- Contingency Planning: Anticipate potential challenges such as comminution, difficulty in reduction, or need for concomitant procedures (e.g., radial head fixation/replacement, LCL repair). Ensure availability of a range of implants and instruments.
Patient Positioning
The patient positioning is critical for optimal exposure and safety.
Place the patient in a
lateral decubitus position
on the operating table.
The affected arm is supported by a padded arm board or a specialized hand table, allowing free movement of the elbow.

- Limb Exsanguination and Tourniquet Application: Exsanguinate the limb by elevating it, then apply a pneumatic tourniquet as high up on the arm as possible to allow for a bloodless field during dissection.
- Arm Position: Allow the elbow to flex to approximately 90 degrees, with the forearm hanging freely or supported over the padded table. This position puts the ulnar nerve on slack and allows for better access to the posteromedial aspect. Some surgeons prefer a supine position with the arm abducted on a hand table, which can facilitate fluoroscopy but may make posteromedial exposure slightly more challenging. The lateral position often provides superior access to the posteromedial aspect of the elbow.
- Padding: Ensure all pressure points are adequately padded, especially the contralateral arm, legs, and bony prominences.
- Draping: The limb is draped sterilely, allowing full access to the elbow joint and proximal forearm, typically from the mid-humerus to the wrist. Allow for unhindered use of a C-arm if intraoperative fluoroscopy is planned.
Detailed Surgical Approach / Technique
The posteromedial approach requires meticulous attention to detail, particularly regarding neurovascular structures.
Incision
-
Skin Incision:
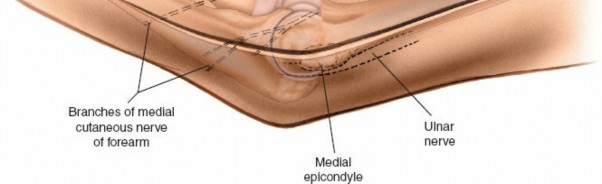
A curvilinear skin incision is made centered posterior to the medial epicondyle. It typically starts approximately 5-7 cm proximal to the medial epicondyle, curves gently posterior to the medial epicondyle, and extends distally along the medial border of the ulna for approximately 5-7 cm. This incision directly overlies the cubital tunnel and the ulnar nerve.
- Pitfall: Avoid a straight incision directly over the medial epicondyle, as this may lead to symptomatic scarring and contracture.
Superficial Dissection
-
Subcutaneous Dissection:
The subcutaneous tissue is carefully dissected. Identify and protect branches of the
medial antebrachial cutaneous nerve (MACN)
. These sensory nerves are highly variable in their course and are vulnerable to iatrogenic injury during this stage. They typically lie superficial to the deep fascia. If encountered, they should be carefully mobilized and retracted.
Deep Dissection and Ulnar Nerve Management
-
Identification of the Ulnar Nerve:
The deep fascia overlying the cubital tunnel is incised. The
ulnar nerve
is the most critical structure in this approach and must be identified early. It lies within the cubital tunnel, posterior to the medial epicondyle, and then passes deep to the arcuate ligament (Osborne's ligament) between the two heads of the flexor carpi ulnaris (FCU).
 -
Ulnar Nerve Mobilization and Transposition:
Once identified, the ulnar nerve is carefully dissected free from its surrounding tissues. It is mobilized proximally and distally, releasing any constricting fascial bands, including the arcuate ligament. In most cases, the ulnar nerve is gently retracted anteriorly throughout the procedure. Some surgeons prefer to perform a prophylactic anterior subcutaneous or submuscular transposition of the ulnar nerve to ensure its complete protection and to provide an unobstructed operative field. This decision depends on the surgeon's preference, the extent of required exposure, and the presence of pre-existing cubital tunnel symptoms. If transposed, ensure the nerve lies in a loose, tension-free bed.
Exposure of the Coronoid Process
-
Flexor-Pronator Mass Management:
- After the ulnar nerve is protected, the common flexor-pronator mass originating from the medial epicondyle is addressed. The approach involves either a partial release and elevation of this mass or an incision directly through the FCU and flexor digitorum superficialis (FDS) muscles.
- Option A (Elevation): A subperiosteal elevation of the common flexor pronator origin from the medial epicondyle and the anterior aspect of the ulna can be performed. This creates a flap of muscle that can be retracted anteriorly and distally, exposing the underlying anterior bundle of the MCL and the elbow capsule.
-
Option B (Split/Incision):
Alternatively, a longitudinal incision can be made through the belly of the FCU, distal to the ulnar nerve, and then extended through the FDS to expose the deeper structures. This direct incision offers excellent access but necessitates meticulous repair at closure.
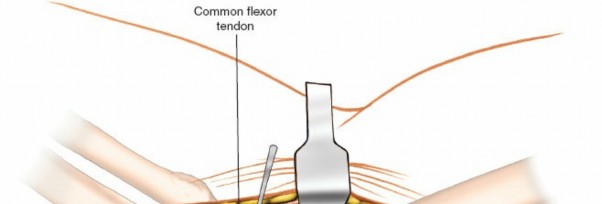
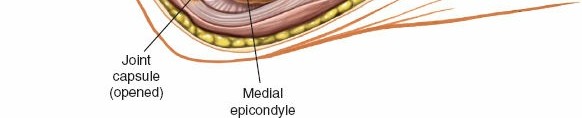
- Exposure of MCL and Capsule: Once the flexor-pronator mass is retracted, the anterior bundle of the MCL (abMCL) and the anterior joint capsule become visible. In cases of associated MCL injury or avulsion from the sublime tubercle, the tears will be evident. If the abMCL is intact, an incision through its anterior fibers or a portion of the capsule may be necessary to gain direct access to the coronoid process. Careful identification of the sublime tubercle is crucial as it guides access to the anteromedial coronoid.
-
Coronoid Exposure:
Retraction of the muscles and ligaments exposes the anteromedial facet of the coronoid process and the sublime tubercle. Any hematoma or granulation tissue is debrided to clearly visualize the fracture fragments.
- Visualization: Flexion of the elbow facilitates better visualization of the coronoid process.
Reduction and Internal Fixation
- Fragment Identification and Mobilization: Identify all fracture fragments. Use small hooks, elevators, or K-wires to carefully mobilize and assess their size and displacement.
- Reduction: The coronoid fragment is anatomically reduced. This often requires gentle traction on the forearm and direct manipulation of the fragment. Temporary fixation is achieved with small K-wires. Ensure anatomical alignment and restoration of the articular surface. Intraoperative fluoroscopy can be used to confirm reduction.
-
Fixation:
-
Buttress Plating:
For larger, displaced anteromedial coronoid fractures (O'Driscoll Type 2 and 3), a small pre-contoured anteromedial coronoid plate (e.g., L-shaped, T-shaped, or specifically designed coronoid plates) is often used. This plate provides a stable buttress against posterior and valgus forces. The plate is typically positioned along the anteromedial aspect of the ulna, with screws engaging the ulna shaft and the coronoid fragment.
 - Lag Screws: If the fragment is large enough (typically >1 cm) and suitable, one or two small fragment lag screws (e.g., 2.0mm, 2.4mm, 2.7mm) can be placed from the anteromedial aspect of the ulna into the coronoid fragment. Headless compression screws can be used for intra-articular fragments to minimize hardware prominence.
- Suture Fixation: For small avulsion fractures (e.g., sublime tubercle, Regan & Morrey Type I) or highly comminuted fragments where screw fixation is not feasible, non-absorbable sutures can be passed through drill holes in the coronoid fragment and then through the anterior ulna or reattached to the abMCL. Suture anchors can also be utilized for reattachment of the abMCL to the sublime tubercle.
-
Buttress Plating:
For larger, displaced anteromedial coronoid fractures (O'Driscoll Type 2 and 3), a small pre-contoured anteromedial coronoid plate (e.g., L-shaped, T-shaped, or specifically designed coronoid plates) is often used. This plate provides a stable buttress against posterior and valgus forces. The plate is typically positioned along the anteromedial aspect of the ulna, with screws engaging the ulna shaft and the coronoid fragment.
- MCL Repair/Reconstruction: If the abMCL is avulsed or torn, it is primarily repaired using suture anchors or transosseous sutures, reattaching it to its anatomical insertion on the sublime tubercle and medial epicondyle as indicated.
- Elbow Stability Assessment: After fixation, the elbow is put through a full range of motion (flexion, extension, supination, pronation) with valgus and varus stress applied to assess stability. Any persistent instability should be addressed.
Wound Closure
- Muscle Repair: The elevated flexor-pronator mass is reattached to the medial epicondyle and proximal ulna using strong absorbable sutures. If an incision was made through the muscle belly, it is meticulously repaired.
- Ulnar Nerve Assessment: Ensure the ulnar nerve lies in a tension-free environment. If transposed, ensure it is covered by sufficient soft tissue.
- Subcutaneous and Skin Closure: The subcutaneous layer is closed, followed by skin closure using standard techniques.
Complications & Management
Despite meticulous technique, complications can arise with the posteromedial approach to the coronoid. Proactive identification and appropriate management are crucial.
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Ulnar Nerve Injury | 5-20% |
Prevention:
Meticulous identification, mobilization, and protection. Prophylactic anterior transposition often considered.
Post-op: Immediate clinical evaluation. If severe deficit, EMG/NCS. Management: Conservative for neuropraxia (splinting, therapy). Exploration and neurolysis for persistent symptoms/severe injury. Nerve repair/grafting for transection. Secondary transposition for delayed onset neuropathy. |
| Elbow Stiffness/Loss of ROM | 10-30% |
Prevention:
Early, controlled range of motion post-operatively. Meticulous soft tissue handling to minimize scarring.
Post-op: Aggressive physical therapy, dynamic splinting. Management: Manipulation under anesthesia for resistant stiffness (after 3-6 months). Arthroscopic or open capsular release for severe, persistent stiffness (usually 6-12 months post-op). Heterotopic ossification prophylaxis (NSAIDs/radiation). |
| Heterotopic Ossification (HO) | 10-50% (higher in severe trauma) |
Prevention:
Prophylactic NSAIDs (Indomethacin) for 3-6 weeks, especially in high-risk patients (head injury, burns, terrible triad, severe comminution). Low-dose radiation therapy (7-10 Gy) may be considered in very high-risk cases.
Post-op: Early detection via radiographs. Management: Aggressive rehabilitation. Surgical excision of mature HO after 6-12 months if limiting function, followed by repeat HO prophylaxis. |
| Nonunion/Malunion | <5% |
Prevention:
Meticulous anatomical reduction and stable internal fixation.
Post-op: Clinical and radiographic follow-up. Management: For symptomatic nonunion, revision surgery with débridement, bone grafting, and more rigid fixation. Malunion may require corrective osteotomy if significantly impacting function or causing instability. |
| Infection | 1-5% |
Prevention:
Strict aseptic technique, prophylactic antibiotics.
Post-op: Clinical signs (erythema, pain, discharge, fever). Management: Superficial infections often respond to oral antibiotics. Deep infections require surgical débridement, irrigation, intravenous antibiotics, and potentially hardware removal (if stable union) or two-stage revision. |
| Hardware Prominence/Irritation | 5-15% |
Prevention:
Use low-profile implants, countersink screws where possible.
Post-op: Symptoms (pain, tenderness over hardware). Management: Removal of symptomatic hardware, typically after fracture union is confirmed (6-12 months). |
| Persistent Instability | 5-15% |
Prevention:
Comprehensive assessment and repair of all stabilizing structures (coronoid, radial head, MCL, LCL). Careful intraoperative stability testing.
Post-op: Clinical examination, stress radiographs. Management: Dynamic bracing. Revision surgery to address remaining instability (ligamentous reconstruction, further bony fixation, or prosthetic replacement for radial head/coronoid). |
| Post-Traumatic Arthritis | Variable (long-term) |
Prevention:
Anatomical reduction of articular surfaces, stable fixation, early motion.
Post-op: Long-term clinical and radiographic follow-up. Management: Conservative (NSAIDs, activity modification, injections) for mild symptoms. For severe arthritis, surgical options include débridement, interposition arthroplasty, or total elbow arthroplasty in older, low-demand patients. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring elbow function, minimizing stiffness, and optimizing outcomes after coronoid fixation. The protocol is individualized based on fracture stability, fixation quality, and associated injuries (e.g., MCL repair).
General Principles
- Pain Management: Adequate analgesia is essential to facilitate early motion.
- Wound Care: Standard wound care until sutures/staples are removed.
- Edema Control: Elevation and gentle compression.
- Protection: The elbow is typically protected in a hinged elbow brace, allowing for controlled range of motion (ROM) while restricting terminal extension or valgus stress, as per the surgeon's discretion based on stability.
Phase I: Protective Phase (Weeks 0-4)
- Goal: Protect fixation, control pain and swelling, initiate gentle motion.
-
Immobilization:
- Typically, a posterior splint or hinged elbow brace is applied, initially locked for comfort or in a specific arc (e.g., 30-90 degrees) based on intraoperative stability.
- The brace is often unlocked for supervised exercises or when transitioning to the next phase.
-
Motion:
- Active-Assisted Range of Motion (AAROM): Initiate gentle AAROM exercises within a safe, pain-free arc as early as post-operative day 1-3, gradually increasing as tolerated. Typically, this starts with 30-90 degrees of flexion/extension, and full forearm pronation/supination.
- Passive Range of Motion (PROM): Gentle PROM may be initiated by the therapist if the fixation is deemed very stable, but often deferred initially to avoid stressing the repair.
-
Activities:
- No weight-bearing on the affected arm.
- Avoid lifting, pushing, pulling.
- Daily activities limited to unaffected limb.
- Precautions: Avoid active elbow extension past the restricted limit, forceful gripping, or valgus stress.
Phase II: Intermediate Phase (Weeks 4-8)
- Goal: Gradually increase ROM, initiate gentle strengthening.
-
Motion:
- Progressive increase in flexion/extension ROM, aiming for near full range by end of this phase, if stable. The hinged brace may be adjusted to allow further extension (e.g., 10-120 degrees) and ultimately unlocked as tolerated.
- Continued AAROM and light PROM.
-
Strengthening:
- Begin with gentle isometric exercises for biceps, triceps, wrist flexors/extensors, forearm pronators/supinators.
- Progress to very light resistance exercises with elastic bands or light weights.
- Activities: Continue to avoid heavy lifting or high-impact activities. Gradually increase use of the extremity for light daily tasks.
- Precautions: Avoid sudden movements, uncontrolled heavy lifting, or activities that produce pain. Continue to monitor for signs of instability.
Phase III: Advanced Strengthening & Functional Phase (Weeks 8-16+)
- Goal: Achieve full, functional ROM and strength, return to activity.
- Motion: Continue to work on achieving full, pain-free ROM. Static progressive splinting may be considered for persistent deficits.
-
Strengthening:
- Progressive resistive exercises with increasing weights and resistance bands.
- Focus on eccentric control and functional movements.
- Introduce sport-specific or work-specific exercises as appropriate.
-
Activities:
- Gradual return to recreational activities and occupational tasks.
- Initiate return-to-sport activities (e.g., throwing programs) under supervision, typically starting after 4-6 months, depending on the sport and injury severity.
- Precautions: Patients should be counseled on gradual progression and avoiding re-injury. Full return to contact sports or heavy labor may take 6-12 months.
Specific Considerations for MCL Repair
If an MCL repair was performed, the rehabilitation protocol will be more conservative regarding valgus stress. The brace will typically be locked to prevent valgus forces in early phases, and gradual, controlled valgus stress may be introduced later in rehabilitation.
Summary of Key Literature / Guidelines
The understanding and management of coronoid fractures have evolved significantly over the past few decades, driven by increased recognition of their critical role in elbow stability.
-
Classification Systems:
- Regan and Morrey (1989): This historical classification, based on fragment size (Type I: tip, <10%; Type II: 10-50%; Type III: >50% of coronoid height), provided an initial framework. However, it lacks specificity for anteromedial fragments.
- O'Driscoll et al. (2003): This landmark classification specifically addresses anteromedial coronoid fractures, categorizing them into three types (Type 1: sublime tubercle avulsion; Type 2: small osteochondral fragment; Type 3: larger fragment involving the articular surface). This classification is particularly relevant for guiding the use of the posteromedial approach, as these injuries are often associated with posteromedial rotatory instability or valgus instability and typically require surgical fixation.
- AO/OTA Classification: Offers a more comprehensive, alphanumeric system that can describe coronoid fractures within the context of proximal ulna fractures.
- Biomechanics and Stability: Numerous biomechanical studies have elucidated the coronoid's role as a primary anterior buttress and the abMCL's role as a primary valgus stabilizer. Loss of these structures, particularly in the terrible triad injury pattern, leads to gross instability. Consensus now exists that anatomical reduction and stable fixation of coronoid fractures, especially larger or anteromedial fragments, are essential for restoring stability and preventing post-traumatic arthritis.
- Surgical Approaches: While posterior and combined medial/lateral approaches have been described, the posteromedial approach has gained prominence for specific anteromedial coronoid fractures. Literature supports its efficacy in providing direct visualization and stable fixation for these complex injuries. The direct anterior approach, though providing good visualization, poses higher risks to the median nerve and brachial artery. The posteromedial approach mitigates these specific anterior risks while placing the ulnar nerve as the primary structure at risk.
- Outcomes: Studies on coronoid fracture fixation generally report good to excellent outcomes in terms of elbow stability and return of function, especially when anatomical reduction and rigid fixation are achieved, and concomitant ligamentous injuries are addressed. However, complications such as stiffness, heterotopic ossification, and ulnar neuropathy remain significant concerns.
- Modern Management Principles: Current guidelines emphasize the need for advanced imaging (CT with 3D), meticulous pre-operative planning, and comprehensive surgical reconstruction addressing all injured stabilizers (bone and ligamentous). Early, controlled motion rehabilitation is also a cornerstone of post-operative management to mitigate stiffness. The posteromedial approach offers a robust solution for a specific subset of these challenging elbow injuries.
Clinical & Radiographic Imaging
You Might Also Like