Comprehensive Guide to Adult Monteggia Fracture-Dislocations: Epidemiology, Anatomy, and Management

Key Takeaway
Monteggia fracture-dislocations are complex injuries characterized by an ulnar fracture combined with a dislocation of the radial head. Primarily occurring in adults from high-energy trauma, they are classified by Bado into Type I-IV based on radial head dislocation direction and ulnar fracture location. Meticulous surgical management is crucial for preventing chronic instability, pain, and functional impairment.
Introduction & Epidemiology
Monteggia fracture-dislocations are complex injuries characterized by a fracture of the ulna associated with a dislocation of the radial head. First described by Giovanni Battista Monteggia in 1814, these injuries represent a critical diagnostic and therapeutic challenge due to their inherent instability and high propensity for poor outcomes if not managed appropriately. In adults, Monteggia injuries typically result from high-energy trauma, often involving a fall onto an outstretched hand (FOOSH) with a hyperpronated or hyperextended elbow, or a direct blow to the forearm.
Epidemiologically, Monteggia injuries are less common in adults than in children, accounting for approximately 1-2% of all forearm fractures. However, they carry significant morbidity in the adult population, frequently resulting in pain, restricted motion, and instability if primary anatomic reduction and stable fixation are not achieved. The classification system proposed by Bado in 1967 remains the most widely accepted for adult Monteggia fractures, categorizing them based on the direction of radial head dislocation and the location/angulation of the ulnar fracture:
*
Type I:
Anterior dislocation of the radial head with an associated fracture of the ulnar diaphysis, typically angulated anteriorly. This is the most common type, accounting for approximately 60% of adult cases.
*
Type II:
Posterior or posterolateral dislocation of the radial head with a fracture of the ulnar diaphysis, typically angulated posteriorly. This type is less common but carries a higher risk of ulnar nerve injury.
*
Type III:
Lateral or anterolateral dislocation of the radial head with a fracture of the ulnar metaphysis (proximal to the coronoid). Often associated with severe comminution.
*
Type IV:
Anterior dislocation of the radial head with fractures of both the radial and ulnar diaphyses at the same level. This type implies extensive soft tissue injury and instability.
Prompt and accurate diagnosis, followed by meticulous surgical management, is paramount to prevent chronic instability, persistent pain, heterotopic ossification, and significant functional impairment in the adult patient.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the elbow and forearm anatomy is fundamental to effectively manage Monteggia fracture-dislocations. The elbow is a complex hinge joint comprising three articulations: the humeroulnar, humeroradial, and proximal radioulnar joints (PRUJ). The stability of the PRUJ is critically dependent on the integrity of the ulna, the annular ligament, and the interosseous membrane.
Bony Anatomy
- Ulna: The ulna serves as the primary forearm stabilizer and provides a fixed axis for forearm rotation. The olecranon and coronoid processes are crucial for humeroulnar articulation. The shaft's length, alignment, and rotation are essential for maintaining the relationship between the radial head and the capitellum. Fractures disrupting ulnar length, angulation, or rotation inevitably lead to instability of the radial head.
- Radius: The radial head articulates with the capitellum of the humerus and the radial notch of the ulna. Its unique shape allows for pronation and supination. The radial neck and tuberosity provide attachment for muscle and ligamentous structures. In Monteggia injuries, the radial head's position is dictated by the ulna's integrity and the annular ligament's status.
- Humerus: The distal humerus provides the articulating surfaces (trochlea and capitellum) for the ulna and radius, respectively.
Ligamentous Structures
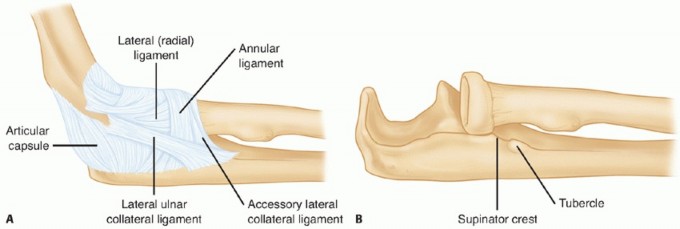
- Annular Ligament: This is the primary stabilizer of the radial head within the radial notch of the ulna. It forms a fibrous ring encircling the radial head and neck, attaching to the anterior and posterior margins of the radial notch. Tears or avulsions of the annular ligament are common in Monteggia injuries and can prevent successful closed reduction or lead to recurrent dislocation even after ulnar fixation.
- Medial Collateral Ligament (MCL): Consists of anterior, posterior, and transverse bundles. Provides valgus stability.
- Lateral Collateral Ligament (LCL) Complex: Comprises the Radial Collateral Ligament (RCL), Ulnar Collateral Ligament (UCL) originating from the lateral epicondyle, and the Accessory Collateral Ligament (ACL). The Lateral Ulnar Collateral Ligament (LUCL) is critical for posterolateral rotatory stability. While less directly involved in radial head dislocation compared to the annular ligament, severe concomitant ligamentous injuries can complicate overall elbow stability.
- Interosseous Membrane (IOM): A strong fibrous sheet connecting the ulna and radius, transmitting axial loads from the hand to the elbow. Its integrity contributes significantly to forearm stability and assists in preventing proximal migration of the radius. While typically not directly repaired, its tension is restored with anatomic reduction of the ulna.
Neurovascular Structures
- Posterior Interosseous Nerve (PIN): A deep branch of the radial nerve, it passes through the supinator muscle. It is particularly vulnerable to injury during Type III Monteggia fractures and during surgical approaches involving the lateral elbow or extensive dissection around the radial neck.
- Ulnar Nerve: Lies in the cubital tunnel posteriorly. It is at risk during posterior approaches or in cases of severe posterior displacement of the ulna.
- Median Nerve: Lies anteriorly in the antecubital fossa. Less commonly injured in Monteggia fractures but should be assessed.
- Brachial Artery: Lies anteriorly, also less commonly injured but requires assessment.
Biomechanics of Injury
Monteggia fracture-dislocations typically occur when a significant force disrupts the intricate relationship between the ulna, radius, and humerus.
*
Hyperpronation Mechanism (Bado Type I):
A fall on an outstretched hand with the forearm in hyperpronation. The pronation force drives the radial head anteriorly, while a combination of axial load and a direct blow (or indirect bending force) fractures the ulna, often with anterior angulation.
*
Hyperextension Mechanism (Bado Type II):
A fall on an outstretched hand with the elbow in hyperextension. This can lead to a posterior dislocation of the radial head and a posteriorly angulated ulnar fracture.
*
Direct Trauma (Bado Type III & IV):
Direct blow to the forearm can result in complex fracture patterns and significant soft tissue disruption, often with lateral or anterior dislocation of the radial head.
The key biomechanical principle in treating Monteggia injuries is that the ulna dictates the stability of the entire forearm and the radial head. Anatomic reduction and rigid internal fixation of the ulna are prerequisites for successful radial head reduction and maintaining its concentric alignment with the capitellum. Failure to restore ulnar length, rotation, or alignment will invariably lead to persistent radial head dislocation or subluxation, causing chronic pain, instability, and premature degenerative changes.
Indications & Contraindications
Indications for Operative Management
In adults, nearly all Monteggia fracture-dislocations require operative management. The inherent instability of these injuries, coupled with the critical need for anatomic alignment of the ulna to restore radial head stability, makes non-operative treatment largely unsuccessful and fraught with complications. The primary indication for surgery is the inability to achieve or maintain an anatomic and stable closed reduction of both the ulnar fracture and the radial head dislocation. This is almost universally the case in adults due to muscle forces, comminution, and soft tissue interposition.
Specific indications include:
*
All Bado Type I, II, III, and IV Monteggia fracture-dislocations in adults.
*
Open Monteggia fractures:
Require immediate surgical debridement and stabilization.
*
Associated neurovascular compromise:
While rare, emergent surgical intervention may be required to address vascular injury or relieve nerve compression.
*
Irreducible radial head dislocation:
If closed reduction of the radial head cannot be achieved after ulnar fixation, open reduction is indicated to address soft tissue interposition (e.g., annular ligament, capsule, muscle).
*
Concomitant injuries affecting stability:
Such as significant coronoid process fractures, which further destabilize the elbow.
Contraindications for Operative Management
Absolute contraindications are rare and typically relate to the patient's overall medical status.
*
Absolute Contraindications:
* Severe systemic comorbidities that preclude safe anesthesia and surgery (e.g., acute myocardial infarction, uncontrolled sepsis). In such scenarios, temporary external fixation or a damage control approach may be considered if life-saving.
*
Relative Contraindications:
*
Active infection at the surgical site:
Requires infection control prior to definitive fixation.
*
Severe soft tissue compromise:
Extensive devitalized tissue or severe swelling may necessitate delayed definitive fixation after soft tissue optimization (e.g., external fixation, serial debridement).
*
Non-reconstructible anatomy:
In very rare, extremely comminuted cases, alternative strategies might be necessary, but every effort is made to restore anatomy.
Operative vs. Non-Operative Indications Table
| Indication Category | Rationale / Description
|
Operative
| Monteggia fracture-dislocation (all Bado types) in adults. The intrinsic instability due to the simultaneous skeletal and soft tissue injury necessitates surgery. |
|
Rare Non-Operative
| Extremely rare. Potentially stable, undisplaced ulnar shaft fractures with a concentrically reduced radial head,
only if
proven stable on dynamic fluoroscopy through full range of elbow motion and forearm rotation, and typically in patients with severe comorbidities where surgery carries unacceptable risk. This scenario is highly uncommon and usually only considered for pediatric injuries. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes and anticipating potential intraoperative challenges in adult Monteggia fracture-dislocations.
Clinical Assessment
- Detailed History: Mechanism of injury, hand dominance, comorbidities, previous elbow injuries.
- Neurovascular Examination: A thorough assessment of motor and sensory function of the median, ulnar, and radial nerves is mandatory. Special attention should be paid to the posterior interosseous nerve (PIN), as a palsy can be present pre-operatively due to traction injury or compartment syndrome. Document all findings meticulously. Assess capillary refill, pulses, and warmth of the hand.
- Soft Tissue Envelope: Evaluate for open wounds, severe swelling, ecchymosis, and potential compartment syndrome. Delaying definitive fixation in the presence of severe swelling or impending compartment syndrome may be necessary, sometimes opting for temporary external fixation.
Imaging Studies
-
Plain Radiographs:
- AP and Lateral views of the entire forearm, including the elbow and wrist: Crucial for diagnosis. The lateral view is essential to assess the relationship of the radial head to the capitellum. A line drawn through the center of the radial head should always bisect the capitellum in all views and positions. Failure to do so indicates dislocation.
- Oblique views: Can help define fracture patterns, especially comminution.
- Contralateral elbow views: Useful for comparison, especially in cases of suspected congenital radial head dislocation or prior injury.
-
Computed Tomography (CT) Scan:
-
Indications:
Highly recommended for complex Monteggia injuries. It provides invaluable detailed information on:
- Fracture morphology of the ulna (comminution, bone loss).
- Presence and extent of radial head or neck fractures (often occult on plain films).
- Coronoid process fractures (critical for elbow stability).
- Articular impaction or osteochondral lesions.
- Identifying intra-articular loose bodies or incarcerated soft tissues preventing reduction.
- 3D Reconstructions: Aid in surgical planning, especially for complex articular involvement.
-
Indications:
Highly recommended for complex Monteggia injuries. It provides invaluable detailed information on:
-
Magnetic Resonance Imaging (MRI):
- Rarely indicated in acute settings unless suspicion for significant ligamentous injury (e.g., severe MCL/LCL tears) persists despite stable fixation of the ulna and radial head. Can also evaluate annular ligament integrity more directly.
Surgical Strategy & Implant Selection
- Classification: Bado classification guides the general approach.
- Approach Selection: Based on the ulnar fracture location and complexity, and the direction of radial head dislocation. Posteromedial, posterior, or combined approaches may be necessary.
-
Plate Selection:
- Ulna: Pre-contoured locking compression plates (LCPs) are generally preferred for adult ulnar shaft fractures due to their enhanced stability in osteopenic bone and comminuted fractures. Plate length should allow at least 6 cortices (3 bicortical screws) proximally and distally to the fracture.
- Radial Head (if fractured): If a radial head fracture is present and reconstructible, small fragment plates (e.g., variable angle LCPs) or headless compression screws may be used. If unreconstructible, prosthetic radial head replacement may be considered (though less common in acute Monteggia and carries specific indications).
- Ancillary Fixation: Kirschner wires (K-wires) for temporary fixation, suture anchors for ligament repair.
- Anticipation of Challenges: Prepare for significant soft tissue stripping, difficulty in reduction (especially in delayed presentations), osteoporotic bone, and potential nerve compromise.
Anesthesia and Patient Positioning
- Anesthesia: General anesthesia is standard. Regional anesthesia (e.g., interscalene or supraclavicular block) can be highly beneficial for post-operative pain management, reducing opioid requirements.
-
Patient Positioning:
- Supine Position: Often preferred, with the arm draped free on a well-padded hand table. This allows for full range of motion assessment (flexion/extension, pronation/supination) and easy access for fluoroscopy. Ensure adequate padding at pressure points.
- Lateral Decubitus Position: Can be used, particularly for posterior approaches to the elbow, providing excellent visualization of the posterior aspect of the ulna.
- Tourniquet: A pneumatic tourniquet on the upper arm is typically applied to minimize blood loss and improve visualization.
- C-arm Access: Essential for intraoperative fluoroscopic confirmation of reduction and fixation. Ensure the C-arm can obtain true AP and lateral views of the elbow and forearm.
Detailed Surgical Approach / Technique
The cornerstone of adult Monteggia fracture-dislocation treatment is anatomical reduction and rigid internal fixation of the ulna, which almost invariably leads to spontaneous reduction of the radial head. If the radial head does not reduce concentrically or remains unstable, direct intervention on the radial head and/or annular ligament is required.
General Principles
- Ulna First: Prioritize stable, anatomical reduction of the ulnar fracture. Restoration of ulnar length, rotation, and alignment is paramount.
- Radial Head Reduction: Once the ulna is fixed, the radial head typically reduces spontaneously. If not, gentle manipulation should be attempted. If still irreducible or unstable, open reduction and repair/reconstruction of the annular ligament are indicated.
- Stability Assessment: Verify concentric radial head reduction and overall elbow stability through a full range of motion and forearm rotation under fluoroscopic guidance.
- Neurovascular Protection: Meticulous dissection and retraction to protect surrounding nerves (especially PIN, ulnar) and vessels.
Surgical Approaches
The choice of incision depends on the fracture pattern and required exposure.
*
Posterior or Posteromedial Approach to the Ulna:
Most common for Bado Type I and II.
*
Incision:
A straight or gently curved posterior incision centered over the ulnar shaft. For proximal ulna, it can extend to the olecranon. For Type I, a posteromedial approach allows better access to anteriorly angulated ulna fractures.
*
Dissection:
The interval between the anconeus and flexor carpi ulnaris (FCU) can be used for the proximal ulna. Distally, the ulna is subcutaneous on its posterior border. Care must be taken to protect the ulnar nerve (in its groove proximally) and the posterior interosseous nerve (PIN), which spirals around the radial neck and enters the supinator. The PIN is generally not at direct risk with a posterior ulnar approach but is vulnerable if dissection extends too far laterally or anteriorly near the radial neck.
*
Anterolateral (Henry) Approach to the Radius:
May be required for open reduction of the radial head or management of associated radial head fractures.
*
Incision:
Longitudinal incision over the anterior aspect of the proximal forearm, between the brachioradialis laterally and the pronator teres/flexor carpi radialis medially.
*
Internervous Plane:
The Henry approach utilizes the interval between the brachioradialis (radial nerve innervation) and the pronator teres/flexor carpi radialis (median nerve innervation). Deep dissection proceeds between the supinator (PIN) and pronator teres (median nerve).
*
Protection:
The PIN is the main concern. It pierces the supinator muscle. Retraction of the supinator muscle should be
anteriorly
to protect the PIN, which lies deep and posterior within the supinator.
Step-by-Step Surgical Technique (Illustrative for Bado Type I)
- Patient Positioning and Prep: Supine on a hand table, tourniquet inflated. Arm prepped and draped to allow full range of motion and fluoroscopic access.
- Incision: A 10-15 cm curvilinear incision centered over the ulnar shaft fracture, extending proximally or distally as needed. For Bado Type I, a posteromedial incision is often advantageous.
-
Dissection:
- Identify the posterior border of the ulna.
- Subperiosteal dissection of muscle attachments (e.g., anconeus, ECU, FCU, brachialis) to expose the fracture site. Minimal stripping is ideal to preserve blood supply.
- If using a posteromedial approach, reflect the FCU and brachialis off the ulna. Identify and protect the ulnar nerve proximally if dissection extends to the olecranon.
-
Ulna Reduction:
- Indirect Reduction: Apply traction to the forearm. Manipulate the fracture fragments to restore length and axial alignment. This is often the most challenging step in comminuted fractures.
- Direct Reduction: Use reduction clamps (e.g., Verbrugge, bone reduction clamps) to achieve anatomical apposition of the fracture fragments. Restore anatomical length, angulation, and rotation. Confirm with fluoroscopy.
-
Ulna Fixation:
- Plate Application: A pre-contoured locking compression plate (LCP) is typically applied to the posterior or posteromedial surface of the ulna. Plate selection (length, width) depends on fracture complexity and bone quality. The plate should span at least 2.5-3 times the length of the fracture fragment.
- Screws: Secure the plate with at least three bicortical screws (or 6 cortices) in each main fragment (proximal and distal to the fracture). For simple transverse or short oblique fractures, interfragmentary lag screws can be used in conjunction with a neutralization plate for absolute stability. For comminuted fractures, relative stability with a bridging LCP is preferred.
- Final Check: Ensure the ulna is anatomically reduced, stable, and the plate is well contoured.
Image caption: Example of internal fixation of the ulnar fracture with a locking compression plate.
-
Radial Head Assessment:
- Once the ulna is rigidly fixed, the radial head should spontaneously reduce into its concentric position relative to the capitellum. Confirm with fluoroscopy in AP and lateral views, ensuring the radial head bisects the capitellum in all positions of elbow flexion and forearm rotation.
-
Open Radial Head Reduction (if necessary):
- If the radial head remains dislocated or subluxated after ulnar fixation, a separate incision is required (usually an anterolateral or Kocher approach).
- Exploration: Identify and clear any interposed soft tissue (e.g., torn annular ligament, joint capsule, brachialis muscle) that is blocking reduction.
- Reduction: Gently reduce the radial head.
- Annular Ligament Repair/Reconstruction: If the annular ligament is torn or avulsed, it must be repaired. Direct primary repair with non-absorbable sutures is often possible. If irreparable or deficient, reconstruction using local tissues (e.g., a strip of triceps fascia, palmaris longus tendon autograft) may be necessary to stabilize the PRUJ.
- K-wire Stabilization (temporary): In highly unstable cases, a temporary trans-articular K-wire from the ulna through the radial head and into the capitellum may be considered for 2-3 weeks, though this limits early motion and carries a risk of stiffness.
-
Management of Radial Head Fractures:
- If an associated radial head fracture is present, assess reconstructibility.
- Reconstructible: Fixation with small headless compression screws or small plates if possible, prioritizing articular congruity.
- Non-reconstructible: In rare cases of severe comminution with joint surface depression in a stable Monteggia construct, primary radial head excision (older, low-demand patients) or radial head arthroplasty (for maintenance of valgus stability) may be considered, but generally avoided in acute Monteggia due to the high risk of valgus instability.
-
Final Stability Check:
- With the ulna fixed and the radial head reduced, gently move the elbow through a full range of flexion, extension, pronation, and supination.
- Re-check stability under fluoroscopy. The radial head should remain concentrically reduced throughout motion.
- Perform a thorough neurovascular assessment.
-
Wound Closure:
- Irrigate wounds thoroughly.
- Achieve meticulous hemostasis.
- Layered closure of deep fascia, subcutaneous tissue, and skin.
- Apply a sterile dressing and a well-padded splint (e.g., sugar tong or posterior splint) with the elbow in 90 degrees of flexion and neutral forearm rotation.
Complications & Management
Despite meticulous surgical technique, Monteggia fracture-dislocations can be associated with various complications, significantly impacting patient outcomes. Proactive recognition and appropriate management are crucial.
Common Complications Table
| Complication | Incidence (Approximate) | Clinical Presentation |
|
*
*Operative Indications
| Repeated or Irreducible dislocation of the Radial Head or Ulna (open Monteggia) |
|
Total Adult Cases
|
All cases
|
|
Monteggia Fracture-Dislocation in Adults (all Bado types) | |
|
|
|
All adult Monteggia fracture-dislocations. |
|
Adult: All Bado Types (I, II, III, IV) |
|
Radial Head Dislocation (Persistent/Recurrent) | 10-30% (depending on series) | Chronic elbow pain, instability, limited forearm rotation (pronation/supination), palpable clunk, progressive osteoarthrosis. |
|
Non-healing ulcer, infection. |
|
The intrinsic instability of the injury in adults. |
| ** |
| ** |
| |
|
Delayed Diagnosis / Presentation:
Many adult Monteggia dislocations present late, often missed initially. Chronic cases (>3-6 weeks) pose additional challenges for reduction due to soft tissue contracture, fibrosis, and early bone consolidation. This may necessitate formal open reduction, release of adhesions, and sometimes osteotomies. |
| |
Reason for Operative Approach
|
| |
|
Primary/All Adult Monteggia Fracture-Dislocations
|
| |
|
Open Monteggia fractures / associated neurovascular compromise.
|
| |
|
Primary/Unstable Monteggia-Equivalent Fractures
|
All cases.
|
| |
|
Primary radial head / neck fracture (Monteggia-equivalent)
|
|
All Monteggia-Equivalent injuries in adults
| Typically requiring open surgery to address skeletal and soft tissue instability. |
|
Management of associated injuries (e.g., radial head fractures, coronoid fractures).
|
|
Management Complications:
Nerve injury (esp. PIN), nonunion/malunion of ulna, persistent radial head dislocation/subluxation, stiffness/loss of motion, heterotopic ossification, infection, delayed union.
Prevention:
Meticulous surgical technique, anatomical reduction of ulna, stable fixation, proper rehabilitation, perioperative antibiotics, early motion.
Salvage:
Revision ORIF, radial head replacement/excision, annular ligament reconstruction, neurolysis, osteotomy, arthrolysis, HO excision. | |
Details of Major Complications and Management
-
Persistent Radial Head Dislocation/Subluxation:
- Cause: This is the most common and critical complication. It's almost always due to inadequate anatomical reduction or unstable fixation of the ulna (malreduction, malalignment, shortening, or rotation). Less commonly, it can be due to irreducible soft tissue interposition (e.g., annular ligament, capsule, pronator quadratus) or an unaddressed radial head fracture block.
- Management: Requires revision surgery. The primary goal is to re-establish anatomical reduction and rigid fixation of the ulna. Intra-articular structures obstructing reduction should be excised (e.g., joint capsule, torn annular ligament). Annular ligament reconstruction (with fascia or tendon graft) may be necessary to maintain reduction, especially if the original annular ligament is irreparable. Temporary K-wire fixation across the PRUJ may be used for a short period (2-3 weeks).
-
Nonunion or Malunion of the Ulna:
- Incidence: Varies with fracture severity, surgical technique, and patient factors (e.g., smoking, comorbidities). Can be 5-10%.
- Clinical Presentation: Persistent pain, deformity, radial head instability, limited forearm rotation.
-
Management:
- Nonunion: Requires revision ORIF, often with plate exchange, bone grafting (autograft or allograft), and re-establishment of a stable mechanical environment.
- Malunion: May require corrective osteotomy of the ulna to restore length, rotation, and angulation, which in turn can resolve radial head issues.
-
Nerve Injury (especially Posterior Interosseous Nerve - PIN):
- Incidence: Can be 5-10%, often neurapraxia due to traction or direct trauma. Iatrogenic injury is also a risk.
- Clinical Presentation: Wrist drop, inability to extend MCP joints of digits, inability to extend thumb, sensory loss over the dorsum of the hand (radial sensory nerve). Painless.
- Management: Pre-operative PIN palsy is typically observed as most are neurapraxic and resolve spontaneously over weeks to months. Post-operative PIN palsy requires immediate evaluation. If a complete palsy exists and there is suspicion of direct transection or impingement (e.g., by hardware), surgical exploration is warranted. Otherwise, observation, splinting, and electrophysiological studies guide management.
-
Elbow Stiffness/Loss of Motion:
- Incidence: Common, varying from mild restriction to severe ankylosis (10-40%).
- Cause: Prolonged immobilization, heterotopic ossification, intra-articular adhesions, capsular contracture.
- Management: Aggressive post-operative physical therapy is the primary prevention and treatment. Dynamic splinting (e.g., dynamic elbow flexion/extension splints) can be beneficial. For recalcitrant stiffness after 6-12 months, surgical arthrolysis (open or arthroscopic) may be considered, but only after fracture union is solid.
-
Heterotopic Ossification (HO):
- Incidence: Can be as high as 20-30% in severe injuries, particularly those with associated head trauma or extensive soft tissue damage.
- Clinical Presentation: Progressive loss of elbow motion, pain, palpable mass.
- Prevention: Prophylactic NSAIDs (e.g., indomethacin) or low-dose radiation therapy (controversial in acute setting, typically reserved for high-risk cases) can be used.
- Management: For symptomatic, mature HO causing functional limitation, surgical excision (osteotomy) is indicated, usually after 6-12 months to allow maturation, with post-operative HO prophylaxis.
-
Infection:
- Incidence: Low (1-5%) with appropriate perioperative antibiotics and sterile technique. Higher in open fractures.
- Clinical Presentation: Localized pain, redness, swelling, warmth, purulent discharge, fever.
- Management: Early detection and aggressive management are key. Deep infections require surgical debridement, hardware removal (if fixation is stable or union achieved), IV antibiotics, and wound care.
-
Post-Traumatic Osteoarthritis:
- Incidence: Long-term complication, highly variable, especially with articular involvement or imperfect reduction.
- Clinical Presentation: Chronic pain, crepitus, progressive loss of motion.
- Management: Conservative management (NSAIDs, activity modification, injections). For severe, debilitating OA, surgical options include arthroscopy, arthroplasty (total elbow arthroplasty, radial head replacement), or arthrodesis (rare).
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful Monteggia treatment, aiming to restore pain-free range of motion, strength, and function while protecting the surgical repair. The protocol must be tailored to the individual patient, the stability of the fixation, and the extent of associated soft tissue injuries. Early, controlled motion is generally favored to prevent stiffness, but not at the expense of fracture healing or radial head stability.
Phase 1: Protection and Early Motion (0-2 weeks post-op)
- Goals: Reduce pain and swelling, protect surgical repair, initiate controlled early motion.
-
Immobilization:
- A well-padded posterior splint or hinged elbow brace is typically applied in a comfortable position (e.g., 90 degrees elbow flexion, neutral forearm rotation) for initial protection.
- The duration of strict immobilization is generally minimal, often just until initial pain and swelling subside (e.g., 3-7 days).
-
Range of Motion (ROM):
- Elbow: Begin with gentle active-assisted and passive range of motion (AAROM/PROM) within a safe arc determined by surgeon (e.g., 30-100 degrees flexion, neutral pronation/supination). Avoid excessive terminal extension or pronation/supination that could stress the annular ligament repair or ulnar fixation.
- Forearm Rotation: Gentle supination and pronation should be initiated cautiously, particularly if the annular ligament was repaired/reconstructed. Some surgeons prefer to limit early aggressive pronation/supination to avoid radial head redislocation.
- Adjacent Joints: Active ROM for the shoulder, wrist, and hand to prevent stiffness in these areas.
- Pain and Edema Management: Elevation, ice, analgesics.
- Weight Bearing: Non-weight-bearing for the affected limb.
Phase 2: Progressive Motion and Light Strengthening (2-6 weeks post-op)
- Goals: Gradually increase elbow and forearm ROM, initiate light strengthening.
- Brace/Splint: Wean from the static splint. A hinged elbow brace may be used for protection during activities or for sleep, progressively increasing the allowable range of motion.
-
Range of Motion:
- Continue progressive AAROM/PROM, aiming for near full elbow flexion and extension.
- Gradually increase active pronation and supination, ensuring stability of the radial head.
- Gentle mobilization techniques as tolerated.
-
Strengthening:
- Begin with isometric exercises for the elbow flexors/extensors and forearm rotators.
- Light resistive exercises can be introduced for grip strength, wrist flexion/extension.
- Avoid direct resistance across the elbow joint or heavy lifting.
Phase 3: Strengthening and Functional Return (6-12+ weeks post-op)
- Goals: Restore full pain-free ROM, achieve full strength, return to normal activities.
- Brace/Splint: Discontinue brace when adequate stability and strength are achieved, and radiographic union is progressing.
- Range of Motion: Continue to work on any residual ROM deficits. Dynamic splinting may be considered for persistent stiffness.
-
Strengthening:
- Progressive resistive exercises for all major muscle groups of the shoulder, elbow, forearm, and hand.
- Concentric and eccentric loading.
- Focus on functional tasks.
-
Activity Progression:
- Gradual return to light daily activities.
- Avoid heavy lifting, pushing, pulling, or contact sports until radiographic union is complete and strength is fully recovered (typically 3-6 months, sometimes longer for high-demand activities).
- Sport-specific or work-specific rehabilitation can begin with guidance.
Key Considerations for Rehabilitation
- Surgeon Communication: Close communication between the surgeon and therapist is vital to ensure the protocol aligns with the stability of the fixation and any intraoperative findings.
- Pain Guidance: Exercises should be performed within a pain-free or tolerable range. Significant pain indicates overstressing the repair.
- Monitoring for Complications: Watch for signs of radial head instability (recurrent clunking, pain), nerve symptoms, or developing heterotopic ossification (increasing stiffness).
- Delayed Union/Nonunion: If delayed union or nonunion is suspected, rehabilitation may need to be modified or paused.
- Patient Education: Emphasize the importance of adherence to the protocol and the potential for long-term complications if not followed.
Summary of Key Literature / Guidelines
The treatment of adult Monteggia fracture-dislocations has evolved significantly, with a strong consensus favoring operative management. The primary principles are well-established and supported by clinical evidence.
Core Principles from Literature
-
Anatomic Reduction of the Ulna is Paramount:
Numerous studies underscore that the key to successful treatment of Monteggia injuries is the anatomic reduction and rigid internal fixation of the ulnar shaft fracture. This often leads to spontaneous and stable reduction of the radial head. Failure to restore ulnar length, alignment, or rotation will result in persistent radial head instability.
- Bado's original description (1967) highlighted this relationship.
- Ring et al. (1998) and Jupiter et al. (1994) emphasized that persistent radial head dislocation post-operatively is almost always due to inadequate ulnar reduction, not primary radial head pathology or annular ligament injury alone.
- Role of Annular Ligament: While the annular ligament is frequently torn in Monteggia injuries, its repair or reconstruction is typically only necessary if the radial head remains unstable after anatomical ulnar fixation. Primary repair of the annular ligament is common in pediatric Monteggia but less frequently required as a primary procedure in adults if ulnar alignment is restored. However, for irreducible dislocations or cases with persistent instability, direct repair or reconstruction is critical.
- Radial Head Fractures: When associated radial head fractures are present, their management is crucial. Reconstructible fractures should be internally fixed. Unreconstructible radial head fractures in the context of an acute Monteggia are challenging. While historically radial head excision was considered, it is now generally discouraged in the acute setting due to the risk of severe valgus instability and proximal radial migration, especially in younger, active adults. Radial head arthroplasty may be considered in selected cases to restore mechanical stability, particularly in older patients with low demand, but its role in acute Monteggia is not universally accepted compared to its use in terrible triad injuries.
- Open Reduction of Radial Head: If the radial head cannot be reduced closed after stable ulnar fixation, open reduction is necessary to clear interposed soft tissue (e.g., annular ligament, joint capsule, muscle).
-
Outcomes:
Good to excellent results are reported in 70-90% of adult Monteggia cases treated with timely and appropriate open reduction and internal fixation. Factors associated with poorer outcomes include:
- Delayed presentation/treatment (>3-6 weeks).
- Severe comminution of the ulna.
- Associated radial head or coronoid fractures.
- Presence of neurological injury.
- Post-operative complications (e.g., stiffness, nonunion, redislocation).
Recent Literature & Guidelines
- AO Principles: Current surgical guidelines generally adhere to AO principles of internal fixation, emphasizing anatomical reduction, stable fixation, preservation of blood supply, and early, safe mobilization. For ulnar shaft fractures, dynamically contoured locking compression plates (LCPs) are often the preferred implant due to their robust fixation capabilities, particularly in comminuted or osteopenic bone.
- Role of CT Imaging: Modern practice increasingly utilizes pre-operative CT scans, especially for complex or comminuted Monteggia injuries, to precisely delineate fracture morphology, identify subtle radial head or coronoid fractures, and aid in surgical planning.
- Chronic Monteggia: The treatment of chronic Monteggia fracture-dislocations (presenting several weeks or months after injury) is more challenging. It often involves ulnar osteotomy to restore length and alignment, open reduction of the radial head, and annular ligament reconstruction. The results for chronic cases are generally inferior to those for acute repairs.
- Prophylaxis for HO: Given the potential for heterotopic ossification, especially in high-energy injuries, some surgeons consider prophylactic measures like NSAIDs (e.g., indomethacin) or low-dose radiation, particularly in patients with additional risk factors (e.g., head injury).
In conclusion, the optimal treatment for adult Monteggia fracture-dislocations is prompt, anatomical open reduction and rigid internal fixation of the ulna, followed by careful assessment and management of the radial head and any associated ligamentous or bony injuries. A well-structured post-operative rehabilitation program is essential to achieve excellent long-term functional outcomes.
You Might Also Like