Deep Hand Infections: Clinical Presentation, Surgical Anatomy, and Management Strategies
Key Takeaway
Deep hand infections are critical orthopedic emergencies involving structures below the skin, demanding prompt diagnosis and aggressive surgical and medical management. They often present with 'tracking pain' away from superficial sites, indicating spread within fascial compartments or tendon sheaths, and require a thorough understanding of hand anatomy to prevent devastating functional compromise.
Introduction & Epidemiology
Deep hand infections represent a critical orthopedic emergency, demanding prompt and accurate diagnosis followed by aggressive surgical and medical management to prevent devastating functional compromise, limb loss, or even mortality. Unlike superficial infections, deep hand infections involve structures below the skin and subcutaneous tissue, often within fascial compartments, tendon sheaths, or joints. The seemingly innocuous presentation of pain originating near the nail, yet exhibiting a propagation pattern away from this superficial site, serves as a crucial clinical indicator for deeper, often more insidious processes. This "tracking pain" suggests involvement of fascial planes, tendon sheaths, or compartmental spread, necessitating a heightened index of suspicion.
The epidemiology of deep hand infections is diverse, influenced by various factors including occupation, comorbidities, and mechanism of injury. Penetrating trauma (e.g., splinters, industrial accidents, animal or human bites), intravenous drug use, and spread from neglected superficial infections (e.g., paronychia, felon) are common antecedents. Risk factors for severe or rapidly progressive infections include diabetes mellitus, peripheral vascular disease, immunosuppression (HIV, organ transplant recipients, chronic corticosteroid use), chronic renal failure, and advanced age. While less common than superficial infections, deep hand infections carry significantly higher morbidity. The incidence of specific types varies, with flexor tenosynovitis being a well-recognized entity often presenting with characteristic Kanavel's signs, while deep fascial space infections (e.g., midpalmar, thenar) may present more subtly. The polymicrobial nature of many hand infections, often involving Staphylococcus aureus (including MRSA), Streptococci, and Gram-negative organisms, underscores the necessity for broad-spectrum empiric antibiotic coverage.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate surgical anatomy of the hand is paramount for the diagnosis and effective management of deep hand infections. The hand's complex arrangement of tendons, nerves, vessels, and fascial planes dictates the potential pathways for infection spread and informs surgical drainage strategies.
Anatomical Compartments and Fascial Spaces:
-
Flexor Tendon Sheaths (Fibro-osseous Canals):
These synovial-lined sheaths encase the flexor tendons from the metacarpal heads to the distal phalanges.
- The thumb and small finger sheaths often communicate directly with the radial and ulnar bursae, respectively, extending into the forearm (Parona's space), creating pathways for widespread infection.
- The index, middle, and ring finger sheaths typically terminate at the metacarpal necks. However, communication with the central palmar space is possible through the lumbrical canals.
- Infection within a sheath (pyogenic flexor tenosynovitis) is a surgical emergency, characterized by Kanavel's four cardinal signs: uniformly swollen digit, held in slight flexion, exquisite tenderness along the flexor sheath, and severe pain with passive extension of the digit.
-
Central Palmar Space:
Located between the flexor tendons and metacarpals dorsally, and the palmar aponeurosis and superficial arch volarly. It is subdivided into:
- Midpalmar Space: Bounded volarly by the flexor tendons and lumbricals of the middle, ring, and small fingers, and dorsally by the interossei and metacarpals. It contains the neurovascular bundles for these digits.
- Thenar Space: Located radial to the midpalmar space, between the adductor pollicis dorsally and the flexor pollicis brevis and abductor pollicis brevis volarly. It contains the flexor pollicis longus tendon sheath.
- Thenar Eminence: Contains the thenar muscles. Infections here can spread to the thenar space.
- Hypothenar Eminence: Contains the hypothenar muscles. Infections here can spread to the hypothenar space.
- Web Spaces (Collar-Button Abscess): These are triangular spaces between the fingers, containing the lumbricals and digital neurovascular bundles. Infection can track from the palmar aspect, perforating the palmar aponeurosis to present dorsally, creating a "collar-button" configuration.
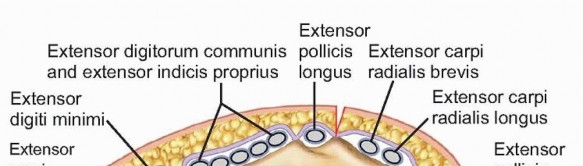
- Dorsal Subcutaneous Space: Superficial to the extensor tendons, this space is often involved in cellulitis or abscesses due to its laxity.
- Dorsal Subaponeurotic Space: Deep to the extensor tendons and superficial to the metacarpals and interossei. Infections here are less common but can result from direct trauma or spread from deep palmar infections via the lumbrical canals.
- Parona's Space: A deep forearm space volar to the pronator quadratus and dorsal to the flexor digitorum profundus and flexor pollicis longus. It communicates with the radial and ulnar bursae, providing a pathway for infections to extend from the hand to the forearm.
- Joints: Septic arthritis can occur in any hand joint (interphalangeal, metacarpophalangeal, carpometacarpal) from direct inoculation, contiguous spread, or hematogenous seeding.
- Bone: Osteomyelitis can result from direct extension of soft tissue infection or open fractures.
Biomechanical Implications of Infection:
The hand's sophisticated biomechanics are exquisitely sensitive to inflammation and infection.
*
Pain:
Limits active motion, leading to stiffness.
*
Edema:
Increases tissue pressure, compromises microcirculation, and further restricts motion. It contributes to fibrosis and adhesion formation.
*
Tendon Adhesions:
Inflammation within flexor or extensor tendon sheaths or surrounding fascial planes can lead to scar formation, tethering tendons and restricting their gliding. This results in loss of active range of motion.
*
Joint Contractures:
Prolonged immobilization in inappropriate positions, capsular fibrosis, and periarticular scarring can lead to fixed joint deformities. The "intrinsic plus" position (MCP flexion, IP extension) is critical for preventing collateral ligament contractures of the MCP joints.
*
Neurovascular Compromise:
Swelling and pus can compress vital neurovascular bundles, leading to ischemic necrosis or permanent nerve damage (e.g., median nerve compression in severe midpalmar space infection).
*
Tissue Necrosis:
Uncontrolled infection can lead to local tissue death, requiring debridement and potentially resulting in significant soft tissue defects.
Indications & Contraindications
The decision for operative intervention in deep hand infections hinges on a careful assessment of clinical presentation, systemic involvement, and imaging findings. Timely surgical drainage and debridement are paramount for optimal outcomes.
Indications for Operative Intervention:
- Confirmed or Highly Suspected Abscess: Any deep collection of pus, whether in fascial spaces, tendon sheaths, or around joints, requires surgical drainage. Clinical fluctuance, tension, or imaging confirmation (ultrasound, MRI) are key indicators.
- Pyogenic Flexor Tenosynovitis (PFTS): Presence of Kanavel's cardinal signs necessitates emergent surgical exploration and irrigation. Delayed treatment leads to high rates of tendon necrosis and adhesion.
- Septic Arthritis: Purulent effusion within a joint, confirmed by aspiration or imaging, requires irrigation and debridement.
- Osteomyelitis: Involvement of bone, especially if associated with soft tissue infection or sequestrum formation.
- Necrotizing Fasciitis: Rapidly progressive infection with signs of tissue necrosis (e.g., rapidly spreading erythema, bullae, crepitus, severe pain out of proportion to exam) demands immediate, aggressive debridement.
- Deterioration Despite Adequate Non-Operative Management: Worsening symptoms, increasing systemic signs of sepsis, or expanding cellulitis despite appropriate intravenous antibiotics and hand elevation.
- Presence of Foreign Body: If a foreign body is implicated in the infection, it often requires surgical removal.
- Compromised Neurovascular Status: Signs of vascular insufficiency or acute nerve compression due to swelling and infection.
- Specific Deep Space Infections: Thenar, midpalmar, hypothenar, and web space abscesses.
Contraindications for Operative Intervention:
Absolute contraindications are exceedingly rare in the context of deep hand infections, given the potential for rapid progression and severe morbidity. Most "contraindications" are relative and pertain to patient stabilization prior to surgery rather than deferring surgery altogether.
*
Localized Cellulitis Without Abscess:
If there are no signs of pus collection, fluctuance, or deep space involvement, and the patient is responding rapidly to empiric intravenous antibiotics with clinical improvement, observation and continued medical management may be appropriate.
*
Unstable Medical Status:
A patient in severe septic shock, impending cardiac arrest, or uncontrolled coagulopathy may require medical stabilization and resuscitation prior to surgical intervention. However, the underlying infection often drives the instability, making surgical source control a critical part of stabilization once the patient can tolerate anesthesia.
*
Known Non-Infectious Etiology:
If the clinical picture suggests an inflammatory process (e.g., gout, inflammatory arthritis, allergic reaction) rather than bacterial infection, surgical drainage would be inappropriate.
Summary of Operative vs. Non-Operative Indications
| Feature | Operative Indication | Non-Operative Indication |
|---|---|---|
| Clinical Presentation | Fluctuance, severe pain with passive motion (Kanavel's signs), severe functional impairment, tense swelling, rapidly spreading erythema, systemic signs of sepsis | Localized cellulitis without fluctuance, mild pain, stable systemic status |
| Pus/Abscess | Present or highly suspected in deep space, tendon sheath, or joint (clinical or imaging) | Absent |
| Infection Type | Deep space infection (thenar, midpalmar, web), pyogenic flexor tenosynovitis, septic arthritis, osteomyelitis, necrotizing fasciitis | Superficial cellulitis, early paronychia (without abscess or deeper spread) |
| Response to ATB | No improvement, worsening symptoms/signs, or new systemic involvement despite appropriate IV antibiotics for 24-48 hours | Rapid and sustained improvement with appropriate empiric oral or IV antibiotics |
| Imaging Findings | Abscess collection, gas in tissues, joint effusion with synovial thickening, cortical erosion/osteolysis, foreign body | Soft tissue edema only, no discrete collections, normal joint/bone structure |
| Systemic Status | Febrile, tachycardic, hypotensive, leukocytosis with left shift, organ dysfunction, signs of sepsis | Afebrile, stable vital signs, normal or mildly elevated WBC |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is crucial to optimize outcomes and minimize complications in deep hand infections. This encompasses thorough diagnostic workup, patient stabilization, and precise intraoperative setup.
Diagnostic Workup:
-
History and Physical Examination:
- Detailed History: Mechanism of injury (puncture, bite, laceration), duration of symptoms, previous treatments, allergies, comorbidities (especially diabetes, immunosuppression), intravenous drug use.
- Focused Hand Exam: Assess for Kanavel's signs, point tenderness, fluctuance, swelling patterns (digit vs. palm vs. dorsum), skin changes (erythema, blistering, crepitus), neurovascular status (capillary refill, sensation, motor function), and range of motion (active and passive). Document the "tracking pain away from the nail" if present.
- Systemic Signs: Fever, tachycardia, hypotension, lymphangitis, lymphadenopathy.
-
Laboratory Studies:
- Complete Blood Count (CBC) with differential: Leukocytosis, left shift.
- Inflammatory Markers: Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP) – useful for tracking response to treatment, though often elevated non-specifically.
- Blood Cultures: Obtain for febrile or septic patients; may identify causative organisms.
- Renal and Hepatic Function Tests, Electrolytes: Essential for baseline and monitoring during aggressive antibiotic therapy.
- Glycemic Control: Essential for diabetic patients (HbA1c, fingerstick glucose).
-
Imaging:
- Plain Radiographs (X-rays): Obtain AP, lateral, and oblique views of the hand/digit. Useful for identifying foreign bodies (metallic, some glass), gas in soft tissues (necrotizing infection), evidence of osteomyelitis (cortical erosion, periosteal reaction – late sign), septic arthritis (joint effusion, joint space narrowing, erosions), or fractures.
- Ultrasound (US): Highly valuable in the acute setting. Dynamic, non-invasive, and can be performed at the bedside. Detects fluid collections (abscesses), differentiates cellulitis from abscess, evaluates tendon sheath thickening and fluid, and guides aspiration.
- Magnetic Resonance Imaging (MRI): Gold standard for delineating soft tissue and bone pathology, particularly for subtle deep space infections, early osteomyelitis, or complex anatomy. However, its use is often limited by urgency, cost, and availability, and typically reserved for uncertain diagnoses or failed initial management.
- Computed Tomography (CT): Useful for complex bone involvement, identification of subtle foreign bodies, and delineating complex fascial plane involvement, but generally provides less soft tissue detail than MRI.
Pre-Operative Preparation:
- Intravenous Antibiotics: Initiate broad-spectrum intravenous antibiotics immediately after cultures are obtained, covering common skin flora, Gram-positives (including MRSA), and Gram-negatives, as indicated by the clinical scenario (e.g., human/animal bites require anaerobic coverage). Adjust based on culture and sensitivity results.
- Tetanus Prophylaxis: Administer if indicated based on wound type and patient's vaccination history.
- Fluid Resuscitation and Electrolyte Correction: For septic or dehydrated patients.
- NPO Status: Standard pre-anesthesia protocol.
- Hand Hygiene and Skin Prep: Chlorhexidine or povidone-iodine scrub.
Anesthesia and Patient Positioning:
-
Anesthesia:
- Regional Anesthesia (Axillary or Supraclavicular Block): Often preferred as it provides excellent analgesia and muscle relaxation for an extended period, minimizing systemic effects. Can be combined with conscious sedation.
- General Anesthesia: May be necessary for anxious patients, extensive infections requiring prolonged surgery, or in children.
- Tourniquet: Essential for a bloodless field, which is critical for identifying subtle anatomical planes, necrotic tissue, and neurovascular structures. A pneumatic upper arm tourniquet is typically used, inflated to 250-300 mmHg (or 100 mmHg above systolic BP).
- Patient Positioning: Supine position with the affected arm abducted and externally rotated, resting comfortably on a padded hand table. Ensure the entire upper extremity, from axilla to fingertips, is prepped and draped to allow for extensile incisions if required (e.g., forearm extension for Parona's space involvement).
- Equipment: Magnification loupes (2.5x to 4.5x) are highly recommended for detailed dissection and protection of delicate structures. A variety of small hand instruments, retractors, irrigation solutions, and drains should be readily available.
Detailed Surgical Approach / Technique
The cornerstone of treating deep hand infections is thorough surgical debridement, drainage of purulent collections, and copious irrigation. Incision planning must balance adequate exposure with preservation of vital structures and minimization of functional and cosmetic sequelae. The principle is to follow the infection, open all involved compartments, and leave wounds open for drainage.
General Principles of Incision and Dissection:
-
Incision Placement:
- Follow natural skin creases or lie in the axis of the hand/digit.
- Avoid crossing flexion creases at right angles.
- Ensure extensibility for broader exposure if necessary.
- Avoid creating skin flaps with compromised vascularity.
- Design incisions to protect underlying neurovascular structures.
- Tourniquet: Essential for a bloodless field, aiding in identification of structures and complete debridement.
- Blunt Dissection: Preferable in infected tissues to minimize trauma to surrounding structures, especially nerves and vessels. Use curved scissors or a hemostat.
- Culture and Biopsy: Always obtain tissue samples for Gram stain, aerobic, anaerobic, fungal, and atypical mycobacterial cultures. Biopsy necrotic tissue.
- Debridement: Remove all necrotic, non-viable tissue. Healthy tissue bleeds and contracts.
- Copious Irrigation: Use large volumes of sterile saline solution (e.g., 1-3 liters for a hand infection).
- Wound Management: Infected wounds are never primarily closed. They are packed loosely with moist gauze (e.g., saline-soaked) and left open for secondary intention healing or delayed primary closure after the infection is controlled. Drains (Penrose, small suction drains) may be considered for large cavities or persistent drainage.
Specific Surgical Approaches:
1. Pyogenic Flexor Tenosynovitis (PFTS):
-
Incision:
- Limited Approach: Two short longitudinal incisions (approx. 1 cm each) for each digit: one over the A1 pulley at the MCP flexion crease and another at the DIP flexion crease. The middle phalanx is avoided to prevent injury to the flexor tendons.
- Extensile Approach (for severe cases, necrosis, or delayed presentation): Mid-lateral approach along the non-functional border of the digit (e.g., radial aspect of index, middle, ring fingers; ulnar aspect of thumb and small finger). Avoid the palmar neurovascular bundle. The skin incision is made just volar to the mid-axial line, allowing the neurovascular bundle to fall dorsally during exposure.
-
Technique (Limited Approach):
- Incisions made.
- Carefully open the flexor tendon sheath at both sites, visualizing pus.
- Insert a small catheter (e.g., intravenous catheter, red rubber catheter) into the proximal incision, advanced distally.
- Copiously irrigate the sheath with saline until clear effluent exits the distal incision.
- A small Penrose drain can be threaded through the sheath and secured to allow continuous irrigation or prolonged drainage if severe. Alternatively, the wounds are loosely packed.
-
Technique (Extensile Approach):
- Skin incision, carefully elevating skin flaps.
- Open the flexor tendon sheath along its length, exposing the flexor tendons.
- Inspect tendons for necrosis. Debride any non-viable tissue.
- Copiously irrigate.
- Leave the sheath open. Loosely pack the wound.
2. Deep Palmar Space Infections (Midpalmar, Thenar):
-
Midpalmar Space Abscess:
- Incision: Longitudinal incision in the distal palm, overlying the involved ray(s), following the distal palmar crease, or slightly oblique parallel to the distal palmar crease. Can be extended proximally along a metacarpal, or obliquely to the wrist crease, respecting the superficial palmar arch and digital neurovascular bundles.
-
Technique:
- Incision through skin and subcutaneous tissue.
- Carefully divide the palmar aponeurosis.
- Blunt dissect between the flexor tendons, lumbricals, and digital neurovascular bundles to enter the midpalmar space.
- Follow the pus. Once the abscess is localized, open it widely.
- Debride necrotic tissue, irrigate copiously.
- Leave the wound open, loosely packed.
-
Thenar Space Abscess:
- Incision: Incision along the thenar crease or parallel to the thenar eminence, between the thumb CMC and MCP joints. Avoid the recurrent motor branch of the median nerve (lies approximately halfway between the palmaris longus tendon and the thenar crease).
-
Technique:
- Incision through skin and subcutaneous tissue.
- Bluntly dissect through the thenar muscles, deep to the flexor pollicis brevis and abductor pollicis brevis, but superficial to the adductor pollicis.
- The space lies between the adductor pollicis (dorsally) and the flexor pollicis brevis (volarly).
- Drain and debride, irrigate.
- Leave open, loosely packed.
3. Web Space Abscess (Collar-Button Abscess):
- Incision: Dorsal transverse incision across the web space. A small, separate palmar incision may be required to completely drain the palmar component, or the palmar component can often be reached and drained through the dorsal approach. Avoid injury to the dorsal digital nerves and vessels.
-
Technique:
- Dorsal incision, often extending slightly onto the proximal phalanges.
- Blunt dissection through the dorsal subcutaneous tissue.
- Identify and incise the dorsal extension of the web space, following the pus.
- Carefully probe through the intermetacarpal space to find the palmar extension of the abscess (often through the lumbrical canal).
- Drainage and debridement.
- Leave both dorsal and palmar wounds open (if two incisions were made), loosely packed.
4. Dorsal Subaponeurotic Space Abscess:
- Incision: Longitudinal incision over the dorsum, often parallel to the metacarpals, or a transverse incision distal to the extensor retinaculum.
-
Technique:
- Incision through skin and subcutaneous tissue.
- Carefully dissect superficial to the extensor tendons to avoid injury to the superficial nerves and vessels.
- Incise the deep dorsal fascia (extensor aponeurosis) to enter the space.
- Drain and debride, irrigate.
- Leave open, loosely packed.
5. Septic Arthritis:
- Incision: Small dorsal or mid-lateral incisions over the joint capsule.
-
Technique:
- Open the joint capsule.
- Irrigate the joint copiously with saline.
- Debride any synovium that appears necrotic.
- Consider placing a small drain (e.g., catheter for continuous irrigation) for 24-48 hours.
- Close the skin loosely or leave open depending on the severity of infection and swelling. Immobilize in a functional position.
Post-Debridement Management:
- Dressing: Bulky hand dressing, splinting in the "intrinsic plus" position (wrist in 20-30° extension, MCP joints in 70-90° flexion, IP joints in full extension) to prevent collateral ligament contracture and maintain optimal hand posture.
- Elevation: Keep the hand elevated above heart level to minimize swelling.
- Antibiotics: Continue intravenous antibiotics, adjusting based on intraoperative culture and sensitivity results.
- Serial Debridement: If infection is extensive or tissue necrosis is suspected, plan for staged debridement every 24-48 hours until healthy, granulating tissue is present.
- Delayed Primary Closure / Skin Grafting: Once the wound is clean and free of infection, it may be closed primarily, allowed to heal by secondary intention, or covered with a skin graft or local flap.
Complications & Management
Deep hand infections are associated with a significant risk of complications, largely due to the aggressive nature of the infection, delayed presentation, and the delicate anatomy of the hand. Early recognition and proactive management are crucial for mitigating long-term morbidity.
Common Complications and Their Management:
-
Persistent or Recurrent Infection:
Often due to inadequate debridement, resistant organisms, or underlying patient comorbidities (e.g., immunocompromise, diabetes).
- Management: Re-exploration, repeat incision and drainage, extensive debridement of any remaining necrotic tissue or foreign bodies. Re-evaluate antibiotic coverage based on new cultures and sensitivities. Assess for underlying conditions.
-
Tendon Adhesions and Stiffness:
Inflammation, edema, and subsequent fibrosis can tether tendons within their sheaths or to surrounding tissues, restricting gliding and causing loss of range of motion. Prolonged immobilization also contributes.
- Management: Aggressive and early hand therapy, including active and passive range of motion exercises, dynamic splinting. Tenolysis may be indicated if conservative measures fail and the infection is fully resolved and quiescent (typically 6-12 months post-infection).
-
Septic Arthritis / Osteomyelitis:
Spread of infection to adjacent joints or bone, particularly if primary infection is left untreated or inadequately managed.
- Management: Repeat surgical irrigation and debridement of the joint, synovectomy, and thorough bone debridement if osteomyelitis is present. Prolonged courses of targeted intravenous antibiotics (often 6 weeks or more for osteomyelitis). In severe cases, joint fusion (arthrodesis) or excision arthroplasty may be necessary as salvage procedures.
-
Neurovascular Injury (Iatrogenic):
Damage to nerves or vessels during surgical exploration and debridement, especially in distorted anatomy due to swelling and inflammation.
- Management: Meticulous surgical technique, use of magnification. If recognized intraoperatively, primary repair of nerves or vessels should be attempted. For delayed recognition of nerve injury, secondary neurolysis or nerve grafting may be considered. Vascular injuries may require repair or reconstruction.
-
Tendon Rupture:
Direct enzymatic degradation of tendons by infection, ischemic necrosis, or iatrogenic injury during debridement.
- Management: Early recognition and surgical repair if feasible. In cases of significant tissue loss or poor tissue quality, tendon grafting or tendon transfer may be required after the infection has fully resolved.
-
Amputation:
A rare but devastating outcome for uncontrollable sepsis, extensive tissue necrosis, or severe functional loss.
- Management: Reserved as a last resort when limb salvage is impossible or would result in a non-functional limb with ongoing morbidity.
-
Complex Regional Pain Syndrome (CRPS):
A debilitating pain condition that can follow trauma, surgery, or infection to an extremity.
- Management: Multidisciplinary approach involving pain management specialists, physical and occupational therapists. Treatments include nerve blocks, oral medications, and desensitization therapy. Early mobilization and aggressive edema control are crucial preventive measures.
-
Scarring and Deformity:
Inevitable consequences of deep infection and surgical intervention.
- Management: Scar massage, silicone sheeting, splinting, and reconstructive procedures (e.g., Z-plasty, skin grafts, local flaps) after the infection has settled and scars have matured.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Persistent/Recurrent Infection | 5-15% (varies by infection type and patient factors) | Repeat I&D, radical debridement, targeted IV antibiotics (based on new cultures), removal of foreign bodies, re-evaluation of source control |
| Tendon Adhesions/Stiffness | Common (30-50% for flexor sheath infections) | Early aggressive PT/OT, active/passive ROM, static/dynamic splinting, tenolysis (delayed, after infection quiescence) |
| Septic Arthritis/Osteomyelitis | 5-10% (higher with delayed presentation/immune comp.) | Repeat joint I&D, synovectomy, bone debridement, prolonged IV ATB, arthrodesis, excision arthroplasty (salvage) |
| Neurovascular Injury (Iatrogenic) | Low (<1-2% in experienced hands) | Primary repair (if recognized acutely), neurolysis, nerve grafting/transfer (delayed) |
| Tendon Rupture | Rare, but devastating (e.g., FPL, extensor hood) | Tendon repair, tendon graft, tendon transfer (after infection resolution) |
| Amputation | Very rare (salvage for uncontrollable sepsis/necrosis) | Extensive debridement, vascular reconstruction, flap coverage, prosthetic fitting (if necessary) |
| Complex Regional Pain Syndrome | Variable (5-20% post-trauma/infection) | Multidisciplinary pain management, nerve blocks, PT/OT, pharmacological agents |
| Scarring/Deformity | Common (functional and cosmetic) | Scar massage, silicone, Z-plasty, skin grafts, local/regional flap reconstruction |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as surgical intervention for achieving optimal functional outcomes in deep hand infections. The primary goals are to control edema, prevent stiffness, restore range of motion, and facilitate return to function, all while protecting healing tissues and managing pain.
Immediate Post-Operative Phase (Days 0-3):
- Elevation: The hand must be continuously elevated above heart level (e.g., on pillows or using a sling while ambulating) to minimize swelling and pain.
- Pain Management: Aggressive pain control with analgesics is crucial to allow for early, gentle motion.
-
Immobilization and Splinting:
The hand is typically immobilized in a bulky hand dressing and an intrinsic plus (safe) position splint:
- Wrist in 20-30° extension.
- Metacarpophalangeal (MCP) joints in 70-90° flexion.
- Interphalangeal (IP) joints in full extension.
-
Thumb in abduction and opposition.
This position maintains collateral ligament length at the MCPs and prevents IP joint contractures.
- Wound Care: Regular dressing changes as per surgical protocol, monitoring for signs of persistent infection or complications. Drain management if applicable.
- Antibiotics: Continue intravenous antibiotics as prescribed, transitioning to oral based on clinical improvement and culture sensitivities.
- Early Gentle Motion (Uninvolved Joints): Patients are encouraged to gently move uninvolved joints (e.g., shoulder, elbow, digits not directly affected) to prevent stiffness.
Early Mobilization Phase (Days 3-14, depending on wound stability):
- Hand Therapy Referral: Prompt referral to a specialized hand therapist is essential.
- Edema Control: Continue elevation, retrograde massage, light compression (e.g., Coban wrap once wounds are clean and dry).
- Active Range of Motion (AROM): Initiate gentle, pain-free active range of motion exercises for the involved digits/hand. This may start with tendon gliding exercises for flexor tendon sheaths (hook fist, full fist, straight fist).
- Passive Range of Motion (PROM): Gentle passive range of motion may be introduced by the therapist, being mindful of pain and tissue healing.
- Splinting: Continue intrinsic plus splinting between exercise sessions and at night. Custom-molded thermoplastic splints may be fabricated for better fit and comfort.
- Scar Management: Once wounds are closed and stable, begin scar massage, silicone gel sheeting, or topical agents to minimize hypertrophic scarring and adhesions.
Intermediate Phase (Weeks 2-6):
- Increased Intensity of ROM: Gradually increase the intensity and duration of AROM and PROM exercises.
- Light Strengthening: Begin with light isometric exercises, progressing to therapeutic putty or light resistive bands for intrinsic and extrinsic muscle strengthening.
- Functional Activities: Incorporate light, pain-free functional tasks and activities of daily living (ADLs).
- Dynamic Splinting: Consider dynamic or static progressive splinting if specific joint contractures are developing despite active/passive ROM.
- Desensitization: If nerve irritation or injury occurred, desensitization techniques may be employed.
Advanced Phase (Weeks 6+):
- Maximal Strengthening: Progress to more vigorous strengthening exercises, focusing on grip and pinch strength, and fine motor dexterity.
- Endurance Training: Prepare the hand for sustained activity.
- Return to Activity: Gradually return to work, sports, and recreational activities, with modifications as needed.
- Residual Stiffness/Pain Management: Continue to address any residual stiffness, pain, or functional limitations. Consideration of secondary surgical procedures (e.g., tenolysis, capsulotomy) if non-operative measures fail after sufficient time for tissue maturation (typically 6-12 months).
Key Principles of Rehabilitation:
- Early, Controlled Motion: Balance protection with gradual, controlled mobilization to prevent stiffness and optimize tendon gliding.
- Pain-Free Movement: Exercises should be performed within the patient's pain tolerance.
- Edema Control: Crucial throughout all phases to minimize fibrosis and promote healing.
- Patient Education and Compliance: Thorough education about the recovery process, home exercise programs, and the importance of adherence is vital.
- Multidisciplinary Approach: Close collaboration between the surgeon, hand therapist, and pain management specialist (if needed) ensures comprehensive care.
Summary of Key Literature / Guidelines
Deep hand infections represent a challenging clinical entity, with management guided by fundamental surgical principles and evolving literature. Key themes consistently emphasized across academic publications and professional guidelines include the urgency of diagnosis, aggressive surgical debridement, appropriate antibiotic stewardship, and structured post-operative rehabilitation.
Foundational Principles and Landmark Literature:
- Kanavel's Cardinal Signs (1923): Allen B. Kanavel's seminal description of the four signs of pyogenic flexor tenosynovitis (uniform swelling of the digit, semi-flexed posture, exquisite tenderness along the flexor sheath, and severe pain with passive extension of the digit) remains the clinical cornerstone for diagnosing this critical condition. His work underscored the importance of early intervention to prevent tendon necrosis and digital stiffness.
- Surgical Drainage: The principle of draining pus and debriding necrotic tissue has been consistently championed since the early 20th century. Classic texts by Bunnell, Littler, and Green’s Operative Hand Surgery have meticulously detailed the surgical anatomy and approaches for various deep space infections. These texts highlight the importance of understanding fascial planes and internervous relationships to achieve effective drainage while preserving vital structures.
Current Evidence and Guidelines:
- Early Diagnosis and Intervention: Contemporary literature uniformly stresses that delay in diagnosis and treatment significantly increases morbidity, including increased rates of stiffness, tendon damage, and potential amputation. Imaging modalities such as ultrasound and MRI have enhanced diagnostic accuracy, allowing earlier and more precise localization of abscesses.
-
Antibiotic Stewardship:
- Empiric Coverage: Initial empiric broad-spectrum intravenous antibiotics are critical, targeting common pathogens such as Staphylococcus aureus (including MRSA, given its rising prevalence), Streptococci, and often Gram-negative bacilli or anaerobes depending on the mechanism (e.g., animal/human bites, immunocompromised host). Guidelines often recommend agents like vancomycin for MRSA coverage, combined with a beta-lactamase inhibitor (e.g., piperacillin-tazobactam) or a carbapenem for broader coverage.
- Culture-Guided Therapy: Antibiotic regimens must be adjusted promptly based on Gram stain results and definitive culture and sensitivity reports from intraoperative specimens. The duration of antibiotic therapy varies widely (from 7-14 days for cellulitis/minor abscesses to 4-6 weeks for osteomyelitis) and should be guided by clinical response and inflammatory markers.
- Resistant Organisms: The increasing prevalence of multidrug-resistant organisms (MDROs), particularly MRSA, poses significant challenges. Local antibiograms and institutional guidelines are crucial for guiding empiric therapy.
-
Surgical Technique:
- Thorough Debridement: Complete removal of all necrotic tissue is non-negotiable. This often necessitates leaving wounds open, potentially requiring serial debridement procedures.
- Copious Irrigation: High-volume lavage with sterile saline is a standard practice to reduce bacterial load and remove debris.
- Wound Management: The consensus is against primary closure of infected wounds. Delayed primary closure, secondary intention healing, or skin grafting/flap coverage are employed once the infection is controlled and healthy granulation tissue is present.
-
Rehabilitation Protocols:
- Early Mobilization: Evidence strongly supports early, controlled mobilization as soon as wound stability permits. This prevents stiffness, minimizes tendon adhesions, and promotes functional recovery. Hand therapy specialists are integral to this process, designing individualized programs.
- Intrinsic Plus Position: Immobilization in the intrinsic plus position is a key principle to prevent MCP collateral ligament shortening and maintain optimal hand posture.
- Prognostic Factors: Several factors influence outcomes: delay in presentation, extent of infection at presentation (e.g., presence of tendon necrosis, osteomyelitis), underlying patient comorbidities (e.g., diabetes, immunosuppression), and virulence of the pathogen. Patients with pyogenic flexor tenosynovitis who have tendon necrosis or significant synovial damage at initial surgery have a poorer prognosis for full functional recovery.
In conclusion, the management of deep hand infections, exemplified by the clinical presentation of "tracking pain away from the nail," demands a highly coordinated, multidisciplinary approach. Swift diagnosis, aggressive surgical intervention, targeted antibiotic therapy, and structured hand rehabilitation are the pillars of achieving optimal functional outcomes and minimizing the devastating long-term sequelae inherent to these challenging conditions. Continuous vigilance regarding evolving pathogen resistance patterns and adherence to evidence-based guidelines are essential for every orthopedic surgeon managing hand infections.
You Might Also Like