Paronychia: Comprehensive Surgical Management, Anatomy & Indications
Key Takeaway
Surgical drainage of paronychia is indicated for pus presence, failure of conservative management, subungual abscess, runaround infection, suspected osteomyelitis, or in immunocompromised patients. Understanding the perionychium's anatomy is crucial for accurate localization and optimal intervention, preventing complications and ensuring effective recovery from this prevalent hand infection.
Effective Drainage of Paronychia: A Key to Hand Infection Recovery
Introduction & Epidemiology
Hand infections represent a significant source of patient morbidity, leading to substantial functional deficits and economic burden due to lost time from work. While advancements in medical care and antibiotic therapy have historically reduced the incidence of major hand infections, the re-emergence of serious infections, particularly in vulnerable populations, including those with intravenous drug use, continues to challenge the field of hand surgery.
Paronychia is the most prevalent hand infection, comprising approximately 35% of all hand infections. It is an inflammatory condition involving the nail fold, typically presenting as an infection of the perionychium. Acute paronychia is most commonly caused by bacterial inoculation, predominantly Staphylococcus aureus , often following minor trauma, nail biting, hangnail manipulation, or aggressive manicuring. Chronic paronychia, conversely, is typically multifactorial, involving a combination of irritants, moisture, trauma, and often secondary fungal colonization ( Candida species ).
The principles governing the surgical treatment of paronychia are consistent with the broader management of hand infections: accurate localization of the infection and optimal timing of surgical intervention . Failure to adhere to these principles can lead to prolonged recovery, complications, and permanent functional deficits.
Surgical Anatomy & Biomechanics
A thorough understanding of the perionychium and nail unit anatomy is paramount for effective diagnosis and surgical management of paronychia, minimizing iatrogenic injury.
The
nail unit
comprises several distinct anatomical structures:
*
Nail Plate:
The keratinized structure, protecting the underlying nail bed.
*
Nail Bed:
Consists of two parts:
*
Germinal Matrix:
Located proximally beneath the eponychium, responsible for producing 90% of the nail plate. Injury here can lead to permanent nail dystrophy.
*
Sterile Matrix:
Extends from the germinal matrix to the hyponychium, responsible for the adhesion of the nail plate and contributing to its thickness.
*
Eponychium:
The skin fold covering the proximal nail matrix, forming the cuticle (eponychial fold). Infection under this fold is known as a
runaround infection
or
eponychial abscess
.
*
Paronychium:
The lateral nail folds, which are the skin folds overlying the lateral borders of the nail plate. This is the primary site of acute paronychia.
*
Hyponychium:
The area of skin beneath the free edge of the nail plate, providing a protective seal.
*
Perionychium:
The collective term for all the soft tissues surrounding the nail plate, including the eponychium, paronychium, and hyponychium.
The underlying distal phalanx provides skeletal support. The pulp of the fingertip contains a dense fibrofatty septal network that contributes to the rigidity and sensory function of the fingertip, but also compartmentalizes infections, hindering their spontaneous drainage.
Neurovascular Supply: The digital arteries run along the lateral aspects of the digits, supplying the pulp and nail unit. The dorsal branches of the digital nerves provide sensation to the dorsal skin, including the eponychial and paronychial regions. Meticulous surgical technique is essential to avoid injury to these structures, particularly the digital nerves, which are superficial along the lateral aspects of the digit.
Biomechanics: The intricate relationship between the nail plate and its surrounding soft tissues, combined with the underlying distal phalanx, is crucial for both protection and tactile discrimination. Infection can compromise this delicate balance, leading to pain, swelling, and reduced dexterity. Swelling within the confined spaces of the perionychium can rapidly lead to increased tissue pressure, compromising microcirculation and accelerating tissue necrosis if not promptly relieved.
Indications & Contraindications
The decision for operative versus non-operative management of paronychia hinges on the presence and extent of purulent collection and the stage of infection.
Indications for Operative Drainage:
The cardinal physical sign of an abscess, anywhere in the body, is the presence of a fluctuant mass within an area of inflammation. In the hand, due to the often small amount of pus and the dense tissue planes, an abscess can be difficult to discern by palpation alone. Therefore, other signs like significant pain, erythema, swelling, and localized tenderness, particularly if progressive despite conservative measures, become critical indicators.
- Presence of Pus: Any evidence of a fluctuant collection, visible pus, or frank purulent discharge.
- Failure of Conservative Management: Progressive symptoms (pain, swelling, erythema) despite appropriate antibiotic therapy and warm soaks after 24-48 hours.
- Subungual Abscess: Pus extending beneath the nail plate.
- Runaround Infection (Eponychial Abscess): Pus tracking around the proximal or lateral nail folds, indicating a more extensive collection.
- Impending or Established Osteomyelitis: Suspected or confirmed bone infection of the distal phalanx.
- Immunocompromised Patients: More aggressive approach due to increased risk of rapid progression and complications.
Indications for Non-Operative Management:
Conservative management is appropriate for early-stage infections characterized by cellulitis without an overt abscess.
- Cellulitis Without Abscess Formation: Early erythema, tenderness, and swelling without fluctuance or visible pus.
- Superficial Inflammation: Mild symptoms confined to the nail fold, with no signs of deep or spreading infection.
Contraindications to Surgical Drainage:
Strict contraindications are few, as drainage of pus is generally considered imperative. However, relative contraindications and cautions exist.
- Pure Cellulitis: Incising an area of cellulitis without a localized pus collection risks spreading the infection. This aligns with the principle from the original seed content: "If an infection is incised too early, the surgeon may incise an area of cellulitis and actually cause the infection to spread."
- Severe Coagulopathy: (Relative) Requires careful risk-benefit analysis and correction of coagulation status if possible.
- Extensive Necrosis or Ischemia: May necessitate alternative strategies or more complex debridement.
Table 1: Operative vs. Non-Operative Indications for Paronychia
| Feature | Non-Operative Management (Conservative) | Operative Management (Drainage) |
|---|---|---|
| Infection Stage | Early cellulitis without abscess | Established abscess, subungual pus, runaround infection |
| Clinical Signs | Erythema, mild swelling, tenderness; No fluctuance or visible pus | Fluctuance, visible pus, severe pain, spreading erythema, systemic signs |
| Response to Tx | Resolving with antibiotics + warm soaks | Progressive symptoms despite 24-48h conservative Tx |
| Complications | Low risk if treated early | Impending or established osteomyelitis, significant nail plate damage |
| Patient Status | Immunocompetent, good overall health | Immunocompromised, diabetic, or history of recurrent infections |
| Intervention | Oral antibiotics, warm soaks, elevation, pain control | Incision and drainage, partial/complete nail plate avulsion, debridement |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning ensures an efficient and safe procedure, minimizing risks to the patient and optimizing surgical outcomes.
Patient Evaluation:
- History: Document duration of symptoms, preceding trauma, nail biting habits, previous infections, antibiotic use, and systemic comorbidities (e.g., diabetes, immunosuppression, peripheral vascular disease), which can impact healing.
-
Physical Examination:
- Localization: Precisely identify the area of maximal tenderness, swelling, erythema, and most importantly, fluctuance. Determine if the infection is confined to a single lateral nail fold, involves both lateral folds, or has tracked under the eponychium or nail plate.
- Neurovascular Status: Assess capillary refill and sensation to ensure baseline function and identify any compromise.
- Regional Lymphadenopathy: Check for signs of lymphatic spread (e.g., epitrochlear or axillary lymph node enlargement).
- Systemic Signs: Evaluate for fever, chills, or malaise indicating systemic inflammatory response.
Imaging:
- Plain Radiographs: Anteroposterior, lateral, and oblique views of the affected digit should be obtained if there is concern for osteomyelitis of the distal phalanx, foreign body, or previous trauma. While osteomyelitis is uncommon in acute paronychia, it is a critical consideration in chronic or severe cases.
- Ultrasound: Can be a useful adjunct to confirm the presence and depth of a fluid collection, particularly when fluctuance is equivocal. It can also help differentiate cellulitis from an abscess.
Anesthesia:
-
Digital Block:
The most common and effective method for localized paronychia.
- Technique: Administer 1-2% lidocaine (without epinephrine) or bupivacaine (without epinephrine for longer duration) through a small gauge needle (25-30G) at the base of the digit, targeting the dorsal and volar digital nerves. Four injections are typically given (dorsal-medial, dorsal-lateral, volar-medial, volar-lateral) to achieve complete anesthesia of the digit.
- Epinephrine Controversy: While generally contraindicated in digital blocks due to theoretical risk of digital ischemia, modern literature suggests judicious use in healthy patients may be safe and beneficial for hemostasis, though it remains controversial in the context of infection due to compromised microcirculation. Standard practice remains to avoid epinephrine.
- Bier Block (Intravenous Regional Anesthesia): Reserved for more extensive infections involving multiple digits or when a digital block is insufficient.
- General Anesthesia: Rarely required for isolated paronychia, typically for uncooperative patients, very young children, or highly complex, extensive hand infections.
Tourniquet:
A digital tourniquet (e.g., sterile glove finger, Penrose drain, or specialized digital tourniquet) is applied at the base of the digit to ensure a bloodless field, which is critical for accurate identification of pus and meticulous dissection. The duration of tourniquet use should be minimized (typically < 15-20 minutes for a digital tourniquet).
Patient Positioning & Preparation:
- Positioning: The patient is positioned supine with the affected upper extremity placed on a hand table, ensuring comfort and stability.
- Magnification: Loupe magnification (2.5x to 4.5x) is highly recommended to visualize fine anatomical structures and ensure precise dissection, particularly in the delicate perionychial region.
- Sterile Prep: The entire hand and forearm are prepared with an antiseptic solution (e.g., povidone-iodine or chlorhexidine) and draped in a sterile fashion.
Detailed Surgical Approach / Technique
The surgical approach for paronychia depends on the extent and location of the purulent collection. The goal is complete drainage of pus while preserving the integrity of the nail unit and minimizing long-term sequelae.
Acute Paronychia Drainage:
-
Single Lateral Nail Fold Abscess:
- Initial Incision (often sufficient): A small, longitudinal incision (1-2 mm) is made in the most fluctuant area of the lateral nail fold, parallel to the nail plate, away from the nail bed. This can often be achieved with a #11 scalpel blade, directed slightly upward, away from the germinal matrix.
- Elevation: A fine mosquito hemostat or a blunt-tipped instrument is then gently inserted into the incision and spread to release the pus. Care must be taken to elevate the nail fold from the underlying nail plate without damaging the sterile matrix.
- Irrigation: The cavity is copiously irrigated with sterile saline.
- Wick Placement: A small, non-adherent gauze strip (e.g., 1/4 inch Iodoform gauze or plain gauze) is often placed into the opened space to maintain drainage and prevent premature skin closure. This wick is typically removed in 24-48 hours.
-
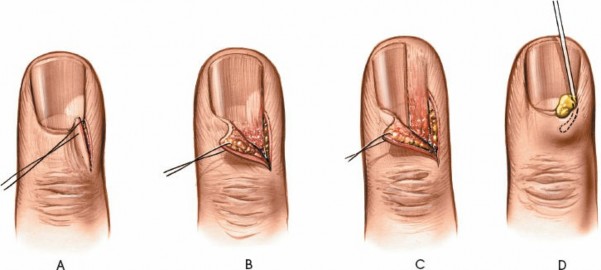
Hockey Stick Incision (Quenu-Kuss Method):
- For more extensive lateral abscesses or when pus has tracked more proximally.
- An incision is initiated in the lateral nail fold, extending proximally and curving around the proximal nail fold (like a hockey stick). This allows for a wider exposure and better drainage of the lateral and potentially proximal eponychial regions.
- This approach risks destabilizing the proximal nail fold, and meticulous closure or specific wound care is needed.
-
Runaround Infection (Eponychial Abscess):
- When pus has tracked underneath the eponychial fold, requiring release of the proximal portion of the nail fold.
- Elevation of Eponychial Fold: The eponychial fold is carefully elevated from the underlying nail plate using a small elevator or the blunt end of a scalpel handle. This often releases the pus.
- Incisions (if necessary): If elevation alone is insufficient, a small longitudinal incision may be made along the lateral borders of the eponychial fold.
- Partial Proximal Nail Plate Excision: If pus is evident beneath the eponychium and extending under the proximal nail plate, a portion of the proximal nail plate (typically 1/4 to 1/3) overlying the germinal matrix may need to be excised or avulsed to allow for drainage. This is achieved by carefully dissecting the eponychial fold proximally to expose the proximal nail plate, then separating the nail plate from the underlying germinal matrix using a small elevator, and excising the involved portion with fine nail scissors. Careful technique is crucial to avoid injury to the germinal matrix.
-
Subungual Abscess:
- Pus localized entirely beneath the nail plate, often visible as a yellowish discoloration through the nail.
- Fenestration: If the abscess is small and very superficial, a small hole can be drilled through the nail plate with a fine drill bit or cautery device (trephination) to allow drainage.
- Partial or Complete Nail Plate Avulsion: If the subungual abscess is extensive, or if the nail plate is significantly undermined by pus, a partial or complete avulsion of the nail plate is indicated. The nail plate is separated from the nail bed using an elevator (e.g., Freer elevator) and then removed with scissors or a hemostat. This allows for thorough debridement and drainage of the underlying nail bed.
Chronic Paronychia Management:
Chronic paronychia often requires a more involved surgical approach, as simple drainage is usually insufficient. The goal is to eliminate the persistently moist environment and remove diseased tissue.
-
Eponychial Marsupialization (e.g., Atasoy technique, Zacherl technique):
- A crescent-shaped excision of the proximal nail fold (eponychium) is performed, removing the diseased tissue and allowing the proximal nail matrix to be exposed. This alters the anatomy, preventing pooling of moisture and promoting healing.
- The wound is typically left open to epithelialize, or sutures may be used sparingly to shape the nail fold.
- This procedure is often combined with partial or complete nail plate removal, and sometimes debridement of hypertrophic granulation tissue from the nail bed.
-
Consideration of Fungal Component: In chronic cases, a fungal culture should be obtained. If positive, systemic antifungal therapy will be necessary in conjunction with surgical debridement.
Post-Drainage Wound Management:
- Packing: If a wick was placed, it is typically removed within 24-48 hours. For larger cavities, a small piece of non-adherent gauze or Gelfoam may be left to allow for continued drainage and prevent premature closure.
- Dressing: A sterile, non-compressive dressing is applied, often incorporating a finger cot.
- Antibiotics: Post-operative oral antibiotics are generally continued for 5-7 days, guided by pre-operative assessment and local resistance patterns. For severe or complicated infections, IV antibiotics might be indicated.
- Elevation and Soaks: Patients are instructed to keep the hand elevated to reduce swelling and to perform regular warm saline soaks (2-3 times daily) once the initial dressing is removed, typically starting after 24 hours.
Key Surgical Principles from Original Seed Content Applied to Paronychia:
- Accurate Localization: Critical. As stated, "Each particular infection has characteristic physical signs, according to the anatomy of the particular compartment that is infected." For paronychia, this means distinguishing between lateral, eponychial, or subungual collections, as each requires a specific drainage approach to prevent incomplete treatment or iatrogenic spread.
-
Timing of the Operation:
"If an infection is incised too early, the surgeon may incise an area of cellulitis and actually cause the infection to spread. In contrast, if pus is left in the hand too long, particularly around the tendon, it may induce irreversible changes in the structures it surrounds." For paronychia, early incision of cellulitis risks spreading bacteria. Delayed drainage, however, increases the risk of:
- Subungual abscess formation: Pus tracking under the nail.
- Osteomyelitis: Involvement of the distal phalanx.
- Chronic paronychia: Leading to nail dystrophy and persistent symptoms.
- Septic arthritis: Though less common, severe paronychia can track proximally to the DIP joint.
- Tendon sheath infection (flexor tenosynovitis): While rare for simple paronychia, severe deep infections originating from the fingertip can track into the flexor tendon sheath.
The correct timing for surgical intervention for paronychia involves acting promptly once a clear abscess is identified or suspected, avoiding incision into mere cellulitis. Ultrasound can be particularly helpful in this regard to confirm the presence of pus.
Complications & Management
Despite appropriate surgical intervention, complications can arise, highlighting the need for careful technique and vigilant post-operative care.
Table 2: Common Complications of Paronychia and Management Strategies
| Complication | Incidence | Description | Salvage Strategies / Management |
|---|---|---|---|
| Recurrence | 5-15% (acute), higher in chronic | Persistence or re-establishment of infection. Often due to incomplete drainage, untreated underlying cause (e.g., nail biting, irritant exposure), or superinfection. | Re-evaluation of the extent of infection; repeat incision and drainage; identification and cessation of underlying contributing factors (e.g., counseling for nail biting); optimization of antibiotic regimen based on culture and sensitivity; consider imaging (ultrasound, X-ray) to rule out deeper collections or osteomyelitis. For chronic cases, more aggressive surgical options like eponychial marsupialization may be required. |
| Nail Dystrophy | 10-25% | Deformity of the nail plate (e.g., ridging, discoloration, thickening, thinning, onycholysis, anonychia) due to germinal matrix injury, chronic inflammation, or scarring. | Prevention is key: careful surgical technique to avoid germinal matrix injury. If mild, may resolve spontaneously. For severe or persistent dystrophy, nail matrix excision (matricectomy) can be considered, but this results in permanent nail loss. Nail cosmetics or prosthetics may be used. Addressing underlying chronic infection is paramount. |
| Osteomyelitis | Rare (<1%), higher in chronic/immunocompromised | Infection spread to the distal phalanx, typically via direct extension from a subungual abscess. | Confirmed via X-ray (late changes), MRI (early changes), or bone scan. Requires aggressive surgical debridement of infected bone and prolonged course of targeted intravenous antibiotics (4-6 weeks). Repeat debridement may be necessary. If extensive bone loss, amputation may be considered as a last resort. |
| Chronic Paronychia | Not applicable (is a condition) | Persistent inflammation of the nail folds for >6 weeks, often associated with multifactorial etiology (moisture, irritants, fungi). | Primarily non-operative (avoiding irritants, keeping dry, topical steroids/antifungals). If refractory, surgical options include eponychial marsupialization, partial or complete nail avulsion, and debridement of granulation tissue. Systemic antifungals may be required for fungal components. Addressing underlying causes like diabetes or occupational exposures is essential. |
| Cellulitis Spread | Rare (due to appropriate Tx) | Inadequate drainage or premature incision leading to wider cellulitis or progression to deeper spaces. | Aggressive systemic antibiotic therapy (often IV initially), hospitalization for close monitoring, and repeat evaluation for abscess formation warranting further drainage. Imaging (ultrasound, MRI) can help delineate extent. |
| Nerve/Vessel Injury | Very rare | Iatrogenic damage to digital nerves or vessels during dissection, leading to numbness, paresthesia, or ischemia. | Prevention through meticulous surgical technique, magnification, and knowledge of anatomy. If nerve transection occurs, primary repair may be considered by a hand surgeon. Vascular injury may require microvascular repair, though typically managed conservatively unless significant ischemia is present. |
| Scarring/Adhesions | Common (mild) | Formation of hypertrophic scars or adhesions limiting nail fold mobility or causing discomfort. | Massage, silicone sheeting, and steroid injections for hypertrophic scars. Surgical release of adhesions may be necessary in severe cases if functional impairment exists. Early mobilization post-operatively can help prevent stiffness and adhesions. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional recovery, preventing stiffness, and ensuring successful resolution of the infection.
Immediate Post-Operative Period (Day 0-3):
- Wound Care: The dressing is kept clean and dry. If a wick was placed, it is typically removed within 24-48 hours by the patient or during the first follow-up visit.
- Elevation: The affected hand should be elevated above the level of the heart continuously to minimize swelling and pain. This can be achieved with a sling or by propping the hand on pillows.
- Pain Management: Oral analgesics (e.g., NSAIDs, acetaminophen, short-course opioids if needed) are prescribed.
- Antibiotics: Oral antibiotics are continued as prescribed, typically for 5-7 days, or longer depending on the severity of infection and culture results.
- Initial Mobilization: Gentle, passive and active range of motion exercises for the unaffected joints of the hand and wrist (e.g., MP and wrist flexion/extension) are encouraged to prevent stiffness, without disturbing the operative site.
Early Rehabilitation Phase (Day 3 - Week 2):
- Dressing Changes and Soaks: Once the initial dressing is removed, patients are instructed to perform regular warm saline soaks (2-3 times daily for 10-15 minutes) to facilitate drainage, clean the wound, and reduce inflammation. Following soaks, a fresh, clean dressing (e.g., non-adherent gauze, finger cot) is applied.
- Active Range of Motion (AROM): Gentle AROM of the affected digit (DIP, PIP, MP joints) is initiated, taking care not to place undue stress on the healing nail fold. The goal is to prevent stiffness, particularly of the DIP joint.
- Scar Management: As the wound heals, gentle massage around the wound edges may be initiated to prevent scar adherence and improve tissue pliability.
- Monitoring: Patients are educated on signs of re-infection (increased pain, swelling, redness, pus) and instructed to contact their surgeon immediately if these occur.
Later Rehabilitation Phase (Week 2 - 6+):
- Progressive Strengthening: As pain subsides and wound healing progresses, gentle grip strengthening exercises (e.g., squeezing soft putty) can be introduced, gradually increasing resistance.
- Desensitization: If nerve irritation or hypersensitivity is present, desensitization techniques (e.g., textures, vibration) may be implemented.
- Nail Care: For cases involving nail plate avulsion, the newly growing nail plate should be protected. Patients are advised on proper nail hygiene and encouraged to avoid nail biting or aggressive manicuring to prevent recurrence.
- Return to Activity: Gradual return to normal activities, avoiding direct trauma or prolonged exposure to moisture, particularly for chronic paronychia cases. Occupational therapy may be beneficial for patients with significant functional deficits or demanding occupations.
- Long-Term Follow-up: Regular follow-up with the surgeon to monitor nail regrowth (if applicable), assess for nail dystrophy, and address any persistent symptoms or complications.
Summary of Key Literature / Guidelines
The management of paronychia is well-established, drawing upon principles of infection control and hand surgery. Key literature and guidelines emphasize early, accurate diagnosis and timely intervention.
-
Acute Paronychia:
- Antibiotic Therapy: For early cellulitis without abscess, oral antibiotics targeting Staphylococcus aureus (e.g., cephalexin, clindamycin, trimethoprim-sulfamethoxazole) combined with warm soaks are the first-line treatment. Studies consistently show high success rates (70-90%) with conservative management in the absence of pus.
- Surgical Drainage: Once an abscess forms, surgical incision and drainage remain the gold standard. A review by Ong et al. (2018) in the Journal of Hand Surgery (European Volume) reiterates the efficacy of simple incision and drainage, often with partial nail plate avulsion for subungual involvement, citing rapid symptom resolution and low recurrence rates when performed appropriately. The precise timing, as noted in the original seed content, is critical to avoid incision of pure cellulitis and to prevent deep tissue damage from prolonged purulence.
- Digital Block Safety: While epinephrine remains largely avoided in digital blocks for infected digits, a systematic review by Thomson et al. (2007) in the Journal of Hand Surgery (American Volume) on the safety of epinephrine in digital blocks, while not exclusively focused on infection, suggests the risk of ischemia is often overstated, though caution remains prudent in already compromised tissue.
-
Chronic Paronychia:
- Multifactorial Etiology: Literature highlights the complex nature of chronic paronychia, often involving Candida species , irritant exposure, and altered nail fold anatomy. Initial management typically involves avoidance of irritants, meticulous hand hygiene, topical antifungals, and steroids.
- Surgical Intervention: For refractory cases, surgical techniques like eponychial marsupialization (e.g., Atasoy technique, Zacherl technique), as described by keys authors such as Zacherl (1987) and Atasoy (1986), are highly effective. These procedures aim to excise the diseased eponychium and prevent the collection of moisture, thereby breaking the cycle of inflammation. Studies, including those by Rigopoulos et al. (2009) in Dermatologic Surgery , demonstrate high cure rates with these approaches.
-
Complications:
- Nail Dystrophy: Literature emphasizes that iatrogenic injury to the germinal matrix during drainage procedures is the primary cause of post-operative nail dystrophy. Meticulous technique and avoiding aggressive curettage of the nail bed are stressed.
- Osteomyelitis: While rare, delayed diagnosis and treatment, particularly in immunocompromised patients, are cited as risk factors for the development of distal phalanx osteomyelitis, as noted by studies in journals like Clinical Orthopaedics and Related Research . Early recognition through imaging and aggressive management with debridement and targeted antibiotics are critical for limb salvage.
Current guidelines from professional organizations, such as the American Society for Surgery of the Hand (ASSH) and the British Society for Surgery of the Hand (BSSH), align with these principles, advocating for a stepwise approach based on clinical presentation, reserving surgical drainage for confirmed abscesses and tailoring the technique to the specific anatomical involvement. The core message remains consistent with the foundational principles of hand infection management: prompt and accurate surgical localization and timely drainage are paramount to prevent morbidity and ensure favorable outcomes.
