Anteromedial Approach to the Elbow: Anatomy, Indications, and Surgical Considerations
Key Takeaway
The anteromedial approach to the elbow is a versatile surgical exposure for conditions like coronoid fractures and medial instability. It provides direct access to the MCL and coronoid process. Critical considerations involve precise knowledge of regional surgical anatomy, especially the ulnar and median nerves, ensuring safe and effective intervention for complex elbow pathologies.
Introduction & Epidemiology
The elbow joint is a complex articulation, critical for upper limb function, facilitating both gross motor activities and fine manipulation. Given its inherent stability conferred by congruent osseous anatomy, strong collateral ligaments, and surrounding musculature, traumatic injuries often result in significant disruption, necessitating precise surgical intervention. The anteromedial approach to the elbow is a versatile and fundamental exposure, providing direct access to the medial collateral ligament (MCL) complex, the coronoid process, the medial humeral condyle and epicondyle, and the anterior capsule.
Historically, challenges in managing complex elbow trauma, particularly coronoid fractures and medial-sided instability, highlighted the need for improved surgical exposures. While arthroscopy has revolutionized the management of many intra-articular pathologies, open approaches remain indispensable for complex fractures, severe ligamentous injuries, and joint reconstruction. The anteromedial approach, either in isolation or as an extensile option, is a cornerstone for addressing injuries involving the medial column and anterior aspects of the joint.
Epidemiologically, coronoid fractures are relatively uncommon in isolation but are frequently associated with elbow dislocations and often contribute significantly to posteromedial rotatory instability. Their incidence is estimated to be between 10-15% of all elbow dislocations, although some series report higher rates. Medial epicondyle fractures are more common in pediatric populations but can occur in adults, often associated with valgus stress injuries or dislocations. Understanding the indications, meticulous surgical technique, and potential complications of the anteromedial approach is paramount for any orthopedic surgeon managing elbow pathology.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is critical for safe and effective utilization of the anteromedial approach.
Osseous Anatomy
The primary bony landmarks include the medial epicondyle, the trochlea, the olecranon, and the coronoid process of the ulna. The coronoid process is a key anterior buttress against posterior subluxation and provides insertion for the anterior bundle of the medial collateral ligament (MCL) and the brachialis muscle. Fractures involving the coronoid can compromise elbow stability. The medial epicondyle serves as the origin for the common flexor-pronator mass and the anterior bundle of the MCL.
Ligamentous Structures
The medial collateral ligament (MCL) complex is the primary static stabilizer against valgus stress. It comprises three distinct components:
*
Anterior Bundle (aMCL):
The strongest and most important stabilizer, taut throughout the range of motion, providing primary resistance to valgus stress from 30° to 120° of flexion. It originates from the anterior aspect of the medial epicondyle and inserts onto the sublime tubercle of the coronoid process.
*
Posterior Bundle (pMCL):
Fans out from the medial epicondyle to the medial olecranon, becoming taut in terminal flexion.
*
Transverse Ligament (Cooper's Ligament):
Connects the medial aspects of the coronoid and olecranon, providing minimal stability.
Damage to the MCL, particularly the anterior bundle, is often associated with elbow dislocations and coronoid fractures, leading to significant instability.
Musculature
The common flexor-pronator mass originates from the medial epicondyle. From superficial to deep, and proximal to distal, these include the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris. Dissection typically involves elevating this entire mass subperiosteally or splitting specific muscles. The brachialis muscle inserts onto the coronoid process and ulnar tuberosity, lying deep to the biceps and providing powerful elbow flexion.
Neurovascular Structures
The principal neurovascular structures at risk during the anteromedial approach are:
*
Ulnar Nerve:
This nerve traverses the posteromedial aspect of the elbow, passing posterior to the medial epicondyle through the cubital tunnel. It is the most frequently injured nerve during medial elbow approaches and must be identified and protected early in the dissection. Its course is highly variable, and it can be found anterior, posterior, or directly over the medial epicondyle depending on arm position and patient anatomy.
*
Median Nerve:
Located anterior to the elbow joint, deep to the bicipital aponeurosis and medial to the brachial artery, it passes between the two heads of the pronator teres. It is typically retracted with the brachialis and flexor-pronator mass.
*
Brachial Artery:
Lies anterior to the joint capsule, medial to the biceps tendon, and closely associated with the median nerve. It bifurcates into the radial and ulnar arteries usually just distal to the elbow joint.
*
Medial Antebrachial Cutaneous Nerve (MACN):
A sensory nerve, it lies subcutaneously and crosses the operative field anterior to the medial epicondyle. It is highly susceptible to iatrogenic injury during skin incision and superficial dissection, leading to dysesthesias or neuromas.

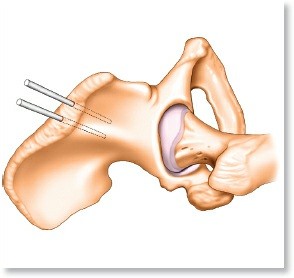
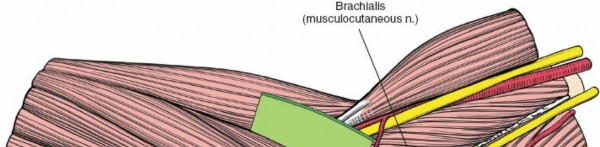
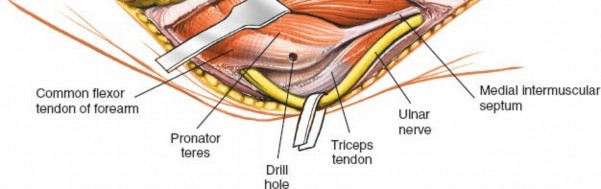
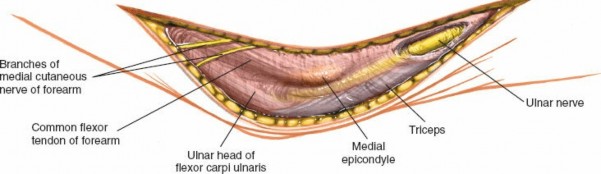
Figure 1: Schematic illustration of the neurovascular structures around the medial aspect of the elbow, highlighting the ulnar nerve (yellow) and median nerve (green) at risk.
Indications & Contraindications
The anteromedial approach offers versatile exposure but its utility must be weighed against alternative approaches, particularly considering the proximity of vital neurovascular structures.
Indications
The primary indications for an anteromedial approach to the elbow include:
*
Coronoid Process Fractures:
Especially Type II and III fractures (according to the Regan-Morrey classification) associated with elbow instability (e.g., varus posteromedial rotatory instability, VPMRI) or elbow dislocations.
*
Medial Collateral Ligament (MCL) Repair/Reconstruction:
Often performed in conjunction with coronoid fracture fixation or for chronic valgus instability.
*
Medial Humeral Condyle/Epicondyle Fractures:
Particularly displaced or intra-articular fractures requiring open reduction and internal fixation (ORIF).
*
Loose Body Removal:
While arthroscopic removal is now common, large or complex loose bodies within the medial compartment may necessitate open removal.
*
Varus Posteromedial Rotatory Instability (VPMRI):
A complex injury involving disruption of the lateral ulnar collateral ligament (LUCL), often a coronoid fracture, and injury to the MCL. The anteromedial approach addresses the coronoid and MCL components.
*
Anterior Capsular Release:
For post-traumatic or post-surgical elbow contractures predominantly affecting flexion.
*
Brachialis Muscle Repair/Advancement:
In cases of chronic instability or specific fracture patterns involving the coronoid.
*
Exploration or Debridement of the Medial Compartment:
For specific septic arthritis cases or tumor resections.
Contraindications
- Isolated Lateral Compartment Pathology: The anteromedial approach provides poor direct access to the lateral side of the joint. Routine exploration of the lateral compartment is better served by lateral or posterior approaches. While a joint dislocation can facilitate lateral access, it increases surgical morbidity.
- Active Infection: Unless the approach is specifically for débridement, active infection generally contraindicates elective ORIF.
- Severe Soft Tissue Compromise: Extensive skin damage, burns, or crush injuries on the medial aspect may preclude this approach.
- Specific Fracture Patterns: Some complex comminuted distal humeral fractures may be better addressed via a posterior olecranon osteotomy approach for comprehensive exposure.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Coronoid Fractures | Displaced Type II/III (Regan-Morrey) causing instability; associated with elbow dislocation or VPMRI. | Minimally displaced Type I (tip avulsion) fractures; stable elbow despite coronoid involvement (rare, requires careful assessment); medically unfit for surgery. |
| Medial Condyle/Epicondyle Fractures | Displaced intra-articular fractures; open fractures; entrapped epicondyle; significant valgus instability. | Minimally displaced, stable extra-articular fractures (e.g., nondisplaced medial epicondyle in adults); avulsion fractures without instability; isolated stress fractures without displacement. |
| MCL Injuries | Acute, complete rupture with gross valgus instability; chronic symptomatic valgus instability; associated with VPMRI. | Partial tears without significant instability; stable isolated MCL injuries often heal with conservative management (bracing, activity modification); patients medically unfit for surgery. |
| Loose Bodies | Symptomatic, recurrent locking/catching; large loose bodies; those causing articular damage. | Asymptomatic loose bodies; very small, non-impinging loose bodies; loose bodies amenable to arthroscopic removal (often preferred if technically feasible). |
| Elbow Contractures | Significant loss of functional range of motion (typically <100° arc of motion); failed conservative therapy. | Mild contractures with adequate functional range of motion; contractures early in post-injury phase where conservative stretching and therapy may still be effective; patients non-compliant with rehabilitation or with medical contraindications to surgery. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for maximizing exposure and minimizing iatrogenic injury.
Pre-Operative Planning
-
Imaging Review:
- Standard Radiographs: AP, lateral, and oblique views of the elbow are essential.
- Computed Tomography (CT) Scan: Crucial for complex fractures, especially coronoid and medial condyle fractures. A 3D reconstruction provides invaluable information regarding fracture morphology, displacement, comminution, and articular involvement. This aids in templating reduction maneuvers and implant selection.
- Magnetic Resonance Imaging (MRI): Useful for assessing associated ligamentous injuries (MCL, LUCL), capsular tears, and soft tissue damage, particularly in cases of instability without clear fracture.
- Implant Selection: Based on fracture pattern, consider small fragment plates (1.5mm, 2.0mm, 2.4mm), lag screws, K-wires, and suture anchors for ligamentous repair. Ensure a variety of lengths and types are available.
- Tourniquet: Plan for an upper arm tourniquet.
- Neurophysiology: Consider intraoperative neuromonitoring (e.g., EMG for ulnar and median nerves) in complex cases or revision surgery, though its routine use is debated.
- Patient Education (Surgeon-to-surgeon): Discuss risks and benefits with the patient, including potential for nerve injury, stiffness, and the need for rehabilitation.
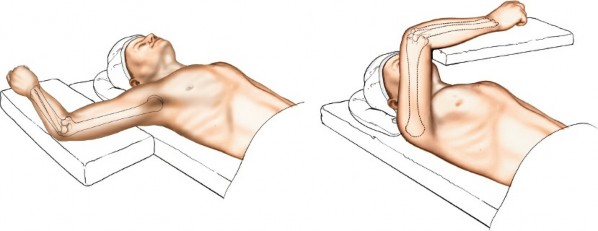
Patient Positioning
The patient is typically placed in the supine position on the operating table. The affected arm can be positioned in one of two main ways:
-
Arm Supported on an Arm Board:
- The arm is abducted to 90 degrees and supported on a radiolucent arm board or hand table attached to the operating table.
- The shoulder is fully externally rotated, and the elbow is flexed to 90 degrees. This maneuver brings the medial epicondyle and the surgical field anteriorly, facilitating direct access.
- The arm board should be securely padded and allow for full pronation and supination of the forearm, as well as extension and flexion of the elbow during the procedure for dynamic assessment.
- This position is generally preferred for broader access and ease of maneuverability.

Figure 2: Patient positioned supine with the arm abducted and supported on an arm board. The shoulder is externally rotated to bring the medial epicondyle anteriorly. -
Arm Across the Chest (Flexed Shoulder and Elbow):
- The patient’s shoulder is flexed, and the elbow is also flexed, bringing the forearm to lie across the patient's chest or face.
- This position provides excellent exposure of the medial aspect of the elbow, often allowing for easier access to the olecranon fossa and posterior structures if an extensile approach is needed.
- However, it typically requires an assistant to maintain the arm's position and can restrict freedom of movement, particularly for intra-operative imaging.
- Padding is crucial at the axilla and elbow to prevent pressure injuries.

Figure 3: Alternative positioning with the arm flexed across the chest, exposing the medial elbow. An assistant is usually required to maintain this position.
Irrespective of the chosen position, ensure:
*
Sterile Prep and Drape:
The entire upper extremity from the shoulder to the hand should be prepped and draped to allow for full range of motion.
*
Tourniquet Application:
A pneumatic tourniquet is applied to the proximal arm.
*
Pressure Point Padding:
All pressure points are meticulously padded.
Detailed Surgical Approach / Technique
The anteromedial approach requires precise anatomical dissection to optimize exposure while safeguarding critical neurovascular structures. The following describes a systematic, step-by-step technique.
1. Incision
A curvilinear skin incision is made, centered over the medial epicondyle. It typically starts approximately 5-7 cm proximal to the medial epicondyle, curves anteriorly over the epicondyle, and then extends distally along the medial aspect of the forearm for another 5-7 cm. This design provides ample exposure and allows for extensibility both proximally and distally if required.

Figure 4: Proposed curvilinear skin incision for the anteromedial approach, centered over the medial epicondyle.
2. Superficial Dissection and Medial Antebrachial Cutaneous Nerve (MACN) Identification
- Carefully incise the skin and subcutaneous tissue.
- The medial antebrachial cutaneous nerve (MACN) runs subcutaneously and crosses the operative field anteriorly. It is highly variable in its course and can be injured. Identify this nerve and protect it by either gently retracting it or dissecting its branches. Dissecting parallel to the nerve's course can help minimize injury.
- Ligate and cauterize any superficial veins encountered.

Figure 5: Superficial dissection demonstrating identification and protection of the medial antebrachial cutaneous nerve (arrow).
3. Ulnar Nerve Identification and Protection
This is a critical step. The ulnar nerve is typically identified posterior to the medial epicondyle within the cubital tunnel.
* Palpate the ulnar nerve behind the medial epicondyle.
* Carefully unroof the cubital tunnel by incising the cubital tunnel retinaculum (Osborne's ligament).
* Trace the ulnar nerve proximally and distally, ensuring it is free of any constrictions. Mobilize it gently.
* The ulnar nerve should be isolated, protected with a vessel loop or Penrose drain, and gently retracted either anteriorly or posteriorly, depending on the desired exposure and stability of the nerve. Prophylactic anterior transposition can be considered if significant soft tissue work is anticipated in its vicinity or if it appears unstable after mobilization, though it is not always necessary. Excessive stretch or aggressive retraction must be avoided.
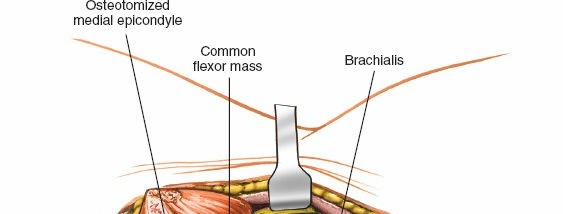
Figure 6: Isolation of the ulnar nerve (held by vessel loop) within the cubital tunnel, following incision of Osborne's ligament.
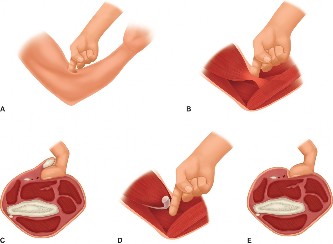
4. Exposure of the Common Flexor-Pronator Origin
- Once the ulnar nerve is protected, attention is turned to the common flexor-pronator mass originating from the medial epicondyle.
- The preferred approach is typically a subperiosteal elevation of the entire common flexor-pronator mass from the medial epicondyle. This provides a single, robust flap that can be retracted anteriorly.
- Incise the fascia over the origin of the pronator teres and flexor carpi radialis.
- Using a Cobb elevator or similar instrument, carefully elevate the entire flexor-pronator mass subperiosteally from the medial epicondyle and the supracondylar ridge proximally. This dissection is carried distal to the joint line.
- Alternatively, the fascia between the pronator teres and brachialis can be incised. The median nerve lies deep to the pronator teres, and the brachial artery lies just medial to the median nerve and anterior to the brachialis. Retract the median nerve and brachial artery anteriorly along with the flexor-pronator mass.
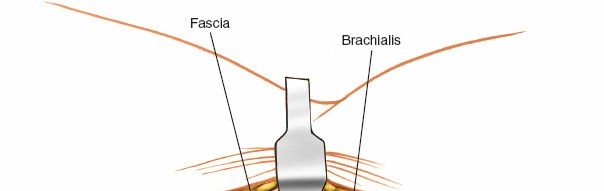
Figure 7: Subperiosteal elevation of the common flexor-pronator mass from the medial epicondyle. The ulnar nerve is retracted posteriorly.
5. Identification of Median Nerve and Brachial Artery
- With the flexor-pronator mass reflected anteriorly and distally, the median nerve and brachial artery come into view, lying directly on the anterior joint capsule and the brachialis muscle.
- Carefully identify these structures and protect them with gentle anterior retraction using a Langenbeck or similar broad retractor. Avoid excessive tension.

Figure 8: Deep dissection revealing the median nerve (white arrow) and brachial artery (black arrow) after retraction of the flexor-pronator mass.
6. Joint Capsule Exposure and Arthrotomy
- After neurovascular protection, the anterior joint capsule and the brachialis muscle are exposed.
- The joint capsule is incised longitudinally, parallel to the long axis of the humerus, allowing access to the medial compartment of the elbow.
- The coronoid process, trochlea, and medial articular surface are now accessible.
- For fractures of the distal humerus, further subperiosteal elevation of the brachialis muscle may be performed to expose the anterior surface of the distal humerus.
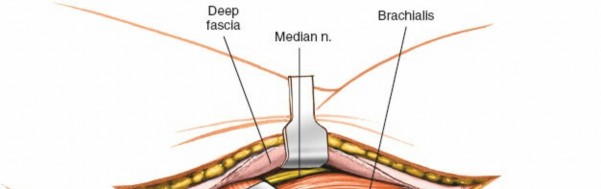
Figure 9: Longitudinal incision of the anterior joint capsule (indicated by dashed line) to enter the medial compartment of the elbow joint.
7. Accessing Specific Structures
Coronoid Process Fractures
- Once the joint is open, the coronoid process is directly visible.
- Reduce the fracture under direct visualization. For small tip fractures (Regan-Morrey Type I), suture repair of the MCL (which inserts on the sublime tubercle) may be sufficient.
- For larger fragments (Type II/III), fixation often involves lag screws, buttress plates (e.g., small fragment T-plate or specific coronoid plates), or suture lasso techniques.
- A small buttress plate can be placed on the anteromedial aspect of the coronoid. Screws are directed into the ulna, ensuring they do not penetrate the joint or impinge on the trochlea.
- In cases of VPMRI, the anteromedial approach allows for fixation of the coronoid and repair of the MCL. The lateral aspect of the joint (LUCL repair) often requires a separate lateral approach or elbow dislocation through the joint for better access.

Figure 10: View into the joint showing a coronoid fracture fragment. The dashed line indicates potential placement for a buttress plate.
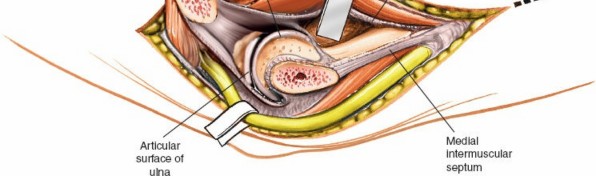
Figure 11: Reduction and provisional fixation of a coronoid fragment with K-wires. This will be followed by definitive screw or plate fixation.
Medial Collateral Ligament (MCL) Repair/Reconstruction
- The anteromedial approach provides direct access to the MCL, especially the anterior bundle, at its humeral origin and ulnar insertion (sublime tubercle).
- For acute avulsions or ruptures, direct repair using suture anchors into the medial epicondyle or sublime tubercle, combined with a transosseous suture technique, can be performed.
- In cases of chronic instability, reconstruction with a tendon graft (e.g., palmaris longus, gracilis) may be necessary, involving creation of bone tunnels at the anatomical insertion sites.

Figure 12: Exposure of the medial collateral ligament (MCL) origin on the medial epicondyle, ready for repair or reconstruction. Suture anchors (dashed circles) are typically used for reattachment.
Medial Humeral Condyle/Epicondyle Fractures
- These fractures are directly under the elevated flexor-pronator mass.
- Reduce the fracture fragments meticulously using pointed reduction clamps or K-wires for provisional fixation.
- Definitive fixation typically involves headless compression screws (e.g., Herbert screws) or small fragment lag screws, ensuring secure fixation and an anatomical reduction of the articular surface. K-wires may be used in pediatric cases.
- Small plates may be indicated for comminuted fractures or those extending proximally into the metaphysis.

Figure 13: Reduction of a medial epicondyle fracture. A clamp holds the reduced fragment in place prior to screw insertion.
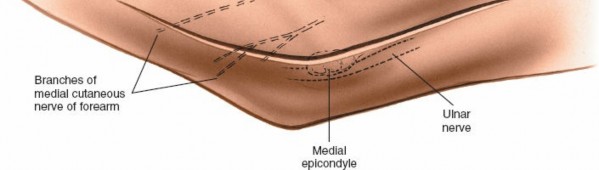
Figure 14: Fixation of a medial epicondyle fracture using small fragment lag screws.
8. Closure
- Perform a thorough washout of the joint.
- Assess elbow stability through a full range of motion.
- Reattach the flexor-pronator mass to its origin on the medial epicondyle using strong, non-absorbable sutures through drill holes or with suture anchors. Ensure adequate tension to restore muscle function while avoiding excessive tension that could lead to stiffness.
- Check the stability of the ulnar nerve. If transposition was performed, ensure it lies comfortably in its new bed. If it was simply retracted, ensure it is not kinked or under tension.
- Close the subcutaneous tissue and skin layers meticulously.
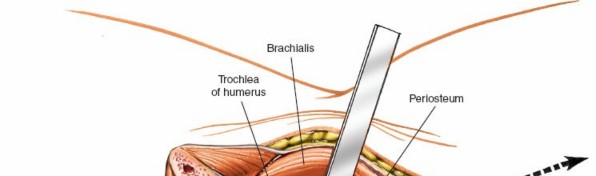
Figure 15: Reattachment of the flexor-pronator mass to the medial epicondyle using transosseous sutures.

Figure 16: Layered closure of the wound. Subcutaneous sutures are placed.
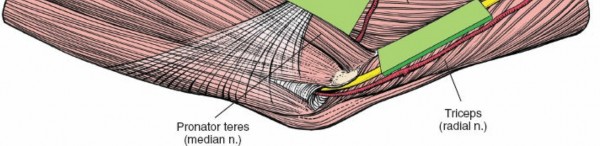
Figure 17: Final skin closure with an aesthetically pleasing approximation of the wound edges.
Complications & Management
Despite meticulous technique, complications can arise with the anteromedial approach. Proactive identification and appropriate management are crucial for optimal patient outcomes.
Common Complications, Incidence, and Salvage Strategies
| Complication Category | Description | Reported Incidence | Salvage Strategies |
|---|---|---|---|
| Neurological Injury | |||
| Ulnar Neuropathy | Most common, ranging from transient paresthesias to motor weakness. Can be due to direct trauma, prolonged retraction, kinking, or post-operative scarring/compression. | 5-20% | Prevention: Meticulous identification, gentle mobilization/retraction, consider prophylactic anterior transposition. Management: Initial observation for transient symptoms. If persistent or progressive, consider neurolysis, revision transposition, or in severe cases, nerve grafting. |
| Median Nerve Injury | Less common, usually due to direct trauma or aggressive anterior retraction. | <1% | Prevention: Careful identification and gentle retraction with the flexor-pronator mass. Management: Observation for neuropraxia. Surgical exploration and neurolysis for persistent deficit; nerve repair/grafting for transection. |
| Medial Antebrachial Cutaneous Nerve (MACN) Injury | Sensory deficit (numbness, dysesthesia) in the medial forearm. Often due to superficial dissection. | 10-30% | Prevention: Careful subcutaneous dissection, sharp incision, avoidance of aggressive cautery. Management: Often self-limiting. Neuroma excision for painful, persistent neuromas. |
| Vascular Injury | Brachial artery injury, typically due to direct trauma during deep dissection or enthusiastic instrumentation. | Rare (<0.5%) | Prevention: Clear identification and protection of brachial artery. Management: Immediate vascular surgery consultation. Arterial repair (primary or graft interposition) or ligation in limb-threatening situations. |
| Infection | Superficial cellulitis or deep surgical site infection (SSI). | 1-5% | Prevention: Strict aseptic technique, prophylactic antibiotics. Management: Superficial: oral antibiotics, wound care. Deep: surgical débridement, IV antibiotics, implant removal if necessary, delayed closure or flap coverage. |
| Heterotopic Ossification (HO) | Formation of ectopic bone, particularly within the brachialis muscle or around the joint capsule, leading to stiffness. | 10-50% (symptomatic 5-10%) | Prevention: Prophylactic NSAIDs (Indomethacin) for 3-6 weeks, or single-dose radiation therapy (700-800 cGy) post-op in high-risk patients. Management: Early ROM, physical therapy. Surgical excision for symptomatic, mature HO after 6-12 months. |
| Elbow Stiffness/Contracture | Restricted range of motion, often due to capsular fibrosis, HO, or inadequate rehabilitation. | 10-30% | Prevention: Meticulous soft tissue handling, early and aggressive post-operative rehabilitation. Management: Intensive physical therapy, dynamic splinting. Surgical capsular release (open or arthroscopic) for persistent, debilitating stiffness after conservative failure. |
| Nonunion/Malunion | Failure of fracture fragments to unite or consolidation in an unacceptable alignment. | 2-10% (fracture dependent) | Prevention: Anatomical reduction, stable fixation, appropriate bone graft if needed. Management: Revision ORIF with debridement, bone grafting, and potentially more rigid fixation. Corrective osteotomy for symptomatic malunion. |
| Implant Failure/Prominence | Breakage of hardware, screw pull-out, or painful implant prominence requiring removal. | Variable | Prevention: Appropriate implant selection, biomechanically sound fixation. Management: Symptomatic implant removal. Revision fixation if nonunion or instability results from hardware failure. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring elbow function while protecting the surgical repair. Protocols vary based on the specific injury (fracture type, ligamentous repair) and surgical stability achieved. The following outlines a general progression.
Phase 1: Protective Phase (0-2 weeks)
- Goals: Control pain and swelling, protect repair, initiate gentle motion.
-
Immobilization:
- Typically, a hinged elbow brace is applied immediately post-operatively, often locked at 30-90° flexion or in a range determined by intra-operative stability.
- For unstable coronoid fractures with MCL repair, the elbow may be immobilized in greater flexion (e.g., 90°) for the first 1-2 weeks.
- A posterior splint may be used initially for comfort and protection.
-
Activity:
- Gentle active and passive range of motion (AROM/PROM) exercises within the protected arc of motion are initiated early (e.g., 2-3 days post-op), focusing on pain-free motion.
- No active flexion against resistance, no lifting, no carrying.
- Hand, wrist, and shoulder AROM exercises are encouraged to prevent stiffness in adjacent joints.
- Pain & Edema Management: Cryotherapy, elevation, and pharmacological pain management.
Phase 2: Early Motion & Strengthening (2-6 weeks)
- Goals: Gradually increase range of motion, initiate light strengthening.
- Immobilization: The hinged brace is gradually unlocked to allow increasing flexion and extension, typically by 10-15° per week, aiming for near full extension by 6 weeks post-op, as tolerated.
-
Activity:
- Continue AROM/PROM exercises, focusing on regaining full extension and flexion.
- Light isometric exercises for biceps, triceps, forearm flexors, and extensors.
- Initiate gentle pronation/supination exercises.
- Continue avoiding lifting, pushing, or pulling heavy objects.
Phase 3: Progressive Strengthening & Functional Return (6-12 weeks)
- Goals: Restore full strength, endurance, and functional use.
- Immobilization: Discontinue hinged brace as stability and range of motion allow.
-
Activity:
- Progressive resistive exercises for all elbow and forearm muscle groups.
- Begin light functional activities.
- Gradual increase in lifting capacity.
- For MCL repairs/reconstructions, valgus stress is carefully monitored, and strengthening exercises are advanced cautiously.
- Introduce sport-specific drills or work-related tasks as appropriate.
Phase 4: Return to Activity (12+ weeks)
- Goals: Full return to previous activity levels, including sports or heavy labor.
-
Activity:
- High-impact activities and overhead sports are gradually introduced, typically not before 4-6 months, depending on the injury severity and healing.
- Continued strengthening and endurance training.
- Emphasis on maintaining flexibility and preventing re-injury.
Specific Considerations:
*
Coronoid Fractures:
If an MCL repair or reconstruction was performed concurrently, the rehabilitation needs to be more guarded to protect the ligamentous repair from excessive valgus stress or early high-load activities.
*
Open Reduction of Joint Surface:
Careful attention to protecting the articular repair from excessive compression or shear forces during early motion.
*
Heterotopic Ossification Prophylaxis:
If used, continue NSAID regimen or monitor radiation effects.
Close communication between the surgeon and physical therapist is essential to tailor the protocol to individual patient progress and intra-operative findings.
Summary of Key Literature / Guidelines
The anteromedial approach to the elbow has been refined through decades of surgical experience and anatomical studies. Key literature emphasizes careful anatomical dissection and appropriate indications.
- Morrey et al. (1993, 2011): Classic texts and subsequent editions of "The Elbow and Its Disorders" provide foundational knowledge on elbow anatomy, biomechanics, and surgical approaches. Morrey's classification of coronoid fractures and associated instability patterns remains standard.
- Regan & Morrey (1989): Their seminal work on coronoid fractures established the classification system widely used today (Type I: tip, Type II: <50% height, Type III: >50% height). This classification directly influences treatment decisions, with Type II and III often requiring fixation via the anteromedial approach due to their role in elbow stability.
- Hotchkiss (1995, 2005): Contributions to surgical approaches, particularly the description of internervous planes, have guided surgeons in safer and more effective exposures. The emphasis on identifying and protecting the ulnar and median nerves is paramount.
- O'Driscoll et al. (2001, 2006): Extensive research on elbow instability, particularly varus posteromedial rotatory instability (VPMRI), has underscored the importance of comprehensive management involving coronoid fracture fixation, MCL repair, and often LUCL reconstruction. The anteromedial approach is central to addressing the medial component of this complex injury.
- Jupiter & Ring (2002): Provided detailed insights into the challenges and techniques for managing complex elbow fractures, including medial column involvement, further solidifying the role of the anteromedial approach.
- Current Consensus: Modern practice increasingly integrates advanced imaging (CT with 3D reconstruction) for pre-operative planning, and recognizes the role of arthroscopy for less complex intra-articular pathology. However, for significant bony injuries of the coronoid and medial condyle, as well as complex ligamentous disruptions, the anteromedial open approach remains the gold standard, offering direct visualization and robust fixation. The principles of stable anatomical reduction and early controlled motion are universally endorsed for optimizing outcomes and minimizing complications like stiffness and heterotopic ossification. Recent literature continues to focus on improving outcomes for specific injury patterns, such as the use of dedicated coronoid plates and refined MCL reconstruction techniques.
Clinical & Radiographic Imaging



You Might Also Like