Terrible Triad of the Elbow: Etiology, Surgical Anatomy & Management Insights
Key Takeaway
The terrible triad of the elbow (TTE) is a complex injury involving a posterior elbow dislocation, radial head fracture, and coronoid process fracture. It typically results from a fall onto an outstretched hand (FOOSH) with axial loading and varying varus/valgus stress, leading to profound instability due to osseous and critical ligamentous disruptions like the lateral ulnar collateral ligament (LUCL).
Triad of the Elbow: Master Diagnosis & Treatment with Our Guide
Introduction & Epidemiology
The "terrible triad of the elbow" (TTE) is a complex, high-energy injury characterized by a posterior elbow dislocation, a radial head fracture, and a coronoid process fracture. This constellation of injuries results in significant instability, often necessitating surgical intervention, and is associated with a high incidence of complications, particularly elbow stiffness and heterotopic ossification. Prognosis is often guarded due to the inherent instability and extensive soft tissue and bony disruption.
Epidemiologically, TTE injuries are predominantly seen in younger, active individuals, frequently resulting from a fall onto an outstretched hand (FOOSH) with an axial load and varying degrees of valgus or varus stress, often combined with supination. Motor vehicle accidents are another common etiology. While the exact incidence of TTE is difficult to ascertain from population-based studies, isolated elbow dislocations are relatively common, and the subset involving associated radial head and coronoid fractures represents a more severe and challenging presentation. Early recognition and a comprehensive management strategy are paramount to optimizing outcomes and mitigating long-term disability.
Surgical Anatomy & Biomechanics
Elbow stability is a complex interplay of osseous articulations, ligamentous constraints, and dynamic muscular stabilizers. Understanding these structures is foundational to managing TTE.
Static Stabilizers
-
Primary Static Stabilizers: These structures provide the majority of elbow stability.
- Ulnohumeral Joint (UHJ): The trochlea-olecranon articulation, specifically the coronoid process engaging the coronoid fossa and the olecranon engaging the olecranon fossa, is the primary osseous stabilizer. The congruent nature of this trochlear notch, particularly the sublime tubercle and the anterior aspect of the coronoid, provides significant resistance to posterior displacement, especially beyond 30° of flexion.
- Medial Collateral Ligament (MCL) Complex / Ulnar Collateral Ligament (UCL) Complex: The anterior bundle (aUCL) is the primary static restraint to valgus stress throughout the range of motion. The posterior bundle (pUCL) acts as a secondary valgus restraint in flexion and forms the floor of the cubital tunnel. The transverse bundle (TB) provides minimal stability. Injury to the aUCL is a critical component of valgus instability.
- Lateral Collateral Ligament (LCL) Complex: The lateral ulnar collateral ligament (LUCL) is the primary static restraint to posterolateral rotatory instability (PLRI) and varus stress. It originates from the lateral epicondyle and inserts on the supinator crest of the ulna. Other components include the radial collateral ligament (RCL) which blends with the annular ligament (AL), providing varus stability, and the annular ligament itself, which stabilizes the radial head. Disruption of the LUCL is central to TTE instability, allowing the ulna to rotate externally off the trochlea.

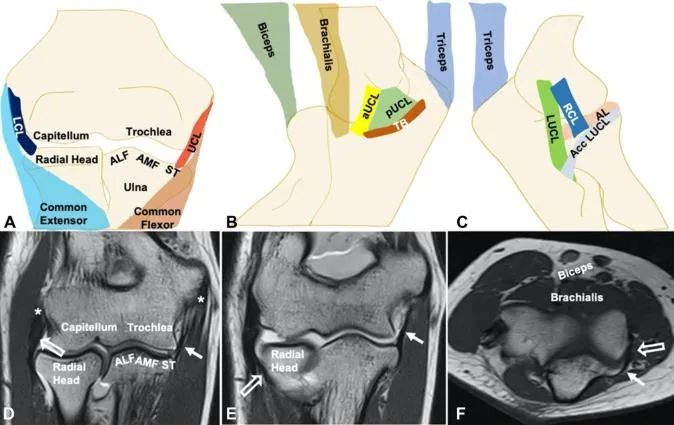
Fig 1: Normal elbow joint anatomy. The intricate network of osseous and soft tissue structures is critical for maintaining elbow stability. Specific emphasis on the coronoid facets (AMF, ALF, ST) and the distinct bundles of the medial (aUCL, pUCL, TB) and lateral (RCL, LUCL, AL) collateral ligament complexes. MRI correlates further delineate these structures. -
Secondary Static Stabilizers: These structures provide supplemental stability, becoming more critical when primary stabilizers are compromised.
- Radial Head: Contributes significantly to valgus stability (approximately 30-50% in the absence of MCL function) and resists axial loading. Its articulation with the capitellum (radiocapitellar joint) also plays a role in forearm rotation.
- Joint Capsule: Provides general confinement and stability, especially at the extremes of motion.
- Common Flexor/Extensor Tendon Origins: While not direct stabilizers, their integrity contributes to overall soft tissue envelope stability.
Dynamic Stabilizers
Muscles crossing the elbow joint, such as the brachialis, triceps, and anconeus, provide dynamic stability. The flexor-pronator mass medially and the extensor-supinator mass laterally also contribute.
Biomechanics of Injury
The terrible triad injury typically occurs from a FOOSH mechanism. The axial load drives the olecranon posteriorly, while the forearm often undergoes a varus or valgus stress with supination.
- Dislocation: The primary force causes posterior dislocation of the ulna from the trochlea.
- Coronoid Fracture: As the olecranon dislocates posteriorly, the coronoid process, specifically its anterior-medial facet, impacts the trochlea, leading to a fracture. The size and displacement of the coronoid fragment dictate the degree of persistent instability. A larger, displaced fragment significantly compromises the osseous buttress against posterior translation.
- Radial Head Fracture: Simultaneously, or sequentially, the radial head impacts the capitellum due to the axial load and often a valgus component. This results in a radial head fracture, which further compromises valgus and axial stability.
- Ligamentous Disruption: Critically, the elbow capsule and collateral ligaments are torn. The lateral collateral ligament complex (LUCL) is typically avulsed from the lateral epicondyle, initiating posterolateral rotatory instability. The medial collateral ligament complex (aUCL) may also be disrupted, either from direct injury or secondary to the dislocation mechanism.
The combination of these three injuries creates a profound instability, often described as "circulatory instability," where the elbow relies on minimal remaining intact structures, making concentric reduction and stable fixation challenging.

Fig 2: Typical mechanism of terrible triad injury. A fall onto an outstretched hand with an axial load and supination/valgus stress vectors results in a levering effect, disrupting the ulnohumeral articulation and causing concomitant radial head and coronoid fractures.
Indications & Contraindications
Management of TTE is complex and primarily surgical due to the inherent instability of the injury pattern. Non-operative management is rarely appropriate for true TTE.
Indications for Operative Management
The presence of a terrible triad injury almost universally indicates the need for surgical stabilization to restore concentric reduction, bony alignment, and ligamentous integrity. Specific components necessitating intervention include:
- Persistent instability after closed reduction: If the elbow remains unstable through a functional range of motion (e.g., less than 30-100 degrees of stable arc) after initial reduction, surgical stabilization is mandatory.
- Irreducible dislocation: If closed reduction fails due to interposed fragments or soft tissues.
-
Displaced Radial Head Fractures:
- Mason Type II: Displaced single fragment radial head fractures involving a significant portion of the articular surface (>2mm displacement, >30% articular involvement, or mechanical block).
- Mason Type III: Comminuted radial head and neck fractures that cannot be anatomically reconstructed.
- Mason Type IV: Radial head fracture with elbow dislocation (by definition part of TTE).
- Radial head fractures where excision alone would lead to unacceptable instability.
-
Displaced Coronoid Fractures:
- Regan & Morrey Type II: Fractures involving 10-50% of the coronoid height.
- Regan & Morrey Type III: Fractures involving >50% of the coronoid height.
- Fractures involving the sublime tubercle or anteromedial facet which are crucial for stability against posteromedial instability.
- Any coronoid fracture that, despite radial head and ligamentous repair, contributes to gross instability.
- Ligamentous Instability: Gross instability following bony fixation, requiring primary repair or augmentation/reconstruction of the MCL and/or LCL complex (especially LUCL).
- Associated Injuries: Open fractures, neurovascular compromise, or concomitant fractures requiring operative fixation.
Contraindications for Operative Management
Absolute contraindications are rare but include:
- Active Infection: Acute infection at the operative site.
- Severe Systemic Comorbidities: Medical instability that precludes safe anesthesia and surgery.
- Non-Reconstructible Anatomy: Severely comminuted fractures or tissue loss precluding stable fixation, though even in these cases, an external fixator may be indicated for stability.
Relative contraindications include:
- Extremely poor soft tissue envelope (e.g., severe open injury with extensive degloving), potentially requiring staged procedures.
- Patient factors precluding compliance with intensive post-operative rehabilitation.
Summary of Operative vs. Non-Operative Indications
| Feature | Operative Indication | Non-Operative Indication (Rare for True TTE) |
|---|---|---|
| Elbow Stability | Gross instability after reduction, inability to achieve concentric reduction, persistent instability throughout a functional arc of motion. | Extremely rare for TTE. May be considered for isolated, minimally displaced components if elbow is stable (e.g., Mason Type I radial head with stable coronoid and ligaments, usually not a TTE). |
| Radial Head Fx | Mason Type II (displaced, articular involvement), Type III (comminuted), Type IV (with dislocation). Unstable Mason Type I after ligament repair. Indications for ORIF, radial head arthroplasty, or rarely excision. | Isolated, truly non-displaced Mason Type I radial head fracture, with a stable elbow (i.e., not a true TTE). |
| Coronoid Fx | Regan & Morrey Type II (>10% height) or Type III (>50% height). Fractures of the sublime tubercle or anteromedial facet. Any coronoid fracture contributing to persistent instability after radial head and ligamentous repair. | Regan & Morrey Type I (tip fracture, <10% height), if elbow is stable after reduction and assessment of other components (highly unlikely in TTE). |
| Ligament Injury | Gross tears of LUCL and/or MCL (especially aUCL) leading to instability. | Minor sprains or partial tears not contributing to gross instability (extremely rare in TTE). |
| Associated Fx/Inj | Open fractures, neurovascular compromise, concomitant fracture of olecranon or distal humerus. | None relevant to TTE. |
| Patient Factors | Medically fit for surgery, good rehabilitation potential. | Medically unstable, severe comorbidities precluding surgery, non-compliant patient (with guarded prognosis). |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial for managing TTE, given its complexity.
Diagnostic Workup
-
Clinical Assessment:
- History: Mechanism of injury, hand dominance, previous elbow injuries.
- Physical Exam: Assess skin integrity, neurovascular status (median, ulnar, radial nerves, brachial artery). Carefully document any deficits pre-operatively. Assess stability after initial reduction (if performed).
-
Imaging:
- Plain Radiographs: AP, lateral, and oblique views (e.g., Greenspan view for radial head). Confirm dislocation, identify fracture patterns of the radial head and coronoid, and assess pre-existing arthrosis.
- Computed Tomography (CT) Scan: Essential for detailed assessment of fracture morphology, comminution, displacement, and joint congruence. 3D reconstructions are invaluable for surgical planning, especially for coronoid fractures (size, location of fragment, involvement of sublime tubercle or anteromedial facet) and radial head (comminution, articular step-off).
- Magnetic Resonance Imaging (MRI): Less commonly performed acutely but can provide superior detail regarding ligamentous integrity (MCL, LCL), capsule, and associated soft tissue injuries, which may influence reconstruction strategies.
Surgical Planning
- Order of Repair: Consensus suggests addressing the most critical stabilizers first: typically coronoid fracture fixation, then radial head fracture fixation or replacement, followed by collateral ligament repair/reconstruction.
-
Choice of Implants:
- Coronoid: Suture lasso technique, small lag screws (anterior-to-posterior, posterior-to-anterior, or medial-to-lateral), buttress plates.
- Radial Head: Headless compression screws for ORIF, low-profile plates for specific patterns, or radial head arthroplasty (metallic or pyrocarbon implants) for highly comminuted or unreconstructible fractures.
- Ligaments: Suture anchors for reattachment, autograft/allograft for reconstruction if primary repair is not feasible.
- Approaches: Determine optimal surgical approaches based on fracture patterns. Often, a combination of lateral (Kocher) and medial (Hotchkiss or direct medial) approaches is required.
- Contingency Planning: Be prepared for potential complications such as persistent instability, need for a hinged external fixator, or conversion from ORIF to arthroplasty.
Patient Positioning
- General Anesthesia: Standard general anesthesia is employed.
-
Positioning:
- Lateral Decubitus: Most commonly preferred. The patient is positioned with the injured arm draped free over a bolster or arm board. This allows for excellent access to both medial and lateral aspects of the elbow, facilitates assessment of stability through range of motion, and allows for easy pronation/supination of the forearm.
- Supine with Arm Table: An alternative, especially if other injuries require supine positioning. However, access to the posterior aspect of the elbow can be more challenging.
- Tourniquet: A pneumatic tourniquet on the proximal arm is routinely used to optimize visualization.
- Sterile Prep and Drape: Standard sterile preparation and draping to allow for full range of motion and access to all necessary approaches.
- Fluoroscopy: Intraoperative fluoroscopy is essential to confirm reduction, assess fixation, and evaluate stability.
Detailed Surgical Approach / Technique
The goal of surgical management for TTE is to achieve a stable, concentric reduction of the elbow joint and enable early range of motion. This is accomplished by sequentially addressing the bony and soft tissue components. The general principle is "fix the bone, then fix the ligaments." The sequence is typically coronoid, then radial head, then collateral ligaments.
1. Initial Access and Evaluation
- Reduce Dislocation: If not already reduced, perform a gentle closed reduction under anesthesia. Assess stability. If still dislocated or grossly unstable, proceed with open reduction.
-
Skin Incisions:
- Lateral Approach (Kocher interval): Incision centered over the lateral epicondyle, extending proximally along the supracondylar ridge and distally along the ulna. The interval is between the anconeus (ulnar nerve innervation) and the extensor carpi ulnaris (ECU) (radial nerve innervation, posterior interosseous nerve branch). This provides access to the radial head, capitellum, and lateral collateral ligament complex.
- Medial Approach (Hotchkiss modification of Kocher or Direct Medial): An incision distal to the medial epicondyle, extending proximally along the supracondylar ridge and distally along the ulna. The interval is between the flexor carpi ulnaris (FCU) and the flexor digitorum superficialis (FDS), protecting the ulnar nerve posteriorly. This approach provides access to the coronoid, medial collateral ligament, and ulnohumeral joint. Alternatively, a posteromedial approach can be used.
- Neurovascular Protection: Carefully identify and protect the ulnar nerve medially and the posterior interosseous nerve (PIN) laterally (within the supinator).
2. Coronoid Fracture Management
The coronoid fracture is often the most challenging component to fix, yet its stable fixation is crucial for elbow stability.
- Exposure: Accessed primarily through a medial approach (often posteromedial). The flexor-pronator mass is either split or elevated off the medial epicondyle. The anterior capsule may be incised to directly visualize the coronoid.
-
Reduction:
- Small, anterior fragments (Regan & Morrey Type I) are often reattached with suture techniques.
- Larger fragments (Type II/III) require direct reduction. This can be challenging due to retraction and comminution. Use small bone hooks, Kocher clamps, or fine instruments to manipulate the fragment.
-
Fixation Options:
- Suture Lasso Technique: For larger fragments (Regan & Morrey Type II/III) involving the sublime tubercle or anteromedial facet. Non-absorbable sutures are passed through drill holes in the proximal ulna, looped around the coronoid fragment, and tied, reducing and compressing it against the ulna. This is often performed through a posterior approach or a drill hole from the posterior cortex of the ulna anteriorly.
- Anterior-to-Posterior Screws: Small cannulated or headless compression screws can be placed from the anterior aspect of the coronoid into the ulna. This requires a dedicated anterior approach or careful manipulation through the medial approach.
- Posterior-to-Anterior Screws: Screws are placed from the posterior cortex of the ulna through the fragment. This requires careful trajectory planning to avoid the ulnohumeral joint.
- Buttress Plating: Small fragment plates (e.g., L-plate or T-plate) can be applied to the anteromedial aspect of the coronoid for larger, comminuted fragments.
- Transosseous Sutures: Similar to lasso, but can be passed directly through the fragment and out the posterior ulna.
-
Image Integration:

Fig 3: Example of coronoid fixation. This image (and subsequent images,,,,,,,,,,will illustrate various aspects of fixation and repair as described in the text.)

Fig 4: Radiographic views of coronoid fixation (e.g., suture lasso). A: Lateral view showing posterior portal for suture passage. B: Anterior view demonstrating the path of sutures around the coronoid. C: Post-operative lateral radiograph with successful fixation.

Fig 5: Various fixation methods for coronoid fractures. From simple suture fixation to lag screws and buttress plating, the choice depends on fragment size and morphology.
3. Radial Head Fracture Management
Addressed via the lateral Kocher approach.
- Exposure: The capsule is incised, and the radial head fracture is exposed.
- Evaluation: Assess fracture pattern, comminution, and articular involvement. Debride any loose fragments.
-
Fixation Options:
- Open Reduction Internal Fixation (ORIF): For Mason Type II fractures. Fragments are anatomically reduced and fixed with two or more low-profile headless compression screws. Care must be taken to ensure screws are recessed below the articular surface and do not impinge on the capitellum or ulna during pronation/supination.
- Radial Head Arthroplasty: For Mason Type III or IV fractures that are highly comminuted and unreconstructible. This restores radial head height and provides stability against valgus stress and axial loading. The prosthesis should be sized appropriately to avoid overstuffing the joint.
- Excision: Rarely indicated in TTE as the radial head is a critical secondary stabilizer, and its excision would exacerbate instability. Only considered for very small, non-articular fragments if the elbow is otherwise stable.
-
Image Integration:

Fig 6: Radial head fracture fixation. A: Comminuted radial head fracture. B: ORIF with headless screws.

Fig 7: Radial head replacement. A: Severely comminuted radial head fracture, not amenable to ORIF. B: Post-operative radiograph with a radial head prosthesis in situ.
4. Collateral Ligament Repair/Reconstruction
Ligamentous stability is assessed after bony fixation. The order of repair typically follows the "inside-out" or "outside-in" principle based on initial stability. The LUCL is always repaired; the MCL may or may not require repair if the elbow is stable after coronoid and radial head fixation. However, in TTE, both are often compromised.
-
Lateral Ulnar Collateral Ligament (LUCL) Repair:
- Exposure: Via the lateral Kocher approach. The torn ends of the LUCL are identified, typically avulsed from the lateral epicondyle or distal to the supinator crest on the ulna.
- Repair: Reattach the LUCL to the isometric point on the lateral epicondyle using suture anchors. The ulna attachment on the supinator crest is also repaired. The posterior capsule can also be incorporated into the repair. Ensure adequate tension to prevent posterolateral rotatory instability.
- Reconstruction: If the native tissue quality is poor or a chronic injury is present, an autograft (e.g., palmaris longus) or allograft may be used to reconstruct the LUCL using a docking technique.
-
Medial Collateral Ligament (MCL) Repair:
- Exposure: Via the medial approach. Identify the anterior bundle (aUCL) and its avulsion point, usually from the medial epicondyle.
- Repair: Direct repair of the aUCL to the medial epicondyle using suture anchors. If the fracture of the medial epicondyle is present, fix it first.
- Reconstruction: If primary repair is not robust (e.g., severe mid-substance tear, chronic injury), MCL reconstruction (e.g., "docking technique") may be necessary, often with a palmaris longus autograft.
- Capsule Repair: Repair any significant capsular tears to contribute to overall stability.
-
Image Integration:

Fig 8: Lateral collateral ligament repair. Suture anchors are placed at the isometric point on the lateral epicondyle for reattachment of the LUCL and associated capsule.

Fig 9: Medial collateral ligament repair. A: Avulsed aUCL from the medial epicondyle. B: Repair with suture anchors.
5. Final Stability Assessment
- After all components are addressed (coronoid, radial head, MCL, LCL), perform a comprehensive dynamic stability assessment under fluoroscopy.
- Gently move the elbow through a full range of motion (flexion, extension, pronation, supination), applying valgus and varus stress.
- The goal is to achieve a stable arc of motion from approximately 30° to 120° of flexion without subluxation or dislocation.
-
If persistent instability remains, consider:
- Revision of fixation.
- Application of a hinged external fixator to provide dynamic stability while allowing motion.
-
Image Integration:

Fig 10: Intraoperative fluoroscopic image showing evaluation of stability after fixation. The elbow is gently moved through its arc of motion under stress to confirm concentric reduction and absence of subluxation.
6. Wound Closure and Post-Operative Dressing
- Copious irrigation.
- Layered closure of all incisions.
- Apply a sterile dressing and a long-arm splint, typically in 90° flexion with the forearm in neutral rotation or slight pronation (to protect the LUCL repair).
-
Image Integration:

Fig 11: Post-operative long arm splint, typically in 90 degrees of flexion with the forearm in neutral or slight pronation.
Complications & Management
The terrible triad of the elbow is associated with a high rate of complications, necessitating diligent post-operative monitoring and aggressive rehabilitation.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategy / Management |
|---|---|---|
| Elbow Stiffness / Loss of ROM | Most common, 30-50% significant stiffness (>30° loss), with some residual loss common. | Aggressive physical therapy, dynamic splinting, manipulation under anesthesia (MUA) after 3-6 months, arthrolysis (open or arthroscopic) for persistent mechanical block (e.g., HO, nonunion). |
| Heterotopic Ossification (HO) | 20-60% clinically significant HO. | Prophylaxis: NSAIDs (Indomethacin) for 3-6 weeks, or single dose radiation (700-800 cGy) post-op. Management: Surgical excision of mature HO (typically >6-12 months post-injury) if symptomatic and limiting ROM. |
| Post-Traumatic Arthritis | Variable, 10-30% long-term. Correlates with initial cartilage damage, malunion, or persistent instability. | Conservative management (NSAIDs, injections). For severe, symptomatic arthritis: arthroplasty (total elbow), interposition arthroplasty, or arthrodesis (salvage). |
| Recurrent Instability / Dislocation | 5-15% after surgical repair. | Revision surgery: re-fixation of bony elements, revision ligament repair/reconstruction, often with application of a hinged external fixator to protect repairs. |
| Ulnar Neuropathy | 10-20% (often transient). Can be due to direct injury, traction, compression from swelling/HO, or iatrogenic. | Management: Observation for transient symptoms. Surgical decompression (in situ neurolysis, anterior transposition) if persistent or progressive deficits, often performed in conjunction with other revision surgeries. |
| Radial Nerve / PIN Injury | Less common, 2-5%. | Management: Observation for transient neuropraxia. Surgical exploration and neurolysis if persistent or progressive deficits. |
| Nonunion / Malunion | Radial head/coronoid: <5% for well-fixed fractures. Usually due to poor fixation or severe comminution. | Nonunion: Revision ORIF with bone grafting, radial head arthroplasty (for radial head). Malunion: Osteotomy to correct deformity, or salvage arthroplasty. |
| Infection | <5%. Higher in open injuries or prolonged surgical times. | Surgical debridement, antibiotics (IV then oral). Retained hardware removal if fixation is stable and infection persists. May require a two-stage approach. |
| Hardware-Related Issues | Prominence, irritation, migration, failure. Up to 10-20% for hardware removal for symptoms. | Symptomatic hardware removal after fracture healing and soft tissue integrity are restored. Revision fixation for hardware failure. |
| Complex Regional Pain Syndrome (CRPS) | Rare, but can be debilitating. | Early diagnosis, aggressive pain management (nerve blocks, medication), physical therapy, psychological support. |
Image Integration: Complications

Fig 12: Example of post-operative complication: Heterotopic Ossification. A: Radiograph showing significant HO limiting elbow motion. B: Surgical excision of mature HO (arthrolysis).

Fig 13: Recurrent instability requiring external fixation. A: Post-operative radiograph after initial repair, showing residual instability. B: Application of a hinged external fixator to provide dynamic stability.

Fig 14: Post-traumatic arthritis. A: Long-term follow-up radiograph showing degenerative changes in the elbow joint. B: Clinical presentation of limited range of motion.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as surgical stabilization for achieving optimal outcomes in TTE, aiming to restore functional range of motion while protecting the healing repairs. Protocols must be individualized based on intraoperative stability.
Phase 1: Protection & Early Motion (Weeks 0-3)
Goals: Control pain and swelling, protect surgical repairs, initiate early, controlled motion to prevent stiffness.
-
Immobilization:
- Typically, a long-arm posterior splint is applied immediately post-op, often in 90° flexion with the forearm in neutral or slight pronation (to minimize stress on the LUCL).
- Splinting may be maintained for 1-2 weeks, depending on intraoperative stability.
- Some surgeons prefer a hinged elbow brace immediately, locked for extension beyond a safe range (e.g., 30° flexion) for the first 1-2 weeks.
-
Range of Motion (ROM):
- Initiate Active-Assisted Range of Motion (AAROM) and Active Range of Motion (AROM): Within the safe, stable arc determined intraoperatively (e.g., 30°-90° or 100° flexion).
- Avoid Passive Range of Motion (PROM): Especially during the first few weeks, as excessive passive stretching can disrupt healing tissues.
- Forearm Rotation: Begin gentle pronation and supination within a comfortable range, avoiding extreme supination if the LUCL repair is tenuous.
-
Activity Restrictions:
- No lifting, pushing, pulling.
- Avoid any varus or valgus stress.
- No weight-bearing on the affected arm.
-
Adjuncts:
- Elevation, ice, and pain medication.
- Heterotopic ossification prophylaxis (NSAIDs or radiation) if indicated.
Phase 2: Increasing Range of Motion & Gentle Strengthening (Weeks 3-6)
Goals: Progress ROM, begin light strengthening, and reduce reliance on external support.
-
Immobilization:
- Transition from splint to hinged elbow brace, worn for protection during activities, but removed for exercises.
- Gradually increase the allowed range of extension in the brace (e.g., progress to 15° or 0° extension by week 6).
-
Range of Motion (ROM):
- Continue AROM/AAROM exercises, gently progressing towards full flexion and extension.
- Initiate gentle, pain-free PROM, emphasizing functional arcs.
- Continue forearm pronation/supination.
-
Strengthening:
- Begin isometric exercises for elbow flexors, extensors, and forearm rotators.
- Introduce very light resistance exercises (e.g., light putty or small weights) for grip and forearm musculature.
-
Activity Restrictions:
- Still no heavy lifting or impact activities.
- Avoid stressing the healing collateral ligaments.
Phase 3: Progressive Strengthening & Functional Return (Weeks 6-12+)
Goals: Achieve full functional ROM, maximize strength, and prepare for return to activity.
-
Immobilization:
- Wean from the brace as comfort and stability allow, typically by 6-8 weeks. May use it for protection during higher-risk activities.
-
Range of Motion (ROM):
- Intensive focus on restoring full, pain-free ROM.
- Continue stretching and mobilization exercises.
- Address any residual stiffness with joint mobilization techniques (by therapist) or self-stretching.
-
Strengthening:
- Progress to moderate and then heavy resistance exercises for all elbow and forearm musculature.
- Incorporate eccentric exercises.
- Begin closed-chain exercises (e.g., wall push-ups).
-
Functional Activities:
- Begin sport-specific or work-specific activities with gradual progression.
- Focus on endurance and power development.
- Return to unrestricted activities usually takes 4-6 months, and sometimes longer for high-demand activities.
Key Considerations:
- Communication: Close collaboration between the surgeon and physical therapist is essential.
- Pain Management: Ensure adequate pain control to allow participation in rehabilitation.
- Patient Education: Manage patient expectations regarding recovery time and potential for residual stiffness.
- Beware of Heterotopic Ossification: Monitor for signs of HO and adjust treatment as needed.
- Protect Ligament Repairs: Avoid specific stress directions (e.g., valgus stress for MCL, varus/supination for LUCL) as guided by intraoperative findings and healing timeline.
Summary of Key Literature / Guidelines
The management of terrible triad injuries has evolved significantly over recent decades, with current guidelines emphasizing early, comprehensive surgical stabilization to restore concentric reduction and allow early range of motion.
- Historical Context: Early management often resulted in poor outcomes, high rates of stiffness, and recurrent instability. Morrey's work on elbow stability and classification systems (e.g., Regan & Morrey for coronoid fractures, Mason for radial head fractures) provided a framework for understanding and treating these complex injuries.
-
Evolution of Treatment:
- Importance of Radial Head: Initial approaches sometimes favored radial head excision for comminuted fractures. However, numerous studies, including those by Ring and Hotchkiss, highlighted the critical role of the radial head as a secondary valgus and axial stabilizer. Radial head arthroplasty has emerged as the preferred option for unreconstructible radial head fractures in TTE to maintain joint stability.
- Coronoid Fixation: The significance of coronoid fractures, particularly the anteromedial facet, in providing osseous stability against posterior displacement has been increasingly recognized. Techniques for coronoid fixation (e.g., suture lasso, plates, small screws) have become more refined and are considered crucial for stability.
- Ligamentous Repair: The importance of repairing the lateral ulnar collateral ligament (LUCL) to prevent posterolateral rotatory instability is well-established. Medial collateral ligament (MCL) repair is also performed if the elbow remains unstable after bony fixation and LUCL repair. If primary repair is not feasible, reconstruction using autograft or allograft is an option.
- Sequencing of Repair: The generally accepted sequence for surgical repair is coronoid fixation first, followed by radial head fixation/arthroplasty, and then collateral ligament repair. This "fix the bone, then fix the ligaments" approach aims to re-establish the bony architecture before restoring soft tissue tension.
- Dynamic External Fixation: For cases with persistent instability despite adequate internal fixation and ligament repair, a hinged external fixator can provide dynamic stability, allowing controlled early motion and protecting the healing structures.
-
Current Consensus and Outcomes:
- Early Surgical Intervention: Prompt surgical stabilization within days of injury is generally recommended to prevent chronic instability and facilitate rehabilitation.
- Comprehensive Approach: A systematic, stepwise approach addressing all three components (coronoid, radial head, ligaments) is critical.
- Rehabilitation: Aggressive, but protected, early range of motion protocols are paramount to prevent stiffness while allowing tissue healing.
- Outcomes: While challenging, modern surgical techniques, combined with dedicated rehabilitation, have improved outcomes. Good to excellent results are reported in 60-80% of cases, though residual stiffness, especially loss of extension, remains the most common complication. Heterotopic ossification, post-traumatic arthritis, and recurrent instability are also recognized challenges that necessitate careful management.
- Future Directions: Ongoing research focuses on optimizing implant design, developing less invasive surgical techniques, improving ligament reconstruction methods, and refining rehabilitation protocols to further minimize complications and enhance long-term functional outcomes. The role of advanced imaging techniques like kinematic MRI in pre-operative planning and post-operative assessment is also expanding.
Clinical & Radiographic Imaging


