Late CRPS: Decoding This Phase of Complex Atrophy & Contracture

Key Takeaway
Here are the crucial details you must know about Late CRPS: Decoding This Phase of Complex Atrophy & Contracture. The late phase of complex regional pain syndrome (CRPS) is marked by limb atrophy, thinned skin, brittle nails, and hair changes. Fascias thicken, leading to contractures resembling Dupuytren disease. Joint capsules and ligaments shorten, causing severe joint contracture. Bone scans normalize, but radiographic features include profound osteoporosis, indicating significant bone loss in this advanced phase of complex.
As Academic Orthopedic Surgeons and Medical Educators, our understanding of Complex Regional Pain Syndrome (CRPS) must extend beyond its acute, inflammatory phases to encompass the challenging and often debilitating late-stage presentation. This phase, characterized by profound structural atrophy and fixed contractures, represents a significant orthopedic and functional challenge, demanding a nuanced approach to diagnosis, patient selection, and potential surgical intervention.
Introduction and Epidemiology
The progression of Complex Regional Pain Syndrome from its early, often hyperemic and edematous phase, into the late stage marks a significant shift in its clinical and pathological manifestations. In this late phase, the initial vasomotor instability (VMI) typically recedes, and the pronounced edema resolves, replaced by a profound and generalized atrophy of the affected limb. This atrophic process impacts every tissue compartment, leading to a cascade of structural changes that fundamentally alter limb architecture and function.
The skin becomes visibly thinned and atrophic, losing its normal turgor and elasticity. Joint creases, which are normal anatomical landmarks, often disappear, and subcutaneous fat diminishes significantly. Hairs in the affected region become fragile, uneven, and characteristically curled. Nails exhibit dystrophic changes, presenting as pitted, ridged, brittle, and often discolored brown. These cutaneous and adnexal changes are outward indicators of a deeper, pervasive tissue remodeling process.
Pathologically, a hallmark of late CRPS is the thickening and contraction of palmar and plantar fascias, often mimicking the appearance and mechanical effects of Dupuytren disease. This fascial contracture can lead to fixed flexion deformities of the digits. Concurrently, tendon sheaths become constricted and fibrotic, impeding normal tendon gliding and causing triggering phenomena or significantly increased resistance to movement. Muscle contracture, frequently involving both intrinsic and extrinsic muscle groups, combined with tendon adherence, leads to a marked reduction in tendon excursion and resultant joint stiffness. The perarticular structures are not spared; joint capsules and collateral ligaments become shortened, thickened, and adherent, culminating in severe, fixed joint contractures.
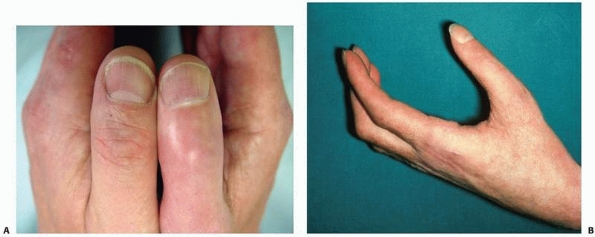
FIGURE 23-2 The late phase of complex regional pain syndrome (CRPS). A. Detail of the thumbs of a patient with late CRPS type 1 of the right hand. There is spindling of the digit particularly distally. The nail is excessively ridged and is discolored. B. The hand of a patient with late CRPS type 1. The patient is trying to make a fist. Note the digital spindling and extension contractures with loss of joint creases.
It is paramount to reiterate that the progression of CRPS is remarkably variable. Within orthopaedic practice, the vast majority of patients who initially demonstrate the features of early-phase CRPS after trauma will not progress to develop the severe, fixed contractures characteristic of the late phase. Nevertheless, a significant proportion will exhibit chronic subclinical contracture or persistent mild to moderate functional limitations. The transition to the severe late-stage phenotype, while less common, presents the most profound diagnostic and therapeutic challenges for the orthopedic surgeon.
Epidemiologically, CRPS affects approximately 5.46 to 26.2 per 100,000 person-years, with a higher incidence observed in females and following distal radius fractures. While the exact prevalence of severe late-stage CRPS with fixed contractures is not precisely quantified, it represents a smaller, yet functionally devastating, subset of patients. The etiology is often linked to trauma, surgery, or immobilization, but spontaneous onset can occur. The socioeconomic burden of CRPS, particularly its late phase, is substantial, stemming from chronic pain, severe functional impairment, lost productivity, and extensive healthcare utilization. Understanding this complex progression is crucial for timely diagnosis and appropriate management strategies.

FIGURE 23-3 Bone scan changes in late CRPS type 1. A. Planar bone scan, posterior image of the hands and wrists, showing diffuse increased uptake in the wrist and carpus, with relative preservation of the metacarpophalangeal joints. B. Planar bone scan, anterior image of the feet and ankles, showing diffuse increased uptake in the forefoot and midfoot, more pronounced on the left. Such diffuse uptake is characteristic of late CRPS.
Surgical Anatomy and Biomechanics
The anatomical and biomechanical derangements in late CRPS are extensive, requiring a thorough understanding for any consideration of surgical intervention. The hallmark of this phase is pervasive fibrosis and contracture affecting nearly all soft tissue structures.
Skin and Subcutaneous Tissues in Late CRPS
The skin in late CRPS is typically thin, atrophic, and often shiny. Subcutaneous fat is diminished, leading to a "spindled" appearance of digits and limbs, particularly noticeable distally. This atrophy results in reduced skin elasticity and vascularity, which has significant implications for surgical incisions and wound healing. The underlying dermal and subdermal tissues may also be fibrotic and adherent to deeper structures, complicating dissection and increasing the risk of skin flap compromise.
Fascial Anatomy and Pathology
The fascial layers, particularly the palmar and plantar aponeuroses, undergo significant fibrous thickening and contracture, structurally and histologically resembling Dupuytren's disease. This process can extend beyond the typical zones of Dupuytren's, affecting the entire palmar or plantar surface and forming cords that tether the skin and flexor tendons. Understanding the three-dimensional architecture of these fascial bands and their relationship to neurovascular structures is critical for safe and effective fasciectomy.
Tendon and Tendon Sheath Involvement
Tendon sheaths become chronically inflamed, fibrotic, and constricted, leading to impaired gliding of the enclosed tendons. This reduced excursion manifests as triggering, catching, or severe limitations in active and passive range of motion. Adhesions can form between the tendon and its sheath, or between the tendon and surrounding soft tissues (e.g., muscle, fascia, bone). This often affects flexor tendons in the hand and foot, and extensor tendons can also be involved. Biomechanically, reduced tendon excursion directly translates to a loss of joint motion, as the muscle-tendon unit is unable to transmit force effectively across the joint.
Muscle Contracture and Fibrosis
Both intrinsic and extrinsic muscles of the affected limb can undergo significant contracture and fibrosis. This is not merely a shortening but often involves histological changes with replacement of contractile elements by fibrous tissue. Intrinsic muscle contractures of the hand, for example, can contribute to severe claw deformities. The altered resting length and reduced extensibility of these muscles further exacerbate joint contractures and limit overall functional capacity. The biomechanical consequence is a fixed deformity that resists passive stretch and active lengthening.
Joint Capsule and Ligament Pathology
Joint capsules become universally shortened, thickened, and adherent, particularly in the periarticular regions. Collateral ligaments, crucial for joint stability and guidance, also stiffen and shorten. This complex pathology leads to severe, fixed joint contractures, where the joint is mechanically locked in a specific position, often flexion for proximal joints and extension for distal interphalangeal joints, or vice-versa depending on the primary muscle contracture. The loss of normal capsular and ligamentous elasticity prevents full joint excursion, regardless of tendon function. Bone scans can sometimes show regional osteopenia in the late phase.

FIGURE 23-4 Bone scan changes. Typical patterns of diffuse uptake in late CRPS. A. Diffuse increased uptake in the hand. B. Diffuse increased uptake in the foot. These images complement Figure 23-3 by illustrating the characteristic bone scan findings across different affected regions in late-stage CRPS, reflecting the chronic inflammatory and remodeling processes within the bone.
Neurovascular Considerations
Neurovascular bundles can be encased in dense scar tissue, making their identification and protection challenging during surgical dissection. The nerves themselves may be sensitive to manipulation, and their compromised vascular supply due to surrounding fibrosis can make them vulnerable to iatrogenic injury. Understanding the typical course of nerves and vessels in relation to fascial planes and joint capsules is critical, especially when addressing deeply embedded contractures.
Overall, the surgical anatomy in late CRPS is characterized by distorted planes, dense fibrosis, and loss of tissue pliability, fundamentally altering the biomechanical function of the limb. Any surgical approach must respect these profound pathological changes to minimize iatrogenic harm and maximize functional restoration.
Indications and Contraindications
Surgical intervention in late CRPS is a complex decision, often representing a salvage procedure rather than a primary treatment. It is primarily considered for severe, fixed deformities that significantly impair function and have failed exhaustive, multidisciplinary non-operative management. The primary goal is typically functional restoration and improvement in limb mechanics, not pain relief, as surgery can paradoxically exacerbate CRPS pain.
Operative Indications
Operative indications are highly selective and revolve around severe, static deformities.
Non-Operative Management Considerations
Non-operative management remains the cornerstone of CRPS treatment across all phases. It includes aggressive physical and occupational therapy, pain management (pharmacological, regional blocks, neuromodulation), psychological support, and splinting/casting. Surgical consideration only arises after failure of maximal, sustained conservative efforts.
| Condition | Operative Indication | Non-Operative Management | Key Considerations |
|---|---|---|---|
| Fixed Joint Contracture | Severe, fixed contractures (e.g., MCP, PIP, wrist, ankle, knee) limiting basic ADLs, refractory to >6-12 months of intensive therapy. | Aggressive physical/occupational therapy, dynamic/static progressive splinting, serial casting, manual therapy, pain management. | Surgical options include capsulotomy, collateral ligament release, arthrolysis. Risks include CRPS exacerbation, recurrence. Careful selection is crucial; aim for functional gain, not necessarily full ROM. |
| Tendon Adhesion/Triggering | Significant functional impairment from refractory tendon triggering or adhesions unresponsive to non-operative measures. | Tenodesis exercises, gliding exercises, splinting, steroid injections (limited use in CRPS due to potential skin atrophy). | Surgical tenolysis to restore tendon excursion. Meticulous technique required to avoid re-adhesion. Post-operative hand therapy is critical for maintaining gains. |
| Fascial Contracture | Severe palmar/plantar fascial contractures (Dupuytren-like) causing fixed digital deformities, limiting grip/weight-bearing, failed non-operative stretching. | Stretching exercises, massage, splinting, collagenase injection (if primary Dupuytren's, less clear for CRPS-related fibrosis). | Partial or total fasciectomy. High risk of recurrence; meticulous dissection to protect neurovascular structures embedded in scar. |
| Persistent Pain | Intractable, severe pain associated with a non-functional limb, after all other therapies (pharmacologic, interventional, psychological) have failed. (Extreme rarity) | Multimodal pharmacotherapy, regional sympathetic blocks, spinal cord stimulation, psychological therapy, physical therapy. | Amputation is a highly controversial and absolute last-resort option, reserved for truly intractable pain in a completely non-functional limb. This decision carries immense psychological burden and has variable outcomes regarding pain relief. Pre-operative psychological and pain specialist clearance is mandatory. |
| Early/Dynamic Contracture | N/A | Aggressive, early, and continuous physical/occupational therapy, edema control, pain management, splinting. | Surgery is absolutely contraindicated in early, dynamic, or active contractures where inflammation and pain are dominant. Focus on preventing progression. |
| Active CRPS Symptoms | N/A | Aggressive CRPS-directed therapy (sympathetic blocks, neuromodulation, pharmacotherapy, desensitization). | Any surgery during an active CRPS flare (significant pain, swelling, allodynia, color changes) is strongly contraindicated due to extremely high risk of exacerbation and worsening of the condition. |
| Non-reconstructable Joint | Severe joint destruction or ankylosis leading to unacceptable functional position or intractable pain. | N/A (conservative management of joint pain) | Arthrodesis (joint fusion) to create a stable, painless, functional position. This is typically reserved for cases where motion preservation is impossible or undesirable due to pain/instability. |
Contraindications for Surgery in CRPS
Absolute contraindications include:
* Active CRPS symptoms: Any signs of ongoing inflammation, significant allodynia, hyperalgesia, significant edema, or autonomic instability. Surgery in this context almost invariably leads to a severe CRPS flare.
* Uncontrolled psychological comorbidities: Major depression, anxiety, or somatization disorder that has not been adequately addressed. These can undermine post-operative rehabilitation and amplify pain perception.
* Unrealistic patient expectations: Patients seeking pain relief exclusively from surgery, or expecting full restoration of normal function without understanding the limitations.
* Mild or reducible contractures: These should always be managed non-operatively.
* Poor general health status: Co-morbidities increasing surgical risk (e.g., severe cardiovascular disease, poorly controlled diabetes).
* Poor patient compliance: Inability or unwillingness to commit to rigorous and prolonged post-operative rehabilitation, which is paramount for successful outcomes.
The decision for surgery in late CRPS must be multidisciplinary, involving orthopedic surgeons, pain specialists, physical and occupational therapists, and often psychologists. It is a decision of last resort, carefully weighed against the significant risks of exacerbating the underlying syndrome.
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is critical for any surgical intervention in late CRPS, given the anatomical distortions, tissue fragility, and inherent risk of CRPS exacerbation. A meticulous, systematic approach minimizes complications and optimizes functional outcomes.
Comprehensive Patient Assessment
A detailed history must include the onset, progression, prior treatments (including type, duration, and response), pain characteristics (intensity, quality, triggers), and functional limitations. A comprehensive physical examination is paramount, documenting:
* Pain mapping: Differentiating mechanical pain from neuropathic or allodynic pain.
* Range of Motion (ROM): Active and passive, goniometric measurements of all affected joints, distinguishing dynamic from fixed contractures.
* Strength: Manual muscle testing, though often limited by pain or contracture.
* Sensory examination: Presence of allodynia, hyperalgesia, hypoesthesia.
* Autonomic signs: Skin temperature, color, sweating, presence of edema (though usually minimal in late CRPS).
* Skin integrity: Assessment for atrophy, fragility, trophic changes, and potential wound healing issues.
Diagnostic Imaging
- Radiographs: Plain X-rays are essential to assess joint space narrowing, subluxation, joint congruity, and regional osteopenia/osteoporosis, which is common in CRPS and affects bone quality for fixation.
- Magnetic Resonance Imaging (MRI): Provides detailed visualization of soft tissue fibrosis, tendon adherence, capsular thickening, and muscle atrophy. It helps delineate scar tissue from normal anatomy, guiding surgical planes.
- Computed Tomography (CT) Scan: Useful for complex bony deformities, osteotomy planning, and assessing joint architecture if arthrodesis is contemplated.
- Bone Scans: While classic in early CRPS for diffuse uptake, in late CRPS, uptake can be normal, decreased, or still diffusely increased (as seen in Figures 23-3 and 23-4), making interpretation challenging for active inflammation but useful for assessing chronic bone remodeling.
Psychological and Pain Management Consultation
Mandatory pre-operative psychological evaluation is necessary to assess coping mechanisms, identify underlying psychopathology, set realistic expectations, and ensure the patient understands the limitations of surgery, especially regarding pain relief. A dedicated pain management consultation is equally crucial. This involves optimizing existing analgesia, considering pre-emptive regional anesthesia (e.g., continuous peripheral nerve blocks or sympathetic blocks) to mitigate post-operative pain and reduce the risk of CRPS exacerbation, and establishing a robust multimodal post-operative pain regimen.
Surgical Goals and Patient Education
Clear, measurable functional goals must be established and communicated to the patient. Emphasize that surgery aims to improve mechanics and function, not necessarily to eradicate pain or fully restore pre-injury status. Detailed discussion of potential complications, particularly CRPS exacerbation, is vital.
Pre-operative Interventions
- Intensive physical therapy: A final course of intensive pre-operative physical therapy can optimize tissue pliability and patient readiness.
- Vitamin C prophylaxis: Some literature supports oral Vitamin C (500-1000 mg/day) starting days or weeks prior to surgery and continuing for a period post-operatively to reduce the incidence of CRPS following trauma or surgery.
- Pain optimization: Ensure the patient's baseline pain is as controlled as possible before surgery.
Patient Positioning
Patient positioning must allow for optimal surgical exposure, minimize pressure points on fragile skin, and ensure neurovascular protection.
* Upper Extremity Surgery: Typically supine position with the arm extended on a hand table, or a chest roll for lateral approach to shoulder. A tourniquet may be applied but its inflation time should be minimized or it may be omitted entirely in some cases due to CRPS sensitivity. If used, inflation pressure and duration must be carefully monitored. Regional block before tourniquet inflation may be beneficial.
* Lower Extremity Surgery: Supine, prone, or lateral position depending on the joint (e.g., hip, knee, ankle, foot). Appropriate padding for all bony prominences and careful positioning of the unaffected limb are critical.
Adequate patient positioning and meticulous attention to detail during preparation are foundational for a successful and safe surgical outcome in the context of late CRPS.
Detailed Surgical Approach and Technique
Surgical intervention in late CRPS is typically characterized by meticulous dissection, careful soft tissue handling, and often requires a combination of procedures to address the multi-planar and multi-tissue contractures. The primary objective is functional restoration, not merely cosmetic improvement. Tourniquet use is controversial; if employed, inflation time must be minimal, or a regional block should be used to minimize tourniquet-induced pain and potential CRPS flare.
General Surgical Principles
- Atraumatic Technique: Handle all tissues with extreme care to minimize tissue injury and inflammation.
- Meticulous Hemostasis: Reduce hematoma formation, which can promote fibrosis and CRPS exacerbation.
- Neurovascular Protection: Identify and protect all major neurovascular structures, which may be distorted and encased in dense scar tissue.
- Controlled Release: Gradual, sequential release of contracted structures to avoid precipitous changes that could cause further trauma or nerve injury.
- Intraoperative Range of Motion: Assess gains in motion after each release to guide further intervention.
Soft Tissue Dissection and Release
- Skin Incision: Use skin incisions that avoid tension on the atrophic skin and provide ample exposure. Z-plasty or multiple small incisions may be necessary to minimize skin contracture risk. Skin flaps should be handled gently to preserve their fragile vascularity.
- Fasciotomy and Fasciectomy:
- Palmar/Plantar Fascia: If Dupuytren-like contractures are present, a partial or total fasciectomy is performed, similar to Dupuytren's surgery. Extreme caution is exercised to protect neurovascular bundles that may be intimately associated with the fibrotic cords. The goal is complete release of the deforming bands.
- Compartment Fasciotomy: In rare cases of chronic compartment syndrome contributing to contracture, a fasciotomy may be considered, though less common in late CRPS.
- Tenolysis:
- Tendon Sheath Release: For constricted tendon sheaths causing triggering (e.g., trigger finger/thumb), the A1 pulley or other constricting bands are released.
- Tendon Adhesion Release: The affected tendon is carefully dissected free from its surrounding adherent tissues. This may involve extensive release of adhesions from the bone, joint capsule, or other tendons. Both flexor and extensor tendons can be involved. The goal is to restore smooth tendon gliding and excursion. Intraoperative assessment of tendon excursion is critical.
- Capsulotomy and Capsulectomy:
- Joint Capsule Release: Thickened and contracted joint capsules (e.g., MCP, PIP, wrist, ankle, knee) are meticulously incised or partially excised (capsulectomy). This often involves a volar/palmar approach for flexion contractures or dorsal approach for extension contractures.
- Collateral Ligament Release: Shortened and adherent collateral ligaments (e.g., MCP, PIP) are released to permit full joint excursion. Care must be taken to release only what is necessary to regain motion without destabilizing the joint.
- Arthrolysis: General term for surgical freeing of a joint. This may encompass capsular and ligamentous releases.
- Muscle Lengthening/Release:
- Intrinsic Muscle Release: For intrinsic contractures of the hand, intrinsic tenotomy or release of the intrinsic muscles may be performed to restore MP joint flexion and PIP extension.
- Extrinsic Muscle Lengthening: In severe cases, lengthening of tight extrinsic muscles may be necessary, especially in the forearm or leg, to achieve full joint motion.
Joint Mobilization and Stability
After soft tissue releases, the joint is gently manipulated through its new range of motion. Forceful manipulation should be avoided to prevent fracture, ligament avulsion, or further tissue trauma. The aim is to achieve a stable, functional range of motion. If instability is noted after release, consideration of capsular plication or ligament repair/reconstruction may be required, but this is less common in CRPS.
Adjunctive Procedures
- External Fixation or Distraction Arthroplasty: For severe, long-standing contractures, gradual distraction using an external fixator may be employed to slowly stretch contracted soft tissues and gradually regain joint motion. This can also be used to maintain surgical gains in the immediate post-operative period.
- Arthrodesis (Joint Fusion): In cases of severe, painful joint destruction, advanced osteoarthritis secondary to chronic CRPS, or a non-reconstructable joint with persistent pain and deformity, arthrodesis may be considered. The goal is to achieve a stable, pain-free joint in a functional position. This sacrifices motion for stability and pain relief.
- Amputation: This is an extremely rare and highly controversial last resort, considered only for intractable pain in a completely non-functional limb despite all other multidisciplinary interventions. The success rate for pain relief is variable, and it carries significant psychological implications. Thorough pre-operative psychological and pain management evaluations are paramount.
The choice of specific techniques depends heavily on the affected joint, the extent and type of contracture, and the patient's overall condition and goals. The overarching principle is to be as minimally invasive as possible while achieving adequate release to restore function.
Complications and Management
Surgical intervention in the setting of late CRPS carries a significantly higher risk profile than routine orthopedic procedures. The unique pathophysiology of CRPS, including pain amplification, autonomic dysfunction, and tissue fragility, predisposes patients to specific complications, the most feared of which is exacerbation of the underlying CRPS.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Estimate) | Salvage/Management |
|---|---|---|
| CRPS Exacerbation/Recurrence | Variable, up to 30-50% in some series, potentially higher in active CRPS patients undergoing surgery | Prophylaxis: Pre-emptive regional anesthesia (nerve block, sympathetic block), multimodal analgesia, Vitamin C, aggressive early post-op PT. Management: Immediate, aggressive multidisciplinary CRPS treatment protocol: regional sympathetic blocks, pharmacological agents (gabapentinoids, TCAs, NSAIDs), physical/occupational therapy (desensitization, graded motor imagery), psychological support, neuromodulation (SCS). Avoid re-operation. |
| Infection | 2-5% | Prompt diagnosis with wound culture and imaging. Aggressive antibiotic therapy (IV initially). Surgical debridement, washout, hardware removal if indicated. Meticulous wound care. |
| Wound Healing Issues | 5-15% (due to atrophic skin, poor vascularity) | Meticulous, tension-free closure. Local wound care (dressings, debridement). Nutrition optimization. Hyperbaric oxygen therapy in refractory cases. Skin grafting or local flaps for severe defects. |
| Recurrence of Contracture | High, but reduced with rehabilitation | Persistent rigorous physical therapy, dynamic splinting, passive ROM. Iterative releases or arthrodesis if functional limitations are severe and fixed. |
| **Incomplete Correction | Variable, moderate to high | Detailed pre-operative planning, intraoperative assessment of ROM. Post-operative intensive rehabilitation, dynamic splinting. If residual contracture persists and is functionally limiting, consider revision surgery, external fixation, or possibly arthrodesis. |
Specific Complications in Detail
CRPS Exacerbation
- Mechanism: Surgical stress (pain, inflammation, psychological distress) can trigger a systemic response, exacerbating the underlying dysregulation of the sympathetic nervous system and inflammatory cascades in vulnerable individuals.
- Prophylaxis:
- Regional Anesthesia: Pre-emptive peripheral nerve blocks (e.g., supraclavicular for upper extremity, femoral/sciatic for lower extremity) or continuous sympathetic blocks initiated pre-operatively and maintained for several days can significantly reduce perioperative pain and sympathetic hyperactivity.
- Multimodal Analgesia: Opioids, NSAIDs, acetaminophen, gabapentinoids, and ketamine infusions can be used in combination.
- Vitamin C: Daily oral Vitamin C (e.g., 500 mg BID) pre- and post-operatively has shown some evidence in reducing CRPS incidence after trauma and surgery.
- Psychological Support: Address anxiety and fear, which are known CRPS triggers.
- Management: Early recognition (increased pain, allodynia, swelling, temperature/color changes) is critical. Initiate aggressive multidisciplinary CRPS treatment immediately: increase regional blocks, optimize pharmacology, intensify physical therapy with desensitization, and psychological intervention.
Wound Healing Issues
- Mechanism: The atrophic, thin skin in late CRPS has compromised vascularity and elasticity. Surgical incisions are more prone to dehiscence, infection, and prolonged healing.
- Management: Meticulous surgical technique, tension-free closures, avoiding excessive electrocautery, and careful dressing application. Strict elevation and edema control are vital. Nutritional support and careful monitoring for early signs of infection. In severe cases, plastic surgery consultation for advanced wound care or flap coverage may be necessary.
Nerve Injury
- Mechanism: Scar tissue often encases and distorts normal anatomical planes, making neurovascular structures vulnerable to iatrogenic injury during dissection or retraction. Fibrotic nerves are also more sensitive to manipulation.
- Management: Meticulous, magnified dissection. Intraoperative nerve monitoring may be considered for high-risk procedures. If injury occurs, primary repair or grafting should be considered based on the extent of injury. Post-operative nerve gliding exercises and pain management for neuropathic pain.
Recurrence of Contracture
- Mechanism: The underlying fibrotic process in CRPS is progressive and often genetically predisposed. Even after successful surgical release, tissues can re-fibrose and contract, especially without diligent post-operative rehabilitation.
- Management: Aggressive and prolonged post-operative physical and occupational therapy is the primary strategy. Dynamic splinting, static progressive splinting, and continuous passive motion (CPM) devices are crucial to maintain gains. Patient education and compliance are paramount. Revision surgery may be considered for severe, functionally limiting recurrence, but with even greater caution.
Incomplete Correction
- Mechanism: The severity and chronicity of fibrosis may physically limit the achievable range of motion, even with extensive surgical release.
- Management: Realistic pre-operative patient counseling. Maximize gains through intensive rehabilitation. If residual contracture remains functionally disabling, consider serial casting, dynamic splinting, or in rare cases, further staged surgical releases or arthrodesis.
Persistent Pain
- Mechanism: Surgery addresses mechanical limitations, not the central pain processing dysfunction characteristic of CRPS. While improved mechanics might indirectly reduce some nociceptive input, neuropathic pain often persists or worsens.
- Management: Emphasize pre-operative counseling regarding pain expectations. Continue multidisciplinary pain management strategies. Neuromodulation techniques (e.g., spinal cord stimulator) may be considered if not already in place.
Surgical management of late CRPS complications demands a highly cautious, multidisciplinary, and patient-centered approach, prioritizing functional improvement while vigilantly guarding against CRPS exacerbation.
Post Operative Rehabilitation Protocols
Post-operative rehabilitation is the cornerstone of successful outcomes following surgical intervention for late CRPS contractures. It is an intensive, prolonged, and multidisciplinary effort designed to maintain surgical gains, restore function, and mitigate the risk of CRPS exacerbation. Compliance is paramount.
Immediate Post-Operative Phase (Days 0-7)
- Pain Management: Aggressive, multimodal analgesia is crucial to facilitate early motion and prevent CRPS flare. This typically includes continuous regional nerve blocks, oral analgesics (opioids, NSAIDs, gabapentinoids), and potentially ketamine infusions in selected cases.
- Edema Control: Strict elevation of the limb above heart level, gentle compression garments, and active muscle pumping exercises (if feasible) are initiated immediately.
- Early Mobilization: The golden rule in CRPS rehabilitation is early, gentle, and active range of motion (AROM). Passive range of motion (PROM) should be gentle and performed within tolerance.
- Continuous Passive Motion (CPM): Often initiated within 24-48 hours post-operatively, especially for major joint releases, to maintain motion gains and prevent re-fibrosis. Settings are adjusted to patient tolerance.
- Gentle AROM/PROM: Guided by a specialized physical/occupational therapist, focusing on maintaining the full range achieved surgically.
- Splinting: Immediate application of a static protective splint or dynamic splint in a functional position (often maximal achieved lengthening) to protect surgical repairs and prevent recurrence of contracture while allowing controlled motion.
- Desensitization: For any residual allodynia or hypersensitivity, desensitization techniques (e.g., graded textures, fluidotherapy) are initiated early.
- Psychological Support: Continued psychological counseling to manage anxiety, pain catastrophizing, and promote active participation in therapy.
Phase I: Early Mobilization and Scar Management (Weeks 1-4)
- Intensified ROM Exercises: Gradually increase the intensity and duration of active and passive ROM exercises. The focus remains on maintaining the surgically achieved range.
- Dynamic and Static Progressive Splinting: These splints are crucial to provide a prolonged, low-load stretch, gradually increasing the resting length of released tissues and countering the tendency for recurrence. Adjustments are made regularly by the therapist.
- Scar Management: As incisions heal, begin scar massage, silicone gel sheets, and other techniques to soften and mobilize the developing scar tissue, preventing adhesions.
- Pain Modulation: Continue to refine pain medication regimen. Biofeedback and relaxation techniques are emphasized.
- Weight Bearing (Lower Extremity): Gradual progression of weight-bearing as per surgeon's protocol, ensuring joint stability.
Phase II: Strengthening and Functional Integration (Weeks 4-12)
- Progressive Resistance Exercises: Once adequate ROM is achieved and maintained, and wound healing is secure, gradually introduce light resistive exercises to build strength in the newly mobilized limb. This is done cautiously to avoid exacerbating pain or inflammation.
- Functional Activities: Incorporate occupation-specific or daily living activities to integrate the increased motion and strength into meaningful function. This may include fine motor tasks for hand/wrist or ambulation drills for lower extremity.
- Endurance Training: Low-impact cardiovascular exercises to improve overall conditioning and promote blood flow.
- Advanced Splinting: Continued use of dynamic or static progressive splints, adjusting as motion improves.
- Proprioception and Balance: Exercises to restore proprioceptive input and balance, especially for lower extremity interventions.
Phase III: Return to Activity and Long-Term Self-Management (Beyond 12 Weeks)
- Activity-Specific Training: Progress to sport-specific drills, work simulations, or other high-level functional tasks.
- Maintenance Program: Establish a long-term home exercise program focusing on ROM and strength maintenance.
- Self-Management Strategies: Empower the patient with strategies for pain self-management, flare-up prevention, and recognizing signs of recurrence.
- Psychological Follow-up: Ongoing support for coping, particularly for managing chronic pain and functional limitations.
Role of the Multidisciplinary Team
Successful rehabilitation for late CRPS requires a cohesive team approach:
* Physical and Occupational Therapists: Provide hands-on therapy, exercise prescription, splinting, and functional training.
* Pain Management Specialists: Manage pharmacological and interventional pain strategies.
* Psychologists/Psychiatrists: Address psychological comorbidities, coping strategies, and pain perception.
* Surgeon: Oversees the entire process, monitors progress, and manages any complications.
The rehabilitation protocol is often individualized and requires constant communication among team members and with the patient. Patience, persistence, and a highly collaborative approach are essential for navigating the complex journey of recovery in late CRPS.
Summary of Key Literature and Guidelines
The literature supporting surgical intervention for late CRPS contractures is relatively limited, primarily consisting of case series, retrospective reviews, and expert opinion rather than high-level randomized controlled trials. This reflects the rarity of severe late-stage CRPS requiring surgery and the ethical challenges in conducting controlled trials for a condition with such variable presentation and high risk of exacerbation.
Diagnostic Criteria and General Guidelines
The International Association for the Study of Pain (IASP) Budapest Criteria remain the gold standard for CRPS diagnosis, emphasizing persistent pain, and sensory, vasomotor, sudomotor, and motor/trophic symptoms. While these criteria are primarily for diagnosis, their recognition is foundational for all management decisions.
General guidelines for CRPS management consistently advocate for a multidisciplinary approach, with non-operative therapies as the first line of treatment. Surgical intervention is positioned as a highly selective, last-resort option for severe, fixed, functionally limiting deformities that have failed exhaustive conservative measures.
Evidence for Surgical Interventions
- Contracture Release (Capsulotomy, Tenolysis, Fasciectomy): Case series often report improved range of motion and functional scores following these procedures for established contractures. However, the risk of CRPS exacerbation (ranging from 10-50% in various reports) and recurrence of contracture remains a significant concern. The overall success rates vary widely, reflecting patient selection and rehabilitation intensity. There is no consensus on optimal timing, but most recommend waiting for the "cold" or "quiescent" phase, where active inflammatory signs are minimal.
- Arthrodesis: For severely painful or destroyed joints unresponsive to other treatments, arthrodesis can provide a stable, pain-free platform. Outcomes regarding pain relief are often favorable, but at the cost of joint motion. Patient selection is crucial to ensure a functional position for fusion.
- Amputation: This is perhaps the most controversial surgical intervention in CRPS. Literature suggests that while some patients experience significant pain relief and improved quality of life post-amputation for intractable CRPS, a substantial percentage (20-50%) may experience phantom limb pain, stump pain, or even recurrence of CRPS symptoms in the stump or in the contralateral limb. Guidelines universally recommend this as an absolute last resort, only after complete failure of all other treatments, and with mandatory pre-operative psychological evaluation and extensive patient counseling.
Prophylactic Measures
- Regional Anesthesia: Strong evidence supports the use of regional anesthesia (e.g., continuous peripheral nerve blocks) to prevent CRPS after trauma or surgery. Its use in CRPS patients undergoing surgery is logically extrapolated as beneficial for mitigating perioperative pain and sympathetic activation.
- Vitamin C: Several studies suggest that prophylactic oral Vitamin C (e.g., 500 mg/day) following wrist fractures may reduce the incidence of CRPS. While not definitively proven for surgical patients with pre-existing CRPS, its low risk and potential benefit make it a reasonable consideration.
Future Directions
Research continues to explore advanced therapeutic modalities:
* Neuromodulation: Spinal cord stimulation (SCS) has shown promise in managing intractable pain, particularly for CRPS of the lower extremities. Its role in the perioperative period for late CRPS surgery is being investigated.
* Pharmacotherapy: Newer pharmacological agents targeting specific inflammatory pathways or neuropathic pain mechanisms are under investigation.
* Biological Therapies: The role of biologics and growth factors in modulating fibrosis and promoting tissue healing in late CRPS is a burgeoning area of research.
* Advanced Imaging: Developing more precise imaging techniques to identify metabolically active fibrotic tissue or nerve pathology could better guide surgical intervention.
In conclusion, the orthopedic management of late CRPS contractures remains a formidable challenge. While surgical options exist for carefully selected patients, the overriding principles are meticulous planning, conservative decision-making, meticulous technique, and an unwavering commitment to intensive, multidisciplinary post-operative rehabilitation. The potential for CRPS exacerbation necessitates extreme caution and places the onus on the surgeon to weigh the functional benefits against these substantial risks.
You Might Also Like