Ulnohumeral (Outerbridge-Kashiwagi) Arthroplasty

Introduction and Epidemiology
Primary osteoarthritis of the elbow is an uncommon but profoundly debilitating clinical entity, accounting for a mere 1% to 2% of all presentations for degenerative joint disease. In stark contrast to primary osteoarthritis of the weight-bearing joints of the lower extremity, which is largely driven by age-related chondral senescence and genetic predispositions, primary elbow osteoarthritis is fundamentally a disease of mechanical overuse and repetitive microtrauma. It demonstrates a profound demographic predilection for males, with a male-to-female ratio historically reported between 4:1 and 5:1. The archetypal patient is a middle-aged male—frequently a heavy manual laborer, competitive weightlifter, or overhead throwing athlete—who subjects the upper extremity to decades of repetitive axial loading, valgus stress, and forceful terminal extension.
The pathogenesis of primary elbow osteoarthritis is distinguished by a progressive, impingement-driven articular cartilage wear pattern. This mechanical conflict at the extremes of motion stimulates robust, hypertrophic osteophyte formation at the apices of the coronoid and olecranon processes, as well as within their corresponding fossae on the distal humerus. Crucially, in the early-to-intermediate stages of the disease process, the central radiocapitellar and ulnohumeral articular cartilage remains relatively preserved. Consequently, patients typically present with sharp, impingement-type pain specifically at the extremes of flexion and extension, accompanied by a progressive, mechanical loss of terminal motion. As the pathology advances, patients may develop mid-arc pain, mechanical catching, crepitus, and locking secondary to the proliferation of intra-articular loose bodies and capsular contracture.
To address this unique pathoanatomy, Outerbridge and Kashiwagi first described the ulnohumeral arthroplasty (now universally referred to as the OK procedure) in 1978. Designed as a joint-preserving intervention, the procedure utilizes a posterior approach to systematically decompress the impinging osseous structures. The classic operation entails the resection of the olecranon osteophyte, clearance of the olecranon fossa, and a controlled trephination (fenestration) through the supratrochlear septum. This transmalleolar window provides direct access to the anterior compartment, permitting the excision of coronoid osteophytes and the extraction of anterior loose bodies without the morbidity of a separate anterior surgical approach. Over subsequent decades, the OK procedure has been refined—most notably by Morrey, who emphasized concomitant anterior capsular release—and can now be executed via open, mini-open, or advanced arthroscopic techniques, remaining a foundational procedure in the orthopedic surgeon's armamentarium.
Surgical Anatomy and Biomechanics
A rigorous understanding of the osseous architecture, capsuloligamentous constraints, and neurovascular topography of the elbow is mandatory for the safe and efficacious execution of ulnohumeral arthroplasty. The elbow functions as a highly congruent, complex modified hinge joint comprising three distinct articulations (ulnohumeral, radiocapitellar, and proximal radioulnar) enclosed within a single continuous joint capsule.
Osseous Architecture
The distal humerus is structurally defined by two divergent columns (medial and lateral) that converge to support the articular segment, forming a biomechanical "tie-arch." This articular segment consists of the trochlea medially and the capitellum laterally. The articular surface is anatomically tilted approximately 30 degrees anterior to the longitudinal axis of the humeral shaft and is aligned in approximately 6 degrees of valgus relative to the shaft.

Proximal to these articular surfaces lie three critical anatomic depressions: the radial fossa and coronoid fossa anteriorly, and the deeper, more capacious olecranon fossa posteriorly. The osseous septum separating the olecranon fossa from the coronoid fossa is remarkably thin, often translucent, and in approximately 5% to 10% of the normal population, naturally fenestrated (the supratrochlear foramen). This thin septum forms the anatomic rationale for the Outerbridge-Kashiwagi procedure; its central removal provides unhindered access to the anterior joint space without compromising the structural integrity of the load-bearing medial and lateral columns.
The proximal ulna features the greater sigmoid notch, formed by the confluence of the olecranon posteriorly and the coronoid process anteriorly. The highly congruent notch articulates with the trochlea, providing the primary intrinsic osseous stability to the elbow joint. Notably, the articular cartilage of the greater sigmoid notch is frequently discontinuous centrally, presenting a transverse "bare area" devoid of hyaline cartilage. Surgeons must recognize this normal anatomic variant to avoid misdiagnosing it as a full-thickness chondral defect during arthroscopic or open evaluation.

Kinematics and Biomechanics
The primary function of the elbow is to position the hand dynamically in space and to stabilize the upper extremity during load-bearing and levering tasks. The physiological range of elbow flexion-extension is 0 to 150 degrees, while normal forearm pronation-supination is 80 degrees in each direction. However, seminal kinematic studies by Morrey et al. demonstrated that the functional arc of motion required for the vast majority of activities of daily living (ADLs) is a 100-degree flexion-extension arc (30 to 130 degrees) and 100 degrees of forearm rotation (50 degrees of pronation and 50 degrees of supination).
In primary osteoarthritis, hypertrophic osteophytes on the olecranon tip impinge within the contracted olecranon fossa during terminal extension, while corresponding coronoid osteophytes impinge within the coronoid fossa during terminal flexion. This mechanical block severely restricts the functional arc. The OK procedure aims to restore this arc by resecting the impinging osseous structures. Biomechanical studies have confirmed that creating a central fenestration in the olecranon fossa up to 15 mm in diameter does not significantly alter the torsional or bending stiffness of the distal humerus, provided the medial and lateral columns remain strictly unviolated.
Indications and Contraindications
Patient selection is arguably the most critical determinant of clinical success for the Outerbridge-Kashiwagi procedure. The ideal surgical candidate is a middle-aged, high-demand patient presenting with primary elbow osteoarthritis characterized by mechanical impingement pain at the extremes of motion, a relatively preserved central ulnohumeral joint space, and failure of exhaustive non-operative management.

Operative vs Non Operative Management Parameters
| Management Strategy | Indications | Considerations and Notes |
|---|---|---|
| Non-Operative Management | Mild to moderate pain, minimal functional deficit, absence of mechanical locking. | First-line treatment includes NSAIDs, activity modification, physical therapy (stretching/mobilization), and intra-articular corticosteroid or hyaluronic acid injections. |
| Ulnohumeral Arthroplasty (OK Procedure) | Pain strictly at extremes of motion, loss of terminal flexion/extension, presence of loose bodies, failure of conservative therapy > 6 months. | Requires preserved central ulnohumeral joint space. Addresses impingement but does not cure central cartilaginous wear. |
| Arthroscopic Debridement | Similar to open OK procedure, isolated loose bodies, early osteophytosis. | Technically demanding, requires advanced arthroscopic skills. Higher risk of neurovascular injury if normal capsular anatomy is severely distorted. |
| Total Elbow Arthroplasty (TEA) | Advanced, bone-on-bone osteoarthritis, inflammatory arthropathy, severe pain throughout the entire arc of motion. | Strictly contraindicated in young, active manual laborers due to lifetime lifting restrictions (typically < 10-15 lbs) and high rates of aseptic loosening. |
| Interposition Arthroplasty | Young, high-demand patients with advanced pan-articular arthritis where TEA is contraindicated. | Often utilizes Achilles tendon allograft or fascia lata. Considered a salvage procedure with unpredictable and deteriorating long-term outcomes. |
Contraindications
Absolute contraindications for the OK procedure include active or latent intra-articular infection, profound elbow instability (e.g., chronic medial ulnar collateral ligament insufficiency), and Charcot arthropathy.
Relative contraindications include advanced joint space narrowing (bone-on-bone articulation throughout the functional mid-arc), as the OK procedure will not relieve pain associated with central articular wear. Significant radiocapitellar arthritis is also considered a relative contraindication; however, if the ulnohumeral joint space remains preserved, the OK procedure can be performed concurrently with radial head excision or prosthetic radial head arthroplasty to comprehensively address the lateral compartment pathology.
Pre Operative Planning and Patient Positioning
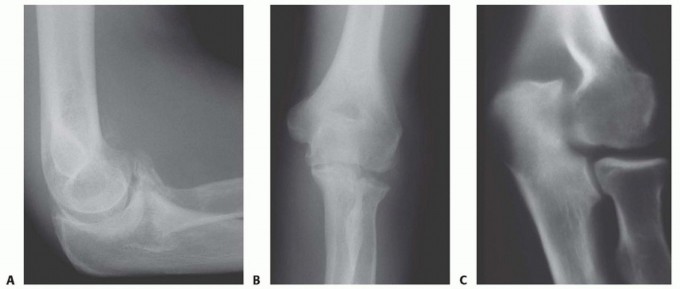
Comprehensive preoperative imaging is essential to accurately map the location and volume of osteophytes, identify intra-articular loose bodies, and quantify the degree of central joint space narrowing. Standard anteroposterior, lateral, and oblique radiographs of the elbow are mandatory. The true lateral radiograph is particularly useful for assessing the size of the coronoid and olecranon osteophytes and evaluating the depth and sclerosis of the respective fossae.

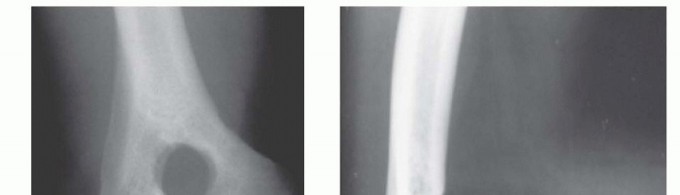
A non-contrast computed tomography (CT) scan with 3D reconstructions is currently considered the gold standard for preoperative planning in elbow osteoarthritis. The CT scan allows the surgeon to precisely localize occult intra-articular loose bodies (which frequently sequester in the radiocapitellar joint, coronoid fossa, or posterolateral gutter) and accurately measure the dimensions of the olecranon fossa to meticulously plan the diameter and trajectory of the trephination.
Patient Positioning
The procedure can be performed with the patient in either the lateral decubitus or prone position, depending on surgeon preference, airway considerations, and the presence of concomitant pathology.

In the lateral decubitus position, the patient is secured with a vacuum beanbag, and the operative arm is draped over a heavily padded L-bar or Mayo stand, allowing the elbow to flex freely to at least 120 degrees. A sterile tourniquet is applied high on the brachium.
The prone position offers unparalleled posterior exposure and is particularly advantageous if the surgeon is operating without a dedicated surgical assistant. In this setup, the arm can be rested on a padded arm board with the forearm hanging freely toward the floor, utilizing gravity to assist with flexion. In either position, all dependent bony prominences must be meticulously padded to prevent perioperative neuropraxia, and the shoulder should be positioned to avoid excessive traction on the brachial plexus.
Detailed Surgical Approach and Technique
The classic open Outerbridge-Kashiwagi procedure requires meticulous soft tissue handling and precise osseous resection to avoid iatrogenic fracture, triceps avulsion, or destabilization of the elbow joint.

Soft Tissue Dissection and Exposure
A longitudinal posterior incision is utilized, centered over the olecranon but curving slightly laterally around the tip to avoid placing the final surgical scar directly over the bony prominence, which can lead to painful bursa formation. Full-thickness fasciocutaneous flaps are elevated medially and laterally.
The ulnar nerve must be identified proximally at the medial border of the triceps and traced distally into the cubital tunnel. While routine ulnar nerve transposition is not strictly required for every OK procedure, an in situ decompression is highly recommended, releasing Osborne’s fascia and the arcade of Struthers. If the patient has preoperative clinical or electromyographic evidence of cubital tunnel syndrome, or if significant medial osteophytes require aggressive resection, an anterior subcutaneous transposition should be performed to protect the nerve from traction and alleviate tension during postoperative rehabilitation.
The triceps tendon can be managed via a triceps-splitting, triceps-reflecting (Bryan-Morrey), or triceps-sparing approach. The triceps-splitting approach is most commonly utilized for the standard OK procedure. A midline longitudinal incision is made through the triceps aponeurosis and muscle belly, extending distally to the tip of the olecranon. The medial and lateral halves of the triceps are elevated off the posterior humerus via sharp subperiosteal dissection, exposing the olecranon fossa, the posterior radiocapitellar compartment, and the posterior band of the medial collateral ligament (which must be preserved).
Ulnohumeral Arthroplasty and Trephination
Once the posterior distal humerus is adequately exposed, a thorough posterior capsulectomy is performed. Fibrotic capsular tissue and posterior loose bodies are systematically cleared to restore posterior volume.
The first osseous step is the resection of the olecranon tip osteophyte. Using a curved osteotome or a high-speed burr, the impinging osteophyte is resected flush with the normal contour of the greater sigmoid notch. Care must be taken to resect only the pathologic osteophyte; excessive removal of the native olecranon (greater than 3-5 mm) can compromise the insertion footprint of the triceps tendon or critically reduce posterior osseous stability.
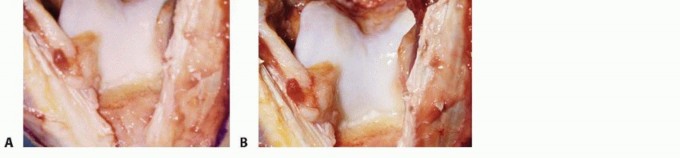
Attention is then turned to the olecranon fossa. Hypertrophic bone surrounding the fossa is debrided to restore its normal concavity. The central, translucent septum of the olecranon fossa is identified.

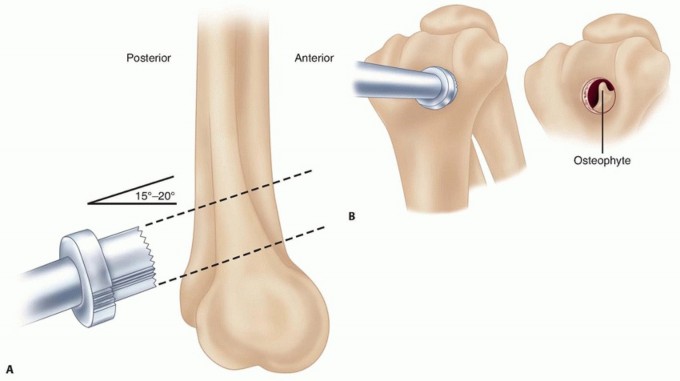
Using a high-speed round burr (e.g., 5.0 mm or 6.0 mm) or a dedicated trephine, a fenestration is created through the septum, connecting the posterior and anterior compartments. The diameter of the fenestration should be approximately 10 to 15 mm, depending on patient size. It is imperative to keep the trephination strictly central. Violating the medial or lateral columns significantly increases the risk of a catastrophic postoperative supracondylar humerus fracture.

Through this newly created transmalleolar window, the anterior compartment is visualized. The elbow is flexed to deliver the coronoid osteophyte into the window. Using a pituitary rongeur, small angled curettes, or a burr, the coronoid osteophyte is meticulously resected. To maximize postoperative extension, the anterior capsule can be systematically released from the anterior humerus through the window (the Morrey modification). A thorough, high-volume lavage is performed to flush out any remaining loose bodies or osseous debris from the anterior compartment out through the posterior window.
Once adequate decompression is confirmed by taking the elbow through a full, unimpeded range of motion under direct visualization, the wound is copiously irrigated. The triceps split is meticulously repaired with heavy non-absorbable sutures (e.g., #2 FiberWire or Ethibond), and the skin is closed in layers. A deep suction drain is routinely placed to minimize postoperative hematoma formation, which is a significant risk factor for subsequent heterotopic ossification and stiffness.
Complications and Management
While the Outerbridge-Kashiwagi procedure is highly effective for pain relief and the restoration of a functional arc of motion, it carries specific inherent risks. Meticulous surgical technique, strict adherence to anatomic boundaries, and appropriate patient selection are paramount to mitigating these complications.

Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology and Salvage Strategy |
|---|---|---|
| Ulnar Neuropathy | 5% - 10% | Caused by direct intraoperative trauma, excessive traction, or compression from postoperative hematoma/scarring. Salvage: If persistent and electromyographically confirmed, requires revision neurolysis and anterior transposition. Prevention via prophylactic in situ decompression is highly recommended. |
| Supracondylar Humerus Fracture | < 2% | Results from over-resection of the olecranon fossa, violating the medial or lateral columns and creating a critical stress riser. Salvage: Requires formal open reduction and internal fixation (ORIF) with dual orthogonal or parallel plating constructs. |
| Heterotopic Ossification (HO) | 3% - 8% | Aggressive, aberrant bone formation post-resection, leading to recurrent, profound stiffness. Salvage: Prophylactic NSAIDs (Indomethacin) or single-dose localized radiation. If mature HO causes severe restriction, revision surgical excision after maturation (typically > 6 months) is required. |
| Recurrent Impingement/Stiffness | 10% - 15% | Secondary to inadequate resection of osteophytes, failure to adequately release the anterior capsule, poor rehabilitation compliance, or progression of central joint OA. Salvage: Revision arthroscopic debridement or conversion to Total Elbow Arthroplasty (TEA) if patient age and functional demands permit. |
| Infection | 1% - 2% | Superficial surgical site infection or deep intra-articular space infection. Salvage: Prompt irrigation and debridement, followed by culture-directed intravenous antibiotic therapy. |
Post Operative Rehabilitation Protocols
The ultimate clinical success of the ulnohumeral arthroplasty is inextricably linked to the immediate initiation of a structured, aggressive postoperative rehabilitation protocol. The primary objective is to prevent capsular scarring, limit hematoma organization, and preserve the intraoperative gains in the functional arc of motion.
Phase 1: Immediate Postoperative Phase (Days 1 to 14)
The elbow is typically immobilized in a bulky, soft compressive dressing (e.g., a modified Jones dressing) for the first 24 to 48 hours to control edema and limit hematoma formation. On postoperative day 1 or 2, the dressing is reduced, and active and active-assisted range of motion exercises are initiated immediately. Gravity-assisted extension stretches and active flexion are encouraged multiple times daily. A continuous passive motion (CPM) machine may be utilized in the immediate postoperative period, although current evidence regarding its long-term superiority over dedicated active therapy remains mixed. NSAIDs (e.g., Indomethacin 75 mg SR daily or Celecoxib) are routinely prescribed for 2 to 3 weeks for both analgesia and heterotopic ossification prophylaxis.
Phase 2: Intermediate Phase (Weeks 2 to 6)
Sutures are removed at 10 to 14 days postoperatively. Physical therapy is advanced to include terminal overpressure stretching. If the patient demonstrates a loss of extension or flexion compared to the documented intraoperative arc, static progressive splinting or dynamic turnbuckle splinting is initiated. Night splinting in maximum extension is commonly employed to combat the natural, gravity-dependent tendency of the elbow to rest in a flexed posture, which promotes anterior capsular contracture.
Phase 3: Strengthening and Return to Function (Weeks 6 to 12+)
Once a functional, stable, and pain-free arc of motion is achieved, progressive isometric and isotonic strengthening of the triceps, biceps, and forearm musculature is introduced. Patients are typically cleared to return to light duty or non-strenuous activities at 6 weeks. Return to heavy manual labor, competitive weightlifting, or overhead sports is generally permitted by 3 to 4 months, provided the patient has regained adequate symmetric strength and remains asymptomatic throughout the functional arc.
Summary of Key Literature and Guidelines
The academic literature robustly supports the efficacy of the Outerbridge-Kashiwagi procedure for the surgical management of primary elbow osteoarthritis, particularly regarding reliable pain relief and the durable improvement of the functional arc of motion.
Long Term Outcomes:
Minami et al. published seminal long-term follow-up data on the OK procedure, demonstrating that over 80% of patients maintained significant pain relief and functional improvement at a minimum of 10 years postoperatively. The study critically highlighted that while radiographic progression of central joint space narrowing occurred in a subset of patients over time, it did not strictly correlate with a return of clinical symptoms, underscoring the procedure's immense value as a durable joint-preserving option.
Modifications and Advancements:
Morrey introduced critical modifications to the classic OK procedure, emphasizing the absolute importance of concomitant anterior capsular release through the fenestration to maximize postoperative extension. Morrey's outcome data suggested that patients could expect a reliable average improvement of 20 to 30 degrees in their flexion-extension arc, primarily gained at the extremes of motion where impingement previously occurred.
Arthroscopic vs Open Techniques:
Recent surgical advancements have popularized the arthroscopic ulnohumeral arthroplasty. Studies comparing open versus arthroscopic techniques (such as those by Savoie and colleagues) indicate that both modalities yield comparable improvements in range of motion and objective pain scores. The arthroscopic approach offers the theoretical advantages of decreased posterior soft tissue morbidity, faster initial rehabilitation, and improved visualization of the radiocapitellar joint. However, the arthroscopic OK procedure is technically demanding, carries a significantly steeper learning curve, and places the neurovascular structures (particularly the ulnar and radial nerves) at higher risk if the capsular anatomy is distorted by severe osteophytosis or prior trauma.
Clinical Guidelines:
Current consensus guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Shoulder and Elbow Surgeons (ASES) firmly position ulnohumeral arthroplasty (whether open or arthroscopic) as the surgical treatment of choice for young, active, or heavy-laboring patients with primary elbow osteoarthritis who have failed conservative management and present with impingement-predominant symptoms. Total elbow arthroplasty remains strictly reserved for older, low-demand patients or those with advanced inflammatory arthropathies due to the catastrophic failure rates and aseptic loosening associated with heavy lifting in TEA.
You Might Also Like


