Surgical Management of Tibial Condyle Malunions: A Comprehensive Guide

Key Takeaway
Tibial condyle malunions alter knee biomechanics, causing axial deformity, joint incongruity, and early post-traumatic arthritis. Surgical correction depends on the deformity's nature. Extra-articular malalignment often requires a transverse subcondylar osteotomy, while intra-articular step-offs necessitate an oblique osteotomy with structural grafting. Accurate restoration of the mechanical axis and joint congruity is paramount to restoring stability and preventing the need for early arthroplasty or arthrodesis.
INTRODUCTION TO TIBIAL CONDYLE MALUNIONS
Fractures of the tibial condyles (tibial plateau) represent complex intra-articular injuries that demand meticulous anatomical reduction and stable internal fixation. When these fractures heal with moderate-to-severe displacement, the resulting malunion profoundly alters the biomechanics of the knee joint. The change in the spatial orientation of the weight-bearing articular surface invariably produces an increase in the joint space on the affected side, a relative relaxation or pseudo-laxity of the collateral ligaments, and a resultant valgus or varus weight-bearing alignment. Frequently, this is accompanied by a rotational deformity of the tibial shaft.
Any such displacement must be aggressively and accurately corrected if severe disability from early-onset traumatic arthritis is to be avoided. The procedure of choice for this type of malunion is highly individualized and varies depending on the specific morphology of the fracture, the quality of the remaining articular cartilage, the patient's physiological age, and the exact source of the functional disability.
Clinical Pearl: Before surgery, apparent lateral or medial instability on clinical examination might strongly suggest that a collateral ligament requires formal reconstruction or repair. However, this is frequently a "pseudo-laxity" caused by the loss of bony support (e.g., a depressed lateral condyle allowing the femur to tilt into valgus, mimicking medial collateral ligament laxity). After precise correction of the bony deformity and restoration of the joint line, the knee joint usually regains excellent ligamentous stability without the need for soft-tissue reconstruction.
PATHOANATOMY AND BIOMECHANICAL CONSIDERATIONS
The knee is a complex hinge joint that relies on both osseous congruity and ligamentous tension for stability. The normal mechanical axis of the lower extremity passes precisely through the center of the knee joint.
Consequences of Condylar Depression
When a tibial condyle heals in a depressed position, the mechanical axis shifts toward the side of the depression. For example, a lateral condyle malunion shifts the mechanical axis laterally, increasing the joint reaction forces on the lateral compartment. This eccentric loading accelerates cartilage wear and subchondral sclerosis.
Ligamentous Implications
The collateral ligaments function under a specific resting tension. A depressed condyle shortens the distance between the femoral and tibial attachments on the affected side, leading to slackening of the ipsilateral ligament. Conversely, the contralateral ligament is subjected to chronic tensile overload. Restoring the height of the depressed condyle re-establishes the normal distance between ligamentous origins and insertions, thereby restoring isometric tension and joint stability.
PREOPERATIVE EVALUATION AND PLANNING
Thorough preoperative planning is the cornerstone of successful deformity correction.
Clinical Assessment
- Gait Analysis: Observe for a varus or valgus thrust during the stance phase of gait, which indicates dynamic instability.
- Ligamentous Examination: Perform varus/valgus stress testing at 0 and 30 degrees of flexion. Differentiate between true ligamentous laxity (soft endpoint) and pseudo-laxity due to bone loss (firm endpoint once the joint surfaces engage).
- Soft Tissue Envelope: Assess previous surgical incisions, skin quality, and the presence of any latent infection.
Radiographic Evaluation
- Standard Radiographs: Weight-bearing anteroposterior (AP), lateral, and Rosenberg (45-degree flexion PA) views of the knee.
- Long-Leg Alignment Films: Essential for calculating the Mechanical Axis Deviation (MAD) and determining the Center of Rotation of Angulation (CORA).
- Computed Tomography (CT): A fine-cut CT scan with 3D reconstructions is mandatory to delineate the exact intra-articular step-off, the presence of cavitary defects, and the rotational profile of the malunion.
SURGICAL INDICATIONS AND DECISION MAKING
The surgical strategy is dictated by the location of the deformity (intra-articular vs. extra-articular), the chronicity of the malunion, and the condition of the articular cartilage.
1. Extra-Articular Axial Malalignment
If the disability is caused mainly by axial malalignment after the depression of a condyle, but the articular surface itself remains relatively congruent (or has remodeled into a congruent but tilted surface), the weight-bearing surfaces of the tibia usually do not need to be disturbed.
* Indication: Middle-aged patients, malunions of long duration, and cases where lateral displacement is not severe.
* Procedure: Transverse subcondylar osteotomy combined with the insertion of a structural bone graft and rigid internal fixation.
2. Intra-Articular Malunion
In instances where there is a distinct, unremodeled intra-articular step-off that disrupts joint kinematics.
* Indication: Young patients, high-demand individuals, and fairly recent fractures (typically within 6 to 12 months).
* Procedure: Oblique intra-articular osteotomy through the old fracture line. The depressed condyle is mobilized, elevated, and fixed with a buttress plate and screws. The resulting metaphyseal defect must be filled with bone grafts.
3. Severe Deformity and Degeneration
Sometimes the deformity of the condyle and the resulting degeneration of the articular cartilage are so severe that joint-preserving reconstruction is impractical.
* Indication: Older patients, severe post-traumatic osteoarthritis, or massive uncontained bone loss.
* Procedure: Total knee arthroplasty (TKA) or, in cases of intractable infection or deficient extensor mechanism, knee arthrodesis.
SURGICAL TECHNIQUES
Technique 1: Transverse Subcondylar Osteotomy
This technique is utilized to correct coronal and sagittal plane deformities without violating the joint capsule.
Positioning and Setup:
The patient is placed supine on a radiolucent table. A bump is placed under the ipsilateral hip to correct natural external rotation. A sterile tourniquet is applied to the proximal thigh. Fluoroscopy must be positioned to allow unimpeded AP and lateral views of the tibia.
Surgical Approach:
1. An anterolateral or anteromedial approach is utilized depending on the direction of the planned opening wedge. For a typical valgus deformity (depressed lateral condyle), a medial opening wedge osteotomy is preferred to restore length and correct the mechanical axis.
2. The pes anserinus is retracted, and the superficial medial collateral ligament (sMCL) is carefully elevated off the proximal tibia.
Osteotomy and Fixation:
1. Guide pins are placed under fluoroscopic guidance, starting medially below the joint line and aiming toward the tip of the fibular head, leaving a lateral cortical hinge intact.
2. The osteotomy is performed using an oscillating saw and completed with thin osteotomes.
3. The osteotomy is slowly opened to the pre-calculated angle using calibrated wedges.
4. A structural autograft (iliac crest) or allograft wedge is impacted into the defect.
5. Rigid fixation is achieved using a proximal tibial locking plate.
Surgical Warning: Extreme care must be taken not to violate the lateral cortical hinge. If the hinge fractures, the construct becomes highly unstable, and a dual-plating technique (adding a lateral plate) may be required to prevent translation.
Technique 2: Intra-Articular Oblique Osteotomy
This is a technically demanding procedure aimed at restoring the articular congruity of a recently malunited fracture.
Surgical Approach:
1. The previous surgical incision is often utilized, typically an anterolateral approach with a submeniscal arthrotomy to visualize the joint surface directly.
2. The lateral meniscus is elevated and retracted superiorly with stay sutures.
Osteotomy and Elevation:
1. The old fracture line is identified. Using a fine osteotome or a high-speed burr, the malunited fragment is carefully osteotomized along the original fracture plane.
2. The depressed articular segment is mobilized. It is crucial to mobilize the segment with its underlying subchondral bone to maintain viability.
3. The segment is elevated to match the height of the intact medial plateau, restoring the joint line.
4. Elevation creates a large cavitary defect in the metaphysis. This must be densely packed with cancellous autograft or a synthetic bone substitute with high compressive strength.
Fixation:
1. The elevated fragment is provisionally held with Kirschner wires.
2. A lateral periarticular locking plate is applied to act as a buttress, preventing subsidence of the elevated fragment. Subchondral raft screws are placed directly beneath the articular surface to support the graft and cartilage.
Technique 3: The Clamshell Osteotomy for Complex Malunions
For complex diaphyseal and metaphyseal malunions that extend from the condylar region, traditional osteotomies may be insufficient. The "clamshell" osteotomy, as described by Russell et al., is a powerful technique for correcting multiplanar deformities while allowing for load-sharing intramedullary fixation.
FIGURE 58-18: A, Deformity correction in the coronal plane utilizing the clamshell osteotomy technique. B, Sagittal plane correction demonstrating the restoration of the anatomical axis prior to intramedullary nailing.
Surgical Steps:
1. Exposure: The area of maximum deformity (the CORA) is exposed.
2. Osteotomy: A transverse osteotomy is made at the apex of the deformity. A longitudinal osteotomy is then added, effectively splitting the deformed segment into a "clamshell." This intra-focal osteotomy allows the bone to be manipulated and "unfolded" to correct both rotational and angular deformities simultaneously.
3. Intramedullary Preparation: Once the deformity is mobilized, a guide wire is passed from the proximal tibia, through the osteotomy site, and into the distal fragment.
4. Reaming and Nailing: The canal is reamed, which generates autologous bone graft that fills the osteotomy site. A statically locked intramedullary nail is inserted. The clamshell fragments wrap around the nail, which acts as an internal template for straightness.
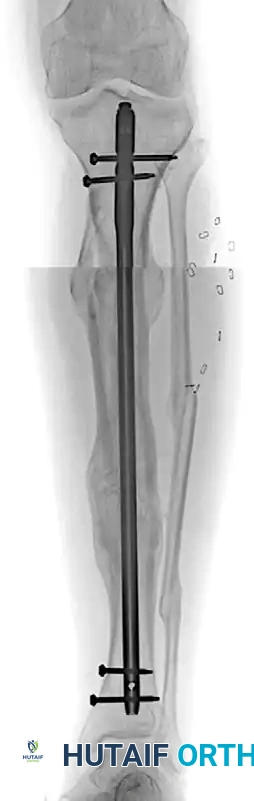
FIGURE 58-19 (A): Anteroposterior radiograph 1 year after surgery, demonstrating a healed clamshell osteotomy with excellent restoration of tibial length, coronal alignment, and joint orientation.
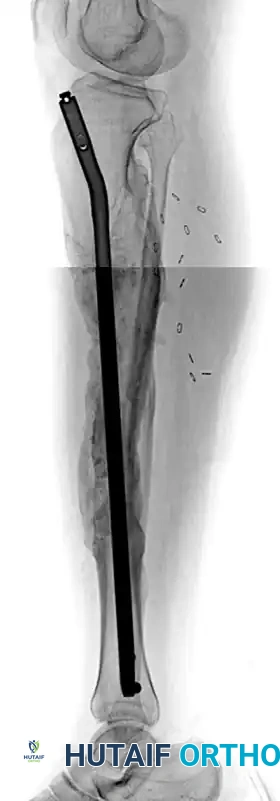
FIGURE 58-19 (B): Lateral radiograph 1 year after surgery, showing complete osseous union and restoration of the sagittal mechanical axis following intramedullary nail fixation.
Pitfall: When performing a clamshell osteotomy, meticulous handling of the soft tissue envelope is critical. Stripping the periosteum excessively from the clamshell fragments will lead to avascular necrosis of the bone segments and subsequent nonunion.
Salvage Procedures: Arthroplasty and Arthrodesis
When joint reconstruction is deemed impossible due to severe cartilage destruction, salvage procedures are indicated.
- Total Knee Arthroplasty (TKA): In older patients with severe post-traumatic arthritis secondary to a condylar malunion, TKA is the treatment of choice. However, these are highly complex arthroplasties. The surgeon must be prepared to use stems to bypass metaphyseal defects, metal augments to manage uncontained bone loss on the depressed condyle, and highly constrained polyethylene inserts (e.g., VVC or rotating hinge) if the collateral ligaments are incompetent.
- Knee Arthrodesis: Reserved for cases of intractable deep infection, massive bone loss precluding arthroplasty, or severe extensor mechanism disruption. Arthrodesis provides a stable, painless limb but sacrifices all knee motion. Intramedullary nailing is the preferred method of fixation for arthrodesis when feasible.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative protocol must balance the need for early joint mobilization to nourish the articular cartilage with the requirement for strict protection of the osteotomy site.
- Phase I (0-6 Weeks):
- Weight-Bearing: Strict non-weight-bearing (NWB) or toe-touch weight-bearing (TTWB) with crutches.
- Range of Motion (ROM): Continuous Passive Motion (CPM) machine is initiated immediately postoperatively. Active-assisted ROM is encouraged to prevent arthrofibrosis.
- Bracing: A hinged knee brace locked in extension during ambulation and sleep, unlocked for ROM exercises.
- Phase II (6-12 Weeks):
- Weight-Bearing: Progressive partial weight-bearing is initiated once radiographic evidence of early callus formation is observed at the osteotomy or graft site.
- Physical Therapy: Focus on quadriceps strengthening, hamstring flexibility, and patellar mobilization.
- Phase III (3-6 Months):
- Weight-Bearing: Progression to full weight-bearing as tolerated, contingent upon radiographic union.
- Activity: Return to low-impact activities. High-impact sports and heavy manual labor are generally restricted until 9 to 12 months postoperatively.
COMPLICATIONS AND MANAGEMENT
Surgical intervention for tibial condyle malunions carries a significant risk profile due to the altered anatomy and compromised soft tissues.
- Nonunion/Delayed Union: The metaphyseal bone of the proximal tibia generally heals well, but structural grafts may undergo delayed incorporation. Management includes prolonged protected weight-bearing, bone stimulators, or revision surgery with autogenous bone grafting.
- Infection: Post-traumatic cases, especially those with previous external fixation or compromised soft tissue envelopes, are at high risk for deep surgical site infections. Prophylactic intravenous antibiotics, meticulous soft tissue handling, and tension-free wound closure are imperative.
- Hardware Failure: Subsidence of the elevated articular fragment or failure of the locking plate can occur if the patient is non-compliant with weight-bearing restrictions or if the metaphyseal void was inadequately grafted.
- Progression of Osteoarthritis: Even with perfect anatomical restoration, the initial chondral injury at the time of the fracture may lead to progressive osteoarthritis. Patients must be counseled preoperatively that osteotomy is often a joint-prolonging procedure, not a definitive cure, and that future arthroplasty may still be required.
CONCLUSION
The management of tibial condyle malunions requires a profound understanding of knee biomechanics, meticulous preoperative planning, and advanced surgical execution. Whether employing a joint-sparing extra-articular osteotomy, an intra-articular reconstruction, or a complex clamshell diaphyseal correction, the ultimate goal remains the same: restoration of the mechanical axis, re-establishment of joint stability, and preservation of native articular cartilage to optimize long-term patient function.
You Might Also Like

