Revision THA Acetabulum: Overcoming Paprosky IIIA & Metallosis
Key Takeaway
We review everything you need to understand about Revision THA Acetabulum: Overcoming Paprosky IIIA & Metallosis. Revision THA acetabulum, specifically for Paprosky Type IIIA defects, addresses severe periacetabular osteolysis, metallosis, and ARMD following a failed primary total hip arthroplasty. This complex procedure involves solid reconstruction using trabecular metal augments, a revision shell, and bone graft to restore acetabular integrity and relieve symptoms like pain and inability to walk due to component loosening.
Revision THA Acetabulum: Overcoming Paprosky IIIA & Metallosis
Introduction & Epidemiology
Revision total hip arthroplasty (THA) for acetabular defects represents one of the most demanding challenges in reconstructive orthopedic surgery. The increasing longevity of patients, combined with extended implant survival, has led to a growing incidence of primary THA. Concomitantly, the volume of revision THA procedures is projected to rise significantly, often necessitated by aseptic loosening, periprosthetic joint infection (PJI), instability, and osteolysis. Within this complex landscape, the management of severe acetabular bone loss, particularly Paprosky IIIA defects, coupled with adverse local tissue reactions to metal debris (ARMD) or metallosis, poses exceptional difficulties.
Paprosky IIIA acetabular defects are characterized by significant cavitary bone loss that often extends beyond the confines of the acetabular rim, frequently associated with mild to moderate segmental defects of the superior or posterior acetabulum. While structural integrity of the columns may be preserved, their strength is often compromised, necessitating robust reconstruction strategies. Metallosis, a local or systemic inflammatory response to particulate metal debris (typically cobalt and chromium ions from metal-on-metal bearings or head-neck taper wear), can severely complicate revision surgery. This condition manifests as pseudotumor formation, extensive soft tissue destruction, and progressive osteolysis, rendering an already compromised acetabulum even more challenging to reconstruct.
The intersection of Paprosky IIIA defects and metallosis creates a particularly formidable scenario. Surgeons must contend with extensive bone loss, often exacerbated by metallosis-induced osteolysis, in the presence of profoundly altered and compromised soft tissue envelopes. These cases carry a significantly higher risk of complications, including infection, dislocation, and aseptic loosening, underscoring the critical need for meticulous pre-operative planning, advanced surgical techniques, and specialized implants. The goal of this review is to provide a high-yield academic reference for the management of these complex revision cases.
Surgical Anatomy & Biomechanics
A profound understanding of acetabular surgical anatomy and biomechanics is paramount for successful revision THA, especially in the context of significant bone loss and metallosis.
Acetabular Osseous Anatomy
The acetabulum is a hemispherical socket formed by the fusion of the ilium, ischium, and pubis. Key anatomical landmarks include:
*
Columns
: The anterior (ilio-pubic) and posterior (ilio-ischial) columns provide the primary structural integrity of the acetabulum. Paprosky classification relies heavily on the status of these columns.
*
Teardrop
: A radiographic landmark formed by the medial wall of the acetabulum, representing the floor of the fovea. Its disruption can indicate medial wall migration.
*
Sourcil (Roof)
: The superior weight-bearing portion of the acetabulum. Loss of this bone, typical in Paprosky IIIA, necessitates structural support.
*
Quadrilateral Plate
: The medial wall of the acetabulum. Medial migration of components occurs through this weakened area.
*
Pelvic Innominates
: The ilium (superior), ischium (inferior-posterior), and pubis (inferior-anterior) are crucial for anchorage of revision implants like cages and augments.
Neurovascular Structures
Close proximity to vital neurovascular structures necessitates meticulous dissection:
*
Sciatic Nerve
: Posterior to the acetabulum, vulnerable during posterior approaches and acetabular component removal/fixation.
*
Femoral Nerve
: Anterior to the acetabulum, within the iliopsoas groove, vulnerable during anterior approaches or extensive anterior column dissection.
*
Obturator Nerve and Vessels
: Medial to the acetabulum, susceptible during medial wall reconstruction or excessive reaming.
*
Superior and Inferior Gluteal Vessels
: Superior and posterior to the acetabulum, supply the abductor musculature, vulnerable during trochanteric osteotomy or superior acetabular dissection.
*
External Iliac Artery and Vein
: Lie anterior to the anterior column, at risk with deep penetration of screws or reamers in this region.
Biomechanics of Bone Loss & Metallosis
- Bone Loss (Paprosky IIIA) : This classification describes a significant contained cavitary defect with compromise of the peripheral rim, often superiorly. While column integrity is maintained, the bone quality is often poor and thin. The deficient weight-bearing dome requires robust reconstruction to restore the center of rotation, which has often migrated superiorly and medially. Restoration of the center of rotation improves abductor mechanics and reduces joint reactive forces.
- Metallosis/ARMD : Metal debris (Co, Cr ions) elicits a chronic inflammatory response, leading to synovial hypertrophy, pseudotumor formation, and extensive soft tissue necrosis. This pathology significantly compromises the remaining soft tissue envelope, increasing the risk of dislocation and PJI. Furthermore, metallosis-induced osteolysis can accelerate bone loss and render the remaining bone friable and structurally unsound, making stable fixation exceptionally difficult. The pseudotumor itself can exert pressure on neurovascular structures, leading to symptoms like sciatica or femoral nerve irritation.
Indications & Contraindications
Indications for Revision THA in Paprosky IIIA & Metallosis
The decision for revision THA in these complex scenarios is multifactorial, balancing potential benefits against significant risks.
- Pain and Functional Limitation : Unremitting, severe hip pain refractory to non-operative management, leading to significant functional decline and impaired quality of life.
- Aseptic Loosening / Component Failure : Radiographic evidence of acetabular component migration, fracture, or loosening, especially with associated significant bone loss (Paprosky IIIA).
- Progressive Osteolysis : Documented progression of acetabular bone loss, particularly if threatening structural integrity of the pelvis or leading to component instability.
-
Symptomatic Metallosis / Pseudotumor
:
- Persistent pain or mechanical symptoms attributable to ARMD.
- Progressive pseudotumor growth on imaging, especially if impinging on neurovascular structures (e.g., sciatic nerve compression causing motor/sensory deficits).
- Significant soft tissue destruction or osteolysis caused by metal debris, increasing the risk of periprosthetic fracture or further component failure.
- Elevated serum metal ion levels (Co/Cr) in conjunction with clinical symptoms and imaging findings consistent with ARMD, even in the absence of obvious pseudotumor.
- Recurrent Dislocation : Persistent instability despite attempts at closed reduction or conservative measures, particularly if related to component malposition or extensive soft tissue damage from metallosis.
- Periprosthetic Joint Infection (PJI) : Confirmed PJI (via aspiration, serology, and intraoperative cultures) necessitates component removal and often leads to significant bone loss, requiring subsequent complex revision.
Contraindications for Revision THA
Absolute contraindications are few, but relative contraindications require careful risk-benefit analysis.
- Uncontrolled Systemic Infection : Active infection elsewhere in the body.
- Severe Medical Comorbidities : Unacceptable operative risk (e.g., ASA IV with uncompensated cardiac, pulmonary, or neurological disease), where the risks of surgery outweigh potential benefits.
- Inadequate Soft Tissue Envelope : Inability to achieve primary wound closure, especially after extensive debridement of metallosis. This may necessitate staged procedures or flap reconstruction.
- Patient Compliance : Unrealistic patient expectations, inability to adhere to post-operative precautions and rehabilitation protocols.
- Neurological Impairment : Severe neurological deficits (e.g., non-ambulatory status due to stroke, spinal cord injury) where revision surgery offers no demonstrable functional benefit.
- Severe Acetabular Bone Loss Beyond Reconstruction : Extremely rare, but situations where no reconstructive option is feasible or durable (e.g., massive pelvic discontinuity with severe soft tissue compromise) may lead to consideration of salvage procedures like resection arthroplasty (Girdlestone) or hip fusion (arthrodesis).
Operative vs. Non-Operative Indications
| Indication Category | Operative Intervention | Non-Operative Management |
|---|---|---|
| Pain | Persistent, severe, and disabling pain unresponsive to conservative measures. | Mild-to-moderate pain manageable with activity modification, analgesics (NSAIDs, acetaminophen), physical therapy, corticosteroid injections (if appropriate for bursitis, not intra-articular with active infection). |
| Component Failure | Aseptic loosening, gross migration of components, implant fracture, polyethylene wear-through leading to symptoms or significant osteolysis. | Stable, well-fixed components with minor radiographic wear or osteolysis that are asymptomatic or have non-progressive symptoms. |
| Instability | Recurrent dislocations (typically ≥2 episodes), irreducible dislocation, or instability significantly impacting quality of life and safety. | Infrequent, easily reducible dislocations with identifiable, correctable factors (e.g., specific activities, muscle weakness), manageable with activity modification and physical therapy to strengthen periarticular muscles. |
| Infection | Confirmed Periprosthetic Joint Infection (PJI) by serological markers, joint aspiration, or intraoperative findings (pus, positive cultures). | Suspected infection with negative workup, or localized cellulitis not involving the joint itself, managed with antibiotics without implant removal. |
| Bone Loss (Paprosky IIIA) | Progressive cavitary and/or segmental bone loss (Paprosky IIIA) with associated pain, instability, or impending structural failure; any defect compromising stable implant fixation. | Stable, non-progressive bone loss (e.g., Paprosky I or IIA) without associated symptoms, instability, or risk of impending structural failure. |
| Metallosis / ARMD | Symptomatic pseudotumor (pain, neurological symptoms, mass effect), progressive soft tissue destruction, significant metal-induced osteolysis, or markedly elevated metal ion levels (Co/Cr) with correlative imaging findings (MARS-MRI/CT) indicating significant tissue reaction. | Asymptomatic elevated metal ion levels without clear clinical symptoms or significant imaging findings of pseudotumor or progressive tissue damage; stable, non-progressive pseudotumors that are incidentally found and not causing symptoms. Close surveillance is often recommended for this cohort. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful revision THA, particularly for Paprosky IIIA defects compounded by metallosis. These cases demand a comprehensive evaluation to anticipate challenges and formulate a robust reconstructive strategy.
Pre-Operative Assessment
- Detailed History : Ascertain the primary diagnosis of the original THA, prior revisions, specific symptoms (pain character, location, radiation; mechanical symptoms; neurological deficits), previous complications (infections, dislocations), comorbidities, medication list (anticoagulants, immunomodulators), and functional status. Inquire specifically about symptoms related to metallosis (groin pain, clicking, pseudotumor mass).
- Physical Examination : Assess gait, limb length discrepancy, range of motion, neurovascular status (sciatic, femoral nerve integrity), abductor strength, soft tissue integrity around the hip, and palpation for pseudotumor or sinus tracts.
-
Laboratory Investigations
:
- Routine blood work : CBC, chemistry panel.
- Inflammatory markers : ESR, CRP (essential for screening for PJI).
- Metal ion levels : Serum Cobalt (Co) and Chromium (Cr) levels are mandatory in suspected metallosis, especially in metal-on-metal or modular junction wear. Thresholds for concern vary, but generally >7-10 µg/L are highly indicative of ARMD, although clinical correlation is paramount.
- Hip Aspiration : If PJI is suspected (elevated ESR/CRP, symptoms, imaging findings), aspiration with cell count, differential, and cultures (aerobic, anaerobic, fungal) is critical. Synovial fluid analysis for alpha-defensin and leukocyte esterase can also aid diagnosis.
Imaging Modalities
-
Standard Radiographs
:
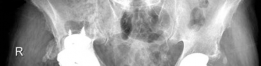
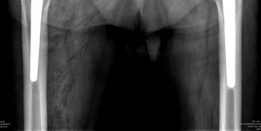
- AP pelvis, true lateral of the affected hip, and Judet views (ilio-oblique and obturator-oblique).
- These views are crucial for assessing the integrity of the anterior and posterior columns, quantifying component migration, identifying signs of loosening (lucent lines, cement mantle fractures), and preliminary classification of bone loss using the Paprosky system.
-
Specific attention to the medial wall (teardrop) and superior acetabulum.

-
Computed Tomography (CT) with Metal Artifact Reduction Sequences (MARS-CT)
:
- Indispensable for Paprosky IIIA defects and metallosis. MARS-CT provides detailed 3D visualization of bone loss, accurately quantifying cavitary and segmental defects.
- Allows precise assessment of acetabular column integrity and morphology, which is critical for planning augment or cage placement.
- Essential for evaluating pseudotumor size, location, and relationship to neurovascular structures in metallosis cases.
-
Facilitates templating for custom triflange components if necessary.
-
Magnetic Resonance Imaging (MRI) with MARS-MRI
:
- Superior for soft tissue assessment. Crucial for visualizing pseudotumors, synovial proliferation, bursitis, and muscle atrophy associated with metallosis.
- Can delineate the extent of soft tissue destruction and aid in planning the extent of debridement.
- Less effective for bone detail compared to CT in the presence of metallic implants.
- Bone Scan / PET Scan : If occult infection is suspected despite negative aspiration and normal inflammatory markers.
Templating and Implant Selection
-
Digital Templating
: Utilize templating software with current and potential revision implants. This allows for:
- Estimating the size of existing components.
- Predicting the amount of bone removal required.
- Planning for appropriate revision cup size, augments (e.g., porous tantalum, trabecular metal), or cage reconstruction.
- Assessing the need for bone grafting (allograft, autograft).
- Planning screw trajectories and lengths to achieve stable fixation, avoiding neurovascular injury.
-
Implant Selection Considerations
:
-
Paprosky IIIA Defects
:
- Porous Augments (Trabecular Metal, Porous Titanium) : Excellent for contained cavitary defects, providing biological fixation. Can be used as standalone structural support or in conjunction with a revision cup.
- Modular Revision Cups : Often larger diameter, highly porous surfaces, multiple screw holes for extensive fixation.
- Antiprotrusio Cages (e.g., Burch-Schneider) : Indicated for severe segmental defects, column discontinuity, or when a hemispherical cup cannot achieve adequate purchase. Provide mechanical stability, protecting bone graft, and are fixed to the intact portions of the ilium, ischium, and pubis. A cemented polyethylene liner or cup is then placed within the cage.
- Custom Triflange Implants : Reserved for massive, irregular defects (often Paprosky IIIB/IV, but considered for very challenging IIIA) where standard augments and cages are insufficient. Require extensive pre-operative CT-based 3D modeling and custom manufacturing.
- Metallosis : All metal-on-metal bearing surfaces must be removed. This usually entails exchanging the femoral head and acetabular liner/cup, regardless of the primary issue. The choice of new bearing surface (e.g., ceramic-on-polyethylene, ceramic-on-ceramic, or metal-on-polyethylene if infection risk is low) should be made carefully.
-
Paprosky IIIA Defects
:
Instrumentation and Resource Allocation
- Ensure availability of a full range of revision instruments, including specialized component removal tools (osteotomes, burrs, extractors), large acetabular reamers (oversized to achieve native bone), bone graft material (morselized and structural allograft), and all selected revision components.
- Anticipate significant blood loss; cross-match adequate units, ensure cell saver is available, and consider antifibrinolytic agents.
- Have neurological monitoring (SSEP/MEP) available if neurovascular injury is a high risk.
Patient Positioning
- Lateral Decubitus Position : Most commonly employed, especially for complex acetabular reconstruction via a posterior approach. Provides excellent exposure of the acetabulum, facilitating visualization of bone defects and access for implant placement and screw fixation. Ensure adequate padding of pressure points, proper stabilization of the pelvis, and clear access to both iliac crests if autograft harvest is considered.
- Supine Position : Used for anterior approaches (e.g., direct anterior or ilioinguinal), which are generally less common for complex Paprosky IIIA defects or extensive metallosis debridement due to more limited extensile exposure of the posterior acetabulum.
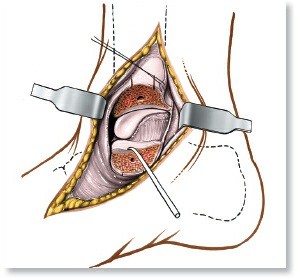
Detailed Surgical Approach / Technique
Revision THA for Paprosky IIIA and metallosis demands a systematic, meticulous approach, often exceeding the complexity of primary procedures. The paramount goals are complete removal of failed components, thorough debridement of metallosis, reconstruction of the acetabular defect, and stable fixation of new components, all while preserving neurological function and soft tissues.
Surgical Approach and Exposure
- Approach Selection : The posterior approach (Kocher-Langenbeck) is generally favored for complex acetabular revisions due to its extensile nature, allowing excellent visualization of the posterior column, ischium, and often the superior ilium. It provides direct access for component removal and reconstruction of large acetabular defects. If an existing posterolateral scar is present, it is typically utilized.
- Incision and Deep Dissection : Skin incision is usually standard. Meticulous dissection through prior scar tissue. Identify and protect the sciatic nerve early in the posterior approach. The abductor musculature often needs to be elevated or released for adequate exposure.
- Trochanteric Osteotomy : In some Paprosky IIIA cases with significant superior bone loss or when extreme exposure is required for implant removal or column reconstruction, a greater trochanteric osteotomy may be considered. This provides maximal exposure, protects the abductors, and aids in limb lengthening but adds morbidity (non-union, hardware irritation).
Component Removal
- Femoral Head Removal : Dislocate the hip. Remove the femoral head. In metallosis cases, the pseudotumor and synovium will appear dark gray/black and thickened.
-
Acetabular Component Explantation
: This is often the most challenging step.
- Cemented Cups : Use specialized osteotomes, burrs, and curettes to carefully remove the cement mantle and cup while preserving host bone.
- Press-fit Cups : Requires careful dissection of fibrous ingrowth. Specialized cup extractors (e.g., serrated blades, hooks) are used. If highly ingrown, the cup may need to be sectioned using carbide burs to preserve the underlying bone. Avoid excessive bone removal.
- Screw Removal : Identify and remove all existing acetabular screws.
Debridement of Metallosis / ARMD
This step is critical and often extensive.
1.
Systematic Excision
: All pseudotumorous tissue, granuloma, and dark-stained synovium must be meticulously excised. This involves careful dissection from surrounding healthy tissue, including around neurovascular structures. The goal is to remove as much metal-laden tissue as possible.
2.
Irrigation and Lavage
: Copious irrigation with saline throughout the debridement process to wash away microscopic debris.
3.
Biopsy and Culture
: Send multiple tissue samples for both pathology (to confirm ARMD and exclude other pathology) and microbiology (aerobic, anaerobic, fungal cultures) to rule out occult infection, as metallosis and infection can coexist or mimic each other.
Assessment of Acetabular Bone Loss (Intra-operative Paprosky Re-evaluation)
After component removal and debridement, a thorough intra-operative assessment of the remaining acetabular bone stock is performed.
*
Paprosky IIIA
: Characterized by significant superior/posterior rim deficiency and contained cavitary defects. The anterior and posterior columns generally remain intact but may be thinned or compromised. There is often medial migration of the original component through the quadrilateral plate.
Acetabular Reconstruction for Paprosky IIIA
The choice of reconstructive strategy depends on the size and location of defects, bone quality, and surgeon preference.
1.
Reaming
:
* Careful, progressive reaming is performed to healthy, bleeding bone. In Paprosky IIIA, this often means creating a non-hemispherical cavity.
* The goal is to provide a stable bed for new component fixation. Often, undersized reaming is utilized to maximize bone preservation.
2.
Bone Grafting
:
*
Cavitary Defects
: Impaction bone grafting using morselized allograft is commonly employed. The graft is packed into the defect and impacted to create a dense, stable bed that will eventually incorporate.
*
Segmental Defects
: Structural allografts (e.g., femoral head autograft/allograft) may be used to reconstruct larger rim defects, fixed with screws, but their long-term survival is variable.
3.
Porous Augments (Trabecular Metal, Porous Titanium)
:
* These are highly effective for contained cavitary and moderate segmental defects in Paprosky IIIA.
* Augments are contoured to fit the defect precisely, filling the void and restoring the acetabular shape. They provide excellent porosity for bony ingrowth and immediate mechanical stability.
* They are secured to the host bone with multiple screws.

4.
Acetabular Cage Reconstruction (e.g., Burch-Schneider, Antiprotrusio Cage)
:
* Indicated for larger segmental defects, medial protrusion, or when column support is compromised, and a primary hemispherical component cannot be rigidly fixed.
* The cage provides immediate mechanical stability by bypassing the deficient bone and fixing into stronger, intact bone (iliac crest, ischium, pubis).
* The cage is carefully positioned to restore the anatomical center of rotation and fixed with multiple screws.
* Bone graft is often placed between the cage and the host bone to promote long-term biological incorporation.
* A cemented polyethylene liner or a conventional cemented cup is then placed within the cage.

5.
Modular Revision Cups
:
* If bone loss allows for adequate peripheral rim contact (after augments or grafting), a large, highly porous revision cup with multiple screw holes can be used.
* These cups often have features for robust fixation and can be combined with augments.
6.
Custom Triflange Implants
:
* For extremely complex, irregular IIIA defects where no off-the-shelf option provides adequate stability, a patient-specific custom triflange implant may be designed based on pre-operative CT scans. These are costly and require significant lead time.
Femoral Component Management (if necessary)
- If the femoral stem is stable and well-fixed, it may be retained.
- If loose, malpositioned, or contributing to metallosis (e.g., taper corrosion), it must be revised. Femoral stem removal can be highly challenging, often requiring specialized osteotomes, burrs, trephines, or even a cortical window.
- Revision femoral stems are typically extensively porous-coated or cemented, chosen based on bone quality and canal morphology.
Trial Reduction and Final Implantation
-
Trial Reduction
: Perform a trial reduction with trial components to assess:
- Stability : Assess for impingement and dislocation in various ranges of motion.
- Limb Length : Ensure appropriate limb length and offset.
- Soft Tissue Tension : Ensure adequate soft tissue tension for stability without undue nerve stretch.
-
Definitive Implantation
:
- Implant the chosen acetabular components (augments, cage, cup).
- If a femoral stem was revised, implant the definitive stem and femoral head.
- Place the definitive liner and femoral head.
-
Reduce the hip.
Closure
- Drainage : Suction drains are typically placed due to the extent of dissection and potential for bleeding, especially after extensive debridement of metallosis.
- Layered Closure : Meticulous, layered closure of the deep fascia, subcutaneous tissues, and skin.
Complications & Management
Revision THA for Paprosky IIIA and metallosis carries a significantly higher complication rate compared to primary THA. Awareness and proactive management are crucial.
Common Complications and Their Management
| Complication | Incidence (approx.) | Salvage Strategies |
|---|---|---|
| Infection (Periprosthetic Joint Infection - PJI) | 2-5% | Debridement, Antibiotics, and Implant Retention (DAIR) for acute infections (<3-4 weeks post-op, stable implant); One-stage or Two-stage revision arthroplasty (excision of all implants and infected tissue, antibiotic spacer, delayed re-implantation); Resection arthroplasty (Girdlestone); Chronic antibiotic suppression. |
| Dislocation | 5-10% | Conservative : Closed reduction, abduction brace, activity modification. Surgical : Revision for component malposition (liner exchange, cup revision, stem revision, dual mobility bearing, constrained liner); Abductor repair (direct, allograft, or transfer). |
| Aseptic Loosening / Failure of Reconstruction | 5-15% | Repeat revision with more complex acetabular reconstruction (e.g., custom triflange, larger augments, different cage design); Bone grafting; Conversion to a Girdlestone or arthrodesis in unsalvageable cases. |
| Periprosthetic Fracture | 1-3% | Intraoperative : ORIF with cerclage wires/plates, or conversion to a revision implant with extended fixation. Postoperative : ORIF if stable, or revision if implant stability is compromised; Bone grafting as needed. |
| Neurovascular Injury | 1-2% | Sciatic nerve : Observation for spontaneous recovery (most common), neurolysis, nerve graft in rare cases; Femoral/Obturator nerve : Usually self-limiting with observation. Intraoperative monitoring (SSEP/MEP) may aid prevention. |
| Persistent Metallosis/ARMD Recurrence | Varies (if debridement incomplete) | Re-exploration, meticulous debridement of all remaining pseudotumor and metal-stained tissue; Ensuring complete removal of all previous metal-on-metal bearing surfaces and addressing any taper corrosion; Exchange of modular components if applicable. |
| Thromboembolism (DVT/PE) | <1% with prophylaxis | Therapeutic anticoagulation for DVT/PE; IVC filter placement for recurrent PE or contraindication to anticoagulation. |
| Heterotopic Ossification (HO) | 5-10% (significant) | Prophylaxis (NSAIDs/radiation therapy for high-risk patients); Surgical excision if symptomatic and mature; Radiation therapy post-excision to prevent recurrence. |
| Abductor Insufficiency / Trendelenburg Gait | 5-10% | Intensive physical therapy; Abductor repair (direct reattachment, allograft, fascia lata flap); Gluteus maximus transfer; Reverse THA (in select cases). |
| Limb Length Discrepancy | Variable | Shoe lift for minor discrepancy; Surgical revision (femoral or acetabular) for severe, symptomatic discrepancy. |
Specific Considerations for Paprosky IIIA and Metallosis
- Higher Risk of Aseptic Loosening : Due to compromised bone quality and extensive defects, achieving durable biological or mechanical fixation can be challenging.
- Incomplete Debridement of Metallosis : Can lead to recurrent pseudotumor, continued osteolysis, and chronic inflammation. Meticulous and extensive debridement is key.
- Soft Tissue Healing : The extensive soft tissue dissection and presence of metallosis can impair wound healing, increasing the risk of wound dehiscence and infection.
- Neurovascular Compromise : Pseudotumors can directly compress nerves (e.g., sciatic nerve). The extensive scarring and altered anatomy from previous surgeries and metallosis increase the risk of iatrogenic nerve injury during re-dissection.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following revision THA for Paprosky IIIA defects and metallosis is crucial for optimizing outcomes and preventing complications. Protocols are often more conservative than for primary THA, emphasizing protection of the complex reconstruction while promoting gradual restoration of function.
General Principles
- Protected Weight-Bearing : A hallmark of rehabilitation for complex acetabular revisions, particularly those involving extensive bone grafting, augments, or cages.
- Dislocation Precautions : Adherence to standard hip precautions to prevent dislocation.
- Gradual Progression : Rehabilitation progresses slowly, guided by radiographic evidence of bone healing and implant stability.
- Patient Education : Comprehensive patient education regarding precautions, exercise progression, and expected recovery timeline is vital for compliance.
Phases of Rehabilitation
Phase 1: Acute Hospitalization (Days 0-5)
*
Weight-Bearing (WB)
: Typically
toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB)
with assistive devices (walker, crutches). The duration of protected WB (often 6-12 weeks) is determined by the surgeon based on the stability of the reconstruction and the extent of bone grafting.
*
Range of Motion (ROM)
: Gentle, controlled active and passive ROM within hip precautions. Avoid extreme hip flexion (>90°), adduction past midline, and internal rotation to minimize dislocation risk.
*
Exercises
:
* Ankle pumps to prevent DVT.
* Gentle isometric quadriceps and gluteal sets.
* Assisted bed mobility and transfers.
* Gait training with appropriate assistive device.
*
Pain Management
: Aggressive multimodal analgesia.
*
Wound Care
: Monitoring incision for signs of infection or hematoma.
Phase 2: Early Home/Outpatient Rehabilitation (Weeks 1-6)
*
Weight-Bearing
: Continue TTWB or PWB as prescribed. Progressive increase in WB may begin towards the end of this phase if radiographs show early signs of healing and fixation is stable.
*
ROM
: Continue gentle, controlled ROM within precautions. Focus on restoring hip extension and promoting gradual increase in flexion.
*
Exercises
:
* Continue isometric exercises.
* Initiate gentle active-assisted and active ROM exercises (e.g., supine heel slides, abduction slides, prone hip extension).
* Light strengthening: Gluteal squeezes, hamstring curls (sitting), straight leg raises (supine, avoiding hip flexion moment).
* Core stability exercises: Pelvic tilts, gentle abdominal bracing.
* Continued gait training with emphasis on proper mechanics and maintaining precautions.
*
Precautions
: Reinforce hip precautions diligently. Avoid twisting, pivoting on the affected leg.
Phase 3: Intermediate Rehabilitation (Weeks 6-12)
*
Weight-Bearing
: Progress to full weight-bearing (FWB) with assistive devices (cane, then unassisted) as tolerated and cleared by the surgeon based on radiographic evidence of bone graft incorporation and implant ingrowth.
*
ROM
: Gradual increase in ROM, working towards functional ranges while still respecting precautions.
*
Exercises
:
* Progressive strengthening exercises for hip abductors, extensors, and flexors (e.g., standing abduction/adduction, bridging, lunges with control).
* Balance and proprioceptive training.
* Stair climbing practice.
* Initiate stationary cycling (low resistance, high seat).
*
Functional Training
: Focus on activities of daily living (ADLs).
Phase 4: Advanced Rehabilitation & Return to Activity (Weeks 12+)
*
Weight-Bearing
: Usually FWB without assistive devices.
*
ROM
: Aim for full functional ROM, respecting individual limitations.
*
Exercises
:
* Advanced strengthening: Higher resistance, multi-planar movements.
* Plyometric exercises (if appropriate for the patient's goals and implant stability).
* Sport-specific training (if applicable, highly selective).
* Cardiovascular conditioning.
*
Return to Activity
: Gradual return to light recreational activities. High-impact sports are generally discouraged.
*
Long-Term Follow-up
: Regular clinical and radiographic follow-up is essential to monitor implant stability, bone remodeling, and identify any delayed complications.
Special Considerations
- Abductor Repair : If abductor muscles were detached or significantly compromised, specific protocols focusing on abductor strengthening and protection will be implemented, often with a longer period of restricted abduction.
- Bone Grafting : Longer periods of protected weight-bearing are typical to allow for graft consolidation and incorporation.
- Metallosis Debridement : While not directly affecting weight-bearing, extensive soft tissue debridement can result in muscle weakness and altered biomechanics, requiring focused strengthening and balance training.
- Patient-Specific : Rehabilitation protocols must be individualized based on the patient's overall health, bone quality, extent of surgical reconstruction, and intraoperative findings.
Summary of Key Literature / Guidelines
The management of revision THA acetabulum, particularly Paprosky IIIA defects and metallosis, has evolved significantly, guided by extensive research and clinical experience. Key literature and guidelines emphasize classification, reconstruction principles, and the unique challenges posed by metallosis.
Paprosky Classification and Reconstruction Strategies
- Paprosky's Classification : The seminal work by Paprosky, Perona, and Lawrence (1994, 1999) on acetabular bone defects remains the gold standard for guiding reconstructive options. Paprosky IIIA defects, characterized by extensive cavitary loss and compromised peripheral rim with intact but attenuated columns, necessitate robust solutions.
- Porous Augments : Numerous studies support the use of highly porous augments (trabecular metal, porous titanium) for contained and cavitary defects, often combined with impaction bone grafting. These augments offer excellent biological fixation potential and restore structural integrity. Long-term studies demonstrate good survival rates for augments in Paprosky II/IIIA defects, with complication rates comparable to other revision techniques.
- Antiprotrusio Cages : When segmental bone loss is significant or column support is compromised, antiprotrusio cages (e.g., Burch-Schneider) are effective. Studies on cages for severe defects (Paprosky IIIA/B) show reasonable long-term results, although aseptic loosening rates can be higher than for augments, particularly in younger, more active patients. Cementation of a polyethylene liner or cup within the cage remains the standard technique.
- Custom Triflange Implants : For truly massive and irregular defects (often Paprosky IIIB/IV, but occasionally very challenging IIIA), custom triflange acetabular components, fabricated from pre-operative CT scans, offer a patient-specific solution. While early results are promising, these are expensive, require specialized planning, and long-term data is still accumulating.
Management of Metallosis and ARMD
- Diagnosis and Screening : Guidelines from organizations like the British Orthopaedic Association (BOA) and the American Academy of Orthopaedic Surgeons (AAOS) recommend screening high-risk patients (e.g., those with MoM bearings, unexplained pain, or audible squeaking) with plain radiographs, and if concerns persist, with serum metal ion levels (Co/Cr) and MARS-MRI/CT. Elevated metal ion levels (typically >7-10 µg/L) with corresponding clinical symptoms or imaging findings often warrant intervention.
- Surgical Debridement : Consensus guidelines emphasize the critical need for meticulous and complete debridement of all metallosis-induced pseudotumorous tissue, granuloma, and dark-stained synovium during revision surgery. Incomplete debridement is associated with recurrence of ARMD symptoms and implant failure.
- Bearing Surface Exchange : All metal-on-metal bearing surfaces and any corroded modular junctions (e.g., head-neck taper) must be removed and replaced with alternative bearings (e.g., ceramic-on-polyethylene, ceramic-on-ceramic) to eliminate the source of metal debris.
Outcomes and Challenges
- Revision THA, particularly for Paprosky IIIA defects and metallosis, consistently demonstrates lower long-term survival rates and higher complication rates (e.g., infection, dislocation, aseptic loosening) compared to primary THA.
- Outcomes are highly dependent on the surgeon's experience, meticulous surgical technique, and appropriate implant selection tailored to the specific defect.
- Bone graft incorporation and implant ingrowth can be unpredictable in compromised host bone.
- The extensive soft tissue damage and inflammation associated with metallosis can further complicate wound healing and increase susceptibility to PJI.
In conclusion, managing revision THA with Paprosky IIIA defects and metallosis represents a frontier of complex orthopedic reconstruction. Adherence to established classification systems, thorough pre-operative planning utilizing advanced imaging, meticulous surgical execution including comprehensive debridement and appropriate reconstructive techniques, and structured post-operative rehabilitation are paramount for achieving the best possible outcomes in these challenging cases. Continued research and technological advancements aim to further improve the longevity and functional results for this patient population.
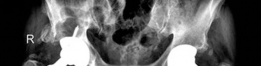
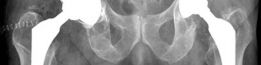
Clinical & Radiographic Imaging
You Might Also Like