Revision Hip Success: Unpacking The Case Title Acetabular Grafting
Key Takeaway
This article provides essential research regarding Revision Hip Success: Unpacking The Case Title Acetabular Grafting. Acetabular impaction grafting, detailed in this case title, treats a loosened hip replacement with a large acetabular bone defect. The procedure reconstructs the acetabulum using metallic meshes and morselized bone allograft, followed by cementing a new cup. This restores hip function for patients experiencing groin pain and walking restrictions, such as a 78-year-old female.
Revision Hip Success: Unpacking Acetabular Grafting
Patient Presentation & History
We present the case of an 82-year-old male, independent in his activities of daily living, who presented with progressively worsening right hip pain, instability, and a limp over the past 18 months. He underwent a primary cementless total hip arthroplasty (THA) on the right side 15 years prior for debilitating osteoarthritis. His initial post-operative course was uneventful, and he enjoyed excellent function for over a decade.
His pain is now described as dull, aching, localized to the groin and lateral hip, and exacerbated by weight-bearing and activity. He reports a sensation of "giving way" or instability, particularly when rising from a seated position or traversing uneven ground. He denies any acute trauma, fevers, chills, or systemic symptoms. His past medical history is significant for well-controlled hypertension, hyperlipidemia, and early-stage chronic kidney disease (CKD stage 2). He is a non-smoker and has no history of diabetes or immunosuppression. He is ambulatory with a single point cane for longer distances.
Upon initial presentation to an outside facility, plain radiographs demonstrated evidence of acetabular component migration, likely superior and medial, with significant osteolysis surrounding the prosthesis. A thorough infection workup, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), was within normal limits. Joint aspiration was attempted but yielded a dry tap. Given the absence of systemic symptoms and normal inflammatory markers, periprosthetic joint infection (PJI) was deemed unlikely at that stage, pointing towards aseptic loosening.
Clinical Examination
On physical examination, the patient was observed to have an antalgic gait with a Trendelenburg sign on the right side. A measurable leg length discrepancy of approximately 2 cm, with the right leg appearing shorter, was noted. Skin integrity around the previous surgical incision was intact, without signs of erythema, warmth, or drainage. There was no palpable mass or significant soft tissue swelling.
Palpation elicited tenderness over the greater trochanter and anterior groin region. Active and passive range of motion (ROM) of the right hip was severely restricted and painful. Flexion was limited to 70 degrees, abduction to 10 degrees, adduction to 0 degrees, internal rotation to 5 degrees, and external rotation to 10 degrees. He demonstrated significant pain at the extremes of motion and with axial loading of the limb.
Neurological assessment revealed intact sensation to light touch in the L2-S1 dermatomes. Motor strength was 5/5 in bilateral lower extremities for hip flexion, extension, abduction, adduction, knee flexion, extension, and ankle dorsi/plantarflexion. Distal pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were palpable and symmetrical bilaterally. Capillary refill was brisk in all digits. No signs of deep vein thrombosis were noted. The patient was unable to perform a single-leg stance due to pain and instability.
Imaging & Diagnostics
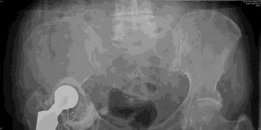
Initial plain radiographs, reviewed from the outside institution, demonstrated significant superior and medial migration of the acetabular component. The cup was clearly loose, with signs of progressive periprosthetic lucencies exceeding 2mm in all three zones, indicative of aseptic loosening. There was evidence of extensive acetabular bone loss, particularly in the superior dome and medial wall, consistent with Type IIB or Type III Paprosky defects. Protrusio acetabuli was evident. The femoral component appeared stable radiographically, without significant subsidence or periprosthetic lucencies.
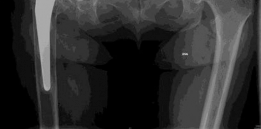
Figure 1: Initial AP pelvis radiograph demonstrating significant superior and medial migration of the acetabular component, with extensive periacetabular osteolysis and protrusio.
Given the complexity of the anticipated revision, a computed tomography (CT) scan of the pelvis with 3D reconstructions was obtained for precise assessment of the bone defect morphology and extent. The CT confirmed severe acetabular bone deficiency, involving the superior dome, anterior and posterior columns, and extensive medial wall erosion, with a large contained defect superiorly and medially. The ischial tuberosity was compromised. There was no evidence of pelvic discontinuity on the initial CT, but severe bone loss raised this as a potential intraoperative finding.

Figure 2: Coronal CT reconstruction highlighting the extent of medial wall erosion and superior dome bone loss, confirming a substantial Paprosky Type III defect.
Templating was performed using both digital software and physical templates. This involved:
1.
Estimating the true acetabular dimensions:
Identifying the intact portions of the acetabulum, particularly the anterior and posterior columns, and the ischial tuberosity, to determine the appropriate host bone for a revision construct.
2.
Assessing bone loss:
Quantifying the extent of uncontained and contained defects. The medial wall deficiency was particularly notable, suggesting the need for medial augmentation or a cage.
3.
Provisional component selection:
Initial templating suggested the need for a highly porous acetabular cup with screws for primary fixation, potentially augmented with a bulk structural allograft for the superior dome defect or an acetabular reconstruction cage to bridge defects and provide stable fixation points. Due to the extent of medial wall loss and potential for medial migration, a cementless cup with supplemental screws and a posterior column screw was considered, potentially combined with a contained impaction grafting technique or a cage. The Paprosky Type III defect strongly indicated the necessity for significant reconstructive options beyond a simple cementless cup.
4.
Leg length discrepancy correction:
Planning for restoration of leg length, which would involve careful selection of femoral head size and neck length.
The pre-operative workup also included a full blood count, renal function tests, liver function tests, and coagulation profile, all of which were within acceptable limits for elective surgery. Repeat ESR and CRP remained normal, further reducing the likelihood of active infection.
Differential Diagnosis
The presentation of chronic hip pain, instability, and radiographic evidence of component migration in a patient with a prior THA necessitates a careful differential diagnosis.
| Feature | Aseptic Loosening with Acetabular Bone Loss (Likely Diagnosis) | Periprosthetic Joint Infection (PJI) | Periprosthetic Fracture (Non-traumatic) |
|---|---|---|---|
| History | Gradual onset pain, instability, increasing limp. No systemic symptoms. Long symptom duration. | Acute or subacute pain, possibly systemic symptoms (fevers, chills, fatigue). Redness, warmth, drainage possible. Shorter symptom duration usually. | Sudden increase in pain, often with a specific event (even minor trauma like twisting or standing). Sometimes atraumatic if stress fracture. |
| Clinical Exam | Painful ROM, restricted motion, instability, leg length discrepancy. No signs of infection. | Warmth, erythema, swelling, sinus tract/drainage. Severe pain with any motion. May have systemic signs (tachycardia, fever). | Acute tenderness, crepitus (if unstable), acute deformity, severe pain, inability to bear weight. |
| Imaging (X-ray/CT) | Component migration, extensive periprosthetic lucencies (>2mm in multiple zones), osteolysis, significant bone loss. No fracture line. | Component loosening/migration. May show aggressive osteolysis. No pathognomonic radiographic signs for infection, but can look similar to aseptic. | Visible fracture line (e.g., Vancouver type B/C for femoral, acetabular fracture around components). Calcar/cortex hypertrophy if chronic stress. |
| Labs (ESR/CRP) | Typically normal or mildly elevated (if chronic inflammation). | Markedly elevated ESR/CRP (>30/10 mg/L usually). Joint aspiration with elevated WBC count (>3000 cells/µL, >80% PMNs). Positive cultures. | Usually normal, unless there is significant hematoma or systemic response to injury. |
| Treatment Implications | Revision THA with bone reconstruction, often involving grafts or cages. | Debridement, antibiotics, implant retention (DAIR) if acute, or two-stage revision (explant, spacer, reimplant) for chronic cases. | Open reduction internal fixation (ORIF) or revision THA depending on fracture type and component stability. |
Surgical Decision Making & Classification
The decision for operative intervention was straightforward in this case. The patient's debilitating pain, functional impairment, and radiographic evidence of severe aseptic acetabular component loosening with extensive bone loss mandated surgical revision. Non-operative management, such as activity modification, bracing, or analgesics, would not address the underlying mechanical failure, progressive bone loss, or functional deficits, and would ultimately lead to further deterioration of the joint and increased morbidity.
The acetabular bone defect was classified using the
Paprosky Acetabular Defect Classification System
:
*
Paprosky Type I:
Minimal or no bone loss.
*
Paprosky Type II:
Significant cavitary defects.
*
Type IIA:
Less than 50% acetabular bone loss, intact rim.
*
Type IIB:
Greater than 50% bone loss, intact rim.
*
Type IIC:
Compromised rim, but contained defects.
*
Paprosky Type III:
Extensive bone loss, often involving pelvic discontinuity.
*
Type IIIA:
Cavitary and segmental defects, but less than 50% superior migration, usually no pelvic discontinuity.
*
Type IIIB:
Significant segmental loss, often superior migration greater than 50% of the normal acetabular diameter, with or without pelvic discontinuity.
Based on our detailed imaging and pre-operative assessment, this case was classified as a Paprosky Type IIIB acetabular defect . This classification was chosen due to the extensive cavitary bone loss, significant superior and medial migration of the component, and erosion of the medial wall and superior dome, which compromised more than 50% of the host acetabulum. While overt pelvic discontinuity was not definitively diagnosed pre-operatively, the severity of the defect mandated preparation for this possibility, including the availability of long reconstruction plates or custom triflange components. The substantial superior migration suggested a Type IIIB rather than IIIA.
The American Academy of Orthopaedic Surgeons (AAOS) Acetabular Bone Graft Classification would also classify this as a Combined Deficiency , indicating a combination of cavitary and segmental defects.
Given the Type IIIB defect, a standard cementless revision cup alone would be insufficient to provide durable fixation and restore the hip center. Therefore, surgical strategy revolved around:
1. Removal of the loose acetabular component and debridement of granulomatous tissue.
2. Addressing the significant bone loss using structural allograft, combined with a highly porous cementless cup and supplemental screw fixation, or a reconstruction cage. Given the extent, the primary plan was for a structural allograft with a cup, but a cage was on standby.
3. Restoration of the hip center of rotation.
4. Restoration of leg length and offset.
Surgical Technique / Intervention
The patient was positioned in the lateral decubitus position on a traction table, ensuring careful padding of all bony prominences. A beanbag was used to stabilize the torso. The approach chosen was a posterior approach , utilizing the existing skin incision. This approach provides excellent exposure to the acetabulum, especially the posterior column and superior dome, which were areas of significant concern for bone loss.
Exposure:
The incision was extended proximally and distally as needed. The skin, subcutaneous tissue, and fascia lata were incised. The gluteus maximus was split along its fibers, and the short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) were identified and tenotomized at their insertion on the greater trochanter, carefully protecting the sciatic nerve. A careful capsulotomy was performed.
Component Removal:
The femoral head was dislocated. The pseudomembrane and granulomatous tissue surrounding the acetabular component were meticulously debrided and sent for frozen section and microbiology culture, despite the low pre-operative suspicion of infection. The loose acetabular shell was carefully explanted. Given the significant osteolysis, the removal was relatively straightforward, with minimal remaining host bone attached to the implant. After removal, the extent of the Paprosky Type IIIB defect became evident, confirming the pre-operative templating. Extensive cavitary defects were present superiorly, anteriorly, and posteriorly. A large contained defect was present medially, with significant erosion of the medial wall. The ischial tuberosity was deficient. Importantly, there was no gross evidence of pelvic discontinuity identified after careful probing and assessment of the columns.

Figure 3: Intraoperative image demonstrating the extensive acetabular bone loss after explantation of the loose component. Note the significant superior and medial wall deficiency.
Acetabular Reconstruction with Structural Allografting:
The remaining host bone was meticulously debrided of all fibrous tissue and sclerotic bone until bleeding bone was encountered. The defects were carefully assessed again. Given the extensive superior and medial contained defect, a structural allograft reconstruction was planned. A cryopreserved
femoral head allograft
was selected. This allograft was meticulously sculpted to fit the superior-medial cavitary defect, aiming to restore the host bone stock and provide a stable platform for cup impaction. The contact between the allograft and the bleeding host bone was maximized to promote biological integration.
The allograft was initially secured with multiple cancellous screws into the remaining host bone, ensuring excellent compression and stability. The reconstruction was aimed at restoring the anatomical hip center of rotation.

Figure 4: Intraoperative view demonstrating the carefully sculpted structural femoral head allograft being impacted into the superior-medial defect, secured with multiple cancellous screws.
Acetabular Cup Implantation:
Following stable fixation of the structural allograft, the augmented acetabulum was reamed sequentially. Reaming was performed carefully, initially to remove any residual fibrous tissue and then progressively to achieve a hemispherical shape, aiming for maximum contact with both the allograft and the remaining host bone. The goal was to achieve at least 50% host bone coverage of the revision acetabular component. A size 60 mm highly porous titanium cementless acetabular shell was chosen. This cup provided good press-fit stability against both the allograft and the host bone, with a goal of achieving at least 3-4 mm of undersizing. The cup was impacted into position, ensuring appropriate version and inclination.
Supplemental screw fixation was then applied through the dome of the acetabular component into the ilium superiorly and posteriorly, utilizing three 45mm cancellous screws for enhanced primary stability. One additional screw was placed through the posterior column for additional purchase. The hip center of rotation was successfully restored, and leg length was visually equalized.

Figure 5: Intraoperative image showcasing the definitive acetabular reconstruction with the porous cementless cup implanted after successful allograft integration and secure screw fixation.
Femoral Stem Assessment and Trial Reduction:
The existing femoral stem was found to be well-fixed and stable. No signs of loosening or osteolysis were evident around the femoral component. Therefore, the femoral stem was retained. A trial reduction was performed with various head sizes and neck lengths to optimize stability, leg length, and soft tissue tension. An optimal combination was found, providing excellent stability through a full range of motion without impingement or dislocation. A 36mm ceramic femoral head on a standard length neck was chosen.
Final Implantation and Closure:
The definitive ceramic femoral head was impacted onto the femoral trunion. The hip was reduced. A thorough inspection confirmed stability through a full range of motion. The short external rotators were repaired through transosseous drill holes in the greater trochanter. The capsule was repaired. The gluteus maximus was approximated. Fascia lata was closed, followed by subcutaneous tissue and skin closure in layers. A sterile dressing was applied.
Figure 6: Post-operative AP pelvis radiograph demonstrating the well-positioned acetabular component, structural allograft, and restored hip center of rotation. The femoral stem is retained.
Post-Operative Protocol & Rehabilitation
The patient was mobilized on post-operative day 1 with protected weight-bearing. Given the extensive acetabular reconstruction with structural allograft, a strict toe-touch weight-bearing (TTWB) protocol was initiated for 6 weeks, progressing to partial weight-bearing (PWB) for another 6 weeks. This protected weight-bearing period is crucial to allow for initial allograft incorporation and osseointegration of the acetabular component.
Key components of the post-operative protocol included:
*
Deep Vein Thrombosis (DVT) Prophylaxis:
Low molecular weight heparin (LMWH) for 4-6 weeks post-operatively, combined with sequential compression devices (SCDs) while in the hospital.
*
Pain Management:
Multimodal analgesia including NSAIDs (if not contraindicated), acetaminophen, and judicious use of opioid analgesics.
*
Antibiotics:
Prophylactic intravenous antibiotics (e.g., Ancef) for 24-48 hours, followed by oral antibiotics for another 5 days based on local protocol and intraoperative cultures.
*
Hip Precautions:
Strict posterior hip precautions were enforced for 6-12 weeks to minimize the risk of dislocation, particularly given the posterior approach. This included avoiding hip flexion beyond 90 degrees, internal rotation, and adduction past midline.
*
Physical Therapy:
*
Phase 1 (Weeks 0-6):
Focus on protected mobility, gentle passive and active-assisted range of motion within precautions, isometric gluteal and quadriceps strengthening. Gait training with TTWB using a walker.
*
Phase 2 (Weeks 6-12):
Gradual progression to partial weight-bearing. Increased active ROM, light resistance exercises for hip abductors, extensors, and external rotators. Core strengthening.
*
Phase 3 (Weeks 12+):
Full weight-bearing as tolerated. Progression to functional exercises, balance training, and advanced strengthening. Return to light activities.
*
Follow-up:
Regular clinical and radiographic follow-up at 2 weeks, 6 weeks, 3 months, 6 months, and annually thereafter to monitor component stability, allograft integration, and overall function.
Pearls & Pitfalls
Pearls:
1.
Meticulous Pre-operative Planning:
This is paramount for complex revision cases. Detailed CT scans with 3D reconstructions are indispensable for accurate assessment of bone loss (Paprosky classification), templating, and identifying potential pelvic discontinuity. Anticipate and plan for all eventualities, including the need for specialized implants (e.g., reconstruction cages, custom components) and structural allografts.
2.
Adequate Exposure:
A extensile approach (e.g., posterior with trochanteric osteotomy or extended trochanteric osteotomy if needed for femoral revision, although not in this case) is often necessary to safely remove components, debride host bone, and reconstruct the acetabulum without compromising neurovascular structures.
3.
Thorough Debridement:
Removal of all fibrous tissue, granuloma, and sclerotic bone is critical to promote allograft integration and host bone ingrowth into the new acetabular component. Bleeding bone must be achieved. Always send intraoperative samples for culture and frozen section, even with a low suspicion of infection.
4.
Allograft Preparation and Fixation:
Structural allografts (e.g., femoral head) must be carefully sculpted to maximize contact with viable host bone. Secure fixation with multiple screws is essential for initial stability and to allow for biological integration. Avoid gaps between the graft and host bone.
5.
Restore Hip Center of Rotation:
This is crucial for biomechanical efficiency, soft tissue tension, and reducing wear rates. Use anatomical landmarks and templating to guide reconstruction. Medialization and inferiorization of the hip center are often goals in revision.
6.
Achieve Primary Stability:
Whether using structural allograft, impaction grafting, or a cage, the revision acetabular component must achieve robust primary stability, ideally with press-fit and supplemental screws, to allow for secondary biological fixation. Aim for at least 50% host bone coverage of the implanted cup.
7.
Consider Impaction Grafting:
For contained defects, impaction bone grafting can be an excellent technique to reconstruct acetabular defects, allowing for placement of a cemented or cementless cup. The use of morselized cancellous allograft packed tightly can induce osteoinduction and osteoconduction.
8.
Sciatic Nerve Protection:
Be vigilant, especially during posterior approach revisions, as the sciatic nerve is at increased risk due to scarring and potential bone distortion.
Pitfalls:
1.
Inadequate Bone Loss Assessment:
Underestimating the extent of bone loss pre-operatively can lead to intraoperative surprises, prolonged surgical time, and an inability to achieve adequate fixation.
2.
Insufficient Primary Stability:
Placing a revision cup without sufficient host bone support or supplemental fixation will inevitably lead to early failure. Relying solely on a press-fit in a severely compromised acetabulum is a common pitfall.
3.
Pelvic Discontinuity:
Missing or inadequately addressing pelvic discontinuity is a catastrophic pitfall. If suspected or encountered, specialized techniques like reconstruction cages, plates, or custom triflange components are mandatory to bridge the defect and stabilize the columns.
4.
Neurovascular Injury:
Scar tissue from previous surgeries increases the risk of sciatic nerve injury (posterior approach), femoral nerve injury (anterior approach), and damage to vascular structures. Meticulous dissection and identification of critical structures are paramount.
5.
Infection:
Despite negative pre-op workup, infection can still be present. Failure to recognize and treat intraoperative signs of infection (purulence, necrotic tissue, positive frozen section) can lead to early failure of the revision.
6.
Ignoring Femoral Side:
While the focus was on the acetabulum in this case, a pitfall would be to ignore potential issues with the femoral stem (e.g., stress shielding, osteolysis, impending fracture) that might require simultaneous revision.
7.
Inadequate Post-operative Protection:
Premature or excessive weight-bearing after extensive allografting can lead to graft collapse, non-union, or loosening of components, especially during the critical initial healing phase. Strict adherence to weight-bearing restrictions is essential.
8.
Heterotopic Ossification:
Complex revisions, especially with extensive soft tissue dissection, are at higher risk for heterotopic ossification (HO). Prophylaxis (e.g., NSAIDs or radiation therapy) should be considered in high-risk patients.
Clinical & Radiographic Imaging

You Might Also Like