Primary Total Hip Arthroplasty: A Detailed Clinical Case Study of Severe OA
Key Takeaway
Diagnosing severe hip osteoarthritis for primary total hip arthroplasty includes detailed patient history and comprehensive physical examination. Essential X-ray imaging typically reveals Kellgren-Lawrence grade IV changes, like severe joint narrowing and osteophytes. Digital templating guides precise surgical planning, ensuring optimal implant selection and placement for successful arthroplasty.
Patient Presentation & History
A 68-year-old male presented with a 5-year history of progressive, debilitating left hip pain. The pain was insidious in onset, localized primarily to the groin and lateral thigh, and exacerbated by weight-bearing activities, prolonged standing, and initiation of movement after rest. He described a mechanical catching sensation occasionally and significant stiffness in the mornings, lasting approximately 45 minutes. His functional capacity had significantly deteriorated, limiting his ability to walk more than 100 meters, ascend/descend stairs, and perform activities of daily living such as putting on shoes or driving. He reported chronic use of over-the-counter NSAIDs with transient relief, followed by several courses of prescription NSAIDs, physical therapy, and a single intra-articular corticosteroid injection approximately 18 months prior, which provided only 3 months of partial pain reduction.
Relevant medical history included well-controlled hypertension (on a thiazide diuretic), hyperlipidemia (on a statin), and diet-controlled Type 2 Diabetes Mellitus (HbA1c 6.5%). He had a remote history of remote appendectomy and no prior hip trauma or surgeries. He was a non-smoker and consumed alcohol socially. His BMI was 29 kg/m². He lived independently and was motivated for surgical intervention to improve his quality of life and maintain an active lifestyle, including gardening and occasional cycling. There was no family history of significant orthopedic conditions.
Clinical Examination
Inspection
Observation revealed an antalgic gait pattern with a compensatory lurch to the left. The patient preferred to externally rotate the left lower extremity slightly. There was mild quadriceps and gluteal atrophy on the left side, with no overt swelling, erythema, or skin changes around the hip joint. A subtle apparent leg length discrepancy (LLD) with the left shorter by approximately 1.5 cm was noted, primarily due to fixed adduction and flexion deformity. Spinal examination was unremarkable, ruling out overt lumbar radiculopathy contributing to hip symptoms.
Palpation
Palpation elicited tenderness over the anterior hip capsule and greater trochanter on the left. No palpable masses or crepitus were identified. Distal pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were all bilaterally strong and symmetrical.
Range of Motion (ROM)
Active and passive ROM of the left hip was significantly restricted and painful.
*
Flexion:
80° (normal >120°) with a firm, painful end-feel.
*
Extension:
0° (normal 15-20°) with a fixed flexion deformity of 10°.
*
Abduction:
15° (normal 40-50°).
*
Adduction:
10° (normal 20-30°).
*
External Rotation:
20° (normal 40-50°).
*
Internal Rotation:
5° (normal 30-40°) with severe pain.
Trendelenburg sign was positive on the left, indicating gluteal abductor weakness or insufficiency related to pain and disuse.
Neurological/Vascular Assessment
Neurological examination of the left lower extremity revealed intact sensation to light touch in all dermatomes (L2-S1). Motor strength was 5/5 in all major muscle groups (hip flexion, extension, abduction, adduction, knee flexion, extension, ankle dorsiflexion, plantarflexion) except for mild weakness in hip abduction (4+/5), likely secondary to disuse and pain inhibition. Deep tendon reflexes (patellar, Achilles) were 2+ bilaterally and symmetrical. Capillary refill was brisk in all digits. No signs of neurovascular compromise were present.
Imaging & Diagnostics
X-ray Findings
Anteroposterior (AP) pelvis, frog-lateral, and true lateral views of the left hip were obtained.
*
AP Pelvis:
Demonstrated severe tricompartmental joint space narrowing of the left hip joint, subchondral sclerosis, extensive osteophyte formation along the femoral head-neck junction and acetabular rim, and subchondral cyst formation in both the femoral head and acetabulum. The femoral head was mildly flattened superiorly. There was evidence of mild acetabular retroversion indicated by a positive cross-over sign. The superolateral migration of the femoral head and acetabular wear contributed to an estimated 1.5 cm leg length discrepancy. Minimal heterotopic ossification was noted adjacent to the greater trochanter. The contralateral hip showed early degenerative changes but no significant narrowing. The Kellgren-Lawrence grade for the left hip was IV.
*
Frog-Lateral View:
Confirmed severe joint space narrowing and demonstrated loss of the anterior offset of the femoral head relative to the neck.
*
True Lateral View:
Provided additional detail on anterior osteophyte burden and the femoral head morphology.
CT/MRI Indications
No CT or MRI was deemed immediately necessary for primary total hip arthroplasty in this uncomplicated case of severe primary osteoarthritis.
*
CT Scan:
Would be indicated in cases of complex acetabular or femoral deformity, previous trauma, significant bone loss, tumor, or for detailed surgical planning for revision arthroplasty. It provides superior bony detail for identifying specific patterns of dysplasia (e.g., acetabular retroversion, femoral anteversion), bone defects, or for 3D templating of custom implants if required.
*
MRI Scan:
Would be considered if avascular necrosis (AVN) was suspected without clear radiographic changes, to rule out soft tissue pathology such as labral tears, bursitis, or occult fractures, or to assess for inflammatory arthropathy not evident on X-rays. In this patient, the classic radiographic findings of severe osteoarthritis made further advanced imaging less critical.
Templating
Digital templating was performed using specialized software (e.g., TraumaCad, OrthoView) based on the calibrated AP pelvis radiograph.
*
Calibration:
A known-size calibration ball (e.g., 25mm) was placed at the level of the greater trochanter for accurate magnification adjustment.
*
Acetabular Component:
Templates of various uncemented hemispheric cups were superimposed onto the acetabulum to determine optimal size, accounting for remaining host bone. Goals included maximizing coverage (80-90%), achieving appropriate inclination (40-45°) and anteversion (15-20°), and assessing for potential wall defects or reaming required. The superior-lateral acetabular rim was identified as the key landmark for cup placement.
*
Femoral Component:
Templates of uncemented, proximally coated femoral stems were used to assess appropriate size, fit, and fill in the femoral canal, aiming for metaphyseal fit. Medial and lateral cortical contact was evaluated. Femoral offset, leg length, and potential for restoration of femoral anteversion were assessed. The lesser trochanter was used as a key landmark for stem depth and leg length adjustments.
*
Leg Length and Offset:
Critical measurements included baseline leg length discrepancy (LLD) from the ischial tuberosity to the lesser trochanter, and femoral offset from the center of rotation to the mid-diaphyseal axis. Templating aimed to restore these parameters to approximate the contralateral hip or achieve functional balance, minimizing LLD and optimizing abductor mechanics.
*
Pre-operative planning:
This involved identifying potential challenges such as extensive osteophytes requiring removal, areas of bone sclerosis, or specific nerve at risk due to severe shortening (e.g., sciatic nerve).
Differential Diagnosis
| Feature | Severe Primary Osteoarthritis (OA) | Avascular Necrosis (AVN) of the Femoral Head | Rheumatoid Arthritis (RA) |
|---|---|---|---|
| Pathophysiology | Cartilage degeneration, subchondral bone remodeling, osteophyte formation. | Interruption of blood supply to femoral head, leading to osteonecrosis and collapse. | Chronic systemic inflammatory autoimmune disease affecting synovial joints. |
| Typical Onset | Insidious, progressive over years. | Often insidious, can be acute with collapse; faster progression than OA. | Insidious, symmetric polyarthritis; hip involvement later in disease. |
| Pain Characteristics | Mechanical pain, activity-related, groin/buttock, stiffness after rest. | Groin/buttock pain, initially intermittent, then constant; pain with weight-bearing. | Inflammatory pain, worse with rest/morning, relieved with activity; often multiple joints. |
| Risk Factors | Age, obesity, previous trauma/dysplasia, genetics. | Steroid use, alcohol abuse, trauma, sickle cell, SLE, Gaucher's disease. | Female sex, genetics (HLA-DR4), smoking. |
| Clinical Exam | Restricted, painful ROM (esp. IR, flexion); antalgic gait; positive Trendelenburg. | Restricted, painful ROM (esp. IR); antalgic gait; may have effusion. | Symmetric polyarthritis, warm/swollen joints, extra-articular manifestations (nodules, vasculitis). |
| X-ray Findings | Joint space narrowing (tricompartmental), osteophytes, subchondral sclerosis/cysts, subluxation. | Crescent sign (subchondral collapse), patchy sclerosis/lucency, flattening of femoral head. | Joint space narrowing (concentric), erosions, juxta-articular osteopenia, absence of osteophytes. |
| MRI Utility | Not typically needed for diagnosis; shows cartilage loss, effusions. | Diagnostic gold standard: Marrow edema, serpentine low signal line, T1/T2 signal changes. | Shows synovitis, erosions, bone marrow edema; aids in early diagnosis. |
| Lab Findings | Normal inflammatory markers (ESR, CRP). | Normal inflammatory markers. | Elevated ESR/CRP, positive Rheumatoid Factor (RF), anti-CCP antibodies. |
| Treatment Considerations | Conservative initially (PT, NSAIDs, injections); THA for advanced disease. | Core decompression in early stages; THA for advanced collapse. | Disease-modifying anti-rheumatic drugs (DMARDs), biologics; THA for severe joint destruction. |
Surgical Decision Making & Classification
Why Operative vs. Non-Operative
The decision to proceed with operative intervention (Total Hip Arthroplasty, THA) was made after a comprehensive discussion with the patient, adhering to established guidelines for severe, symptomatic osteoarthritis.
Indications for THA:
*
Failure of Non-Operative Management:
The patient had undergone an appropriate course of conservative treatments, including activity modification, NSAIDs, physical therapy, and a corticosteroid injection, all of which failed to provide sustained symptomatic relief.
*
Severe Pain:
Debilitating, chronic hip pain significantly impacting quality of life and sleep.
*
Functional Limitation:
Progressive restriction in activities of daily living, ambulation distance, and ability to participate in desired recreational activities.
*
Radiographic Evidence:
Advanced degenerative changes consistent with Kellgren-Lawrence Grade IV osteoarthritis.
*
Patient Desire:
Highly motivated patient with realistic expectations for surgical outcomes and commitment to rehabilitation.
*
Medical Fitness:
Thorough pre-operative medical evaluation confirmed the patient was medically optimized and a suitable candidate for elective surgery despite his comorbidities (controlled hypertension, hyperlipidemia, T2DM).
Contraindications (relative or absolute):
* Active deep infection in the hip or systemic sepsis.
* Uncontrolled medical comorbidities posing extreme anesthetic or surgical risk.
* Neuropathic joint (Charcot arthropathy) with progressive bone destruction.
* Severe muscle weakness or paralysis rendering joint replacement ineffective.
* Skeletally immature patient (not applicable here).
* Non-ambulatory status with no realistic potential for ambulation improvement (not applicable here).
* Rapidly progressive neurological disease.
In this case, the patient met all the primary indications for THA, and no absolute contraindications were identified.
Specific Classifications
- Kellgren-Lawrence Classification for Osteoarthritis: The patient's hip was classified as Grade IV , indicating severe osteoarthritis with large osteophytes, marked joint space narrowing, severe sclerosis, and definite deformity of bone ends. This classification is primarily radiographic and helps in categorizing the severity of degenerative changes.
- Paprosky Classification for Femoral Bone Loss: While more commonly used in revision arthroplasty, it can be conceptually considered in primary cases with significant metaphyseal or diaphyseal bone defects or deformities. In this primary case, significant femoral bone loss was not present, hence it was not formally applied, suggesting a Type I or Type IIA femur, amenable to standard uncemented stem fixation.
- Acetabular Bone Defect Classifications (e.g., Paprosky, AAOS): Similarly, in this primary case, while there was some osteophyte formation and superior migration, there was no severe acetabular bone loss or discontinuity that would warrant complex reconstruction. The acetabulum was considered a Type I or IIA, requiring standard reaming and hemispheric cup implantation.
-
DORR Classification for Femoral Canal Morphology:
This classification assesses the proximal femoral canal morphology based on the cortical index and presence of a "champagne flute" vs. "stovepipe" appearance.
- Type A: Champagne flute, thick cortex, narrow canal (risk of fracture with uncemented stems).
- Type B: Intermediate, good metaphyseal-diaphyseal flare (ideal for uncemented stems).
-
Type C:
Stovepipe, thin cortex, wide canal (often better for cemented stems or specific uncemented designs).
Our patient's radiographs suggested a Dorr Type B femur, which is generally favorable for cementless stem implantation due to good metaphyseal bone stock for primary press-fit stability.
Surgical Technique / Intervention
The planned procedure was a left uncemented Total Hip Arthroplasty (THA) via a posterior approach.
Patient Positioning
The patient was positioned in the right lateral decubitus position on a standard operating table, with the torso secured by an anterior chest roll and posterior sacral support. The lower extremities were padded appropriately, and the contralateral leg was flexed and supported on a pillow. The operative leg was draped free to allow for full range of motion intraoperatively for stability assessment. The entire left lower extremity was prepped and draped in a sterile fashion from the costal margin to the toes. An anterior bump was placed at the level of the anterior superior iliac spine (ASIS) to stabilize the pelvis and prevent internal rotation, ensuring proper acetabular component orientation.
Approach
A standard posterior (Kocher-Langenbeck) approach was utilized.
1.
Incision:
A curvilinear skin incision of approximately 15 cm was made centered over the greater trochanter, extending proximally towards the posterior superior iliac spine (PSIS) and distally along the femoral shaft.
2.
Fascia and Muscles:
The incision was carried through the skin and subcutaneous tissues. The fascia lata was incised in line with the skin incision. The gluteus maximus muscle fibers were split bluntly.
3.
Short External Rotators and Capsule:
The short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) were identified. The piriformis tendon, which inserts on the greater trochanter, was identified as the most superior structure and tagged with a non-absorbable suture for later repair. The tendons of the gemelli and obturator internus were then tenotomized close to their femoral insertion and tagged. The quadratus femoris was optionally incised or retracted, depending on exposure needs. This exposure revealed the posterior hip capsule.
4.
Capsulotomy:
A T-shaped or H-shaped capsulotomy was performed. The capsule was incised longitudinally and then transversely near its acetabular attachment. Capsular tissue was also tagged for repair.
5.
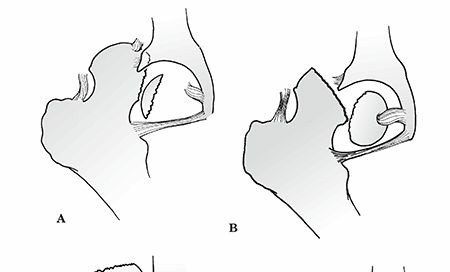
Dislocation:
The hip was dislocated posteriorly by internally rotating, adducting, and flexing the hip. This typically reveals the arthritic femoral head and acetabulum.
Acetabular Preparation
- Osteophyte Removal: Extensive acetabular osteophytes, particularly along the inferior and posterior rim, were meticulously removed using an osteotome and rongeur to define the true acetabular rim and facilitate component placement.
- Femoral Head Resection: The femoral head was resected using an oscillating saw, typically at the level of the femoral neck, preserving as much femoral neck as possible, usually at one finger-breadth above the lesser trochanter. The resected head was measured for pre-operative templating accuracy.
- Acetabular Reaming: Progressive reaming of the acetabulum commenced with a reamer size typically 2-4 mm smaller than the templated cup size. Reaming proceeded systematically from the periphery to the medial wall, ensuring a hemispheric shape and removal of all cartilage and sclerotic bone until bleeding cancellous bone was exposed. The goal was to achieve a robust peripheral press-fit and a stable interface. Care was taken to avoid over-reaming medially or perforating the medial wall. The acetabular fossa was preserved minimally.
- Acetabular Component Implantation: The final reamer size (equal to the templated cup size) was used. An uncemented hemispheric cup with a porous coating (e.g., plasma spray titanium with hydroxyapatite) was impacted into the prepared acetabulum, aiming for 40-45° inclination and 15-20° anteversion. The pelvic anterior bump and leg position facilitated accurate orientation. Multiple peripheral screws were inserted for additional rotational stability and fixation, ensuring no screw impingement or neurovascular risk.
- Liner Insertion: A polyethylene liner (conventional or cross-linked, depending on patient age and activity level) was inserted into the acetabular shell. The chosen liner was a 36mm cross-linked polyethylene liner to optimize range of motion and reduce wear while maintaining stability.
Femoral Preparation
- Femoral Canal Preparation: The femoral canal was prepared using progressive broaches, starting with a small size and gradually increasing until a stable metaphyseal press-fit was achieved. The broach size was determined by pre-operative templating and intraoperative feel. The broaching process sculpted the femoral metaphysis and proximal diaphysis to match the implant geometry, ensuring appropriate anteversion.
- Trial Reduction: A trial femoral head and neck component of the appropriate offset and length (based on templating and intraoperative assessment of leg length) were assembled with the trial stem.
-
Reduction and Stability Assessment:
The hip was reduced, and comprehensive stability testing was performed through a full range of motion.
- Flexion: The hip was flexed to 90 degrees, and the resistance to internal rotation was assessed.
- Extension: The hip was extended, and the resistance to external rotation and adduction was assessed.
- Adduction/Internal Rotation (Posterior dislocation test): With the hip in flexion, adduction, and internal rotation, the hip stability was assessed. No impingement or undue laxity should be present.
- Leg Length Assessment: The leg length was assessed clinically by comparing the level of the medial malleoli or by using a caliper to measure from the ASIS to the medial malleolus, confirming restoration to the contralateral side or the planned adjustment.
-
Offset Restoration:
Femoral and global offset were evaluated to ensure appropriate abductor tension.
Adjustments to neck length (e.g., +0, +5, +10mm) or head diameter/offset were made until optimal stability, leg length, and offset were achieved.
- Final Stem Implantation: The trial components were removed. The definitive uncemented femoral stem, made of titanium alloy with a porous coating, was then impacted into the prepared femoral canal, ensuring it matched the final broach size and position.
- Final Femoral Head and Liner Placement: The chosen femoral head (e.g., CoCr or ceramic) was then securely impacted onto the Morse taper of the femoral stem. A ceramic 36mm femoral head was chosen for its low wear properties. The chosen polyethylene liner was locked into the acetabular shell.
- Final Reduction: The hip was reduced for the final time.
- Final Stability Check: A final check of stability, leg length, and range of motion was performed.
Closure
- Capsular and Rotator Repair: The short external rotators (piriformis, gemelli, obturator internus) were repaired back to their original insertions or the posterior capsule using non-absorbable sutures. The posterior capsule was meticulously repaired to enhance stability and reduce the risk of posterior dislocation.
- Fascia and Subcutaneous Tissue: The fascia lata was closed. Subcutaneous tissues were closed in layers.
- Skin Closure: The skin was closed with staples or absorbable sutures. A sterile dressing was applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative (Day 0-3)
- Pain Management: Multimodal analgesia (NSAIDs, acetaminophen, opioids as needed, regional blocks where appropriate) to minimize pain and facilitate early mobilization.
- Prophylaxis: Deep vein thrombosis (DVT) prophylaxis initiated (e.g., LMWH or oral anticoagulants) for 4-6 weeks, alongside mechanical compression devices.
- Weight-Bearing: Immediate weight-bearing as tolerated (WBAT) with an assistive device (walker or crutches) for uncemented components. Patients are instructed to limit flexion to 90 degrees, avoid adduction past midline, and avoid internal rotation past neutral (posterior approach precautions).
- Mobilization: Physical therapy initiated on post-operative day 0 or 1, focusing on bed mobility, transfers, gait training, and gentle hip ROM exercises within precautions.
- Wound Care: Daily wound inspection, dressing changes as needed. Staples typically removed at 10-14 days.
Early Rehabilitation (Weeks 1-6)
-
Physical Therapy:
Continued outpatient or home-based physical therapy.
- Goals: Restore full weight-bearing, progress off assistive devices, improve hip strength (especially abductors), maintain ROM within precautions, and improve gait mechanics.
- Exercises: Isometric gluteal sets, quadriceps sets, ankle pumps, hip abduction/adduction in supine, heel slides, controlled hip flexion, progressive gait training.
- Precautions: Strict adherence to hip precautions (no hip flexion beyond 90°, no adduction past midline, no internal rotation past neutral) for 6-12 weeks, depending on surgeon preference and patient compliance.
- Activity: Avoid high-impact activities, prolonged standing/walking initially. Gradual return to light activities of daily living.
Intermediate Rehabilitation (Weeks 7-12)
-
Physical Therapy:
Continued progression of strength and conditioning.
- Goals: Wean off all assistive devices, normalize gait, improve balance, regain functional strength for daily activities.
- Exercises: Closed-chain exercises, light resistance training (bands, light weights), stationary cycling, swimming, proprioceptive exercises.
- Precautions: Gradual easing of hip precautions may be considered based on soft tissue healing, patient compliance, and surgical findings (e.g., secure capsular repair).
- Activity: Introduction of low-impact recreational activities, if appropriate.
Advanced Rehabilitation (Months 3-6+)
- Physical Therapy: Focus on return to higher-level activities and sport-specific training if desired and approved.
- Goals: Full functional recovery, return to previous activities (excluding high-impact), maintenance of strength and flexibility.
- Exercises: Continued progressive strengthening, cardiovascular conditioning, dynamic balance training.
- Long-Term: Patients are encouraged to maintain a regular exercise program to preserve strength and mobility. Avoid high-impact sports (running, jumping) and heavy lifting indefinitely to maximize implant longevity. Regular follow-up with the surgeon (e.g., at 1 year, then every 3-5 years) with radiographs to monitor implant stability and detect any signs of loosening or wear.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
-
Pre-Operative Planning is Paramount:
- Templating: Crucial for accurate prediction of component sizes, leg length, and offset. Always use calibrated radiographs. Consider both AP and lateral views.
- Deformity Analysis: Identify pre-existing deformities (e.g., acetabular retroversion, femoral anteversion/retroversion, severe osteophytes, proximal femoral bone loss) to anticipate surgical challenges and adjust technique.
- Patient Optimization: Rigorous medical optimization of comorbidities (diabetes, anemia, cardiac risk) significantly reduces perioperative complications.
-
Surgical Approach Selection:
- Each approach (posterior, anterior, anterolateral, direct lateral) has distinct advantages and disadvantages regarding dislocation risk, muscle damage, recovery profile, and learning curve. Choose an approach that you are proficient with and that best suits the patient's anatomy and specific pathology.
- The posterior approach offers excellent exposure of both acetabulum and femur, with reproducible results when short external rotators and capsule are meticulously repaired.
-
Achieving Biomechanical Restoration:
- Leg Length Equality: A primary goal. Use consistent intraoperative landmarks (e.g., ischial tuberosity to lesser trochanter, pin in ASIS/greater trochanter) to measure and restore leg length. Discrepancies >1 cm can be problematic.
- Femoral Offset: Restoration is critical for optimal abductor tension and gait mechanics. Loss of offset leads to Trendelenburg gait and increased abductor fatigue.
- Center of Rotation: Medialization of the femoral head's center of rotation reduces joint reactive forces and improves hip mechanics.
-
Acetabular Component Placement:
- Inclination (40-45°) and Anteversion (15-20°): The "safe zone" for minimizing dislocation risk and maximizing liner wear. Use patient positioning (pelvic obliquity), anatomical landmarks (anterior pelvic plane, transverse acetabular ligament), and intraoperative navigators/robotics if available.
- Reaming: Ream to bleeding bone, avoid over-reaming medially. Ensure circumferential bone contact for press-fit stability.
-
Femoral Component Selection and Placement:
- Stem Type (Cemented vs. Uncemented): Uncemented stems require good bone stock (Dorr B/C femur) and rely on press-fit for primary stability and bone ingrowth for secondary stability. Cemented stems are preferred in osteoporotic bone (Dorr A femur) or specific revision scenarios.
- Anteversion: Ensure appropriate femoral anteversion (typically 10-20°) to prevent impingement and dislocation, especially in conjunction with acetabular anteversion. Use the lesser trochanter or epicondylar axis as a reference.
- Broaching: "Whisper to a woman, yell at a broach." Ensure firm impaction to achieve a stable fit without fracturing the femur.
-
Soft Tissue Tension and Stability:
- Trial Reduction: Perform meticulous trial reductions to assess stability through a full range of motion. Check for impingement, subluxation, and dislocation.
- Capsular/Rotator Repair: Meticulous repair of the posterior capsule and short external rotators (if using posterior approach) significantly enhances stability and reduces posterior dislocation rates.
Pitfalls
- Wrong Leg/Wrong Side Surgery: A cardinal sin. Strict adherence to universal protocol, "time-out," and double-checking of patient identification, surgical site, and implant orders.
-
Neurovascular Injury:
- Sciatic Nerve: Most common nerve injury, especially with leg lengthening or posterior approach. Avoid excessive traction or prolonged hyperextension/external rotation. Protect with retractors.
- Femoral Nerve: Risk with anterior approaches or aggressive medial retraction.
- Obturator Nerve: Risk during aggressive acetabular reaming or screw placement medially.
- Vascular Injury: External iliac vessels at risk during medial acetabular reaming/screw placement. Femoral artery/vein at risk during anterior approaches.
-
Intraoperative Fracture:
- Femoral Fracture: During broaching or stem impaction, especially in Dorr A femurs, osteoporotic bone, or with forceful impaction. Prepare for cerclage wiring or revision to a different stem design.
- Acetabular Fracture: During reaming (medial wall perforation) or cup impaction (rim fracture). Managed with screws, revision to a larger cup, or bone graft.
-
Malposition of Components:
- Acetabular Malposition: Excessive inclination (too vertical) increases dislocation risk and wear. Excessive anteversion/retroversion increases impingement and dislocation risk.
- Femoral Malposition: Incorrect femoral anteversion can lead to impingement and dislocation.
- Consequences include recurrent dislocation, impingement, accelerated wear, and chronic pain.
- Leg Length Discrepancy: Over-lengthening can cause sciatic nerve neuropraxia, back pain, and gait disturbance. Under-lengthening can cause instability, Trendelenburg gait, and continued functional limitations. Meticulous templating and intraoperative checks are crucial.
- Inadequate Soft Tissue Tension: Leads to instability and dislocation. Ensure proper component sizing and restoration of offset and leg length to achieve adequate abductor tension.
- Infection: Despite prophylactic antibiotics, periprosthetic joint infection (PJI) remains a devastating complication. Strict aseptic technique, laminar flow, reduced OR traffic, and minimizing surgical time are critical.
- Dislocation: The most common early mechanical complication. Factors include patient non-compliance with precautions, component malposition, inadequate soft tissue tension, and implant design. Posterior approach has a slightly higher risk of posterior dislocation if capsule/rotators are not repaired.
- Heterotopic Ossification (HO): Formation of new bone in soft tissues around the hip. Risk factors include male sex, hypertrophic OA, previous HO. Prophylaxis with NSAIDs (e.g., indomethacin) or low-dose radiation post-op may be considered in high-risk patients.
You Might Also Like