Analyzing a Hybrid Primary Hip Arthroplasty Patient Case

Key Takeaway
Learn more about Analyzing a Hybrid Primary Hip Arthroplasty Patient Case and how to manage it. A case title hybrid primary hip arthroplasty combines both cemented and uncemented prosthetic components. For this 76-year-old female with bilateral hip osteoarthritis, it involved a press-fit uncemented acetabular component and a cemented femoral stem (Exeter). This method was chosen to optimize bone fit for the patient's bone quality and minimize the risk of periprosthetic fractures.
Patient Presentation & History
A 78-year-old male presented to the emergency department following a mechanical fall at home. He reported immediate, severe left hip pain and an inability to bear weight. The patient was ambulating independently prior to the fall, with a full activities of daily living (ADL) capacity and no significant gait aids. He lives alone in a single-story residence.
His medical history is notable for:
* Hypertension, well-controlled on a single anti-hypertensive agent.
* Hyperlipidemia, managed with statin therapy.
* Mild osteoarthritis of the contralateral knee, managed conservatively.
* No history of previous hip pathology, inflammatory arthropathy, or significant systemic comorbidities.
* Current medications: Amlodipine 5mg OD, Atorvastatin 20mg OD.
* No known allergies.
* Social history: Non-smoker, occasional alcohol use. Mentally astute and fully oriented.
The mechanism of injury involved tripping over a rug and falling directly onto his left hip. There was no preceding prodromal pain or weakness. Review of systems was otherwise unremarkable, with no signs of systemic illness or prodromal symptoms suggesting a pathological fracture or transient ischemic attack as a precipitating factor for the fall.
Clinical Examination
Upon initial assessment, the patient was alert, oriented, and in significant pain.
*
Inspection:
The left lower extremity was noted to be shortened by approximately 2 cm, with obvious external rotation of the entire limb, consistent with a displaced femoral neck fracture. There was no obvious ecchymosis or open wound.
*
Palpation:
Diffuse tenderness was elicited over the left greater trochanter and groin. Axial loading of the femur and gentle internal/external rotation maneuvers of the hip were excruciatingly painful.
*
Range of Motion:
Grossly restricted and painful range of motion in all planes, with particular resistance to internal rotation and abduction. Attempts at passive motion were met with guarding and severe pain.
*
Neurological Assessment:
* Motor: Unable to voluntarily move the left hip due to pain. Distal motor function (knee extension, ankle dorsiflexion, plantarflexion, great toe extension) intact (5/5).
* Sensory: Light touch and pinprick sensation intact in the L2-S1 dermatomes.
* Reflexes: Patellar and Achilles reflexes symmetrically 2+ bilaterally.
*
Vascular Assessment:
* Peripheral pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were present and strong, bilaterally symmetric.
* Capillary refill time was less than 2 seconds in all toes.
* No signs of acute limb ischemia.
*
Systemic Examination:
Cardiopulmonary examination revealed regular heart sounds without murmurs, and clear lung fields. Abdominal examination was benign.
Imaging & Diagnostics
Initial Radiographs
Antero-posterior (AP) and lateral radiographs of the pelvis and left hip were obtained immediately.
*
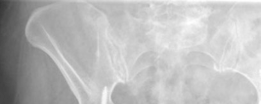
AP Pelvis and Left Hip:
These views clearly demonstrated a displaced left femoral neck fracture. The fracture line was intracapsular. The femoral head was superiorly and posteriorly displaced relative to the femoral neck. There was evidence of approximately 1.5 cm of shortening. The bone quality appeared reasonable for the patient's age. No signs of pre-existing significant hip osteoarthritis in the ipsilateral joint were noted. The contralateral hip appeared unremarkable.
``
*Figure 1: Initial AP pelvis radiograph demonstrating a displaced left femoral neck fracture.*
The fracture was classified as a **Garden Type IV** (complete displacement, with loss of trabecular alignment between the femoral head and acetabulum, and the head rotated independently of the neck), and a **Pauwels Type III** (fracture line angle > 70 degrees from the horizontal, indicating high shear forces and poor prognosis for union with internal fixation).
Advanced Imaging
- Computed Tomography (CT) Scan: Not routinely indicated for isolated displaced femoral neck fractures in the elderly, where surgical management is usually clear based on plain radiographs. However, in cases of suspected comminution, impaction, or preoperative planning for complex acetabular reconstruction (not applicable here), a CT scan may be beneficial. It was not performed in this case.
- Magnetic Resonance Imaging (MRI): Not indicated acutely. Primarily used to diagnose occult fractures or avascular necrosis (AVN) in cases of persistent pain with normal radiographs, or to assess soft tissue pathology.
Pre-operative Templating
Pre-operative templating is a critical step for primary hip arthroplasty to ensure accurate component sizing, restoration of leg length, and appropriate offset.
*
Templating Procedure:
* Standardized AP pelvis and lateral hip radiographs were obtained with a known magnification marker (e.g., 25mm ball bearing).
* Acetabular templating involved overlaying templates of various cup sizes to determine the optimal diameter and position for maximum coverage and stability, aiming for 45 degrees of abduction and 20 degrees of anteversion.
* Femoral templating involved overlaying stem templates to determine appropriate stem size, canal fill, and restoration of femoral offset and leg length. Given the plan for a cemented stem, templating focused on achieving adequate cement mantle thickness.
* The goal was to restore the center of rotation, leg length, and femoral offset to match the contralateral side as closely as possible, minimizing the risk of impingement and dislocation while optimizing abductor muscle tension.
* For this patient, templating suggested a 54mm uncemented acetabular cup and a size 12 cemented femoral stem.
Differential Diagnosis
The acute presentation of a fall with severe hip pain and deformity in an elderly patient necessitates consideration of several diagnoses.
| Diagnosis | Clinical Features | Radiographic Features | Management Strategy |
|---|---|---|---|
| Displaced Femoral Neck Fracture | Shortened, externally rotated limb; severe groin/hip pain; inability to bear weight. | Intracapsular fracture line; Garden Type III/IV displacement; Pauwels Type II/III. | Arthroplasty (Hemiarthroplasty vs. THA) for elderly, active patients; ORIF for younger patients. |
| Intertrochanteric Fracture | Similar deformity (shortening, external rotation); often more ecchymosis; pain localized to greater trochanter/lateral hip. | Extracapsular fracture line between greater and lesser trochanters; often comminuted. | Internal fixation with cephalomedullary nail or dynamic hip screw. |
| Acetabular Fracture | Depending on fracture pattern; severe hip pain; often associated with high-energy trauma (though possible with falls in osteoporotic patients); deformity less consistent than femoral fractures. | Fracture lines involving the acetabulum (columns, walls, transverse, T-type); assessed by Judet views and CT. | Non-operative vs. ORIF, depending on stability, displacement, joint congruence. |
| Posterior Hip Dislocation | Shortened, internally rotated, adducted limb; severe pain; history of high-energy trauma often (but can be low energy with prosthetic hip). | Femoral head out of acetabulum, typically posterior-superior. | Urgent closed reduction; if irreducible or associated with fracture, open reduction. |
| Pathological Fracture | History of cancer or systemic disease; insidious onset of pain preceding fall; constitutional symptoms. | Lytic or blastic lesions on X-ray; often with cortical destruction. | Depends on primary etiology; fixation, sometimes with cement augmentation or arthroplasty. |
In this patient, the classic clinical signs and clear radiographic findings of a Garden Type IV, Pauwels Type III displaced femoral neck fracture made the diagnosis unequivocal, guiding the subsequent surgical decision-making.
Surgical Decision Making & Classification
Rationale for Operative Management
Given the patient's age (78 years), his pre-injury activity level (independent ambulator), and the nature of the fracture (Garden Type IV, Pauwels Type III displaced femoral neck fracture), operative intervention was the only viable option. Non-operative management would result in prolonged bed rest, high risk of non-union, avascular necrosis (AVN) of the femoral head, severe pain, and significant morbidity (e.g., DVT, pulmonary embolism, pneumonia, pressure ulcers).
Choice of Arthroplasty
For displaced femoral neck fractures in the elderly, the primary options are:
1.
Open Reduction and Internal Fixation (ORIF):
Primarily for younger patients (< 60-65 years) or very frail, non-ambulatory elderly where the risks of arthroplasty outweigh potential benefits. High rates of AVN and non-union in displaced fractures in the elderly make it less favorable.
2.
Hemiarthroplasty (HA):
Replacement of the femoral head and neck only, articulating with native acetabular cartilage. Suitable for older, less active patients, or those with significant medical comorbidities where a shorter surgical time and less blood loss are paramount. Unipolar or bipolar designs.
3.
Total Hip Arthroplasty (THA):
Replacement of both the femoral head and neck, and the acetabulum. Offers superior functional outcomes and lower revision rates compared to HA in active, physiologically younger elderly patients, by addressing potential acetabular cartilage erosion and reducing acetabular wear.
Considering the patient's relative physiological youth (78 years, active, independent, minimal comorbidities), his pre-injury functional status, and the absence of pre-existing significant ipsilateral hip arthritis, a Total Hip Arthroplasty (THA) was chosen over hemiarthroplasty. THA provides a more durable solution with better long-term functional results and lower rates of acetabular erosion and groin pain compared to HA.
Rationale for Hybrid Fixation
The decision for a
hybrid THA
(uncemented acetabular component and cemented femoral component) was based on several factors:
*
Acetabular Component (Uncemented):
In an active 78-year-old with reasonable bone quality, the potential for biological ingrowth of an uncemented acetabular component offers excellent long-term fixation and durability. It avoids the challenges and potential long-term issues associated with cemented acetabular components (e.g., aseptic loosening rates).
*
Femoral Component (Cemented):
While uncemented femoral stems are common, a cemented femoral stem was preferred in this scenario for several reasons:
*
Immediate Stability:
Provides immediate, secure fixation, which is particularly advantageous in osteopenic bone, common in this age group, ensuring early weight-bearing and rehabilitation.
*
Predictable Fixation:
Cement fills irregularities in the femoral canal, optimizing load transfer and reducing the risk of subsidence or periprosthetic fracture that can sometimes be associated with uncemented stems in less robust bone.
*
Reduced Risk of Intraoperative Fracture:
Cemented stems can be less prone to intraoperative femoral fracture during insertion compared to press-fit uncemented stems in dense or osteoporotic bone.
*
Surgeon Preference/Experience:
The operating surgeon's extensive experience with cemented stems and their reliable long-term outcomes in this demographic also factored into the decision.
Therefore, the surgical plan involved a primary hybrid THA utilizing a modern highly cross-linked polyethylene liner, a ceramic femoral head, an uncemented acetabular shell, and a polished, tapered cemented femoral stem.
Surgical Technique / Intervention
Pre-operative Preparation
- Pre-operative antibiotics (cefazolin) administered within 60 minutes of incision.
- Regional anesthesia (spinal/epidural) combined with general anesthesia for optimal pain control and muscle relaxation.
- The patient was positioned in the lateral decubitus position on a fracture table, allowing for controlled limb manipulation and optimal exposure via a posterior approach. The operative limb was draped free.
Surgical Approach
A standard
posterior (Kocher-Langenbeck) approach
was utilized.
1.
Incision:
A curvilinear incision centered over the greater trochanter, extending proximally towards the posterior superior iliac spine and distally along the line of the femoral shaft.
2.
Dissection:
* The gluteus maximus fibers were split bluntly.
* The short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) and their neurovascular bundle were identified and typically tagged and released from their femoral insertion to expose the posterior capsule. The sciatic nerve was identified and protected.
* The hip joint capsule was incised (capsulotomy) to expose the dislocated femoral head and the fracture site. The femoral head was completely dislocated from the acetabulum.
``
*Figure 2: Intraoperative view following exposure and capsulotomy, demonstrating the displaced femoral head fracture.*
Acetabular Preparation
- Femoral Head Excision: The fractured femoral head was carefully excised using a reciprocating saw, ensuring the remaining femoral neck cut was at the templated level.
- Acetabular Exposure: The acetabulum was cleared of any remaining ligamentum teres, labral remnants, and osteophytes.
-
Reaming: Progressive reaming of the acetabulum was performed using hemispherical reamers, starting from a smaller size and incrementally increasing until host bone was exposed circumferentially in the periphery and bleeding bone was evident throughout the dome, indicating viable cancellous bone for ingrowth. Care was taken to avoid over-reaming or eccentric reaming.

Figure 3: Acetabular reaming in progress, preparing the host bone for uncemented cup insertion.
Figure 4: A clear view of the reamed acetabulum, demonstrating optimal host bone exposure.
4. Trial Reduction (Acetabular): A trial acetabular component was inserted to confirm appropriate size and position, aiming for 40-45 degrees of abduction and 15-20 degrees of anteversion.
5. Definitive Acetabular Component Insertion: A 54mm porous-coated, uncemented acetabular shell was impacted into the prepared acetabulum, ensuring a tight press-fit. Multiple locking screws were placed strategically for enhanced primary stability, particularly in the superior and posterior quadrants.
Figure 5: Impaction of the definitive uncemented acetabular cup.
Figure 6: Placement of locking screws to augment the primary stability of the acetabular component.
6. Polyethylene Liner Insertion: A highly cross-linked polyethylene liner (e.g., 32mm inner diameter) was then securely locked into the acetabular shell.
Femoral Preparation and Cemented Stem Insertion
-
Femoral Canal Preparation: The femoral canal was prepared sequentially using reamers and rasps, starting from the piriformis fossa, progressing distally until cortical contact was achieved circumferentially. The goal was to achieve optimal canal fill and shape for the chosen cemented stem.

Figure 7: Femoral canal preparation with a rasp, shaping the metaphysis and diaphysis for stem insertion.
2. Trial Stem Insertion: A trial femoral stem (size 12) was inserted, and a trial ceramic head was attached.
3. Trial Reduction and Stability Assessment: The hip was reduced, and meticulous assessment of leg length, offset, and stability was performed through a full range of motion. Any impingement or excessive laxity indicated a need for adjustment (e.g., different neck length, head size, or component position).
4. Cementing Technique:
* The femoral canal was thoroughly lavaged and dried. A cement restrictor was placed at the appropriate depth (typically 2 cm distal to the stem tip).
* Bone cement (PMMA) was mixed under vacuum to optimize its mechanical properties and reduce porosity.
* The cement was introduced retrograde into the femoral canal using a cement gun, starting distally and filling proximally, ensuring complete canal filling and pressurization.
* The definitive polished, tapered cemented femoral stem (size 12) was then carefully inserted, ensuring correct alignment and rotation. Excess cement was removed from around the stem and the calcar region.
Figure 8: Insertion of the definitive cemented femoral stem into the prepared canal, with cement pressurization.
5. Definitive Head Placement: Once the cement had fully polymerized, the ceramic femoral head (32mm diameter, +0mm neck length) was impacted onto the femoral trunion.
6. Final Reduction: The definitive prosthesis was reduced.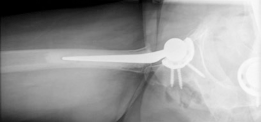
Figure 9: Final reduction of the hip prosthesis after component placement.
Wound Closure
- The short external rotators were repaired to the posterior aspect of the greater trochanter through drill holes, if viable, to enhance posterior stability and restore function.
- The capsule was repaired or imbricated.
- The fascia, subcutaneous tissue, and skin were closed in layers. A surgical drain was typically not used unless significant bleeding was encountered.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Care (Day 0-2)
- Pain Management: Multimodal analgesia including regional blocks, oral opioids, NSAIDs (if not contraindicated), and acetaminophen.
- DVT Prophylaxis: Low molecular weight heparin (LMWH) initiated post-operatively, continued for 4-6 weeks, combined with mechanical prophylaxis (foot pumps, compression stockings).
- Antibiotics: Post-operative antibiotic doses typically for 24 hours.
- Mobility: Early mobilization is crucial. The patient was encouraged to sit out of bed and begin transfers with physical therapy guidance on Post-operative Day 1.
- Weight-Bearing: Immediate full weight-bearing as tolerated was permitted due to the secure fixation of both cemented and uncemented components.
-
Hip Precautions:
Due to the posterior approach, hip precautions were initiated to prevent dislocation:
- Avoid hip flexion > 90 degrees.
- Avoid hip adduction past midline.
- Avoid hip internal rotation.
- These precautions are typically maintained for 6-12 weeks, depending on surgeon preference and patient compliance.
In-Hospital Rehabilitation (Day 2-5)
-
Physical Therapy:
Daily sessions focusing on:
- Bed mobility, transfers (bed to chair, chair to commode).
- Gait training with appropriate assistive devices (walker initially, progressing to crutches/cane).
- Strengthening exercises for quadriceps, hamstrings, and gluteal muscles (within precautions).
- Range of motion exercises (within precautions).
- Occupational Therapy: Assessment of home environment and ADL retraining.
- Discharge Planning: Aim for discharge to home with outpatient physical therapy, or to a skilled nursing facility if further intensive rehabilitation is required. This patient was discharged home with home health physical therapy.
Outpatient Rehabilitation (Weeks 1-12)
-
Weeks 1-6:
- Focus on gradual increase in strength, endurance, and range of motion.
- Weaning off assistive devices.
- Reinforcement of hip precautions.
- Progressive strengthening exercises.
-
Weeks 6-12:
- Discontinuation of hip precautions (surgeon dependent).
- Advanced strengthening, balance, and proprioception exercises.
- Return to light activities.
- Return to driving typically around 6 weeks if ambulating safely and pain is controlled.
Long-term Follow-up
- Clinical and Radiographic Assessment: Regular follow-up appointments at 6 weeks, 3 months, 6 months, 1 year, and annually thereafter. Radiographs at these intervals to assess component stability, signs of loosening, wear, or osteolysis.
- Patient Education: Emphasis on avoiding high-impact activities, recognizing signs of infection or dislocation, and maintaining a healthy weight.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Patient Selection is Paramount: For femoral neck fractures in active, physiologically young elderly patients, THA offers superior long-term outcomes to hemiarthroplasty. Consider patient age, functional demands, and presence of pre-existing arthritis.
- Templating is Non-Negotiable: Meticulous pre-operative templating on calibrated radiographs is essential for accurate leg length, offset restoration, and component sizing, minimizing intraoperative surprises and optimizing outcomes.
- Hybrid Fixation Rationale: A hybrid THA, particularly an uncemented acetabulum with a cemented femoral stem, combines the benefits of biological ingrowth for long-term acetabular fixation with the immediate and reliable stability of a cemented stem in potentially osteopenic femurs. This strategy can be particularly advantageous in trauma cases where immediate weight-bearing is desired.
- Posterior Approach Advantages: Offers excellent exposure of both the acetabulum and femur, allowing for efficient component preparation and insertion. The ability to repair the short external rotators and posterior capsule helps restore stability.
- Cementing Technique: Ensure proper canal preparation (reaming, lavage, drying), appropriate cement restrictor placement, retrograde cement delivery, and pressurization for a durable cement mantle. Use of vacuum-mixed cement improves mechanical properties.
- Soft Tissue Balancing: Restoration of soft tissue tension, achieved by correct leg length and offset, is crucial for stability and minimizing dislocation risk.
- Early Mobilization: Aggressive but safe rehabilitation, including immediate full weight-bearing, is key to minimizing complications (DVT, deconditioning) and optimizing functional recovery.
- Prophylaxis: Scrupulous attention to infection and DVT prophylaxis significantly impacts outcomes.
Pitfalls
- Underestimation of Physiological Age: Basing surgical choice solely on chronological age can lead to suboptimal outcomes. A frail 65-year-old may be better served by a hemiarthroplasty than an active 80-year-old.
- Inadequate Pre-operative Planning: Skipping or rushing templating can lead to leg length discrepancies, malpositioning, or use of incorrect component sizes, increasing complication rates.
- Poor Cementing Technique: Inadequate canal preparation, insufficient pressurization, or premature stem insertion can lead to a poor cement mantle, increasing the risk of early aseptic loosening.
- Sciatic Nerve Injury: A risk with the posterior approach, especially with excessive retraction or during reattachment of short external rotators. Careful identification and protection are mandatory.
- Dislocation: The most common early complication, particularly with the posterior approach if hip precautions are not strictly adhered to or if soft tissue repair is inadequate. Incorrect component positioning (excessive anteversion/retroversion, malabduction) is a major contributor.
- Leg Length Discrepancy: A common cause of patient dissatisfaction. Careful templating, intraoperative measurement (e.g., using a ruler from the medial epicondyle to the tip of the greater trochanter, or pelvic landmarks), and trial reductions are essential.
- Periprosthetic Fracture: Can occur intraoperatively (during reaming or stem insertion) or post-operatively (trauma or stress shielding). Risk factors include osteoporotic bone and undersized uncemented stems.
- Infection: A devastating complication. Strict adherence to aseptic technique, appropriate antibiotic prophylaxis, and meticulous wound care are critical.
- Avascular Necrosis (AVN) of the Greater Trochanter: Can occur if the blood supply to the greater trochanter is compromised during the approach, especially with excessive stripping.
- Ignoring Native Acetabular Pathology: In cases of pre-existing significant acetabular arthritis, a hemiarthroplasty may lead to accelerated erosion and early revision. This reinforces the decision for THA in appropriate patients.
Clinical & Radiographic Imaging

