Posterolateral Ankle Approach: Surgical Technique for Posterior Malleolar Fractures & Anatomy
Key Takeaway
The posterolateral ankle approach is a surgical corridor for posterior malleolar fractures, offering direct visualization for anatomical reduction and restoring syndesmotic stability. It requires careful navigation, protecting the FHL muscle/tendon, sural nerve, and posterior tibial neurovascular bundle. Understanding key osseous and ligamentous structures is paramount for effective outcomes.
Introduction & Epidemiology
The posterolateral approach to the ankle joint represents a highly effective surgical corridor for addressing a spectrum of pathologies affecting the posterior aspect of the distal tibia and ankle. While historically less frequently utilized than medial or lateral approaches, its utility, particularly in the management of posterior malleolar fractures, has garnered increasing recognition in contemporary orthopedic trauma surgery. This approach offers direct visualization and anatomical reduction capabilities, which are paramount for restoring articular congruity and syndesmotic stability.
Posterior malleolar fractures, often components of complex ankle fracture patterns (trimalleolar, pilon variants), have a significant impact on ankle stability and long-term functional outcomes. Epidemiological data indicate that posterior malleolar involvement occurs in approximately 7-44% of all ankle fractures, with larger fragments and greater displacement being associated with poorer outcomes if inadequately managed. The increasing understanding of the posterior malleolus's role in syndesmotic integrity and ankle joint stability has driven a shift towards direct anatomical reduction and stable internal fixation for fragments meeting specific criteria, typically involving more than 25% of the articular surface, significant displacement, or evidence of syndesmotic instability after primary fibular fixation.
While other approaches, such as the posteromedial or direct lateral trans-fibular fracture approach, can provide access to the posterolateral corner, they often compromise direct visualization, particularly for larger or more complex posterior malleolar fragments. The posterolateral approach, therefore, serves as a cornerstone in the armamentarium of the orthopedic surgeon for specific indications, emphasizing precision and comprehensive anatomical restoration.
Surgical Anatomy & Biomechanics
A profound understanding of the intricate anatomy of the posterior ankle is critical for safe and effective execution of the posterolateral approach. The key structures encountered, and those requiring meticulous identification and protection, include osseous landmarks, musculotendinous units, neurovascular elements, and ligamentous complexes.
Osseous Structures
The primary osseous targets for this approach are the posterior aspect of the distal tibia, specifically the posterior malleolus, and the distal fibula. The posterior malleolus contributes significantly to the posterior articular surface of the tibiotalar joint and serves as the attachment point for the posterior inferior tibiofibular ligament (PITFL), a crucial component of the syndesmosis. The fibula, located laterally, forms the lateral malleolus and provides attachment for the posterior talofibular and calcaneofibular ligaments. Recognition of the fibular incisura on the tibia is also important for syndesmotic reduction.
Musculotendinous Units
The posterolateral approach involves navigating through several distinct musculotendinous planes:
*
Superficial Posterior Compartment:
This compartment contains the gastrocnemius, soleus, and plantaris muscles, which converge to form the Achilles tendon. The Achilles tendon forms the medial boundary of the superficial dissection plane.
*
Lateral Compartment:
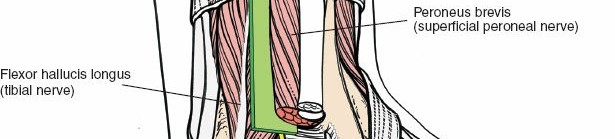
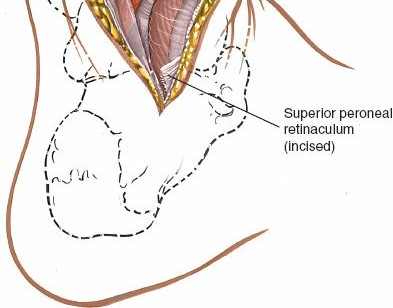
The peroneus longus and brevis tendons are situated laterally, deep to the peroneal retinaculum, and define the lateral boundary of the approach. These tendons are typically retracted laterally.
*
Deep Posterior Compartment:
This compartment houses the tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) muscles and their respective tendons.
*
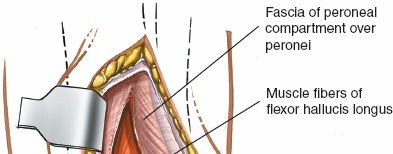
Flexor Hallucis Longus (FHL):
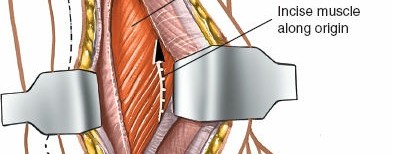
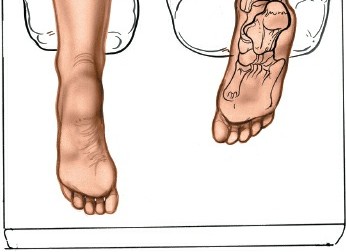
This muscle is of paramount importance in the posterolateral approach. Its muscle belly originates from the posterior aspect of the fibula and the interosseous membrane, with its tendon coursing distally along the posterior aspect of the distal tibia, deep to the peroneal tendons and superficial to the posterior tibiofibular ligament. The FHL tendon then passes through its own groove on the posterior aspect of the talus, inferior to the sustentaculum tali, before inserting into the distal phalanx of the great toe. During the posterolateral approach, the FHL muscle belly and tendon lie directly over the posterior aspect of the distal tibia and the posterior malleolus. It serves as a key surgical landmark and its careful medial retraction is crucial for exposing the operative field.
*
Flexor Digitorum Longus (FDL):
Located medial to the FHL, its tendon also contributes to the deep posterior compartment.
*
Tibialis Posterior (TP):
Most medially located in the deep posterior compartment, its tendon passes through the tarsal tunnel.
Neurovascular Structures
The principal neurovascular structures at risk in this approach are:
*
Sural Nerve:
Arising from the tibial and common peroneal nerves, it typically courses superficially along the posterolateral aspect of the leg, crossing the incision line in its distal part. It must be identified and protected during skin incision and superficial dissection, usually by retracting it laterally.
*
Posterior Tibial Neurovascular Bundle:
Comprising the tibial nerve, posterior tibial artery, and accompanying veins, this bundle courses through the tarsal tunnel region. It lies posteromedial to the FHL tendon, typically between the FDL and FHL. Meticulous medial retraction of the FHL must be performed with caution to avoid traction injury or direct damage to this critical bundle.
Ligamentous Structures
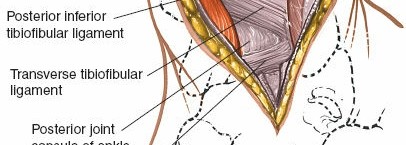
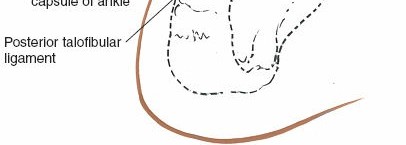
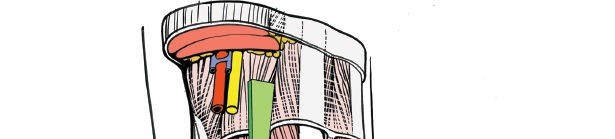
- Syndesmotic Ligaments: The posterior inferior tibiofibular ligament (PITFL) is a robust ligament that originates from the posterior aspect of the distal tibia (posterior malleolus) and inserts into the fibula. It is often intimately involved in posterior malleolar fractures, as the fragment may represent its avulsion or the ligament may remain attached to the fragment. The PITFL is visualized directly with this approach.
- Posterior Capsular Ligaments: The posterior capsule of the ankle joint and its thickenings (e.g., posterior talofibular ligament, calcaneofibular ligament) are encountered and may need to be incised or elevated for direct articular visualization.
Biomechanics
The posterior malleolus plays a critical role in ankle joint stability, particularly in preventing posterior talar subluxation and contributing to syndesmotic integrity. Its posteromedial aspect provides attachment for the deep portion of the PITFL, while its posterolateral portion often relates to the superficial PITFL. Fixation of displaced posterior malleolar fractures aims to restore not only the articular surface but also these crucial ligamentous attachments, thereby re-establishing syndesmotic stability. The FHL muscle, while a surgical landmark, is also a powerful plantarflexor of the great toe and an accessory ankle plantarflexor. Injury or impingement of the FHL during or after surgery can result in hallux pain, weakness, or tenosynovitis, underscoring the need for careful handling.
Indications & Contraindications
The decision to utilize the posterolateral approach is guided by specific indications for direct posterior ankle pathology and by a careful consideration of contraindications.
Indications
Operative Indications
-
Displaced Posterior Malleolar Fractures:
- Fragments comprising ≥25% of the articular surface (though newer evidence often emphasizes displacement and instability over fixed size thresholds).
- Articular step-off or gap ≥2 mm.
- Persistent syndesmotic instability after fibular and/or medial malleolar fixation.
- Posterior pilon fractures involving significant comminution or displacement of the posterior metaphysis and articular surface.
- Posterior Ankle Impingement: Excision of posterior osteophytes (e.g., in "nutcracker" type impingement or os trigonum syndrome), or removal of soft tissue hypertrophic synovium.
- Posterior Ankle Arthrodesis: Particularly for isolated posterior facet subtalar fusion or posterior tibiotalar fusion.
-
Excision of Posterior Ankle Lesions:
- Removal of sequestra (e.g., in osteomyelitis).
- Biopsy or excision of benign tumors (e.g., osteoid osteoma, ganglion cysts).
- Removal of loose bodies from the posterior ankle joint.
- Posterior Capsulotomy and Syndesmotomy: For specific cases of ankle contractures or syndesmotic tethering, although these are rare primary indications for this extensive approach.
- Tendon Procedures: While not a primary approach for isolated tendon lengthening, it may facilitate accessory lengthening of the FHL or FDL if necessary in the context of other procedures.
Non-Operative Indications
Fractures not meeting the criteria for surgical intervention, such as:
* Non-displaced or minimally displaced posterior malleolar fragments (<2 mm step-off/gap).
* Fragments comprising <25% of the articular surface with no evidence of syndesmotic instability.
* Patients with significant medical comorbidities precluding surgical intervention.
* Patients who are non-ambulatory or have limited functional demands.
| Indication Type | Specific Conditions |
|---|---|
| Operative |
- Displaced posterior malleolar fractures (≥25% articular surface, ≥2mm displacement, syndesmotic instability)
- Posterior pilon fractures - Posterior ankle impingement (osteophyte excision) - Posterior ankle arthrodesis (tibiotalar, subtalar posterior facet) - Excision of sequestra, benign tumors, loose bodies |
| Non-Operative |
- Non-displaced or minimally displaced posterior malleolar fractures (<2mm displacement, <25% articular surface, stable syndesmosis)
- Patients with prohibitive medical comorbidities - Non-ambulatory patients |
Contraindications
- Significant Soft Tissue Compromise: Open fractures with extensive contamination or severe crush injuries, active local infection, or critical soft tissue necrosis precluding safe wound closure.
- Concomitant Injuries Limiting Patient Positioning: As noted in the original seed content, if simultaneous open reduction and internal fixation of combined fibular and medial malleolar fractures are required, a prone position may not be ideal. In such cases, alternative approaches (e.g., dual incisions with patient supine, or sequential procedures) should be considered, although direct visualization of the posterior malleolus through the fibular fracture site may be insufficient for anatomical reduction.
- Severe Peripheral Vascular Disease or Neuropathy: Impaired healing potential and increased risk of complications.
- Morbid Obesity: May hinder adequate patient positioning, surgical access, and increase the risk of wound complications.
- Absence of Specific Indications: The approach should not be undertaken without a clear indication, as it is invasive and carries inherent risks.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for optimizing surgical outcomes and minimizing complications.
Pre-Operative Planning
- Clinical Assessment: A comprehensive history and physical examination, focusing on neurovascular status, soft tissue envelope integrity, and evaluation for open wounds or blisters.
-
Imaging Review:
- Standard Radiographs: Anteroposterior, lateral, and mortise views of the ankle are initial requirements.
- Computed Tomography (CT) Scan: This is indispensable for evaluating posterior malleolar fractures. A CT scan with 3D reconstructions provides detailed information regarding fragment size, comminution, articular step-off, displacement, and involvement of the incisura fibularis. This aids in surgical approach selection and implant templating.
- Magnetic Resonance Imaging (MRI): Rarely indicated for acute fractures but useful for soft tissue pathology (e.g., FHL tenosynovitis, posterior impingement syndrome) or assessment of ligamentous injuries.
-
Surgical Strategy:
- Determine the optimal approach based on fracture morphology and concomitant injuries.
- Plan for implant selection (e.g., small fragment plates, specialized posterior malleolar plates, lag screws).
- Anticipate the need for syndesmotic fixation if instability is present or expected.
- Discuss potential adjunctive procedures (e.g., arthroscopy).
- Patient Counseling: Comprehensive discussion of the surgical procedure, potential risks (infection, nerve injury, wound issues, nonunion, post-traumatic arthritis), expected recovery, and rehabilitation protocol.
- Prophylaxis: Administer pre-operative antibiotics (e.g., cefazolin) within one hour of incision. Institute deep vein thrombosis (DVT) prophylaxis according to institutional guidelines.
Patient Positioning
The prone position is standard for the posterolateral approach, offering optimal visualization of the posterior ankle.
1.
Anesthesia:
General or regional anesthesia is suitable.
2.
Positioning:
* The patient is carefully turned to the prone position on the operating table.
* Adequate padding is crucial to prevent pressure points: under the chest/shoulders, knees, and shins. A bolster placed under the distal tibia and feet, allowing the ankle to flex freely, is often beneficial.
* The torso can be slightly elevated to facilitate abdominal breathing and reduce venous congestion, which helps minimize bleeding.
* Ensure the foot can be freely manipulated and is accessible for fluoroscopy.

3.
Tourniquet:
A thigh tourniquet is typically applied for hemostasis, although its inflation time should be closely monitored.
4.
Sterile Prep and Drape:
The entire leg from above the knee to the toes is prepped and draped in a sterile fashion, allowing for full range of motion of the ankle and access for intraoperative fluoroscopy.
5.
C-arm Positioning:
The image intensifier should be positioned to allow for clear anteroposterior, lateral, and mortise views of the ankle joint without repositioning the patient.
Detailed Surgical Approach / Technique
The posterolateral approach provides direct access to the posterior tibia and fibula, utilizing well-defined anatomical planes. The meticulous execution of each step is critical for successful outcomes and avoidance of complications, especially concerning the FHL and neurovascular structures.
Landmarks and Incision
-
Landmarks:
Clearly identify and palpate the lateral malleolus, the palpable border of the Achilles tendon, and the fibular shaft. The sural nerve location should be anticipated.
 -
Incision:
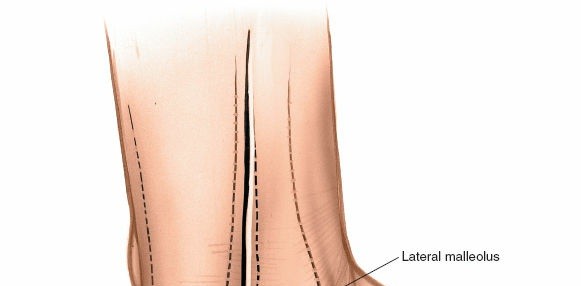
A longitudinal incision, typically 10-15 cm in length, is made on the posterolateral aspect of the leg. It generally runs parallel to the Achilles tendon and the fibular shaft, centered between the Achilles tendon medially and the peroneal tendons laterally. The incision starts approximately 5-7 cm proximal to the tip of the lateral malleolus and extends distally to the level of the calcaneal tuberosity or beyond, depending on the pathology. A curvilinear or slightly S-shaped incision may be preferred by some surgeons to improve skin laxity for closure and reduce tension.

Superficial Dissection and Internervous Plane
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue. Exercise caution to identify and protect the sural nerve, which typically lies superficial and lateral to the incision, but can have anatomical variations. The lesser saphenous vein, often accompanying the sural nerve, should also be identified and ligated or protected if encountered.
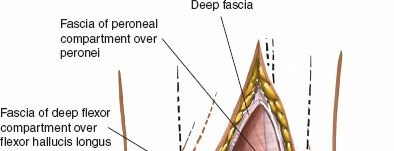
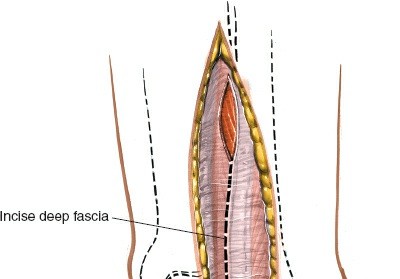
- Deep Fascia: Incise the deep fascia of the leg along the line of the skin incision. This exposes the superficial posterior compartment muscles.
-
Internervous Plane:
The posterolateral approach exploits the interval between the Achilles tendon (medially) and the peroneal tendons (laterally).
- Retract the Achilles tendon and the overlying gastrocnemius-soleus complex medially.
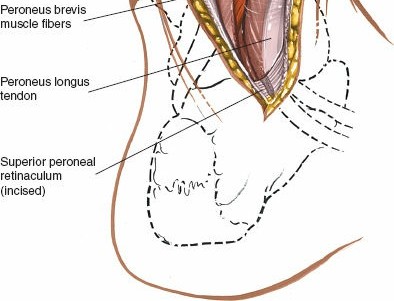
- Identify the peroneal longus and brevis tendons lying within their sheath along the lateral aspect of the fibula. Retract these tendons laterally, taking care to preserve their retinacula if possible.
Deep Dissection and FHL Exposure
-
Exposure of Deep Posterior Compartment:
After retracting the Achilles tendon medially and peroneal tendons laterally, the deep fascia overlying the deep posterior compartment is exposed. Incise this deep fascia carefully.
 -
Identifying the FHL:
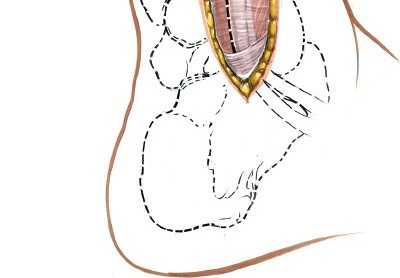
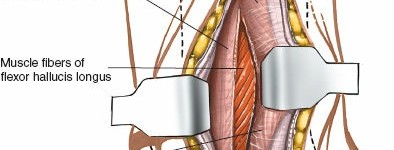
The flexor hallucis longus (FHL) muscle belly and tendon are the crucial structures encountered in this deeper plane. The FHL lies directly on the posterior aspect of the distal tibia and fibula. Identify its muscle belly proximally and trace its tendon distally as it courses over the posterior tibia. It is enveloped in its own synovial sheath.

 -
Neurovascular Protection:
The posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery, accompanying veins) is located
medial
to the FHL, nestled between the FHL and FDL tendons within the tarsal tunnel area. To expose the posterior malleolus, the FHL is carefully retracted
medially
. This maneuver must be performed with utmost care to protect the underlying neurovascular bundle from traction, compression, or direct injury. Using a broad blunt retractor (e.g., Hohmann or Fukuda) and maintaining constant visual vigilance is paramount.

Access to Posterior Malleolus/Distal Tibia
-
Posterior Capsule/Ligaments:
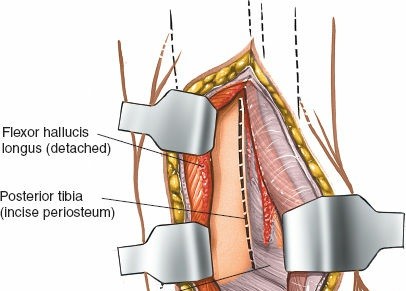
With the FHL retracted medially, the posterior aspect of the distal tibia, including the posterior malleolus, becomes visible. The posterior tibiofibular ligament (PITFL) and the posterior capsule of the ankle joint lie directly superficial to the bone. These structures may need to be incised or elevated off the posterior malleolar fragment for direct visualization of the fracture site and the articular surface. Incisions should be longitudinal to allow for later repair.
Fracture Reduction and Fixation
-
Reduction:
Direct visualization of the articular fragment allows for precise anatomical reduction.
- Periosteal elevators or small, pointed reduction clamps can be used to manipulate the fragment.
- Small K-wires or Hohmann retractors can serve as joysticks to control the fragment.
- Restore the articular surface congruity first, ensuring no step-off or gap.
-
Assess the syndesmotic reduction directly by visualizing the fibular incisura or by gently stressing the syndesmosis.

- Temporary Fixation: Once anatomical reduction is achieved, temporarily secure the fragment with one or more K-wires, ensuring they do not interfere with definitive hardware placement.
-
Definitive Fixation:
- Lag Screws: For large, single fragments, 3.5mm or 4.0mm cortical lag screws can be placed from posterior to anterior, crossing the fracture line and engaging the anterior tibial cortex. Ensure correct screw length to avoid penetration of the anterior skin or soft tissues.
-
Plating:
A contoured small fragment plate (e.g., 1/3 tubular plate, 2.7/3.5mm locking plate designed for posterior malleolus) is commonly used. The plate is typically positioned along the posterior aspect of the distal tibia, providing buttress or neutralization fixation. Screws are inserted through the plate, ensuring bicortical purchase where appropriate and avoiding joint penetration.
-
Syndesmotic Assessment:
After fixation of the posterior malleolus, reassess syndesmotic stability. If instability persists (e.g., positive Cotton test, external rotation stress radiographs under fluoroscopy), syndesmotic fixation with a screw or suture button construct is necessary.
Wound Closure
- Irrigation: Copious irrigation of the surgical site to remove debris.
- FHL Tendon Sheath: Reapproximate the fascial sheath over the FHL tendon to prevent impingement.
- Deep Fascia: Close the deep fascia, restoring the anatomical planes.
-
Subcutaneous and Skin:
Close the subcutaneous tissue and skin layers meticulously to minimize dead space and optimize wound healing. A drain may be considered if significant hematoma formation is anticipated.

 -
Dressing:
Apply a sterile dressing and a posterior splint or protective boot, maintaining the ankle in a neutral or slightly plantarflexed position.
Complications & Management
Despite meticulous surgical technique, complications can arise following the posterolateral ankle approach. Awareness of these potential issues and their management strategies is crucial for optimal patient care.
Common Complications
| Complication | Incidence (Approximate) | Salvage/Management Strategy ## Introduction & Epidemiology
The posterolateral approach to the ankle joint represents a highly effective surgical corridor for addressing a spectrum of pathologies affecting the posterior aspect of the distal tibia and ankle. While historically less frequently utilized than medial or lateral approaches, its utility, particularly in the management of posterior malleolar fractures, has garnered increasing recognition in contemporary orthopedic trauma surgery. This approach offers direct visualization and anatomical reduction capabilities, which are paramount for restoring articular congruity and syndesmotic stability.
Posterior malleolar fractures, often components of complex ankle fracture patterns (trimalleolar, pilon variants), have a significant impact on ankle stability and long-term functional outcomes. Epidemiological data indicate that posterior malleolar involvement occurs in approximately 7-44% of all ankle fractures, with larger fragments and greater displacement being associated with poorer outcomes if inadequately managed. The increasing understanding of the posterior malleolus's role in syndesmotic integrity and ankle joint stability has driven a shift towards direct anatomical reduction and stable internal fixation for fragments meeting specific criteria, typically involving more than 25% of the articular surface, significant displacement, or evidence of syndesmotic instability.
While other approaches, such as the posteromedial or direct lateral trans-fibular fracture approach, can provide access to the posterolateral corner, they often compromise direct visualization, particularly for larger or more complex posterior malleolar fragments. The posterolateral approach, therefore, serves as a cornerstone in the armamentarium of the orthopedic surgeon for specific indications, emphasizing precision and comprehensive anatomical restoration. Its other uses include the following, as provided in the initial content:
1. Excision of sequestra
2. Removal of benign tumors
3. Arthrodesis of the posterior facet of the subtalar joint
4. Posterior capsulotomy and syndesmotomy of the ankle
5. Elongation of tendons
Surgical Anatomy & Biomechanics
A profound understanding of the intricate anatomy of the posterior ankle is critical for safe and effective execution of the posterolateral approach. The key structures encountered, and those requiring meticulous identification and protection, include osseous landmarks, musculotendinous units, neurovascular elements, and ligamentous complexes.
Osseous Structures
The primary osseous targets for this approach are the posterior aspect of the distal tibia, specifically the posterior malleolus, and the distal fibula. The posterior malleolus contributes significantly to the posterior articular surface of the tibiotalar joint and serves as the attachment point for the posterior inferior tibiofibular ligament (PITFL), a crucial component of the syndesmosis. The fibula, located laterally, forms the lateral malleolus and provides attachment for the posterior talofibular and calcaneofibular ligaments. Recognition of the fibular incisura on the tibia is also important for syndesmotic reduction.
Musculotendinous Units
The posterolateral approach involves navigating through several distinct musculotendinous planes:
*
Superficial Posterior Compartment:
This compartment contains the gastrocnemius, soleus, and plantaris muscles, which converge to form the Achilles tendon. The Achilles tendon forms the medial boundary of the superficial dissection plane.
*
Lateral Compartment:
The peroneus longus and brevis tendons are situated laterally, deep to the peroneal retinaculum, and define the lateral boundary of the approach. These tendons are typically retracted laterally.
*
Deep Posterior Compartment:
This compartment houses the tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) muscles and their respective tendons.
*
Flexor Hallucis Longus (FHL):
This muscle is of paramount importance in the posterolateral approach. Its muscle belly originates from the posterior aspect of the fibula and the interosseous membrane, with its tendon coursing distally along the posterior aspect of the distal tibia, deep to the peroneal tendons and superficial to the posterior tibiofibular ligament. The FHL tendon then passes through its own groove on the posterior aspect of the talus, inferior to the sustentaculum tali, before inserting into the distal phalanx of the great toe. During the posterolateral approach, the FHL muscle belly and tendon lie directly over the posterior aspect of the distal tibia and the posterior malleolus. It serves as a key surgical landmark, and its careful medial retraction is crucial for exposing the operative field.
*
Flexor Digitorum Longus (FDL):
Located medial to the FHL, its tendon also contributes to the deep posterior compartment.
*
Tibialis Posterior (TP):
Most medially located in the deep posterior compartment, its tendon passes through the tarsal tunnel.
Neurovascular Structures
The principal neurovascular structures at risk in this approach are:
*
Sural Nerve:
Arising from the tibial and common peroneal nerves, it typically courses superficially along the posterolateral aspect of the leg, crossing the incision line in its distal part. It must be identified and protected during skin incision and superficial dissection, usually by retracting it laterally.
*
Posterior Tibial Neurovascular Bundle:
Comprising the tibial nerve, posterior tibial artery, and accompanying veins, this bundle courses through the tarsal tunnel region. It lies posteromedial to the FHL tendon, typically between the FDL and FHL. Meticulous medial retraction of the FHL must be performed with caution to avoid traction injury or direct damage to this critical bundle.
Ligamentous Structures
- Syndesmotic Ligaments: The posterior inferior tibiofibular ligament (PITFL) is a robust ligament that originates from the posterior aspect of the distal tibia (posterior malleolus) and inserts into the fibula. It is often intimately involved in posterior malleolar fractures, as the fragment may represent its avulsion or the ligament may remain attached to the fragment. The PITFL is visualized directly with this approach.
- Posterior Capsular Ligaments: The posterior capsule of the ankle joint and its thickenings (e.g., posterior talofibular ligament, calcaneofibular ligament) are encountered and may need to be incised or elevated for direct articular visualization.
Biomechanics
The posterior malleolus plays a critical role in ankle joint stability, particularly in preventing posterior talar subluxation and contributing to syndesmotic integrity. Its posteromedial aspect provides attachment for the deep portion of the PITFL, while its posterolateral portion often relates to the superficial PITFL. Fixation of displaced posterior malleolar fractures aims to restore not only the articular surface but also these crucial ligamentous attachments, thereby re-establishing syndesmotic stability. The FHL muscle, while a surgical landmark, is also a powerful plantarflexor of the great toe and an accessory ankle plantarflexor. Injury or impingement of the FHL during or after surgery can result in hallux pain, weakness, or tenosynovitis, underscoring the need for careful handling.
Indications & Contraindications
The decision to utilize the posterolateral approach is guided by specific indications for direct posterior ankle pathology and by a careful consideration of contraindications.
Indications
Operative Indications
-
Displaced Posterior Malleolar Fractures:
- Fragments comprising ≥25% of the articular surface (though newer evidence often emphasizes displacement and instability over fixed size thresholds).
- Articular step-off or gap ≥2 mm.
- Persistent syndesmotic instability after fibular and/or medial malleolar fixation.
- Posterior pilon fractures involving significant comminution or displacement of the posterior metaphysis and articular surface.
- Posterior Ankle Impingement: Excision of posterior osteophytes (e.g., in "nutcracker" type impingement or os trigonum syndrome), or removal of soft tissue hypertrophic synovium.
- Posterior Ankle Arthrodesis: Particularly for isolated posterior facet subtalar fusion or posterior tibiotalar fusion.
-
Excision of Posterior Ankle Lesions:
- Removal of sequestra (e.g., in osteomyelitis).
- Biopsy or excision of benign tumors (e.g., osteoid osteoma, ganglion cysts).
- Removal of loose bodies from the posterior ankle joint.
- Posterior Capsulotomy and Syndesmotomy: For specific cases of ankle contractures or syndesmotic tethering, although these are rare primary indications for this extensive approach.
- Tendon Procedures: While not a primary approach for isolated tendon lengthening, it may facilitate accessory lengthening of the FHL or FDL if necessary in the context of other procedures.
Non-Operative Indications
Fractures not meeting the criteria for surgical intervention, such as:
* Non-displaced or minimally displaced posterior malleolar fragments (<2 mm step-off/gap).
* Fragments comprising <25% of the articular surface with no evidence of syndesmotic instability.
* Patients with significant medical comorbidities precluding surgical intervention.
* Patients who are non-ambulatory or have limited functional demands.
| Indication Type | Specific Conditions |
|---|---|
| Operative |
- Displaced posterior malleolar fractures (≥25% articular surface, ≥2mm displacement, syndesmotic instability)
- Posterior pilon fractures - Posterior ankle impingement (osteophyte excision) - Posterior ankle arthrodesis (tibiotalar, subtalar posterior facet) - Excision of sequestra, benign tumors, loose bodies |
| Non-Operative |
- Non-displaced or minimally displaced posterior malleolar fractures (<2mm displacement, <25% articular surface, stable syndesmosis)
- Patients with prohibitive medical comorbidities - Non-ambulatory patients |
Contraindications
- Significant Soft Tissue Compromise: Open fractures with extensive contamination or severe crush injuries, active local infection, or critical soft tissue necrosis precluding safe wound closure.
- Concomitant Injuries Limiting Patient Positioning: As noted in the original seed content, if simultaneous open reduction and internal fixation of combined fibular and medial malleolar fractures are required, a prone position may not be ideal. In such cases, alternative approaches (e.g., dual incisions with patient supine, or sequential procedures) should be considered, although direct visualization of the posterior malleolus through the fibular fracture site may be insufficient for anatomical reduction.
- Severe Peripheral Vascular Disease or Neuropathy: Impaired healing potential and increased risk of complications.
- Morbid Obesity: May hinder adequate patient positioning, surgical access, and increase the risk of wound complications.
- Absence of Specific Indications: The approach should not be undertaken without a clear indication, as it is invasive and carries inherent risks.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for optimizing surgical outcomes and minimizing complications.
Pre-Operative Planning
- Clinical Assessment: A comprehensive history and physical examination, focusing on neurovascular status, soft tissue envelope integrity, and evaluation for open wounds or blisters.
-
Imaging Review:
- Standard Radiographs: Anteroposterior, lateral, and mortise views of the ankle are initial requirements.
- Computed Tomography (CT) Scan: This is indispensable for evaluating posterior malleolar fractures. A CT scan with 3D reconstructions provides detailed information regarding fragment size, comminution, articular step-off, displacement, and involvement of the incisura fibularis. This aids in surgical approach selection and implant templating.
- Magnetic Resonance Imaging (MRI): Rarely indicated for acute fractures but useful for soft tissue pathology (e.g., FHL tenosynovitis, posterior impingement syndrome) or assessment of ligamentous injuries.
-
Surgical Strategy:
- Determine the optimal approach based on fracture morphology and concomitant injuries.
- Plan for implant selection (e.g., small fragment plates, specialized posterior malleolar plates, lag screws).
- Anticipate the need for syndesmotic fixation if instability is present or expected.
- Discuss potential adjunctive procedures (e.g., arthroscopy).
- Patient Counseling: Comprehensive discussion of the surgical procedure, potential risks (infection, nerve injury, wound issues, nonunion, post-traumatic arthritis), expected recovery, and rehabilitation protocol.
- Prophylaxis: Administer pre-operative antibiotics (e.g., cefazolin) within one hour of incision. Institute deep vein thrombosis (DVT) prophylaxis according to institutional guidelines.
Patient Positioning
The prone position is standard for the posterolateral approach, offering optimal visualization of the posterior ankle.
1.
Anesthesia:
General or regional anesthesia is suitable.
2.
Positioning:
* The patient is carefully turned to the prone position on the operating table.
* Adequate padding is crucial to prevent pressure points: under the chest/shoulders, knees, and shins. A bolster placed under the distal tibia and feet, allowing the ankle to flex freely, is often beneficial.
* The torso can be slightly elevated to facilitate abdominal breathing and reduce venous congestion, which helps minimize bleeding.
* Ensure the foot can be freely manipulated and is accessible for fluoroscopy.


3.
Tourniquet:
A thigh tourniquet is typically applied for hemostasis, although its inflation time should be closely monitored.
4.
Sterile Prep and Drape:
The entire leg from above the knee to the toes is prepped and draped in a sterile fashion, allowing for full range of motion of the ankle and access for intraoperative fluoroscopy.

5.
C-arm Positioning:
The image intensifier should be positioned to allow for clear anteroposterior, lateral, and mortise views of the ankle joint without repositioning the patient.
Detailed Surgical Approach / Technique
The posterolateral approach provides direct access to the posterior tibia and fibula, utilizing well-defined anatomical planes. The meticulous execution of each step is critical for successful outcomes and avoidance of complications, especially concerning the FHL and neurovascular structures.
Landmarks and Incision
-
Landmarks:
Clearly identify and palpate the lateral malleolus, the palpable border of the Achilles tendon, and the fibular shaft. The sural nerve location should be anticipated.
 -
Incision:
A longitudinal incision, typically 10-15 cm in length, is made on the posterolateral aspect of the leg. It generally runs parallel to the Achilles tendon and the fibular shaft, centered between the Achilles tendon medially and the peroneal tendons laterally. The incision starts approximately 5-7 cm proximal to the tip of the lateral malleolus and extends distally to the level of the calcaneal tuberosity or beyond, depending on the pathology. A curvilinear or slightly S-shaped incision may be preferred by some surgeons to improve skin laxity for closure and reduce tension.

Superficial Dissection and Internervous Plane
- Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue. Exercise caution to identify and protect the sural nerve, which typically lies superficial and lateral to the incision, but can have anatomical variations. The lesser saphenous vein, often accompanying the sural nerve, should also be identified and ligated or protected if encountered.
- Deep Fascia: Incise the deep fascia of the leg along the line of the skin incision. This exposes the superficial posterior compartment muscles.
-
Internervous Plane:
The posterolateral approach exploits the interval between the Achilles tendon (medially) and the peroneal tendons (laterally).
- Retract the Achilles tendon and the overlying gastrocnemius-soleus complex medially.
- Identify the peroneal longus and brevis tendons lying within their sheath along the lateral aspect of the fibula. Retract these tendons laterally, taking care to preserve their retinacula if possible.
Deep Dissection and FHL Exposure
-
Exposure of Deep Posterior Compartment:
After retracting the Achilles tendon medially and peroneal tendons laterally, the deep fascia overlying the deep posterior compartment is exposed. Incise this deep fascia carefully.
 -
Identifying the FHL:
The flexor hallucis longus (FHL) muscle belly and tendon are the crucial structures encountered in this deeper plane. The FHL lies directly on the posterior aspect of the distal tibia and fibula. Identify its muscle belly proximally and trace its tendon distally as it courses over the posterior tibia. It is enveloped in its own synovial sheath.

 -
Neurovascular Protection:
The posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery, accompanying veins) is located
medial
to the FHL, nestled between the FHL and FDL tendons within the tarsal tunnel area. To expose the posterior malleolus, the FHL is carefully retracted
medially
. This maneuver must be performed with utmost care to protect the underlying neurovascular bundle from traction, compression, or direct injury. Using a broad blunt retractor (e.g., Hohmann or Fukuda) and maintaining constant visual vigilance is paramount.

Access to Posterior Malleolus/Distal Tibia
-
Posterior Capsule/Ligaments:
With the FHL retracted medially, the posterior aspect of the distal tibia, including the posterior malleolus, becomes visible. The posterior tibiofibular ligament (PITFL) and the posterior capsule of the ankle joint lie directly superficial to the bone. These structures may need to be incised or elevated off the posterior malleolar fragment for direct visualization of the fracture site and the articular surface. Incisions should be longitudinal to allow for later repair.


Fracture Reduction and Fixation
-
Reduction:
Direct visualization of the articular fragment allows for precise anatomical reduction.
- Periosteal elevators or small, pointed reduction clamps can be used to manipulate the fragment.
- Small K-wires or Hohmann retractors can serve as joysticks to control the fragment.
- Restore the articular surface congruity first, ensuring no step-off or gap.
-
Assess the syndesmotic reduction directly by visualizing the fibular incisura or by gently stressing the syndesmosis.

- Temporary Fixation: Once anatomical reduction is achieved, temporarily secure the fragment with one or more K-wires, ensuring they do not interfere with definitive hardware placement.
-
Definitive Fixation:
- Lag Screws: For large, single fragments, 3.5mm or 4.0mm cortical lag screws can be placed from posterior to anterior, crossing the fracture line and engaging the anterior tibial cortex. Ensure correct screw length to avoid penetration of the anterior skin or soft tissues.
-
Plating:
A contoured small fragment plate (e.g., 1/3 tubular plate, 2.7/3.5mm locking plate designed for posterior malleolus) is commonly used. The plate is typically positioned along the posterior aspect of the distal tibia, providing buttress or neutralization fixation. Screws are inserted through the plate, ensuring bicortical purchase where appropriate and avoiding joint penetration.



-
Syndesmotic Assessment:
After fixation of the posterior malleolus, reassess syndesmotic stability. If instability persists (e.g., positive Cotton test, external rotation stress radiographs under fluoroscopy), syndesmotic fixation with a screw or suture button construct is necessary.

Wound Closure
- Irrigation: Copious irrigation of the surgical site to remove debris.
- FHL Tendon Sheath: Reapproximate the fascial sheath over the FHL tendon to prevent impingement.
- Deep Fascia: Close the deep fascia, restoring the anatomical planes.
-
Subcutaneous and Skin:
Close the subcutaneous tissue and skin layers meticulously to minimize dead space and optimize wound healing. A drain may be considered if significant hematoma formation is anticipated.

 -
Dressing:
Apply a sterile dressing and a posterior splint or protective boot, maintaining the ankle in a neutral or slightly plantarflexed position.

Complications & Management
Despite meticulous surgical technique, complications can arise following the posterolateral ankle approach. Awareness of these potential issues and their management strategies is crucial for optimal patient care.
Common Complications
| Complication | Incidence (Approximate) | Salvage/Management Strategy |
|
Infection
| 1-3% | -
Superficial:
Local wound care, topical antibiotics.
-
Deep:
Surgical debridement, hardware retention if fracture stable, appropriate systemic antibiotics. If severe or persistent infection, hardware removal.
-
Osteomyelitis:
Debridement, long-term antibiotics, potential bone resection and reconstruction. |
|
Neurovascular Injury
| Low (0.5-2%) | -
Sural Nerve:
Most common. Observe for recovery if neuropraxia suspected. If neuroma or persistent pain, consider neurectomy or neurolysis.
-
Tibial Nerve/Posterior Tibial Artery:
Requires immediate exploration, microvascular repair of artery/vein, nerve repair/grafting if transected. |
|
Wound Healing Complications
| 2-5% | -
Dehiscence:
Secondary intention healing, wound vac, local flap if severe.
-
Hematoma:
Evacuation if symptomatic or expanding.
-
Seroma:
Aspiration.
-
Skin Necrosis:
Debridement, plastic surgery consultation for skin grafting or local flap. |
|
FHL Tendonitis/Impingement
| Low | - Rest, NSAIDs, physical therapy.
- Local corticosteroid injection (if no fracture consolidation concerns).
- Surgical release of the tendon sheath, debridement if needed. |
|
Malunion/Nonunion
| 1-5% | -
Malunion (asymptomatic):
Observation.
-
Malunion (symptomatic/deforming):
Corrective osteotomy and fixation.
-
Nonunion:
Revision surgery with debridement, bone grafting, and stable fixation. |
|
Malunion/Nonunion
| 1-5% | -
Malunion (asymptomatic):
Observation.
-
Malunion (symptomatic/deforming):
Corrective osteotomy and fixation.
-
Nonunion:
Revision surgery with debridement, bone grafting, and stable fixation. |
Management of Specific Complications
- Infection: Superficial infections are managed with aggressive local wound care and oral antibiotics. Deep infections, especially around hardware, often require surgical debridement, intravenous antibiotics, and sometimes hardware removal. If the fracture is stable, removal of hardware may be delayed until the fracture is healed.
- Neurovascular Injury: If a nerve palsy is observed postoperatively, it is initially treated expectantly, as neuropraxia is common. Nerve conduction studies and electromyography can confirm the extent of injury. If no recovery is noted after several months, surgical exploration may be warranted. Vascular injuries require immediate surgical exploration and repair by a vascular surgeon.
- Wound Healing Complications: Local wound care, strict elevation, and offloading are key. Dehiscence may require secondary intention healing, negative pressure wound therapy, or surgical débridement and re-closure. Severe soft tissue deficits may necessitate plastic surgical intervention (e.g., local or free flap).
- Malunion/Nonunion: Asymptomatic malunion may be observed. Symptomatic malunion, particularly with articular incongruity or deformity, typically requires corrective osteotomy. Nonunion requires revision surgery with thorough debridement, bone grafting (autograft or allograft), and stable internal fixation.
- Post-traumatic Arthritis: Long-term management involves conservative measures (NSAIDs, activity modification, bracing). For end-stage arthritis, surgical options include arthrodesis (fusion) or total ankle arthroplasty, depending on patient factors and surgeon preference.
- FHL Tenosynovitis/Impingement: Initial management includes rest, NSAIDs, physical therapy, and potentially a corticosteroid injection into the tendon sheath (avoiding the tendon substance). If conservative measures fail, surgical release of the FHL sheath or debridement of inflammatory tissue may be necessary. Ensure that hardware is not impinging on the tendon.
- Hardware Irritation: If hardware becomes prominent or painful after fracture healing, elective removal can be considered, usually 6-12 months post-surgery.
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is crucial for achieving optimal functional outcomes after the posterolateral ankle approach. The protocol is typically staged and tailored to the specific fracture pattern, stability of fixation, and patient's healing capacity.
Initial Phase (Weeks 0-2)
- Immobilization: The ankle is immobilized in a posterior splint or controlled ankle motion (CAM) boot in a neutral or slightly plantarflexed position to protect the repair.
- Weight Bearing: Strict non-weight bearing (NWB) is maintained on the operative limb.
- Elevation and Ice: Consistent elevation of the limb above heart level and application of ice to reduce swelling and pain.
- Pain Management: Opioids and non-opioid analgesics as needed.
- Early Motion: Gentle, active range of motion of the toes, quadriceps sets, and gluteal strengthening exercises are encouraged. Ankle ROM is typically withheld in this phase to protect soft tissue and bony healing.
Intermediate Phase (Weeks 2-6)
- Immobilization: Transition to a CAM boot if not already in one.
- Weight Bearing: Gradual progression to partial weight bearing (PWB) as tolerated, typically starting at 25% of body weight, increasing weekly as per surgeon preference and radiographic evidence of early healing.
- Range of Motion: Begin gentle, active and passive range of motion exercises for the ankle, focusing on dorsiflexion, plantarflexion, inversion, and eversion, within pain limits. Avoid aggressive stretching or forced movements.
- Soft Tissue Management: Scar massage and desensitization exercises once the wound is well-healed.
- FHL-specific Exercises: Begin gentle, active great toe flexion exercises to promote FHL tendon gliding and prevent adhesions, once soft tissue healing permits.
Advanced Phase (Weeks 6-12)
- Immobilization: Discontinue CAM boot once radiographic healing is evident, pain permits, and ankle strength/ROM are adequate. Transition to supportive footwear.
- Weight Bearing: Progress to full weight bearing (FWB) as tolerated.
- Strengthening: Initiate progressive strengthening exercises for all ankle muscle groups, using resistance bands, calf raises (bilateral progressing to unilateral), and balance board exercises.
- Proprioception and Balance: Focus on single-leg stance, wobble board, and uneven surface walking to restore proprioception and balance.
- Functional Activities: Gradually increase activities of daily living (ADLs).
- FHL Strengthening: Progress FHL strengthening with resistance against great toe flexion.
Return to Sport/Full Activity (Months 3-6+)
- Sport-Specific Training: If applicable, begin sport-specific drills, agility training, and plyometrics under the guidance of a physical therapist.
- Endurance and Power: Continue with strengthening, conditioning, and cardiovascular exercises.
- Objective Criteria: Return to full activity or sport is typically based on achievement of specific functional benchmarks (e.g., >90% strength compared to contralateral limb, pain-free range of motion, successful completion of sport-specific tests).
- Hardware Management: If hardware is symptomatic, elective removal can be discussed after adequate bone healing (typically 12 months post-surgery).
Throughout all phases, close communication between the surgeon, physical therapist, and patient is paramount to tailor the protocol, address specific challenges, and ensure a safe and effective return to function.
Summary of Key Literature / Guidelines
The landscape of posterior malleolar fracture management has evolved significantly, largely driven by advances in imaging and surgical techniques, including the increasing utilization of direct posterior approaches.
Historically, posterior malleolar fractures were often considered secondary to fibular or medial malleolar injuries, with fixation thresholds frequently set at 25-33% of the articular surface. However, current literature, as outlined by Haraguchi et al. (2006) and Bartoníček et al. (2015) , emphasizes that even smaller fragments can significantly destabilize the syndesmosis and contribute to joint incongruity. Modern understanding prioritizes anatomical reduction of the articular surface and restoration of syndesmotic stability, irrespective of an arbitrary fragment size, especially in high-energy injuries or those with persistent syndesmotic instability after fibular fixation.
The superiority of direct posterior approaches (posterolateral or posteromedial) over indirect reduction techniques (e.g., via anterior approaches or external manipulation) for displaced posterior malleolar fractures is now widely accepted. Direct visualization facilitates anatomical reduction of the articular surface and stable fixation. Gardner et al. (2011) demonstrated improved anatomical reduction rates with direct posterior approaches compared to indirect methods.
Comparing the posterolateral and posteromedial approaches, Bartoníček et al. (2010, 2013) have extensively described the surgical anatomy and technical considerations. The posterolateral approach, which is the focus here, is particularly well-suited for fragments that are primarily posterolateral, often associated with pronation-external rotation or supination-external rotation injuries. It offers excellent visualization of the distal fibula and the posterior tibiofibular ligament complex. The posteromedial approach is preferred for larger, purely posteromedial fragments or those extending into the medial malleolus. The choice between these two posterior approaches depends on the precise fracture morphology as delineated by pre-operative CT imaging.
Recent advancements include specialized posterior plating systems designed to buttress the posterior malleolus and provide improved fixation stability, especially for comminuted fragments or those with metaphyseal extension. These plates often incorporate locking technology and anatomical contours to optimize outcomes.
Guidelines generally advocate for CT imaging in all ankle fractures with suspected posterior malleolar involvement to accurately characterize fragment size, displacement, and comminution. Surgical intervention is recommended for fragments with articular step-off or gapping ≥2mm, or those that contribute to syndesmotic instability even after primary fibular stabilization. The long-term outcomes of anatomically reduced and stably fixed posterior malleolar fractures are generally favorable, with lower rates of post-traumatic arthritis compared to malreduced fractures. The meticulous handling of the FHL muscle and protection of the posterior neurovascular bundle during the posterolateral approach are critical technical considerations supported by anatomical studies and clinical experience to mitigate specific approach-related complications.
Clinical & Radiographic Imaging