Optimizing the Posterior Approach with Olecranon Osteotomy for Elbow Trauma & Reconstruction
Key Takeaway
The posterior approach with olecranon osteotomy offers unparalleled visualization of the elbow's articular surfaces, crucial for complex distal humeral fractures, nonunions, or revision arthroplasty. It provides direct access for precise reduction and fixation, despite introducing a surgically created osteotomy requiring meticulous fixation and careful postoperative management to mitigate risks like nonunion.
Optimizing the Posterior Approach for Elbow with Olecranon Osteotomy
Introduction & Epidemiology
The posterior approach to the elbow, particularly when augmented by an olecranon osteotomy, offers unparalleled direct visualization of the distal humerus, olecranon, and the articular surfaces of the humeroulnar and humeroradial joints. This extensive exposure is critical for the accurate reduction and stable internal fixation of complex intra-articular fractures, removal of challenging intra-articular loose bodies, and the meticulous dissection required for the treatment of nonunions or revision arthroplasty of the distal humerus.
While providing a superior operative field, the posterior approach with an olecranon osteotomy introduces a surgically created "fracture" of the olecranon, which necessitates stable internal fixation as an integral part of the overall procedure. This secondary procedure inherently carries risks, including delayed union, nonunion, or symptomatic hardware, which underscore the importance of meticulous surgical technique and careful postoperative management. The decision to employ this approach is predicated on a careful risk-benefit analysis, weighing the enhanced visualization and improved potential for anatomical reduction against the potential morbidity associated with the osteotomy itself.
Distal humeral fractures, particularly the complex intra-articular types (e.g., AO/OTA C-type fractures), represent approximately 2-7% of all elbow fractures in adults, with a bimodal distribution affecting younger, high-energy trauma patients and older individuals with osteoporotic bone. Nonunions of the distal humerus, while less common, present significant functional challenges and often require extensive surgical intervention for satisfactory outcomes. The posterior approach with olecranon osteotomy is a cornerstone technique for addressing these challenging pathologies, emphasizing its enduring relevance in orthopedic trauma and reconstructive surgery of the elbow.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the regional anatomy and biomechanics is paramount for optimizing outcomes with the posterior approach and olecranon osteotomy.
Bony Anatomy
The elbow joint is a complex trochoginglymoid articulation, primarily comprising the humeroulnar, humeroradial, and proximal radioulnar joints.
*
Distal Humerus:
The distal humerus features the medial and lateral epicondyles, the capitellum (articulates with the radial head), and the trochlea (articulates with the olecranon). The olecranon fossa posteriorly accommodates the olecranon during extension. The columns of the distal humerus (medial and lateral) are critical for stability and fixation.
*
Olecranon:
The olecranon is the proximal projection of the ulna, forming the posterior part of the trochlear notch. Its articular surface, lined with cartilage, articulates with the trochlea. The triceps brachii tendon inserts robustly onto its posterior and superior aspects. The osteotomy site must be carefully selected to optimize exposure while preserving a sufficient fragment for stable fixation and minimizing damage to the articular cartilage.
Ligamentous Structures
The primary stabilizers of the elbow are the medial (ulnar) collateral ligament (UCL) complex and the lateral collateral ligament (LCL) complex. While the posterior approach does not directly disrupt these structures, excessive traction or uncontrolled dissection can risk their iatrogenic injury. The stability of the olecranon osteotomy and subsequent early motion protocols are dependent on the integrity of these ligaments.
Musculature
The triceps brachii muscle is the primary extensor of the elbow and inserts onto the olecranon. The continuity of the triceps mechanism with the olecranon fragment is crucial for its vascularity and for the functional recovery of elbow extension postoperatively. The approach effectively utilizes this muscle-tendon unit for reflection.
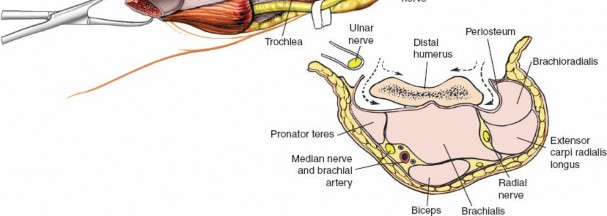
Neurovascular Structures
- Ulnar Nerve: The ulnar nerve is the most vulnerable structure in the posterior elbow. It courses in the cubital tunnel posterior to the medial epicondyle. Meticulous identification, isolation, and protection, often involving anterior transposition, are essential to prevent iatrogenic injury during exposure, osteotomy, or subsequent closure.
- Posterior Cutaneous Nerve of the Forearm: A branch of the radial nerve, it can be at risk during skin incision, contributing to sensory deficits if damaged.
- Brachial Artery and Median/Radial Nerves: These major neurovascular structures are situated anteriorly within the antecubital fossa and are generally not directly threatened by a carefully executed posterior approach, but their proximity necessitates awareness during deep dissection.
Biomechanics of Olecranon Osteotomy Fixation
The olecranon osteotomy must be rigidly fixed to allow for early motion and prevent nonunion. The olecranon is subjected to significant tensile forces from the triceps during extension.
*
Tension Band Principle:
This principle is often applied in olecranon osteotomy fixation, converting distractive forces (from triceps pull) into compressive forces at the articular surface when the elbow is flexed. This is typically achieved with K-wires and cerclage wire.
*
Plate Fixation:
Plates provide robust neutralization and compression, particularly for comminuted osteotomies or in osteoporotic bone, offering superior stability compared to tension band wiring alone in some biomechanical studies.
* The choice of osteotomy configuration (transverse, oblique, chevron) can influence stability and ease of fixation. A chevron osteotomy, for instance, provides inherent rotational stability.
Indications & Contraindications
The posterior approach with olecranon osteotomy is a powerful tool in the orthopedic surgeon's armamentarium, reserved for specific indications where maximal exposure is required.
Indications
-
Complex Intra-articular Distal Humerus Fractures:
Particularly AO/OTA type C fractures with significant comminution, displacement, or articular involvement requiring direct visualization for anatomical reduction and stable internal fixation.
- Examples: Bicolumnar distal humeral fractures, T-type, Y-type fractures.
- Distal Humerus Nonunions or Malunions: When revision surgery demands extensive exposure for debridement, bone grafting, and re-fixation.
- Removal of Difficult Intra-articular Loose Bodies: Especially when multiple, large, or incarcerated fragments are present within the olecranon fossa or trochlear notch.
- Complex Elbow Arthroplasty (Primary or Revision): Facilitates implant removal, precise bone preparation, and component insertion, particularly for total elbow arthroplasty.
- Coronoid Fractures Requiring Direct Anterior-Posterior Exposure: In conjunction with a lateral approach, the olecranon osteotomy can offer unique access to the coronoid from posterior in certain complex fracture patterns.
- Extensive Synovectomy or Debridement: For conditions like severe synovial chondromatosis or inflammatory arthritis where complete access to the joint is necessary.
Contraindications
- Active Infection: Any active infection in the vicinity of the elbow is a strict contraindication due to the risk of osteomyelitis and hardware infection.
- Severe Soft Tissue Compromise: Compromised skin integrity, severe burns, or significant soft tissue defects may preclude this approach.
- Severe Osteoporosis: While not an absolute contraindication, severe osteoporosis can make stable fixation of both the primary fracture and the olecranon osteotomy challenging, increasing the risk of failure.
- Patient Unfit for Prolonged Surgery/Anesthesia: The approach, especially for complex fractures, can be lengthy.
- Less Invasive Options Available: For simple fractures, extra-articular pathologies, or loose bodies accessible via smaller arthrotomies, an olecranon osteotomy is unnecessary.
- Relative Contraindications: Prior surgery with scar tissue, existing ulnar neuropathy (may necessitate additional caution/transposition).
Summary of Operative Indications
| Indication Type | Specific Conditions/Pathologies | Rationale for Posterior Approach with Olecranon Osteotomy | Alternative/Non-Operative Considerations |
|---|---|---|---|
| Fracture Fixation | Complex intra-articular distal humerus fractures (AO/OTA Type C), severe comminution, displaced articular fragments, bicolumnar. | Maximal articular visualization for anatomical reduction, stable internal fixation. | Simple, non-displaced fractures may be treated non-operatively or via less invasive approaches (e.g., triceps-sparing). |
| Nonunion/Malunion Management | Distal humerus nonunions/malunions requiring debridement, bone grafting, and revision fixation. | Extensive exposure for scar tissue excision, osteotomy/deformity correction. | Initial nonunions may be managed with less invasive techniques or targeted grafting. |
| Loose Body Excision | Large, multiple, or incarcerated intra-articular loose bodies, especially in olecranon fossa/trochlear notch. | Direct visualization for complete removal. | Smaller, fewer loose bodies may be managed arthroscopically. |
| Arthroplasty | Primary or revision total elbow arthroplasty, complex hemiarthroplasty. | Facilitates implant removal, bone preparation, and precise component insertion. | Only specific circumstances require this level of exposure for arthroplasty. |
| Joint Debridement/Synovectomy | Extensive synovial chondromatosis, severe inflammatory arthropathy requiring comprehensive debridement. | Full access to all joint compartments. | Less extensive disease may be managed arthroscopically or with limited approaches. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical steps to ensure a safe and efficient surgical procedure, minimize complications, and optimize exposure.
Pre-Operative Planning
-
Imaging Review:
- Standard Radiographs: AP, lateral, and oblique views of the elbow are essential.
- Computed Tomography (CT) Scans: Crucial for complex intra-articular fractures and nonunions. CT with 3D reconstructions provides invaluable insights into fracture patterns, articular comminution, fragment displacement, and bone loss, aiding in pre-operative templating.
- MRI: May be considered for soft tissue pathologies, ligamentous injuries, or avascular necrosis, though less commonly for the primary indication of an olecranon osteotomy approach.
- Templating: Use radiographs and CT scans to template implant size, configuration (e.g., plate length and contour), screw trajectories, and osteotomy location. Consider the need for bone grafting material (allograft or autograft).
- Implant Selection: Have a comprehensive array of plates (precontoured distal humerus specific plates, reconstruction plates), screws (cortex, lag), K-wires, and cerclage wire for both the primary pathology and the olecranon osteotomy fixation. A tension band wiring set and potentially an olecranon plating system should be available.
- Ulnar Nerve Considerations: Plan for prophylactic ulnar nerve anterior transposition if there is pre-existing neuropathy, significant instability of the nerve, or if extensive hardware will be placed in close proximity.
- Patient Education: While strictly doctor-to-doctor, it's important to be aware of the patient's understanding of potential complications, including the risk of olecranon nonunion or ulnar nerve issues.
Patient Positioning
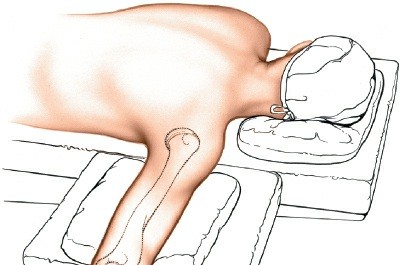
The position of the patient significantly influences surgical access, ergonomic comfort for the surgeon, and anesthetic management. The prone position is frequently favored for the posterior approach due to excellent exposure and simplified draping.
- Anesthesia and Exsanguination: The patient is intubated and general anesthesia is induced. The limb is exsanguinated by elevating it for 3 to 5 minutes, followed by the application of a pneumatic tourniquet as high up on the arm as possible (typically on the proximal humerus). The tourniquet pressure is set according to institutional protocol, typically 100 mmHg above systolic blood pressure.
-
Prone Position:
- Place the intubated patient prone on the operating table.
- Ensure adequate padding for the chest and pelvis to allow free movement of the abdomen during respiration and minimize pressure points.
- Abduct the ipsilateral arm approximately 90 degrees from the torso.
- Place a small sandbag or padded support underneath the proximal upper arm, just distal to the tourniquet, elevating the upper arm from the operating table. This maneuver allows the elbow to flex freely.
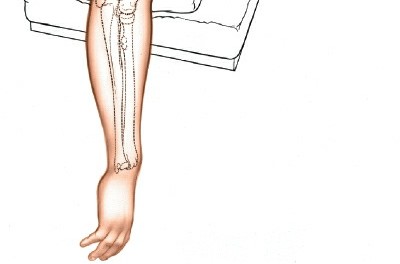
- Allow the elbow to flex, and the forearm to hang over the side of the table or be supported by an arm rest or bolster, ensuring maximum flexion. This position provides gravitational distraction of the joint, facilitates a straight posterior incision, and allows dynamic assessment of reduction and range of motion.
- Careful padding of all pressure points, especially the contralateral arm, face, and knees, is essential. The ulnar nerve in the contralateral elbow must be protected.
-
 - Alternative Positioning: While prone is standard, some surgeons prefer the lateral decubitus position with the arm draped over a bolster, or the supine position with the arm crossed over the chest and supported by a specific arm holder (e.g., a "cantilevered" arm table). These alternatives may be used based on surgeon preference or specific patient co-morbidities. However, the prone position generally offers superior and reproducible access.
-
Draping: The arm is sterilely prepped and draped from the mid-humerus to the hand, allowing full visualization and manipulation of the elbow and forearm.
Detailed Surgical Approach / Technique
The execution of the posterior approach with olecranon osteotomy demands precision and an understanding of the sequential steps to achieve optimal exposure while minimizing iatrogenic injury.
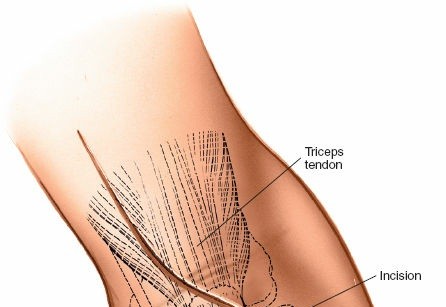
1. Skin Incision
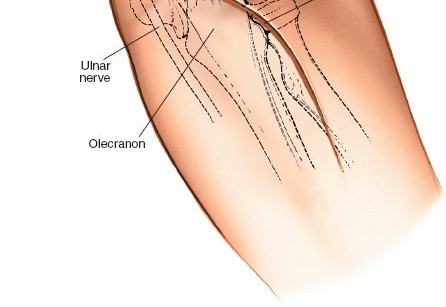
- A straight longitudinal posterior incision is made, centered over the olecranon and extending proximally along the triceps aponeurosis and distally along the subcutaneous border of the ulna. The length of the incision depends on the extent of the pathology, typically 10-15 cm.
-
2. Superficial Dissection and Ulnar Nerve Identification
- The incision is deepened through the skin and subcutaneous tissue. Subcutaneous flaps are carefully raised, minimizing injury to the posterior cutaneous nerve of the forearm.
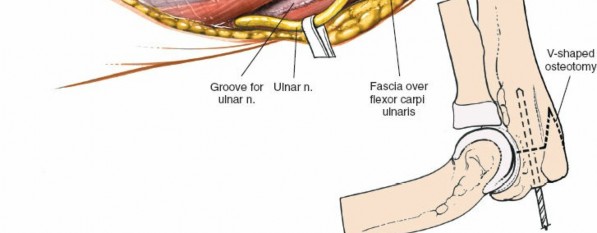
- The medial aspect of the incision is carefully dissected to identify the ulnar nerve. The nerve is typically found in the cubital tunnel posterior to the medial epicondyle, running between the two heads of the flexor carpi ulnaris (FCU).
- The ulnar nerve is meticulously dissected free from its surrounding fascial attachments, gently mobilized, and protected throughout the procedure. Depending on the pathology, planned hardware placement, or if there is pre-existing neuropathy, the nerve may be transposed anteriorly. This typically involves incising the fascia of the cubital tunnel and detaching the humeral head of the FCU, then relocating the nerve anterior to the medial epicondyle.
-

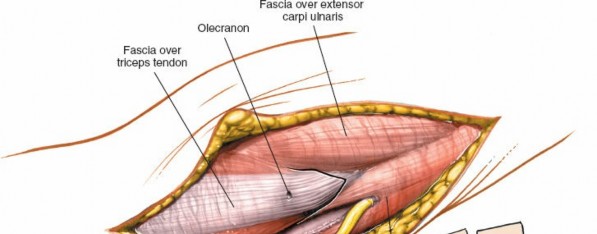
3. Exposure of Triceps and Olecranon
- Once the ulnar nerve is protected, the triceps tendon and aponeurosis are exposed.
- The triceps can be managed in several ways to expose the distal humerus, but for an olecranon osteotomy, the triceps is left attached to the osteotomized fragment.
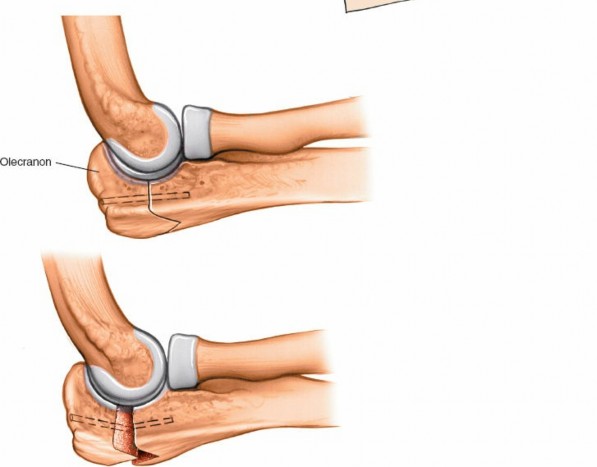
4. Olecranon Osteotomy
The olecranon osteotomy is the defining step of this approach, providing extensive intra-articular exposure. The type of osteotomy chosen (transverse, oblique, or chevron) depends on surgeon preference, bone quality, and fracture pattern. A chevron osteotomy is often preferred due to its inherent rotational stability upon reduction.
-
Planning the Osteotomy:
- The osteotomy should be carefully planned to be distal to the tip of the olecranon, preserving enough bone proximally for robust fixation of the fragment.
- It should also be distal to the articular cartilage of the trochlear notch but proximal to the coronoid process, avoiding injury to the trochlear notch and ensuring a good bone-to-bone contact surface for healing.
- The apex of a chevron osteotomy should typically point distally.
- Pre-drilling for fixation wires or screws (e.g., K-wires for tension band wiring) can be performed prior to the osteotomy to facilitate accurate placement later.
-
-
Performing the Osteotomy:
- Using a fine oscillating saw, the osteotomy is carefully performed. Constant irrigation is crucial to prevent thermal necrosis of the bone.
- Protect the articular cartilage of the olecranon fossa anteriorly with a broad retractor or elevator.
- The cut should be complete, ensuring the fragment can be freely mobilized.
-
-
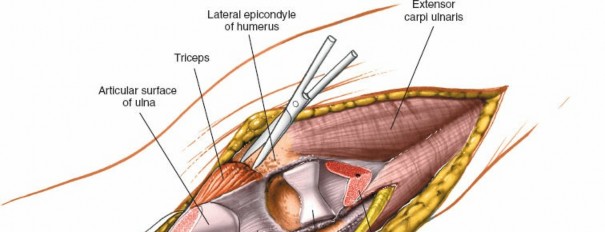
Reflection of the Olecranon Fragment:
- Once the osteotomy is complete, the proximal olecranon fragment, with the attached triceps tendon, is gently reflected proximally, hinged on the remaining soft tissues of the triceps. This provides an excellent view of the posterior distal humerus, the olecranon fossa, and the articular surfaces of the trochlea and capitellum.
- Retractors are carefully placed to maintain the exposure without compromising the ulnar nerve or other neurovascular structures.
-
 -

5. Addressing the Primary Pathology
With the elbow joint now widely exposed, the surgeon can address the primary pathology:
*
Fracture Reduction:
Identify and reduce articular fragments of the distal humerus first, using K-wires for temporary fixation. Restore the trochlear articular surface meticulously. Reconstruct the medial and lateral columns.
*
Internal Fixation:
Apply appropriate implants (e.g., dual plating for distal humeral fractures, often 90-degree divergent plates) to achieve stable internal fixation, restoring the anatomy and allowing for early mobilization.
*
Loose Body Removal:
Directly visualize and remove any loose bodies.
*
Debridement/Nonunion Repair:
Perform debridement of nonunion sites, apply bone graft, and stabilize.
6. Olecranon Osteotomy Fixation
Once the primary pathology is addressed and stable, the olecranon fragment is carefully reduced back into its anatomical position. The stability of this fixation is paramount for functional recovery.
-
Techniques:
- Tension Band Wiring (TBW): Often used for simple, non-comminuted osteotomies. Two parallel K-wires are inserted from the tip of the olecranon, crossing the osteotomy site and engaging the anterior cortex of the ulna. A figure-of-eight stainless steel wire is then passed through a transverse drill hole in the ulnar shaft distal to the osteotomy and around the posterior aspects of the K-wires. This converts the tensile forces of the triceps into compressive forces at the osteotomy site.
- Intramedullary Screw: A large cancellous screw can be inserted from the tip of the olecranon across the osteotomy site, engaging the anterior cortex.
- Plate Fixation: A small contoured plate (e.g., an olecranon plate or 1/3 tubular plate) applied to the posterior surface of the olecranon offers robust fixation, especially for comminuted osteotomies, osteoporotic bone, or as an adjunct to TBW. Screws are placed across the osteotomy site.
- Verification: Ensure anatomical reduction of the olecranon fragment, particularly its articular surface. Check stability through a full range of elbow motion. Avoid prominent hardware.
-
 -

7. Closure
- Perform a thorough irrigation of the joint and wound.
- Confirm hemostasis.
- If performed, ensure the ulnar nerve is lying free in its transposed position or protected from direct contact with hardware.
- Close the deep fascia and subcutaneous layers with absorbable sutures.
- A drain may be placed if significant dead space or anticipated bleeding is present.
- Close the skin with staples or non-absorbable sutures.
-
 - Apply a sterile dressing, often followed by a posterior splint or hinged elbow brace, depending on the stability of the fixation and the specific rehabilitation protocol.
-
 -
 -
(This image typically represents a post-operative radiograph, confirming fixation.)
Complications & Management
Despite meticulous technique, complications can arise following the posterior approach with olecranon osteotomy. Proactive recognition and appropriate management are crucial for salvage and optimizing patient outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Description | Salvage Strategies |
|---|---|---|---|
| Olecranon Nonunion/Malunion | 5-15% | Failure of the osteotomy to heal, leading to pain, weakness, and potentially loss of elbow extension. Malunion involves healing in a deformed position. Often due to inadequate fixation, poor bone quality, or premature aggressive rehabilitation. | Nonunion: Revision surgery with debridement of fibrous tissue, refresh bone ends, stable refixation (often with plate and screws, +/- tension band), and bone grafting (autograft or allograft). Malunion: Corrective osteotomy and refixation if symptomatic. |
| Ulnar Nerve Injury/Neuropathy | 5-20% | Can range from transient neurapraxia (due to traction/compression) to permanent axonotmesis or neurotmesis (due to direct transection or entrapment). Symptoms include numbness/tingling in the small finger and ulnar half of the ring finger, and motor weakness. | Transient: Observation, nerve gliding exercises, NSAIDs. Persistent Neuropathy: Electrodiagnostic studies. If severe or progressive, consider exploration and neurolysis, potentially with anterior transposition. If nerve transection, primary repair or nerve grafting if gap is too large. Revision of hardware if nerve irritation is due to prominent hardware. |
| Hardware Irritation/Prominence | 10-30% | Pain or discomfort over the olecranon due to prominent K-wires, cerclage wire, or plating, especially under the skin. Common given the superficial location of the olecranon. | Symptomatic hardware removal after osteotomy union (typically 6-12 months post-op). Careful planning during initial surgery to bury hardware as much as possible. |
| Infection (Superficial/Deep) | 1-5% | Infection of the surgical site, potentially leading to osteomyelitis, implant failure, and systemic complications. | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, thorough irrigation, intravenous antibiotics targeted to culture results. Consideration of implant removal (if fixation is stable or union achieved) or staged reconstruction. |
| Elbow Stiffness/Loss of Motion | 10-40% | Restricted range of motion (flexion/extension, pronation/supination). Can be due to periarticular scarring, heterotopic ossification, persistent intra-articular derangement, or inadequate rehabilitation. | Early, controlled mobilization post-op. If established: Intensive physical therapy, dynamic splinting. If conservative measures fail, consider surgical arthrolysis (open or arthroscopic), heterotopic ossification excision, or hardware removal (if contributing) after bony union. |
| Post-Traumatic Arthritis | Variable | Degenerative changes in the articular cartilage, often a long-term sequela of intra-articular fractures, especially if anatomical reduction was not achieved or if there was significant initial cartilage damage. | Early: Symptomatic management (NSAIDs, activity modification, injections). Advanced: Surgical options include arthroscopic debridement, osteotomies, interpositional arthroplasty, or ultimately total elbow arthroplasty (especially in older, lower-demand patients) or fusion in severe cases. |
| Heterotopic Ossification (HO) | 5-20% (clinically significant) | Abnormal bone formation in soft tissues around the joint, limiting motion. Risk factors include high-energy trauma, head injury, burns, and genetic predisposition. | Prophylaxis: NSAIDs (e.g., Indomethacin) or low-dose radiation post-op, especially in high-risk patients. If established and symptomatic: Surgical excision of HO, typically after it has matured (assess with bone scan or CT). Post-excision, consider further HO prophylaxis. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical determinant of functional outcome following the posterior approach with olecranon osteotomy. The protocol is tailored to the stability of the primary fixation and the olecranon osteotomy. The goal is to maximize functional range of motion while protecting the healing structures.
General Principles
- Pain Management: Adequate pain control is essential to allow participation in therapy.
- Wound Care: Meticulous wound care to prevent infection.
- Protection: The elbow is typically placed in a bulky soft dressing and a posterior splint immediately post-operatively, often in 30-45 degrees of flexion.
- Early Motion (Controlled): The trend is towards early, controlled motion to prevent stiffness, but only if fixation is deemed stable. This often requires close collaboration between the surgeon and physical therapist.
Phased Rehabilitation Protocol (Example - May Vary Based on Fixation Stability)
Phase I: Immediate Post-operative (Weeks 0-2)
- Goals: Reduce pain and swelling, protect surgical repair, initiate gentle range of motion (ROM).
-
Immobilization:
- Surgical dressing and posterior splint in 30-45 degrees of flexion.
- For highly stable fixation, a hinged elbow brace may be applied within the first few days, set to allow a restricted arc of motion (e.g., 30-90 degrees).
-
Exercises:
- Gentle Passive & Active-Assisted ROM: Flexion and extension within protected limits as tolerated. Gravity-assisted movements (e.g., allowing forearm to hang gently).
- Forearm Pronation/Supination: Gentle active-assisted.
- Hand/Wrist Exercises: Active ROM for fingers, thumb, and wrist to prevent stiffness and promote circulation.
- Shoulder Exercises: Active ROM for shoulder (pendulums, flexion, abduction) to prevent shoulder stiffness.
- Weight Bearing: Non-weight bearing for the involved extremity.
- Precautions: Avoid active resisted elbow extension to protect the healing triceps-olecranon complex. No lifting, pushing, or pulling.
Phase II: Early Motion & Strengthening (Weeks 2-6)
- Goals: Gradually increase active and passive ROM, begin gentle strengthening.
- Bracing: Continue hinged elbow brace, gradually increasing the allowable arc of motion (e.g., 10-120 degrees by week 6), as tolerated and dictated by fixation stability.
-
Exercises:
- Active-Assisted & Active ROM: Progressively increase elbow flexion and extension.
- Gentle Strengthening: Initiate isometric exercises for elbow flexors and extensors.
- Forearm Strengthening: Gentle active pronation/supination with light resistance.
- Scar Massage: Once sutures/staples are removed and wound is healed, gentle scar massage.
- Weight Bearing: Still non-weight bearing, but can progress to very light functional use (e.g., holding a cup) as comfort allows.
- Precautions: Continue to avoid heavy lifting or sudden, uncontrolled movements.
Phase III: Intermediate Strengthening & Functional Return (Weeks 6-12)
- Goals: Achieve near full pain-free ROM, progressive strengthening, prepare for return to light activities.
- Bracing: May discontinue brace for daily activities if stable and ROM is good, but may use for protection during activities or sleep.
-
Exercises:
- Full ROM: Work towards full active and passive ROM.
- Progressive Strengthening: Light weights, resistance bands for elbow flexion, extension, pronation, supination.
- Functional Activities: Begin integrating activities of daily living (ADLs) that require light lifting and controlled movements.
- Weight Bearing: Gradual progression to light weight bearing as pain allows.
- Precautions: Avoid activities that place excessive stress on the elbow, such as heavy lifting, throwing, or repetitive impact.
Phase IV: Advanced Strengthening & Return to Activity (Weeks 12+)
- Goals: Restore full strength and endurance, gradual return to sport/work-specific activities.
-
Exercises:
- Advanced Strengthening: Progressive resistance exercises, eccentric loading, plyometrics (if indicated for return to sport).
- Sport/Work-Specific Drills: Gradually introduce activities specific to the patient's occupation or sport.
- Return to Activity: Phased return to demanding activities. Full return to contact sports or heavy labor typically not before 4-6 months, and only after achieving satisfactory strength, ROM, and radiographic evidence of osteotomy union.
Important Note: This is a generalized protocol. Individualized adjustments are frequently necessary based on the specific fracture pattern, quality of fixation, patient factors, and the presence of any complications. Radiographic assessment of olecranon osteotomy union is crucial before advancing to unrestricted activity.
Summary of Key Literature / Guidelines
The posterior approach with olecranon osteotomy remains a fundamental technique in elbow surgery, with an extensive body of literature supporting its efficacy for complex pathologies. Key considerations from the literature emphasize careful surgical planning, meticulous execution, and dedicated rehabilitation.
-
Exposure and Visualization: Early studies and subsequent biomechanical analyses consistently highlight the superior intra-articular visualization afforded by the olecranon osteotomy, particularly for complex distal humeral fractures. Authors like Colton (1973) and Bryan and Morrey (1985) described the initial techniques and emphasized the importance of a well-executed osteotomy for access. Modern orthopedic texts universally endorse its use for achieving anatomical reduction in challenging cases.
-
Olecranon Osteotomy Fixation: The literature has evolved concerning optimal olecranon osteotomy fixation.
- Tension Band Wiring (TBW): Historically, TBW has been a popular and effective method, applying the tension band principle to convert triceps tensile forces into compressive forces. Studies have shown good to excellent union rates, though hardware prominence and migration remain common. Chapman et al. (1998) provided a comprehensive review of olecranon fracture fixation, including osteotomies.
- Plate Fixation: Biomechanical studies, such as those by Josefsson et al. (1990) and later by Schwartz et al. (2007) , have demonstrated that plate fixation, particularly precontoured olecranon-specific plates, can offer superior biomechanical stability compared to TBW, especially for comminuted osteotomies or in osteoporotic bone. This has led to an increased adoption of plates, either alone or in conjunction with intramedullary screws, for greater stability and potentially lower rates of symptomatic hardware requiring removal.
- Chevron vs. Transverse Osteotomy: While transverse osteotomies are simpler, the chevron osteotomy is often favored for its inherent rotational stability and larger surface area for healing, as supported by Holden et al. (1998) and others.
-
Ulnar Nerve Management: The vulnerability of the ulnar nerve is a recurrent theme in the literature.
- Prophylactic ulnar nerve anterior transposition is a debated topic. Some surgeons advocate for routine transposition, especially in cases of pre-existing neuropathy or if hardware is anticipated to be prominent. Others suggest that meticulous identification, mobilization, and protection are sufficient, with transposition reserved for specific indications. Studies by Morrey and Sanchez-Sotelo (2009) provide extensive discussion on this, highlighting that rates of ulnar neuropathy vary, and the decision often remains surgeon-dependent.
- Careful padding and positioning are critical to prevent traction or compression injuries.
-
Complication Rates: The literature consistently reports specific complication rates associated with this approach.
- Nonunion of the olecranon osteotomy (5-15%) remains a concern, prompting the evolution of fixation techniques.
- Symptomatic hardware requiring removal (10-30%) is the most common reason for secondary surgery, directly related to the superficial nature of the olecranon.
- Post-operative stiffness (10-40%) is a significant challenge, driving the emphasis on early, controlled rehabilitation protocols.
- Infection (1-5%) and heterotopic ossification (5-20%) are also recognized. Prophylaxis for HO with NSAIDs or radiation in high-risk patients is supported by evidence (e.g., Coventry et al., 1983 ).
-
Rehabilitation: The consensus in modern orthopedic practice is to initiate early, controlled range of motion post-operatively, as long as stable fixation of both the primary pathology and the osteotomy has been achieved. This strategy, supported by studies like Ring et al. (2003) , aims to minimize elbow stiffness, which is a major determinant of long-term functional outcome. Protocols are tailored to individual patient factors and the stability of the reconstruction.
In conclusion, the posterior approach with an olecranon osteotomy is a highly effective, yet demanding, surgical technique. Its successful application relies on a thorough understanding of elbow anatomy, meticulous surgical execution (especially regarding the osteotomy and ulnar nerve), robust fixation, and a well-structured, early mobilization rehabilitation program to mitigate potential complications and restore optimal elbow function. Continued advancements in implant design and surgical techniques aim to further improve patient outcomes and reduce morbidity associated with this powerful approach.
Clinical & Radiographic Imaging
You Might Also Like