Diagnostic Approach to Median Nerve Schwannoma: A Detailed Orthopedic Case Study
Key Takeaway
Median nerve schwannoma diagnosis involves progressive pain, paresthesia, and a palpable forearm mass, often with a positive Tinel's sign. Clinical examination reveals neurological deficits. MRI is key, demonstrating a characteristic 'target sign' on T2-weighted images and avid, heterogeneous post-contrast enhancement, confirming the nerve's involvement and guiding further management.
Solving Complex Orthopedic Oncology Cases: Schwannoma
Patient Presentation & History
A 48-year-old right-hand dominant male presented to the orthopedic oncology clinic with a chief complaint of progressive right forearm pain, paresthesia, and a palpable mass. The patient reported an insidious onset of symptoms approximately 10 months prior to presentation. Initially, the pain was intermittent, described as a deep ache localized to the volar aspect of the distal forearm, occasionally radiating into the thumb, index, and middle fingers. Over the past 4 months, the pain had become constant, exacerbated by repetitive wrist movements and direct pressure on the mass. He also reported a subjective increase in numbness and tingling in the median nerve distribution, accompanied by a perceived decrease in grip strength and difficulty with fine motor tasks, such as buttoning shirts.
His past medical history was significant for well-controlled essential hypertension, managed with an ACE inhibitor, and mild osteoarthritis of the knees. There was no personal or family history of neurofibromatosis or other genetic syndromes predisposing to nerve sheath tumors. He denied any history of trauma to the affected limb, previous surgeries, or infections. He was a non-smoker and consumed alcohol socially. His occupational history involved prolonged desk work with extensive computer use, which he initially attributed his symptoms to, attempting self-management with ergonomic adjustments and over-the-counter NSAIDs, none of which provided significant relief. The progressive nature of his neurological symptoms, despite conservative measures, prompted his referral to our service.
Clinical Examination
Inspection:
On inspection of the right upper extremity, there was a subtle, localized fusiform fullness visible on the volar aspect of the distal forearm, approximately 8 cm proximal to the wrist crease, slightly radial to the midline. No skin discoloration, erythema, atrophy, or trophic changes were noted. The overall alignment of the limb appeared normal.
Palpation:
Palpation revealed a firm, well-circumscribed, ovoid mass, approximately 3 x 2 cm in size, situated deep within the flexor compartment of the forearm. The mass was mobile in a transverse plane but restricted longitudinally, consistent with a nerve sheath tumor. It was mildly tender to direct palpation. A positive Tinel's sign was elicited directly over the mass, producing electric-shock-like sensations radiating distally into the thumb, index, and middle fingers. There was no warmth or crepitus. Proximal and distal palpation of the median nerve revealed no additional masses or areas of tenderness.
Range of Motion (ROM):
Active and passive range of motion of the wrist, elbow, and shoulder were full and pain-free, although forceful resisted wrist flexion and forearm pronation marginally aggravated the deep forearm pain. Grip strength was subjectively reduced on the right side (4/5 compared to 5/5 on the left), and pinch strength was also mildly impaired.
Neurological Assessment:
*
Motor:
Manual muscle testing revealed mild weakness in muscles innervated by the median nerve distal to the lesion:
* Flexor pollicis longus (FPL): 4+/5
* Flexor digitorum profundus (FDP) to index and middle fingers: 4+/5
* Abductor pollicis brevis (APB): 4/5
* Opponens pollicis (OP): 4/5
* All other motor groups in the right upper extremity were 5/5.
* Mild thenar atrophy was noted on the right compared to the left.
*
Sensory:
Diminished sensation to light touch and pinprick was observed in the palmar aspect of the thumb, index, middle fingers, and the radial half of the ring finger, as well as the distal palmar crease, consistent with median nerve involvement. Two-point discrimination was impaired at 7mm on the right index fingertip (normal <6mm) compared to 4mm on the left.
*
Reflexes:
Biceps and triceps reflexes were 2+ bilaterally and symmetrical. The brachioradialis reflex was also 2+ bilaterally.
Vascular Assessment:
Radial and ulnar pulses were bilaterally palpable, strong, and symmetrical. Capillary refill was brisk in all digits. No evidence of vascular compromise or bruits was noted.
Imaging & Diagnostics
Plain Radiographs:
Anteroposterior and lateral radiographs of the right forearm and wrist were obtained. These revealed no evidence of osseous abnormalities, periosteal reaction, cortical erosion, or calcification. Soft tissue swelling was subtly evident in the area corresponding to the palpable mass. The radiographs served primarily to rule out bony pathology and were otherwise unremarkable.
Ultrasound:
Initial ultrasound examination of the forearm demonstrated a well-circumscribed, hypoechoic, ovoid mass measuring approximately 3.1 x 2.0 x 1.8 cm, located deep to the flexor digitorum superficialis and closely associated with the median nerve. Color Doppler imaging showed internal vascularity. The ultrasound confirmed the presence and location of the mass and its intimate relationship with the median nerve.
Magnetic Resonance Imaging (MRI):
A dedicated MRI of the right forearm was performed with intravenous contrast, which proved to be the most informative diagnostic tool.
*
T1-weighted images:
The mass appeared largely isointense to hypointense relative to muscle.
*
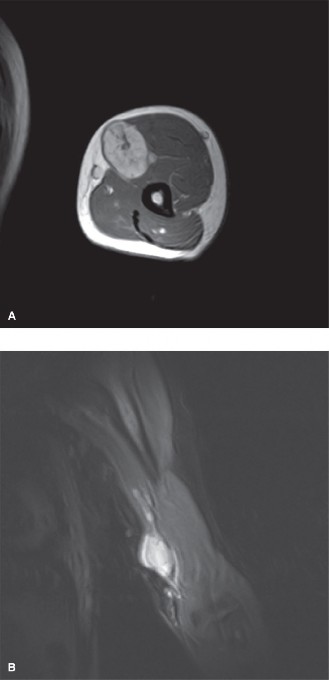
T2-weighted images:
Demonstrated a heterogeneous signal, predominantly hyperintense with areas of cystic degeneration and hemorrhage. A classic "target sign" was evident, characterized by a central low signal intensity area (collagenous stroma) surrounded by a peripheral high signal intensity rim (myxoid changes and looser cellular areas).
*
Post-contrast T1-weighted images with fat suppression:
Showed avid, heterogeneous enhancement of the mass, with a non-enhancing central component corresponding to the cystic areas. The median nerve was clearly seen entering and exiting the tumor capsule, indicating an intraneural or eccentric epineurial location. The tumor appeared well-encapsulated with clear margins from surrounding soft tissues, though its intimate association with the nerve fascicles was highlighted. There was no evidence of aggressive features such as extraneural infiltration, periosteal reaction, or significant surrounding edema. The estimated volume of the tumor was approximately 5.6 cm³.
Figure 1: Pre-operative axial T2-weighted MRI demonstrating the well-circumscribed, hyperintense mass (arrow) within the median nerve, consistent with a schwannoma.
Nerve Conduction Studies (NCS) and Electromyography (EMG):
These studies were performed to objectively assess the degree of median nerve compression and rule out other causes of neuropathy. NCS revealed prolonged distal motor latency and reduced amplitude of the compound muscle action potentials (CMAPs) recorded from the abductor pollicis brevis, consistent with focal demyelination and axonal loss at the level of the mass. Sensory nerve action potentials (SNAPs) of the median nerve were also reduced. EMG showed fibrillation potentials and positive sharp waves in the abductor pollicis brevis, opponens pollicis, and flexor pollicis longus, indicating active denervation, along with signs of chronic reinnervation (increased duration and amplitude of motor unit potentials). These findings confirmed a severe focal median mononeuropathy at the level of the mass.
Biopsy:
Given the strong suspicion for a benign nerve sheath tumor (most likely schwannoma) based on clinical and radiological findings, and the desire to avoid potential nerve injury from a diagnostic incisional biopsy, a decision was made to proceed directly to excisional biopsy/resection under frozen section control. The primary goal was complete tumor removal while preserving nerve function.
Differential Diagnosis
A comprehensive differential diagnosis for a soft tissue mass with associated neurological symptoms in the forearm must consider various entities. The most pertinent differentials are compared below:
| Feature | Schwannoma (Neurilemoma) | Neurofibroma | Malignant Peripheral Nerve Sheath Tumor (MPNST) |
|---|---|---|---|
| Origin | Schwann cells, eccentric to nerve | Schwann cells, fibroblasts, perineurial cells, integrates with nerve fascicles | Schwann cells, fibroblasts, perineurial cells, dedifferentiated cells |
| Nature | Benign, encapsulated | Benign, unencapsulated (can be plexiform) | Malignant, aggressive |
| Association with NF | Usually sporadic; rarely seen in NF2 | Common in Neurofibromatosis Type 1 (NF1); can be sporadic | ~50% associated with NF1 |
| Symptoms | Pain, paresthesia, Tinnel's sign. Symptoms often provoked by pressure on the mass. Progressive neurological deficit. | Pain, paresthesia. Symptoms less often directly related to pressure on mass. Can be asymptomatic. | Rapidly growing mass, severe pain, progressive neurological deficit, often new or worsening. |
| Mobility | Mobile transversely, restricted longitudinally (Tinel's) | Mobile transversely, restricted longitudinally | Variable, often fixed, rapidly growing |
| MRI Features | Well-circumscribed, encapsulated. T2 hyperintense with heterogeneous signal. Target sign (central low, peripheral high T2). Fascicular sign. Avid, heterogeneous enhancement. Can have cystic changes. | Well-circumscribed but unencapsulated. T2 hyperintense. Target sign (central fibrous, peripheral myxoid). Less cystic change than schwannoma. | Ill-defined margins, infiltrative. Heterogeneous signal. Necrosis, hemorrhage. Rapid growth on serial imaging. Peritumoral edema. |
| Histology | Antoni A (dense, palisading nuclei, Verocay bodies) and Antoni B (loose, myxoid stroma) areas. S-100 positive. | Mix of Schwann cells, fibroblasts, mast cells, collagen. Bland nuclei. S-100 positive. | High cellularity, pleomorphism, mitotic activity, necrosis, infiltrative growth. Variable S-100 expression. |
| Surgical Approach | Intracapsular enucleation with nerve preservation. Easy dissection off nerve. | Difficult to enucleate from nerve fascicles; often requires partial nerve resection for complete removal, risking nerve deficit. | Wide en bloc resection with clear margins; often requires nerve sacrifice and reconstruction. Adjuvant therapy. |
| Prognosis | Excellent, low recurrence after complete excision. | Good, but risk of malignant transformation (5-10% in NF1). | Poor, high recurrence, high metastatic rate. |
Surgical Decision Making & Classification
The decision for operative intervention was straightforward in this case due to several compelling factors:
1.
Progressive Neurological Deficit:
The patient exhibited worsening pain, paresthesia, and objective motor weakness, indicating ongoing median nerve compression and axonal injury. Non-operative management would likely lead to irreversible nerve damage.
2.
Symptomatic Mass:
The mass was consistently painful and interfered with the patient's daily activities and occupational demands.
3.
Diagnostic Uncertainty:
While imaging was highly suggestive of a schwannoma, definitive histological diagnosis was required to rule out other benign or, less likely, malignant entities. Excisional biopsy offers the benefit of both diagnosis and treatment.
4.
Benign Tumor Characteristics:
MRI findings strongly suggested a benign, well-circumscribed nerve sheath tumor (target sign, fascicular sign, lack of aggressive features). Schwannomas are typically amenable to complete surgical excision without sacrificing the parent nerve.
Classification:
While there isn't a specific fracture classification applicable here, the Enneking Staging System for benign soft tissue tumors is relevant. The tumor in this case would be classified as
Stage 1 (Benign), Type 2 (Intracompartmental)
.
*
Stage 1:
Benign nature based on clinical behavior and imaging.
*
Type 2 (Intracompartmental):
The tumor was located within the median nerve sheath, confined within a well-defined fascial compartment (flexor compartment of the forearm), and did not extend beyond its capsule or into neurovascular bundles outside the nerve itself. This classification guides the surgical approach towards an intralesional or marginal excision, emphasizing preservation of critical structures.
The alternative to surgery, continued observation, was deemed inappropriate given the progressive neurological symptoms. Pain management, physical therapy, and steroid injections would address symptoms but not the underlying compressive pathology, making them temporizing at best.
Surgical Technique / Intervention
The primary surgical goal was complete enucleation of the schwannoma while meticulously preserving the integrity of the median nerve fascicles, thus preventing further neurological deficit and allowing for recovery of function.
Patient Positioning and Preparation:
The patient was positioned supine on the operating table. The entire right upper extremity was prepped and draped in a sterile fashion, allowing full mobility of the limb. A tourniquet was applied to the upper arm, but not inflated initially, to allow for assessment of vascularity and identification of the tumor prior to creating a bloodless field if necessary. A sterile arm board was used to support the limb in a comfortably abducted position, with the forearm supinated.
Surgical Approach:
A longitudinal curvilinear incision, approximately 6 cm in length, was marked on the volar aspect of the distal forearm, centered directly over the palpable mass and guided by pre-operative MRI localization. The incision was made just ulnar to the predicted course of the median nerve to facilitate later dissection and provide good exposure.
Subcutaneous tissues were incised, and meticulous hemostasis was achieved. The deep fascia of the forearm was then incised longitudinally. The flexor carpi radialis and palmaris longus tendons were retracted ulnarly, and the flexor digitorum superficialis was gently retracted radially, exposing the underlying median nerve.
Identification and Dissection of the Median Nerve and Tumor:
Under magnification (using surgical loupes 3.5x), the median nerve was carefully identified. It appeared thickened and fusiformly enlarged at the site of the mass. Proximally and distally to the mass, the nerve appeared normal. The epineurium overlying the tumor was often thin and translucent, allowing visualization of the tumor beneath.
A nerve stimulator was used to confirm nerve viability and to identify motor fascicles, particularly those supplying the thenar musculature, which were often displaced by the tumor. Fine micro-dissection instruments were employed to carefully open the epineurium longitudinally over the most superficial aspect of the tumor, approximately 1-2 cm on either side of the visible mass.
Intracapsular Enucleation:
Schwannomas typically displace nerve fascicles to one side, or they arise from a single fascicle, making intracapsular enucleation feasible. The tumor capsule was carefully identified, and a plane of dissection was established between the tumor and the surrounding nerve fascicles. This is a critical step, requiring patience and meticulous technique. The tumor was gently mobilized using a combination of blunt and sharp micro-dissection.
The median nerve fascicles were seen splayed around the tumor capsule. The goal was to peel the tumor away from these fascicles without compromising their integrity. Small feeding vessels entering the tumor were coagulated with bipolar cautery. The pseudocapsule of the schwannoma, which is distinct from the epineurium, was meticulously dissected.
Once the tumor was largely free, its origin from the nerve was identified. In this case, the tumor arose eccentrically from a small branch or fascicle of the median nerve. This fascicle was sharply divided at the points where it entered and exited the tumor, effectively freeing the schwannoma from the main nerve trunk. This partial fascicular sacrifice is often necessary for complete tumor removal and typically results in minimal functional deficit if the parent nerve's main fascicles are preserved.
The tumor was then completely excised. The specimen was oriented and sent for histopathological analysis, including frozen section, which confirmed a benign schwannoma. The remaining nerve fascicles appeared healthy and intact. A small amount of absorbable hemostatic agent (e.g., Gelfoam) was placed in the tumor bed for local hemostasis. The integrity of the remaining nerve was confirmed, and there was no tension.

Figure 2: Intraoperative view after intracapsular enucleation of the schwannoma (removed specimen shown), demonstrating the preserved splayed median nerve fascicles.
Closure:
The epineurium was gently coapted with a few interrupted 8-0 non-absorbable sutures to provide mild support, without tension. The deep fascia was closed with absorbable sutures. Subcutaneous tissues were approximated, and the skin was closed with a running subcuticular suture, followed by sterile dressings. A bulky soft dressing and a removable wrist splint in a neutral position were applied to protect the surgical site and minimize tension on the nerve.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Days 0-7):
*
Immobilization:
The patient was maintained in a neutral wrist splint to minimize tension on the median nerve repair site and facilitate wound healing. This was primarily for comfort and protection.
*
Pain Management:
Multimodal analgesia, including NSAIDs, acetaminophen, and short-term oral opioids as needed.
*
Wound Care:
Regular dressing changes. Instructions on monitoring for signs of infection (erythema, swelling, discharge).
*
Neurovascular Monitoring:
Close monitoring of digital perfusion, sensation, and motor function.
*
Elevation:
Limb elevation to minimize swelling.
*
Gentle Finger ROM:
Patients were encouraged to perform gentle active range of motion of the fingers (flexion and extension) to prevent stiffness, but instructed to avoid excessive wrist motion.
Early Rehabilitation (Weeks 1-6):
*
Splint Removal:
The removable splint was typically used for 2-3 weeks, primarily at night and for protection during activities. During the day, gentle, active wrist range of motion was initiated.
*
Physical Therapy:
Referral to hand therapy for a structured rehabilitation program.
*
Nerve Glides:
Gentle median nerve gliding exercises were introduced to promote nerve mobility and prevent adhesions, once the wound was well-healed and pain permitted.
*
Progressive ROM:
Gradual progression of active and passive wrist ROM, elbow, and forearm rotation.
*
Desensitization:
If significant post-operative dysesthesia or hypersensitivity was present, desensitization techniques were employed.
*
Edema Control:
Compression gloves or massage for persistent swelling.
*
Activity Modification:
Avoid heavy lifting, gripping, or sustained pressure on the surgical site.
Intermediate to Late Rehabilitation (Weeks 6-12+):
*
Strengthening:
Once full, pain-free ROM was achieved, progressive strengthening exercises for the wrist and hand musculature were initiated, targeting the median nerve innervated muscles (e.g., thenar eminence).
*
Functional Training:
Return to activities of daily living (ADLs) and work-specific tasks. Ergonomic assessment and modification if relevant.
*
Sensory Re-education:
For persistent sensory deficits, sensory re-education programs were implemented.
*
Follow-up:
Regular clinical follow-ups at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year post-operatively to assess neurological recovery, monitor for recurrence (rare for benign schwannoma), and address any ongoing symptoms. MRI surveillance is typically not indicated for completely excised benign schwannomas unless new symptoms arise.
The patient in this case demonstrated gradual but significant improvement. By 3 months post-operatively, his pain had resolved, and sensation in the median nerve distribution was markedly improved, with only mild residual hypesthesia in the index fingertip. Grip and pinch strength returned to near pre-morbid levels, and the patient was able to return to his full work duties without restriction.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
1.
High Index of Suspicion:
For any deep-seated soft tissue mass in an extremity, especially if associated with pain, paresthesia, and a positive Tinel's sign, a nerve sheath tumor must be high on the differential.
2.
MRI is King:
MRI with and without contrast is indispensable. Look for the classic "target sign" on T2-weighted images and the "fascicular sign" (nerve fascicles splayed around the lesion) which are highly suggestive of a benign nerve sheath tumor. It also defines the tumor's exact relationship to the parent nerve and surrounding structures, crucial for surgical planning.
3.
NCS/EMG for Objective Neuropathy:
These studies confirm the presence and severity of neuropathy, helping to quantify deficits and distinguish from other causes of nerve compression. They also serve as a baseline for post-operative comparison.
4.
Intracapsular Enucleation for Schwannoma:
The hallmark of schwannoma excision is careful intracapsular enucleation. Schwannomas typically displace nerve fascicles rather than incorporate them, allowing for complete removal with minimal or no sacrifice of the main nerve trunk. This is a key distinguishing feature from neurofibromas.
5.
Microsurgical Technique:
Use of surgical loupes (3.5x minimum) or an operating microscope is paramount for meticulous dissection, fascicle preservation, and achievement of a clean plane between the tumor and the nerve.
6.
Nerve Stimulator:
Intraoperative nerve stimulators are invaluable for identifying functional nerve fascicles, especially in areas where anatomical distortion is significant.
7.
Histopathological Confirmation:
Always send the specimen for definitive histology. Frozen section can confirm benignity and guide the extent of resection intraoperatively, especially if there is any ambiguity.
Pitfalls:
1.
Misdiagnosis as Carpal Tunnel Syndrome:
Early symptoms of a distal forearm schwannoma may mimic carpal tunnel syndrome, leading to delayed diagnosis or inappropriate initial management (e.g., carpal tunnel release without addressing the tumor). A detailed neurological exam and imaging are key to differentiation.
2.
Inadequate Imaging:
Relying solely on X-rays or basic ultrasound can miss the critical details provided by MRI regarding tumor morphology and its relationship to the nerve, leading to suboptimal surgical planning.
3.
Aggressive Resection Leading to Nerve Injury:
Misidentifying a schwannoma as a neurofibroma (which often requires fascicle sacrifice) or failing to appreciate the plane of dissection can lead to inadvertent sacrifice of important nerve fascicles and permanent neurological deficit.
4.
Incomplete Resection:
Though rare for schwannomas due to their encapsulation, incomplete removal can lead to recurrence and persistent symptoms.
5.
Confusing Schwannoma with Neurofibroma:
While both are benign nerve sheath tumors, their surgical management differs significantly. Neurofibromas are unencapsulated and often infiltrate nerve fascicles, making complete removal without fascicle sacrifice very difficult, frequently necessitating partial nerve resection. Pre-operative MRI characteristics and intraoperative findings are crucial for differentiation.
6.
Missing Malignant Transformation:
Although rare, especially in sporadic schwannomas, the possibility of a malignant peripheral nerve sheath tumor (MPNST) should always be considered, particularly with rapid growth, severe pain, or aggressive features on imaging. MPNSTs require wide en bloc resection, often with nerve sacrifice and adjuvant therapy.
7.
Post-operative Adhesions:
Inadequate post-operative nerve gliding and early mobilization can lead to adhesions around the nerve, causing persistent pain or limiting recovery.
You Might Also Like