Proximal Humerus Lateral Approach: Comprehensive Guide to Anatomy & Surgical Technique
Key Takeaway
The proximal humerus lateral approach, or deltoid-splitting approach, offers direct access to the greater tuberosity and surgical neck for managing displaced fractures. Critical considerations include precise anatomical knowledge, especially the axillary nerve's location, to prevent deltoid paralysis and restore function, minimizing risks like avascular necrosis.
Proximal Humerus Lateral Approach: Unlock Surgical Precision
Introduction & Epidemiology
Proximal humerus fractures represent a significant burden on orthopedic trauma services, accounting for approximately 5-6% of all fractures and 45% of all humeral fractures. Their incidence peaks in two distinct populations: younger, active individuals involved in high-energy trauma, and elderly patients, predominantly postmenopausal women, who sustain low-energy falls secondary to osteoporosis. The surgical management of these fractures is complex, given the intricate anatomy, variable fracture patterns, and potential for significant functional impairment. While non-operative treatment remains viable for many stable, minimally displaced fractures, surgical intervention is often indicated for displaced or unstable patterns to restore anatomy, preserve function, and prevent complications such as malunion, nonunion, or avascular necrosis (AVN).
The lateral approach to the proximal humerus, often colloquially referred to as the deltoid-splitting approach, offers direct access to the greater tuberosity and surgical neck, making it a valuable tool in the armamentarium of an orthopedic surgeon. Historically, its application was more limited due to concerns regarding axillary nerve injury and restricted visualization. However, advancements in surgical technique, anatomical understanding, and implant design have expanded its utility, particularly with the advent of percutaneous or minimally invasive techniques that leverage the principles of this approach. This detailed review will delineate the anatomical considerations, indications, technical nuances, potential complications, and rehabilitation strategies associated with the lateral approach, providing a comprehensive guide for orthopedic surgeons, residents, and medical students.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective utilization of the lateral approach.
Bony Anatomy
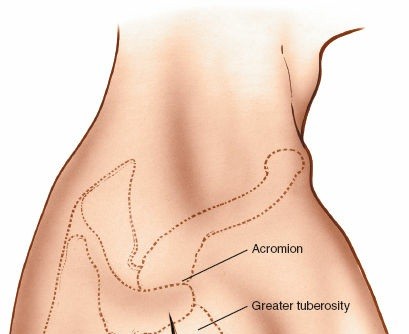
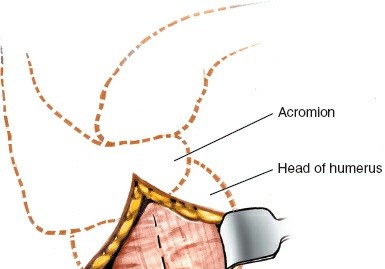
The proximal humerus comprises four key anatomical parts as per Neer's classification: the humeral head, greater tuberosity, lesser tuberosity, and surgical neck. The anatomical neck lies superior to the tuberosities, defining the articular surface. The surgical neck, distal to the tuberosities, is a common site for fracture. The greater tuberosity serves as the insertion site for the supraspinatus, infraspinatus, and teres minor tendons, while the lesser tuberosity accepts the subscapularis tendon. The bicipital groove separates the tuberosities anteriorly, housing the long head of the biceps tendon.
Neurovascular Structures
The most critical structure at risk during a lateral approach is the
axillary nerve
. This nerve originates from the posterior cord of the brachial plexus (C5-C6), courses inferior to the glenohumeral joint, passes through the quadrangular space, and then wraps around the surgical neck of the humerus. It typically lies approximately 5-7 cm distal to the lateral acromion, entering the deep surface of the deltoid muscle. It innervates the deltoid and teres minor muscles and provides sensory supply to the lateral shoulder via the superior lateral cutaneous nerve of the arm. Damage to the axillary nerve can lead to deltoid paralysis, significant abduction weakness, and sensory deficits.
The
radial nerve
courses posteriorly and obliquely across the humerus in the spiral groove, typically distal to the area of the surgical approach but can be at risk with extensive distal dissection or with intramedullary nailing.
The primary arterial supply to the humeral head is from branches of the
anterior and posterior circumflex humeral arteries
. The posterior circumflex humeral artery, often accompanying the axillary nerve, is the dominant blood supply. Its ascending branch gives rise to the arcuate artery, which penetrates the humeral head. Compromise of this blood supply, particularly in complex fractures involving displacement of the medial calcar or multifragmentary patterns, significantly increases the risk of avascular necrosis.
Muscular Anatomy
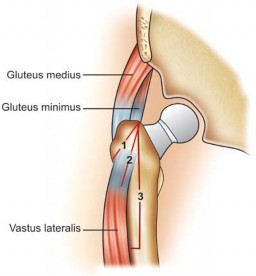
The
deltoid muscle
forms the bulk of the shoulder contour and is the primary muscle encountered in this approach. It originates from the lateral clavicle, acromion, and spine of the scapula, inserting into the deltoid tuberosity on the lateral aspect of the humerus. The deltoid is composed of anterior, middle (acromial), and posterior fibers. The lateral approach typically utilizes a split in the anterior-to-middle or purely middle deltoid fibers. This split must respect the axillary nerve. Generally, a safe deltoid split extends no more than 5 cm distally from the lateral acromion to avoid injury to the axillary nerve, which enters the deep surface of the deltoid at this level or slightly more distally. Extending the split beyond this point without direct visualization and protection of the nerve is hazardous.
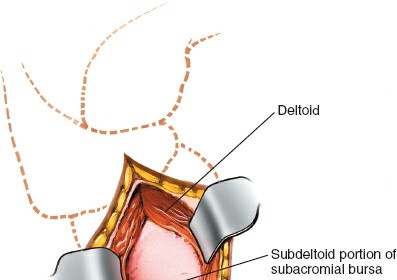
Deep to the deltoid lie the
rotator cuff muscles
: supraspinatus, infraspinatus, teres minor, and subscapularis. The supraspinatus and infraspinatus tendons insert onto the greater tuberosity and are often exposed or can be directly addressed via the lateral approach, particularly for repairs or calcific deposit removal.
Biomechanics
The stability of the proximal humerus is governed by a combination of bony architecture, ligamentous restraints (capsule, glenohumeral ligaments), and the dynamic compression of the rotator cuff muscles. In the context of fracture fixation, understanding the forces acting on the proximal humerus (deltoid pull, rotator cuff pull) is critical for stable implant placement. The metaphyseal bone of the proximal humerus is often cancellous and osteoporotic, particularly in elderly patients, which can challenge implant purchase and stability. Fixation strategies via the lateral approach typically involve plates with multiple locking screws to create a stable construct, often aiming to engage the calcar fragment for medial support.
Indications & Contraindications
The lateral approach provides limited but direct access, making it suitable for specific pathologies. Its utility in fracture surgery is reserved for fractures of the surgical neck and tuberosities of the humerus. More complex or distal fractures may necessitate alternative approaches (e.g., anterior deltopectoral, anterolateral extensile, or minimally invasive variations).
Indications
The uses of the lateral approach include the following:
1.
Open reduction and internal fixation (ORIF) of displaced fractures of the greater tuberosity of the humerus:
Particularly those with significant displacement (>5 mm or >3 mm in young, active patients, or involving significant rotation) that impair rotator cuff function or impinge.
2.
Open reduction and internal fixation of humeral surgical neck fractures:
Especially two-part surgical neck fractures without significant comminution, where a plate can be applied laterally.
3.
Insertion of intramedullary nails into the humerus:
The lateral approach can serve as an entry point, particularly for retrograde nailing or antegrade nailing using a deltoid-splitting technique.
4.
Removal of calcific deposits from the subacromial bursa or rotator cuff:
Direct visualization and excision can be achieved.
5.
Repair of the supraspinatus tendon:
When isolated or part of a larger rotator cuff tear, especially if the tear is in the anterior or middle portion of the supraspinatus, or for debridement.
6.
Repair of the rotator cuff:
For isolated tears of the supraspinatus and/or infraspinatus where the lateral approach offers adequate exposure.
7.
Debridement of glenohumeral joint:
For conditions such as septic arthritis or synovial chondromatosis, when combined with arthroscopy or limited open exploration.
8.
Internal fixation of specific Neer 2-, 3-, and 4-part fractures:
This approach can be utilized for valgus-impacted fractures, some two-part surgical neck or greater tuberosity fractures, and certain three-part fractures where a PHILOS plate can be applied to buttress the tuberosity and stabilize the head-shaft junction. Minimal osteotomies or additional portals may be necessary for reduction.
Contraindications
- Severe comminution of the humeral head or surgical neck requiring extensive visualization: In such cases, a more extensile approach (e.g., deltopectoral) may be preferred to allow for direct reduction of multiple fragments and better access to the medial calcar.
- Significant vascular compromise: While not an absolute contraindication, if there's concern for vascular injury or the need for vascular repair, a different approach might be safer.
- Active infection: Local or systemic infection is a contraindication to elective surgical intervention.
- Poor soft tissue envelope: Pre-existing skin compromise, severe open injury, or extensive scarring may preclude this approach.
- Fractures extending significantly distal to the surgical neck: These are often better managed with an anterior deltopectoral approach to protect the radial nerve and provide better plate length.
- Irreparable axillary nerve damage prior to surgery.
Operative vs. Non-Operative Indications
| Condition | Operative Indications | Non-Operative Indications |
|---|---|---|
| Proximal Humerus Fractures | ||
| Greater Tuberosity Fractures |
- Displacement > 5 mm (or > 3 mm in active patients)
- Rotational malpositioning of the fragment - Impingement of the fragment under the acromion - Associated rotator cuff tear requiring repair |
- Minimally displaced (< 5 mm displacement)
- No significant rotational malposition - Absence of impingement - Stable fracture pattern - Low functional demand in elderly, frail patients |
| Surgical Neck Fractures (2-part) |
- Angulation > 45 degrees
- Translation > 1 cm - Displaced valgus-impacted fractures where reduction improves stability - Displaced humeral neck fractures with significant rotator cuff avulsion requiring reattachment |
- Minimally displaced or non-displaced
- Stable, impacted fractures (e.g., stable valgus-impacted) with acceptable alignment - High surgical risk in elderly, frail patients where functional outcome may not justify risks - Low functional demand |
| 3- and 4-part Proximal Humerus Fractures |
- Select cases (e.g., some 3-part involving greater tuberosity and surgical neck) where lateral plating can achieve stable reduction; often requires adjuncts (e.g., percutaneous screws, minimal capsulotomy for head reduction).
- Failed non-operative management with progressive displacement. |
- Significant comminution precluding stable fixation via lateral approach
- Severe osteoporosis (poor bone stock for fixation) - High risk for AVN (some 4-part fractures) where arthroplasty may be preferred - Patient comorbidities precluding surgery - Very elderly, low-demand patients where comfort and limited function are prioritized over anatomical reduction. |
| Rotator Cuff Tears |
- Full-thickness tears with significant functional impairment
- Partial-thickness tears unresponsive to non-operative treatment - Acute traumatic tears in younger, active patients - Tears associated with fracture (e.g., greater tuberosity avulsion) |
- Small, asymptomatic partial-thickness tears
- Full-thickness tears in very elderly, low-demand patients with minimal functional deficit - Failed prior attempts at repair (in some cases, although revision surgery might be considered) - Significant muscle atrophy and fatty infiltration rendering repair futile |
| Subacromial Impingement/Calcific Tendinitis |
- Chronic symptoms unresponsive to conservative management (NSAIDs, PT, injections)
- Large, symptomatic calcific deposits causing severe pain or mechanical symptoms - Associated with significant bursal inflammation or rotator cuff pathology necessitating debridement/repair |
- Acute or mild-to-moderate symptoms
- First-line treatment with conservative measures - Small, asymptomatic calcific deposits - Patients with significant medical comorbidities precluding surgery |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to anticipate potential challenges and optimize surgical outcomes.
Pre-Operative Planning
-
Imaging:
- Standard Radiographs: True AP, scapular Y, and axillary views are crucial for initial assessment of fracture pattern, displacement, and comminution.
- Computed Tomography (CT) Scan with 3D Reconstructions: Indispensable for complex fracture patterns (3- and 4-part, fracture-dislocations) to delineate fragment orientation, assess articular involvement, evaluate medial calcar integrity, and plan screw trajectories. It helps identify subtle tuberosity displacement and comminution.
- MRI: Rarely required acutely for fractures but can be useful for assessing associated soft tissue injuries (e.g., rotator cuff tears, biceps pathology) or avascular necrosis pre-operatively if suspected.
- Fracture Classification: Utilize Neer and/or AO/OTA classifications to accurately describe the fracture and guide treatment decisions.
- Implant Selection: Determine the appropriate implant (e.g., locking plate, tension band wires, intramedullary nail) based on fracture pattern, bone quality, and surgeon preference. For lateral plating, consider the plate length and screw trajectory options.
- Patient Optimization: Address any medical comorbidities, optimize nutrition, and discontinue antiplatelet/anticoagulant medications as appropriate. Prophylactic antibiotics should be administered pre-operatively.
- Informed Consent: Discuss the risks (nerve injury, infection, nonunion, AVN, stiffness, implant-related issues) and benefits of the procedure, as well as alternative treatments.
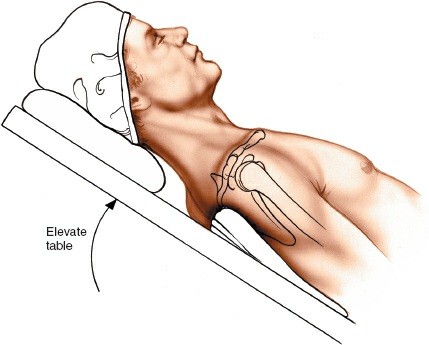
Patient Positioning
The patient is typically positioned in a
semi-recumbent (beach chair) position
or
supine position
on a radiolucent operating table.
*
Beach Chair Position:
* Provides excellent access to the shoulder and allows for easy manipulation of the arm in various planes.
* The head is secured in a headrest, ensuring neck alignment.
* The torso is elevated 30-45 degrees, which can reduce venous pressure and bleeding.
* The arm is draped free to allow for full range of motion, facilitating reduction maneuvers.
* A
sandbag
or bolster is often placed under the ipsilateral scapula to protract the shoulder girdle, optimizing access to the posterior and lateral aspects of the shoulder. This also ensures the scapula is elevated off the bed, preventing impingement during manipulation.
* An arm board can support the contralateral arm.
* Fluoroscopy equipment should be positioned to allow AP and lateral (axillary) views without repositioning.

*
Supine Position:
* Can also be used, with a bump placed under the ipsilateral scapula to elevate the shoulder.
* The arm is draped free for manipulation.
* May be preferred in cases requiring more extensive arm manipulation or in patients where beach chair positioning is contraindicated.
Prepping and Draping:
The entire upper extremity, from the sternum to the fingertips, is prepped with an antiseptic solution. The arm is then draped free, allowing full sterile manipulation during the case. Image intensifier should be draped to ensure sterile operation.
Detailed Surgical Approach / Technique
The lateral approach, while limited, offers direct access to the greater tuberosity and surgical neck. The key is to respect the deltoid muscle and its axillary nerve innervation.
Incision
-
Skin Incision: A straight or slightly curvilinear incision (typically 5-8 cm) is made centered over the lateral aspect of the acromion, extending distally along the line of the deltoid fibers.
- For greater tuberosity fractures or rotator cuff repair, the incision may be more posterior.
-
For surgical neck fractures or plate fixation, the incision will be more directly lateral, following the course of the deltoid.
- Minimally Invasive Extension: For an extended approach, an initial deltoid split may be performed followed by a more distal, separate deltoid split or interval distal to the axillary nerve, utilizing small incisions, potentially guided by fluoroscopy. This is typically for longer plates or IM nailing.
-
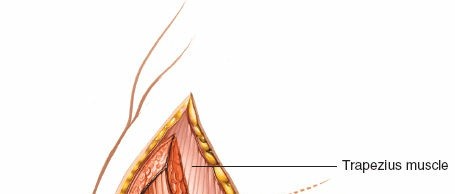
Subcutaneous Dissection: The incision is deepened through the subcutaneous tissues. Hemostasis is achieved. Careful dissection identifies the fascia overlying the deltoid muscle.
Deltoid Split & Internervous Plane
- Identify Deltoid Fibers: The deltoid muscle fibers are identified. The optimal split is typically through the middle or anterior part of the deltoid.
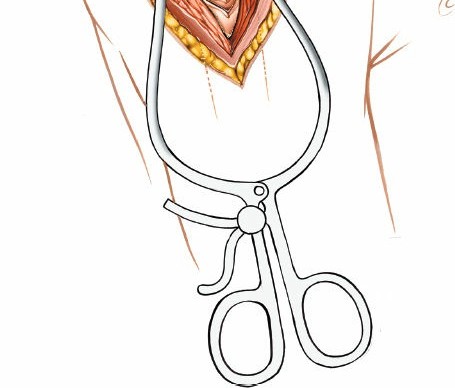
-
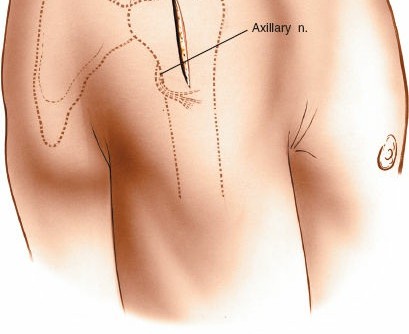
Deltoid Split:
The deltoid fibers are carefully split longitudinally. This split should not extend more than
5 cm distally from the lateral acromion
to protect the axillary nerve. A blunt instrument (e.g., finger, scissors) can be used to palpate the deep surface of the deltoid to ensure the split remains superficial to the nerve.
-
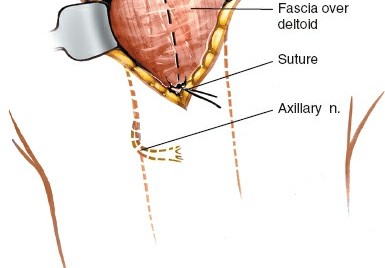
Axillary Nerve Protection:
Proximally, the nerve is relatively safe, but distally, it spirals around the humerus. Excessive retraction or a split exceeding 5 cm significantly increases the risk of injury. Some surgeons advocate for palpation of the nerve or even direct visualization if extension is required.
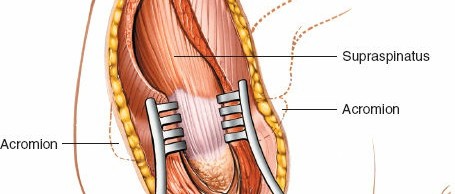
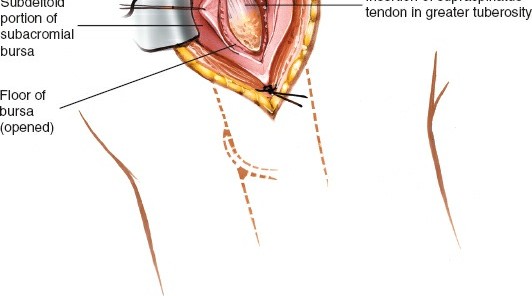
-
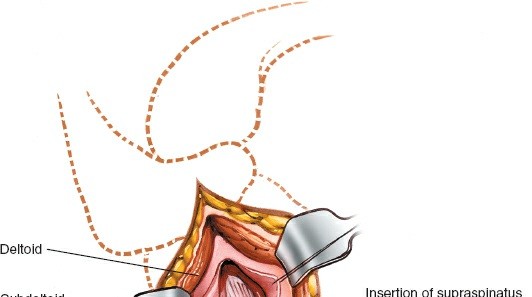
Exposure:
Once the deltoid is split, the underlying bursa, rotator cuff tendons (supraspinatus, infraspinatus), and the greater tuberosity become visible.

-
Axillary Nerve Protection:
Proximally, the nerve is relatively safe, but distally, it spirals around the humerus. Excessive retraction or a split exceeding 5 cm significantly increases the risk of injury. Some surgeons advocate for palpation of the nerve or even direct visualization if extension is required.
Fracture Reduction (Specific to Proximal Humerus Fractures)
- Hematoma Evacuation: The fracture hematoma is evacuated to improve visualization.
- Fragment Identification: Identify the humeral head, greater tuberosity, and surgical neck fragments.
-
Initial Reduction Maneuvers:
- Ligamentotaxis: Traction on the arm can help align the fragments.
- Direct Manipulation: Use blunt hooks, periosteal elevators, or bone clamps (e.g., Verbrugge, pointed reduction clamps) to directly reduce the fragments.
- Joy-sticks: K-wires can be inserted into the humeral head or tuberosity fragments to gain control and manipulate them into anatomical position.
- Valgus-Impacted Fractures: These often require disimpaction and reduction of the head from its varus position, sometimes needing a medial calcar reduction technique.
- Greater Tuberosity Fractures: Reduced by direct manipulation and often provisionally fixed with K-wires or suture loops. The rotator cuff insertion must be respected.
-
Provisional Fixation:
Once reduced, the fragments are provisionally secured with K-wires. Confirm reduction and K-wire placement with fluoroscopy (AP, lateral, and axillary views).
Internal Fixation (e.g., Locking Plate)
-
Plate Application:
A pre-contoured locking plate (e.g., PHILOS plate, LCP Proximal Humerus Plate) is typically chosen. The plate is positioned on the lateral aspect of the proximal humerus, generally 5-8 mm distal to the superior margin of the greater tuberosity to avoid impingement and allow for superior screw placement into the humeral head.
- Ensure the plate is centered on the humeral shaft distally.
- The plate should buttress the greater tuberosity, providing support and preventing varus collapse.
- Important: Avoid placing the plate too proximally, which can lead to subacromial impingement, or too anteriorly, risking biceps tendon irritation.
-
Screw Insertion:
- Shaft Screws: At least two to three bicortical locking screws are placed distally into the humeral shaft for stable fixation.
-
Head Screws:
Multiple unicortical or bicortical locking screws (typically 5-7) are inserted into the humeral head fragment. Aim for divergent trajectories to maximize bone purchase and create a "calcar screw" for medial support.
- Calcar Screws: One or two screws should be directed inferiorly and medially to engage the inferomedial cortex (calcar) of the humeral head. This provides crucial medial support and resists varus collapse, especially in osteoporotic bone.
-
Tuberosity Screws:
If a greater tuberosity fragment is present, screws are directed into it to secure its position and restore rotator cuff tension.
- K-wire removal: Once plate and screws are satisfactorily in place, the provisional K-wires are removed.
- Rotator Cuff Repair (if indicated): If the procedure is for rotator cuff repair or associated with a displaced tuberosity fracture, sutures are passed through the tendon and anchored to the humerus or to the plate itself, providing additional security.
-
Intramedullary Nailing (alternate fixation):
If an IM nail is used, the lateral approach can serve as an entry point for antegrade nailing or for exposing the surgical neck for retrograde nailing. The entry portal for antegrade nailing is typically through the rotator cuff, lateral to the biceps groove. The deltoid split allows for nail insertion and distal locking screw placement.
Final Assessment
- Fluoroscopy: Obtain final AP, lateral, and axillary fluoroscopic images to confirm anatomical reduction, correct plate and screw position, adequate screw length, and absence of intra-articular screw penetration. Perform a range of motion assessment under fluoroscopy to check for impingement or articular penetration.
- Range of Motion: Carefully assess shoulder range of motion to ensure no mechanical impingement of the plate and to assess the stability of the fixation.
Wound Closure
- Irrigation: Thorough irrigation of the surgical site.
- Deltoid Repair: The deltoid muscle split is loosely approximated with absorbable sutures, taking care not to overtighten and risk muscle ischemia or tethering.
- Subcutaneous and Skin Closure: The subcutaneous layer is closed with absorbable sutures, followed by skin closure with staples or non-absorbable sutures.
- Dressing: Apply a sterile dressing. A sling or shoulder immobilizer is typically applied for post-operative immobilization.
Complications & Management
Despite careful surgical technique, complications can occur following the lateral approach and internal fixation of proximal humerus fractures. Understanding these potential issues and their management is crucial.
| Complication | Incidence | Management Strategies |
|
NNerve Injury
|
Axillary Nerve:
1-10% (transient) to 0.5-2% (permanent)
Radial Nerve:
Rare (with lateral approach, more with direct fracture injury or distal extensive fixation) | -
Initial management:
Rest, observation, pain management.
-
Physiotherapy:
Nerve gliding exercises.
-
EMG/NCS:
At 3-6 weeks to assess denervation and prognosis.
-
Surgical exploration:
If no signs of recovery after 3-6 months (or earlier for suspected direct nerve laceration), considering neurolysis or nerve grafting.
-
Tendon transfers:
For chronic deficits with no recovery. |
|
Infection
| 1-5% (superficial or deep) | -
Superficial:
Oral antibiotics, local wound care.
-
Deep:
Surgical debridement, thorough irrigation, intravenous antibiotics (culture-specific), potentially implant removal (if nonunion or chronic infection) and staged reconstruction.
-
Prevention:
Meticulous sterile technique, prophylactic antibiotics. |
Clinical & Radiographic Imaging
You Might Also Like