Comprehensive Guide to the Direct Lateral Approach (DLA) for Hip Arthroplasty
Key Takeaway
The Direct Lateral Approach (DLA) is a foundational hip surgery technique, prioritizing adequate exposure while minimizing abductor damage. It's often used for total hip arthroplasty, aiming for early post-operative mobility and reduced dislocation risk. A thorough understanding of its anatomy, biomechanics, and indications is critical for successful patient outcomes and preserving crucial neurovascular structures.
Hip Lateral Approach: Surgical Technique for Early Patient Mobility
Introduction & Epidemiology
The direct lateral approach (DLA), often referred to as the modified Hardinge or transgluteal approach, represents a foundational surgical pathway to the hip joint. Its development was driven by the imperative to balance adequate surgical exposure with minimizing iatrogenic soft tissue damage, particularly to the abductor mechanism, thereby facilitating early post-operative mobilization and reducing dislocation risk. Historically, approaches to the hip have evolved from extensive and often morbid exposures, such as the Ollier or Kocher-Langenbeck for trauma, to more nuanced pathways optimized for total hip arthroplasty (THA).
The DLA gained prominence due to its perceived advantages in reducing posterior dislocation rates compared to the posterior approach, and its ability to preserve the anterior abductor musculature, differentiating it from true transgluteal approaches that involve a more significant split of the gluteus medius. Epidemiologically, the choice of surgical approach for primary THA varies geographically and by surgeon preference. While the posterior approach remains highly popular globally, and the direct anterior approach has seen a recent surge in adoption, the DLA maintains a significant role in many practices. Its utility is particularly recognized in patients where robust abductor function is paramount for early rehabilitation and stability, and in cases where a direct and controlled view of the acetabulum and proximal femur is desired without the need for extensive anterior soft tissue release or complex patient positioning.

Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is critical for minimizing complications and optimizing outcomes with the direct lateral approach.
Musculature
- Gluteus Maximus : This large, superficial muscle is typically retracted posteriorly or split longitudinally in line with its fibers, without significant detachment. It acts as a primary extensor and external rotator of the hip.
- Tensor Fascia Lata (TFL) : Located anterior to the gluteus medius, the TFL originates from the anterior iliac crest and inserts into the iliotibial (IT) band. The IT band must be incised longitudinally to access deeper structures. The TFL assists in hip flexion, abduction, and internal rotation.
- Gluteus Medius : The cornerstone of the hip abductor mechanism, originating from the external surface of the ilium and inserting onto the greater trochanter. In the modified DLA, the anterior portion of the gluteus medius is preserved, while the posterior portion, along with the gluteus minimus, is either partially detached from the greater trochanter or split judiciously in line with its fibers and the superior gluteal neurovascular bundle.
- Gluteus Minimus : Lying deep to the gluteus medius, it also originates from the ilium and inserts onto the greater trochanter, sharing the abductor function. Careful management is essential to avoid denervation or irreparable damage.
- Vastus Lateralis : This muscle originates from the greater trochanter and linea aspera, forming part of the quadriceps femoris. It is typically reflected anteriorly or split longitudinally from its origin on the vastus ridge of the femur to expose the femoral shaft.
Neurovascular Structures
- Superior Gluteal Nerve and Artery : These structures supply the gluteus medius and minimus. The nerve typically enters the deep surface of the gluteus medius approximately 4-5 cm proximal to the tip of the greater trochanter. Preserving the integrity of this neurovascular bundle is paramount to preventing post-operative abductor weakness and Trendelenburg gait. The surgical plane must be developed carefully to avoid injury.
- Lateral Femoral Cutaneous Nerve (LFCN) : While not directly within the primary surgical field of the DLA, it can be vulnerable during the initial skin incision, particularly if the incision is placed too anteriorly or extended excessively. It typically courses under the inguinal ligament, piercing the fascia lata distal to the anterior superior iliac spine (ASIS).
- Sciatic Nerve : Located deep and posterior to the hip joint, it is generally safe with the DLA. However, excessive posterior retraction during femoral exposure or in cases of severe posterior osteophytes can place it at risk.
- Femoral Artery and Nerve : These are located far anteriorly and medially, posing no direct risk during a standard DLA.
Biomechanics
The primary biomechanical advantage of the DLA is its potential for preserving a functional abductor mechanism. Unlike the posterior approach which can involve release of the short external rotators and posterior capsule, or some truly transgluteal approaches that involve a more extensive gluteus medius split, the modified DLA aims to minimize disruption to the abductors. A meticulous reattachment of any detached gluteus medius/minimus complex to the greater trochanter is crucial for restoring abductor moment arm and preventing Trendelenburg gait. Early mobilization post-operatively is facilitated by the relative stability conferred by an intact or well-repaired abductor mechanism and often a relatively preserved posterior capsule. This reduces the need for severe post-operative precautions common with approaches associated with higher dislocation risk.
Indications & Contraindications
The direct lateral approach offers a versatile pathway for various hip pathologies, particularly those requiring reconstructive surgery.
Indications for the Direct Lateral Approach (DLA)
-
Primary Total Hip Arthroplasty (THA)
:
- Osteoarthritis (OA) : The most common indication, where the DLA provides excellent exposure for acetabular and femoral component implantation.
- Rheumatoid Arthritis (RA) : Offers good visualization in inflammatory arthropathies, though soft tissue integrity may be compromised.
- Avascular Necrosis (AVN) : When hip replacement is indicated due to collapse of the femoral head.
- Post-traumatic Arthritis : After prior trauma to the hip, facilitating component placement in potentially altered anatomy.
- Femoral Neck Fractures : In elderly patients requiring hemiarthroplasty or THA due to displaced femoral neck fractures.
- Selected Revision THA : While the seed content notes difficulty, a DLA can be utilized for revisions primarily involving the femoral stem or liner exchange, especially if the original approach was lateral or if posterior access is challenging. However, it is less ideal for extensive acetabular revision or explantation of well-fixed components due to limited exposure.
- Abductor Repair : Direct visualization and repair of gluteal tendon tears can be achieved through this approach.
- Resurfacing Arthroplasty : Although less common, the DLA can provide the necessary exposure.
Contraindications for the Direct Lateral Approach (DLA)
- Extensive Revision Surgery : As noted in the seed content, the limited posterior and medial exposure compared to approaches like the posterior or extended trochanteric osteotomy makes it suboptimal for complex revisions, particularly those involving extensive acetabular reconstruction or difficult component removal.
- Severe Abductor Dysfunction/Pathology : Pre-existing severe atrophy, fatty infiltration, or irreparable tears of the gluteus medius and minimus may preclude the use of an approach that relies on their integrity, potentially exacerbating post-operative weakness. In such cases, a different approach or specific surgical techniques may be considered.
- Developmental Dysplasia of the Hip (DDH) with severe deformity : Cases requiring significant femoral shortening or complex acetabular reconstruction may benefit from approaches offering wider or more anterior exposure.
- Extreme Obesity : While not an absolute contraindication, significant adipose tissue can make dissection challenging and increase the risk of wound complications.
- Infection : In cases of active periprosthetic joint infection, the choice of approach may be secondary to the primary goal of débridement and component removal, which may necessitate a more versatile exposure.
Operative vs. Non-Operative Indications
The table below summarizes clinical scenarios, highlighting when the direct lateral approach (DLA) is typically indicated for operative management, contrasted with situations where non-operative management or alternative operative approaches may be preferred.
| Clinical Scenario | Operative Management (DLA Often Preferred) | Non-Operative Management | Alternative Operative Approach (DLA Less Preferred) |
|---|---|---|---|
| Primary Osteoarthritis | Symptomatic end-stage OA refractory to conservative measures. | Early/mild OA, pain manageable with PT, NSAIDs, injections. | Direct Anterior (DAA) for minimal muscle disruption; Posterior for extensive posterior release. |
| Avascular Necrosis (AVN) | Femoral head collapse (ARCO stage III/IV) with pain. | Early AVN (ARCO stage I/II), core decompression considered. | DAA for some; Posterior for complex femoral head reconstruction. |
| Rheumatoid Arthritis | Destructive arthropathy, functional impairment, pain. | Early disease, systemic management, non-surgical pain control. | DAA or Posterior based on surgeon preference and joint involvement. |
| Displaced Femoral Neck Fx | Unstable, displaced fractures in active elderly patients (THA/Hemiarthroplasty). | Non-displaced, stable impacted fractures in low-demand patients (internal fixation). | Posterior for easier access to femoral neck/head if fracture morphology complex. |
| Abductor Tendon Tears | Symptomatic, full-thickness, or chronic partial tears refractory to conservative care. | Partial tears responsive to PT, injections, activity modification. | - (DLA provides excellent access for repair) |
| Revision THA | Aseptic loosening of femoral stem or liner exchange, well-contained acetabular osteolysis. | None (once revision is indicated). | Extensive Acetabular Reconstruction (Posterior, Extended Trochanteric Osteotomy); Complex Femoral Revision (Extended Trochanteric Osteotomy). |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful execution of the direct lateral approach and optimizing outcomes.
Pre-Operative Planning
-
Clinical Assessment
:
- Patient History : Thorough review of medical comorbidities, prior hip surgery, neurological status, and functional goals. Assess for pre-existing abductor weakness or gait abnormalities.
- Physical Examination : Document hip range of motion, strength (especially abductors), limb length discrepancy, and neurovascular status. Identify palpable bony landmarks.
- Risk Stratification : Evaluate for risk factors for DVT/PE, infection, and general surgical risks. Implement appropriate prophylactic measures (e.g., DVT prophylaxis, pre-operative antibiotics, nutritional optimization).
-
Radiographic Templating
:
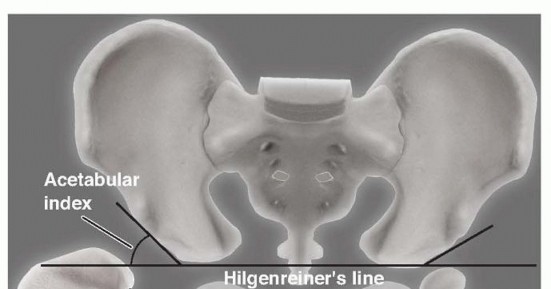
- Standard Views : Obtain a weight-bearing anteroposterior (AP) pelvis radiograph with both hips, a true lateral view of the affected hip, and potentially a cross-table lateral or frog-leg lateral. For complex cases, a CT scan with 3D reconstruction may be beneficial.
- Templating : Utilize digital templating software to estimate component size (femoral stem, acetabular cup, head size), identify potential difficulties (e.g., osteophytes, bone defects), and plan for restoration of hip biomechanics (e.g., leg length, offset). This aids in minimizing intraoperative guesswork and ensuring appropriate implant selection.
-
Equipment and Instrumentation
:
- Ensure all necessary retractors (e.g., Hohmann, cobra, army-navy), reamers, broaches, trial components, and definitive implants are available and sterilized.
- Confirm presence of fluoroscopy if intraoperative imaging is anticipated for specific cases (e.g., acetabular component positioning).
Patient Positioning
The patient is typically placed in a supine position on the operating table, as indicated in the seed content.

-
Operating Table Setup
:
- Position the patient such that the greater trochanter is at the edge of the operating table . This allows the ipsilateral buttock muscles and gluteal fat to fall posteriorly away from the operative field, improving exposure of the lateral aspect of the hip and proximal femur.
- A sandbag or positioning device may be placed under the contralateral hip or buttock to achieve a slight internal rotation of the affected limb, which can optimize femoral access later in the procedure.
- Ensure the table is positioned appropriately for the surgeon's comfort and ease of access.
-
Padding and Support
:
- Meticulously pad all pressure points, especially the contralateral arm, heels, sacrum, and peroneal nerve at the fibular head, to prevent nerve palsies or skin breakdown.
- Secure the patient to the table to prevent intraoperative movement, especially during manipulation for dislocation or component insertion.
-
Limb Preparation
:
- The entire lower extremity from the foot to the iliac crest should be prepped and draped to allow for full range of motion during the procedure. This is crucial for dislocating the femoral head and for assessing stability and leg length post-component insertion.
- A sterile stockinette is typically applied to the foot and ankle, leaving the toes exposed for neurovascular monitoring.
-
Sterile Draping
:
- Standard sterile draping protocols are followed, ensuring a wide operative field and maintaining sterility throughout the procedure. The draping should allow for full hip flexion, adduction, and external rotation, as these maneuvers are often necessary during femoral preparation and reduction.
Detailed Surgical Approach / Technique
The direct lateral approach, specifically the modified Hardinge technique, prioritizes preservation of the anterior portion of the gluteus medius while providing robust exposure.
Landmarks and Incision
The initial steps involve precise identification of anatomical landmarks to guide the incision.

-
Palpation
:
- Anterior Superior Iliac Spine (ASIS) : Located by palpating upward from below the iliac crest.
- Greater Trochanter (GT) : Palpate its lateral aspect, identifying its tip and superior border.
- Line of the Femur : Distal to the GT, identify the shaft of the femur as a resistance against the examining hand.
- Vastus Ridge : Identify the origin of the vastus lateralis from the lateral aspect of the greater trochanter and vastus ridge.
-
Incision
:
- Begin the incision approximately 5 cm proximal to the tip of the greater trochanter , aligning it slightly posterior to the anterior margin of the GT.
- Extend the incision distally along the line of the femoral shaft, usually 10-15 cm in length, centered over the greater trochanter. The length should be sufficient to allow adequate exposure for implant insertion without excessive retraction.
- The skin incision can be oriented slightly obliquely, parallel to the fibers of the tensor fascia lata, or directly longitudinal.

Step-by-Step Dissection
-
Skin and Subcutaneous Tissue
:
- Incise the skin and subcutaneous tissue down to the fascia lata. Achieve meticulous hemostasis.
- Reflect the skin and subcutaneous fat anteriorly and posteriorly using self-retaining retractors. Identify the glistening fascia lata.
-
Fascia Lata Incision
:
- Incise the fascia lata longitudinally along the line of the skin incision, extending proximally and distally.
- Identify the anterior border of the gluteus maximus, which often blends with the posterior aspect of the fascia lata. Retract the gluteus maximus posteriorly.

-
Gluteus Medius Management (Modified Hardinge)
:
- Identify the vastus lateralis origin on the greater trochanter.
- Incise the tendon of the gluteus medius in a controlled fashion. The key is to detach the posterior one-third to one-half of the gluteus medius and minimus from their insertion on the greater trochanter, leaving the anterior portion of the gluteus medius largely intact. This detachment is performed as an L-shaped incision, originating at the vastus ridge, coursing proximally along the anterior aspect of the GT, and then extending posteriorly along the superior aspect of the GT.
- Alternatively, a fascial flap containing a portion of the gluteus medius and minimus can be created by incising the fascia covering the gluteus medius and then detaching the muscle flap from the bone. This muscle-tendon unit is then reflected anteriorly.
- Carefully preserve the superior gluteal neurovascular bundle, which lies approximately 4-5 cm proximal to the tip of the greater trochanter. Avoid excessive superior dissection or retraction that could compromise these structures.
- With the gluteus medius partially detached or reflected, the piriformis and obturator internus tendons, as well as the hip capsule, become visible.
-
Femoral Exposure and Vastus Lateralis Reflection
:
- Incise the origin of the vastus lateralis from the greater trochanter and vastus ridge. Elevate it anteriorly to expose the lateral aspect of the proximal femur.
- Place Hohmann retractors around the femoral neck and greater trochanter to aid in exposure.
-
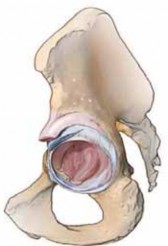
Capsulotomy
:
- Incise the hip capsule. Typically, an anterior or anterosuperior capsulotomy is performed. Some surgeons prefer a T-shaped or H-shaped capsulotomy to allow for wider exposure and later repair.
- Release the reflected head of the rectus femoris from its origin on the anterior inferior iliac spine if necessary for acetabular exposure.
-
Femoral Head Dislocation and Resection
:
- The hip is typically dislocated by flexing, adducting, and externally rotating the limb. Posterior dislocation is common with this approach, facilitated by capsular release.
- Resect the femoral head with an oscillating saw, typically at a level approximately one finger-breadth above the lesser trochanter, guided by pre-operative templating.
-
Acetabular Preparation
:
- Place appropriate retractors to expose the acetabulum (e.g., anterior Hohmann on the ilium, posterior Hohmann in the sciatic notch, medial retractor on the transverse acetabular ligament).
- Sequential reaming of the acetabulum is performed to create a hemispherical bed for the acetabular component.
- Insert the acetabular cup, ensuring appropriate anteversion (15-20 degrees) and inclination (40-45 degrees) for optimal stability and wear. Verify position with fluoroscopy if indicated.
- Impact the polyethylene liner or ceramic insert into the cup.
-
Femoral Preparation
:
- Address the femoral canal. Position the femur for optimal broaching (flexion, adduction, internal rotation).
- Sequential broaching of the femoral canal is performed, progressing in size until appropriate cortical fit and fill are achieved.
- Perform trial reduction with the selected femoral stem and head size to assess stability, leg length, and offset.
-
Reduction and Stability Assessment
:
- Reduce the trial components.
- Assess hip stability through a full range of motion, noting any impingement or signs of instability.
- Verify limb length equality.
- Once satisfied, remove trial components and implant definitive femoral stem and head.
- Perform final reduction.
-
Closure
:
- Irrigate the wound thoroughly.
- Abductor Repair : Meticulously reattach the detached gluteus medius/minimus complex to the greater trochanter using strong, non-absorbable sutures placed through drill holes in the bone or using transosseous sutures. This is a critical step for restoring abductor function and preventing Trendelenburg gait.
- Repair the vastus lateralis origin if it was incised as a separate layer.
- Close the fascia lata with interrupted or running absorbable sutures.
- Close subcutaneous tissues in layers.
- Close skin with staples or sutures.
- Apply a sterile dressing. A drain may or may not be used based on surgeon preference and intraoperative hemostasis.

(Illustrative image for deeper dissection or capsulotomy)

(Illustrative image for implant placement or final reduction)
Complications & Management
Despite its advantages, the direct lateral approach is not without potential complications. A thorough understanding of these risks and their management is essential.
Common Complications and Management Strategies
| Complication | Incidence (Approximate) | Salvage/Management Strategies
Clinical & Radiographic Imaging





You Might Also Like