Optimizing the Femur Lateral Approach: Comprehensive Guide to Technique, Anatomy, and Indications
Key Takeaway
The lateral approach to the femur provides direct access to the proximal and diaphyseal femur, crucial for fracture fixation. It involves a transmuscular split through the vastus lateralis muscle, requiring precise anatomical knowledge of the lateral femoral cutaneous nerve and perforating arteries from the profunda femoris to optimize technique and minimize complications.
Optimizing the Femur Lateral Approach: Technique & Uses
Introduction & Epidemiology
The lateral approach to the femur represents a cornerstone of orthopedic surgical access, particularly for the proximal and diaphyseal regions of the bone. Its utility stems from its directness, extensibility, and relative anatomical simplicity for achieving robust fixation. Historically, this approach has been instrumental in the management of high-energy trauma, degenerative conditions, and oncological pathologies affecting the femur.
The original description of a lateral approach to the femoral shaft is often attributed to Henry in the early 20th century, though its principles have been refined over decades. Its prominence in contemporary orthopedic practice is largely driven by the high incidence of hip and femoral fractures, particularly in the aging population. Intertrochanteric fractures alone account for a significant portion of fragility fractures, with projections indicating a substantial increase globally. Subtrochanteric and femoral shaft fractures also contribute significantly to the orthopedic trauma burden, often resulting from high-energy mechanisms in younger patients or low-energy falls in the elderly. The lateral approach facilitates the application of diverse internal fixation devices, including intramedullary nails and extramedullary plates, making it indispensable for fracture stabilization and anatomical restoration. While recognized for its efficiency, it inherently involves a transmuscular split through the vastus lateralis, leading to potential, typically self-limiting, intramuscular hemorrhage. The advantages often outweigh this consideration, especially when direct visualization and strong fixation are paramount.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is fundamental to optimizing the lateral approach. The approach navigates through distinct layers to expose the lateral cortex of the femur.
- Skin and Subcutaneous Tissue: The incision follows the long axis of the femur. Underlying subcutaneous fat contains superficial vessels and cutaneous nerves, notably branches of the lateral femoral cutaneous nerve (LFCN) proximally, which must be identified and protected where possible to mitigate dysesthesia.
- Fascia Lata: This dense, fibrous investing layer of the thigh muscles is incised longitudinally. Anteriorly, it blends with the tensor fascia lata; posteriorly, it forms the iliotibial band (ITB). Distally, the ITB inserts onto Gerdy's tubercle of the tibia.
-
Vastus Lateralis Muscle:
This is the largest component of the quadriceps femoris, originating from the greater trochanter, intertrochanteric line, gluteal tuberosity, and linea aspera, and inserting into the patella via the quadriceps tendon. The lateral approach involves a longitudinal split within the vastus lateralis, usually along its posterior third, to avoid the bulk of its nerve supply and vasculature.
- Vascular Supply: The vastus lateralis receives its primary blood supply from the lateral circumflex femoral artery (LCFA), a branch of the profunda femoris artery, which typically runs between the rectus femoris and vastus lateralis. Additionally, perforating branches from the profunda femoris artery traverse the vastus lateralis to reach the femur. These perforators are the primary vessels encountered and potentially disrupted during the muscle splitting, contributing to the described blood loss. Meticulous electrocautery or ligation of these vessels is crucial.
- Innervation: The vastus lateralis is innervated by branches of the femoral nerve (L2-L4), typically entering the muscle from its deep surface, anterior to the plane of the surgical split. Staying in the posterior third of the vastus lateralis generally minimizes neural injury.
- Femoral Periosteum: Once the vastus lateralis is split and retracted, the underlying periosteum is exposed. This layer is then incised and elevated subperiosteally to expose the lateral femoral cortex.
Internervous Plane: While often described as a transmuscular split, the lateral approach technically exploits an internervous plane between the vastus lateralis (femoral nerve innervation) and the muscles posterior to it (hamstrings and gluteus maximus, innervated by sciatic and inferior gluteal nerves, respectively). However, within the vastus lateralis itself, the split is transmuscular, carefully dissecting between its fibers to minimize muscle fiber transection and preserve nerve branches that typically enter the muscle more anteriorly. The ability to expose the entire length of the femur by extending this approach highlights its anatomical versatility. Proximally, it can be extended towards the greater trochanter, and distally, towards the lateral femoral condyle, carefully navigating around the knee joint.
The biomechanical implications of the vastus lateralis split are generally minimal in terms of long-term quadriceps function, provided the split is judicious and muscle re-approximation is meticulous. Acute blood loss and transient muscle edema are more common, contributing to post-operative pain and potential, albeit rare, compartment syndrome.
Indications & Contraindications
The lateral approach offers direct visualization and robust access to a significant portion of the femur, making it a workhorse approach for numerous orthopedic pathologies.
Common Indications:
*
Open Reduction and Internal Fixation (ORIF) of Intertrochanteric Fractures:
This is arguably the most frequent application. The approach allows for precise reduction and stable fixation with devices such as dynamic hip screws (DHS), intramedullary nails (recon nails), or locking plates.

*
Insertion of Internal Fixation for Subcapital Fractures or Slipped Upper Femoral Epiphysis (SUFE):
For unstable subcapital fractures or revision SUFE cases requiring open reduction, this approach facilitates guidewire placement and screw insertion, although percutaneous techniques are often preferred for stable variants.
*
Subtrochanteric or Intertrochanteric Osteotomy:
Corrective osteotomies for malunions, angular deformities, or developmental dysplasia of the hip (e.g., varus derotation osteotomy for SUFE sequelae) are well-managed via this exposure.
*
ORIF of Femoral Shaft Fractures, Subtrochanteric Fractures, and Supracondylar Fractures:
While intramedullary nailing is often performed minimally invasively for shaft fractures, open reduction with plating (e.g., for comminuted fractures, those with significant soft tissue injury precluding nailing, or non-unions) frequently employs the lateral approach. Distal extension provides access for supracondylar fractures managed with locking plates.
*
Extra-articular Arthrodesis of the Hip Joint:
Though less common today, in specific complex cases like failed total hip arthroplasty with intractable infection or severe paralytic hip instability, this approach can facilitate fusion.
*
Treatment of Chronic Osteomyelitis of the Femur:
Debridement, sequestrectomy, and antibiotic-impregnated bead placement for chronic infections of the femoral shaft or proximal femur.
*
Biopsy and Treatment of Bone Tumors:
For primary or metastatic lesions of the femoral diaphysis or metaphysis requiring open biopsy, curettage, or wide local excision with reconstruction.
Contraindications:
Absolute contraindications are few, primarily relating to patient factors precluding surgery (e.g., critical medical comorbidities, uncontrolled sepsis). Relative contraindications or considerations for alternative approaches include:
*
Extensive Medial or Posterior Soft Tissue Injury:
If the lateral soft tissues are severely compromised (e.g., large open wound, crush injury, compartment syndrome affecting the vastus lateralis), an alternative approach may be necessary to preserve viable tissue.
*
Primary Access Required for Medial or Posterior Femur:
For specific procedures like direct visualization of the posteromedial cortex, extensive posterior column exposure, or where the pathology is predominantly on the opposite side, other approaches (e.g., posteromedial, direct anterior) might be more appropriate or necessitate significant anterior or posterior retraction from the lateral approach.
*
Proximal Femoral Pathologies requiring Articular Access:
For intra-articular hip pathologies, the direct anterior, anterolateral, or posterior approaches are generally preferred as the lateral approach is primarily extra-articular.
*
Prior Surgery with Significant Scarring:
Extensive scarring from previous lateral approaches could make re-entry challenging and increase the risk of neurovascular injury.
Table 1: Indications for Lateral Femoral Approach vs. Considerations for Alternative Approaches
| Category | Indications for Lateral Femoral Approach | Considerations for Alternative Approaches/Non-Operative Management |
|---|---|---|
| Fracture Management | - Unstable intertrochanteric fractures (ORIF with DHS/IMN/plate) | - Stable, undisplaced intertrochanteric fractures (IMN or percutaneous screws via limited approaches) |
| - Subtrochanteric fractures (ORIF with IMN/plate) | - Non-displaced femoral neck fractures (percutaneous screw fixation via anterolateral or direct anterior approaches) | |
| - Femoral shaft fractures requiring open reduction and plating (e.g., highly comminuted, open fractures, segmental defects, non-unions) | - Most femoral shaft fractures (closed reduction with intramedullary nailing via piriformis or trochanteric entry; often minimally invasive) | |
| - Distal femoral/supracondylar fractures (ORIF with locking plates) | - Certain intercondylar fractures (posterior approach for specific fragment fixation) | |
| Deformity Correction | - Subtrochanteric or intertrochanteric osteotomies (e.g., for varus/valgus deformities, malunions, SUFE sequelae) | - Minor angular deformities (non-operative bracing/observation if skeletally immature or asymptomatic) |
| Infection | - Chronic osteomyelitis of the femoral shaft or proximal femur (debridement, sequestrectomy, local antibiotic delivery) | - Acute osteomyelitis without significant bony destruction (IV antibiotics alone) |
| Oncology | - Open biopsy of femoral bone tumors (primary or metastatic) | - Image-guided core needle biopsy (for initial diagnosis of accessible lesions) |
| - Wide local excision and reconstruction for femoral tumors | - Chemotherapy/radiation for systemic disease without need for surgical intervention | |
| Other | - Failed Total Hip Arthroplasty requiring femoral revision or reconstruction (when lateral access is sufficient) | - Primary Total Hip Arthroplasty (Direct Anterior, Anterolateral, Posterior approaches generally preferred for primary articular access) |
| - Extra-articular hip arthrodesis (rare) | - Most hip pathologies requiring intra-articular access (posterior, direct anterior, anterolateral approaches) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and optimal patient positioning are critical for successful execution and minimizing complications with the lateral approach.
Pre-Operative Planning:
1.
Imaging Review:
Thorough review of radiographs (AP pelvis, AP and lateral femur), CT scans (for complex fractures, comminution, deformity), and MRI (for tumors, osteomyelitis, soft tissue involvement).
2.
Templating:
Crucial for selecting appropriate implant size, length, and trajectory (e.g., plate length, screw number and position, IM nail diameter/length/distal locking options).
3.
Anatomical Assessment:
Identification of potential anatomical variants or previous surgical scars that may alter the approach.
4.
Blood Management:
Assess patient's baseline hemoglobin, coagulation status, and potential need for blood products. Consider anti-fibrinolytic agents (e.g., tranexamic acid) as per institutional protocols for appropriate cases.
5.
Tourniquet Considerations:
While a tourniquet can reduce blood loss, it is often not feasible or contraindicated for proximal femoral procedures or lengthy cases. When used, careful consideration of inflation time and potential ischemic complications is necessary.
Patient Positioning:
The patient's position depends on the specific pathology and implant to be utilized.
-
Supine Position on a Fracture Table:
- Indications: Primarily for intertrochanteric and subtrochanteric fractures managed with intramedullary nails or dynamic hip screws. This setup allows for controlled traction, rotation, and adduction/abduction for fracture reduction, as well as easy access for fluoroscopy in both AP and lateral planes without repositioning.
- Technique: The patient is placed supine on the fracture table. The affected leg is placed in traction, with appropriate padding at the perineum and under the non-affected leg. The torso is typically tilted away from the operative side to allow for clear fluoroscopic visualization of the proximal femur.
-
Image placement
: This image would be suitable here to illustrate the supine position and prep for a proximal femur case.
- The contralateral leg is abducted and elevated on a leg holder to allow for fluoroscopic image intensifier access to the surgical field.
-
Image placement
: Another positioning image.
-
Lateral Decubitus Position:
- Indications: Often preferred for femoral shaft fractures requiring plating, certain subtrochanteric fractures, or distal femoral fractures when the operative leg needs to be free for manipulation. It provides excellent direct lateral access to the femoral shaft.
- Technique: The patient is placed in a true lateral decubitus position with the operative side up. Adequate padding is placed between the knees and ankles. The pelvis and torso are stabilized with bolsters or beanbags to prevent rotation. The operative limb is draped free, allowing for full range of motion at the hip and knee.
- Advantages: This position offers unrestricted access to the lateral aspect of the femur for the full extent of the approach. It also facilitates easier identification of the ITB and vastus lateralis.
- Disadvantages: Fluoroscopic imaging can be more challenging in this position, often requiring repositioning of the C-arm or careful angling to obtain true AP and lateral views.


Draping:
Standard sterile draping is performed, exposing the entire lateral aspect of the thigh from the iliac crest to just above the knee, depending on the anticipated extent of the exposure. A sterile tourniquet may be applied proximally if anticipated.
Detailed Surgical Approach / Technique
The lateral approach provides excellent direct access to the vast majority of the femoral shaft and both proximal and distal metaphyses. The primary challenge lies in meticulous management of the vastus lateralis and its neurovascular supply.
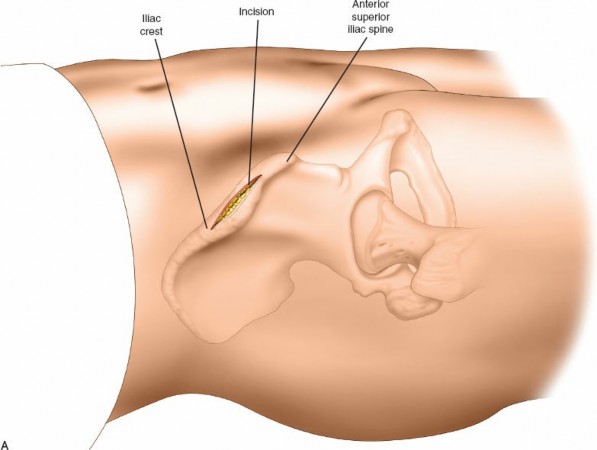
1. Incision
The skin incision is typically longitudinal, centered over the lateral aspect of the femoral shaft.
*
Proximally:
The incision begins approximately 2-3 cm distal and posterior to the tip of the greater trochanter, extending distally. For proximal femoral fractures (intertrochanteric, subtrochanteric), it will be centered over the greater trochanter and extend distally along the line connecting the greater trochanter to the lateral femoral condyle.
*
Length:
The length of the incision is dictated by the pathology and the implant chosen. For a standard plating of a femoral shaft fracture, it must be long enough to accommodate the plate and allow for necessary reduction maneuvers.
*
Image placement
: This image showing incision marking would be appropriate here.

2. Subcutaneous Dissection
- The skin and subcutaneous tissue are incised, and subcutaneous fat is bluntly and sharply dissected to expose the underlying fascia lata.
- Careful hemostasis is maintained throughout this layer to minimize blood loss. Identification and protection of sensory nerves, particularly branches of the LFCN superiorly, should be attempted, although nerve injury can still occur due to retraction.
3. Incision of the Fascia Lata
- The fascia lata is identified, which appears as a glistening, dense fibrous layer.
- A longitudinal incision is made through the fascia lata, in line with the skin incision. This incision should be carefully placed to avoid injury to the underlying vastus lateralis muscle fibers.
- The incision in the fascia lata can be extended proximally and distally as needed. Proximally, it often involves splitting the fibers of the iliotibial band (ITB) which is a thickened lateral portion of the fascia lata.
4. Splitting the Vastus Lateralis
This is the critical step of the approach, requiring precision to minimize muscle damage and preserve perforating vessels until they can be ligated or cauterized.
* The vastus lateralis muscle is identified beneath the incised fascia lata.
* The muscle fibers are bluntly or sharply separated longitudinally. A common plane for splitting is the posterior third of the muscle, which is generally less vascular and typically avoids the main motor nerve supply entering more anteriorly.
*
Image placement
: This image could represent the initial split through the vastus lateralis.

* The splitting process should be carried out down to the femoral periosteum. Using two large Hohmann retractors or a self-retaining retractor can facilitate this exposure.
*
Managing Perforating Vessels:
As the vastus lateralis is split, several perforating vessels from the profunda femoris artery and lateral circumflex femoral artery will be encountered. These typically run transversely through the muscle to supply the vastus lateralis and the femoral cortex.
*
Image placement
: This image illustrating vessels within the muscle is highly relevant here.

* These vessels must be meticulously ligated (with absorbable suture) or coagulated (with electrocautery) to minimize blood loss, which can otherwise be significant and obscure the field. Attempting to preserve some perforators, especially more distal ones, when extensive exposure is not required, can theoretically contribute to preserving femoral vascularity, particularly in fracture healing.
5. Subperiosteal Exposure of the Femur
- Once the vastus lateralis is sufficiently split and retracted anteriorly and posteriorly, the femoral periosteum is exposed.
-
The periosteum is incised longitudinally along the desired length of the bone and elevated off the lateral cortex using a Cobb elevator or similar periosteal elevator. This subperiosteal dissection provides a relatively bloodless plane.
-
Image placement
: This image showing the exposed femur with retractors would fit well here.
- The degree of periosteal stripping should be carefully controlled. Excessive stripping, particularly in a comminuted fracture, can compromise the blood supply to the bone fragments and increase the risk of non-union.
-
Image placement
: This image showing the exposed femur with retractors would fit well here.

6. Reduction and Fixation
- With the femoral cortex exposed, the fracture can be directly visualized.
-
Reduction:
Reduction techniques vary depending on the fracture pattern. Direct manipulation with bone clamps, reduction forceps, or joystick techniques (using small Kirschner wires) may be employed. Traction applied via a fracture table or manual traction can assist.
-
Image placement
: An image showing the exposed femur, possibly with a fracture or during reduction.
-
Image placement
: An image showing the exposed femur, possibly with a fracture or during reduction.
-
Fixation:
Once reduction is satisfactory, the chosen internal fixation device (e.g., dynamic hip screw, intramedullary nail, locking plate) is applied.
- For plating, the plate is contoured as needed and positioned on the lateral cortex. Screws are then inserted according to established principles of osteosynthesis, ensuring bicortical purchase where appropriate and respecting the fracture biology.
-
Image placement
: Images showing plate application and final fixation.
-
Fluoroscopy is used intermittently to confirm reduction and implant position.
-
Image placement
: This image showing an X-ray/fluoroscopy of fixation.
-
Image placement
: This image showing an X-ray/fluoroscopy of fixation.



7. Wound Closure
- After irrigation and final check for hemostasis, the periosteum (if significantly elevated) can be loosely re-approximated, although this is not always necessary.
- The vastus lateralis muscle is allowed to fall back into place. Often, a few interrupted absorbable sutures can be placed to loosely re-approximate the muscle fascia, but direct repair of the muscle fibers is typically not performed or required.
- The fascia lata is repaired with a strong, interrupted or running absorbable suture.
-
The subcutaneous layer is closed, followed by the skin. A surgical drain may be placed in cases of extensive dissection or significant anticipated blood loss.
-
Image placement
: This image representing wound closure.
-
Image placement
: This image representing wound closure.

Complications & Management
While the lateral approach is considered safe and effective, several complications can arise, necessitating vigilant post-operative monitoring and appropriate management strategies.
Table 2: Common Complications of the Lateral Femoral Approach, Incidence, and Salvage Strategies
| Complication | Estimated Incidence | Management Strategies |
|---|---|---|
| Intraoperative Blood Loss | Common (often >500mL) |
- Meticulous hemostasis: meticulous cautery/ligation of perforating vessels.
- Pre-operative optimization of coagulation. - Intraoperative use of tranexamic acid. - Blood transfusion as needed. |
| Post-operative Hematoma | 5-10% |
- Close monitoring, re-exploration for expanding hematoma.
- Surgical drain placement in select cases. - May contribute to infection risk. |
| Infection (Superficial/Deep) | 1-5% |
- Prophylactic antibiotics.
- Meticulous sterile technique. - Superficial: wound care, oral antibiotics. - Deep: surgical debridement, IV antibiotics, implant retention (if stable) or removal (if unstable/persistent infection), wound vac. |
| Lateral Femoral Cutaneous Nerve (LFCN) Injury/Dysesthesia | 5-15% (sensory) |
- Careful identification and protection during incision and retraction.
- Most are neuropraxia, resolving spontaneously. - Persistent dysesthesia: conservative management (NSAIDs, gabapentin), rarely neurectomy. |
| Vastus Lateralis Weakness/Atrophy | Mild: Common; Severe: Rare |
- Minimizing muscle trauma during splitting.
- Physiotherapy focusing on quadriceps strengthening. - Most cases are transient and mild; significant weakness is uncommon if proper technique is followed. |
| Non-Union / Malunion (Fracture-Specific) | Varies greatly by fracture type (e.g., Femoral Shaft: 5-15%) |
- Optimized reduction and stable fixation.
- Bone grafting (autograft/allograft) for biologically challenging unions. - Revision surgery with plate exchange, IM nail exchange, dynamization, or compression, potentially with bone stimulators. |
| Hardware Failure / Prominence | 5-10% |
- Careful implant selection and placement.
- Early weight-bearing restrictions if fracture is unstable. - Symptomatic hardware prominence: elective hardware removal after fracture healing. |
| Iatrogenic Nerve Injury (other) | <1% (Sciatic, Femoral) |
- Meticulous surgical technique, avoiding excessive deep/posterior retraction.
- Careful patient positioning. - Post-op neurophysiological evaluation. - Management based on severity: observation, physical therapy, nerve repair/grafting in severe cases. |
| Heterotopic Ossification (HO) | 5-15% (especially in trauma/head injury) |
- Prophylactic NSAIDs or radiation therapy in high-risk patients.
- Excision for symptomatic HO after maturity. |
| Refracture | 1-3% |
- Adequate healing time before hardware removal (if applicable).
- Avoidance of premature aggressive activity. - Revision surgery for stabilization. |
Key Management Considerations:
*
Preventative Measures:
Strict adherence to surgical principles, including careful dissection, meticulous hemostasis, appropriate implant selection, and gentle soft tissue handling, are the best preventative strategies.
*
Early Recognition:
Post-operative surveillance for signs of complications (e.g., wound dehiscence, excessive drainage, fever, neurological deficits) is crucial.
*
Multidisciplinary Approach:
Management of complex complications often requires collaboration with infectious disease specialists, neurologists, plastic surgeons, and rehabilitation therapists.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following a lateral femoral approach is highly individualized, depending on the specific pathology treated, the stability of fixation, and patient-specific factors (e.g., age, comorbidities, pre-injury function). The overarching goals are to restore function, minimize pain, and prevent complications while protecting the integrity of the repair.
General Principles:
- Pain Management: A multimodal approach including opioids, NSAIDs, acetaminophen, and regional nerve blocks can effectively manage post-operative pain, facilitating early mobilization.
-
Early Mobilization:
- Within 24-48 hours: Patients are typically encouraged to perform ankle pumps, isometric quadriceps sets, and gentle hip/knee range of motion (ROM) exercises as tolerated.
- Out-of-bed activity: Ambulation with assistive devices (walker, crutches) is initiated as soon as medically stable, often within the first post-operative day, particularly for hip fracture patients.
-
Weight-Bearing (WB) Status:
This is the most critical variable and is determined by the stability of the fracture fixation.
- Non-weight bearing (NWB) or Toe-touch weight-bearing (TTWB): For highly unstable fractures, severe comminution, or osteoporotic bone where initial fixation strength is a concern (e.g., certain subtrochanteric fractures, distal femur peri-articular fractures). This may be maintained for 6-12 weeks.
- Partial weight-bearing (PWB): Gradually progressed from TTWB as pain subsides and radiographic signs of healing appear.
- Weight-bearing as tolerated (WBAT): Often permitted for stable intertrochanteric fractures fixed with intramedullary nails or plates, and selected stable femoral shaft fractures. This is typically initiated early and advanced as tolerated.
- Full weight-bearing (FWB): The ultimate goal, achieved once there is definitive radiographic evidence of fracture union and clinical stability.
-
Range of Motion (ROM):
- Hip and Knee: Gentle active-assisted and active ROM exercises for the hip and knee are initiated early to prevent stiffness, typically within pain limits. For certain cases like distal femoral fractures, a hinged knee brace may be used to control ROM.
- Adductor Precaution: For proximal femoral approaches, care must be taken with excessive adduction if a large fragment has been internally fixed or if there's concern for medial soft tissue disruption.
-
Strengthening:
- Isometric Exercises: Initially, focusing on quadriceps and gluteal muscle activation.
- Progressive Resistance: As healing progresses and WB status improves, strengthening exercises are advanced to include isotonic and eventually functional resistance activities. Special attention is paid to quadriceps (particularly vastus lateralis) and hip abductor strength.
-
Functional Training:
- Gait training, balance exercises, stair climbing, and proprioceptive drills are incorporated to restore functional independence and reduce fall risk.
- For athletes or highly active individuals, sports-specific rehabilitation is phased in once bone healing is robust and strength has returned.
Typical Phased Rehabilitation (Example for a Stable Femoral Shaft Fracture with Plating):
-
Phase 1 (Weeks 0-6: Acute Post-operative / Protection Phase):
- WB: PWB to WBAT (if stable).
- ROM: Gentle active and active-assisted hip and knee ROM.
- Strength: Isometric quadriceps, gluteal sets, ankle pumps.
- Activity: Out-of-bed to chair/commode, ambulation with walker/crutches.
-
Phase 2 (Weeks 6-12: Intermediate / Controlled Mobility Phase):
- WB: Progress to FWB as tolerated, guided by radiographs.
- ROM: Full, pain-free hip and knee ROM.
- Strength: Light resistance exercises for quadriceps, hamstrings, glutes, core. Closed-chain exercises (e.g., mini-squats).
- Activity: Progress to single crutch, then cane. Stationary cycling (low resistance).
-
Phase 3 (Weeks 12+: Advanced / Strengthening & Return to Function Phase):
- WB: FWB.
- Strength: Progressive resistance training, functional strength, balance, proprioception.
- Activity: Gradual return to recreational activities. Impact activities or sports-specific training initiated only after confirmed radiographic union and full strength recovery.
Duration: Full rehabilitation can take 6-12 months or longer, depending on the complexity of the injury and patient goals. Regular clinical and radiographic follow-up is essential to guide progression.
Summary of Key Literature / Guidelines
The lateral approach to the femur has been extensively studied and continues to be a subject of ongoing research, particularly concerning its application in specific fracture patterns, comparison with minimally invasive techniques, and optimization of outcomes.
1. Intertrochanteric Fractures:
*
Intramedullary Nailing (IMN) vs. Dynamic Hip Screw (DHS):
For unstable intertrochanteric fractures, IMN has become the preferred implant, often utilizing a limited lateral approach (mini-open or percutaneous for nail insertion) and the standard lateral approach for reduction if needed. Studies consistently show IMN to be biomechanically superior in unstable patterns, with potentially lower rates of cut-out and non-union compared to DHS in certain fracture types (e.g., reverse obliquity).
*
Entry Point and Reduction:
The lateral approach facilitates direct visualization for reduction maneuvers when closed reduction is challenging. Proper entry point for IMN (piriformis fossa vs. greater trochanter tip) and reduction of the fracture fragments are paramount, guiding outcomes.
*
Literature
: Meta-analyses and large prospective studies (e.g., from the AO Foundation) frequently compare outcomes of various implants and techniques, emphasizing the importance of anatomical reduction and stable fixation.
2. Femoral Shaft Fractures:
*
IMN as Gold Standard:
For most femoral shaft fractures, closed reduction and intramedullary nailing (often via a piriformis or trochanteric entry point) remains the gold standard, often performed with minimally invasive incisions.
*
Role of Open Reduction and Plating:
The lateral approach for open reduction and plating is reserved for specific situations:
* Polytrauma patients with associated head injuries (where reaming for IMN might be contraindicated due to fat emboli risk).
* Open fractures requiring extensive debridement.
* Segmental bone loss or severe comminution requiring direct visualization and bone grafting.
* Non-unions or malunions requiring revision.
* Distal femoral shaft/supracondylar fractures where locking plates are applied using the lateral approach.
*
Literature
: Studies on locked plating via the lateral approach highlight its utility for complex femoral shaft fractures, achieving high union rates with proper surgical technique, though careful soft tissue handling is crucial to mitigate periosteal stripping effects on vascularity.
3. Subtrochanteric Fractures:
*
IMN vs. Plating:
This remains an area of debate for certain fracture patterns, particularly with extensive comminution. While IMN is increasingly favored due to its load-sharing characteristics, locked plating via the lateral approach provides excellent stability, particularly for comminuted fractures with cortical defects or in revision settings.
*
Literature
: Research evaluates various plating constructs (e.g., long vs. short, number of screws) and their biomechanical properties, emphasizing the need for robust fixation in this high-stress region.
4. Soft Tissue Considerations and Muscle Splitting:
* The original seed content highlighted the "blood loss that results from the rupture of vessels during this procedure." Modern surgical techniques emphasize meticulous hemostasis and careful dissection to minimize this.
* The comparison with the "posterolateral approach... favored by some surgeons for surgery on the proximal femur" reflects a historical preference for planes that avoid muscle splitting entirely. However, the lateral approach's directness and extensibility often outweigh this consideration for the vastus lateralis split, particularly when direct visualization is critical for complex reductions or precise plate application.
*
Literature
: Studies have investigated the long-term functional outcomes of vastus lateralis splitting, generally concluding that significant functional deficits are rare, especially with meticulous technique. The balance between direct visualization for optimal reduction and fixation versus minimally invasive approaches (which may compromise direct visualization) is a continuous subject of clinical discussion.
5. Minimally Invasive Techniques:
While the classic lateral approach involves a significant incision, advancements in minimally invasive techniques (MIPO - Minimally Invasive Plate Osteosynthesis) often utilize smaller lateral incisions for plate insertion, tunneling the plate submuscularly. This aims to preserve soft tissue attachments and blood supply, potentially reducing infection rates and improving bone healing. However, these techniques still rely on the fundamental anatomical understanding derived from the standard lateral approach and may require a larger lateral incision for initial reduction or complex cases.
In conclusion, the lateral approach to the femur remains an indispensable tool in the orthopedic surgeon's armamentarium. Its consistent utility across a broad spectrum of femoral pathologies, coupled with ongoing refinements in surgical technique and implant design, solidifies its position as a critical access route for optimizing patient outcomes. Continuous academic discourse and adherence to evidence-based guidelines ensure its effective and safe application.
Clinical & Radiographic Imaging








You Might Also Like