Intracapsular Hip Fractures in Young Patients: Epidemiology, Anatomy, Biomechanics & Management
Key Takeaway
Intracapsular hip fractures in young, neurologically intact patients are high-energy injuries primarily challenging due to the risk of avascular necrosis (AVN) and nonunion. Management emphasizes anatomic reduction and stable fixation to preserve the native hip. Understanding femoral head blood supply and fracture classifications (Garden, Pauwels) is crucial for optimal outcomes and preventing devastating complications.
Introduction & Epidemiology
Intracapsular hip fractures in young, neurologically intact patients are high-energy injuries that represent a distinct challenge in orthopedic trauma. Unlike their geriatric counterparts, these fractures typically result from significant trauma, such as motor vehicle accidents, falls from height, or industrial injuries. While less common than intertrochanteric or femoral neck fractures in the elderly, their management carries profound implications due to the patient's expected longevity and functional demands. The primary concern in this population is the prevention of devastating complications, notably avascular necrosis (AVN) of the femoral head and nonunion, which can severely compromise long-term hip function and often necessitate secondary arthroplasty.
The definition of "young" patients in this context generally refers to individuals under 50-60 years of age, emphasizing the goal of native hip preservation. Incidence rates are relatively low, estimated at 3-5% of all hip fractures, but their impact is disproportionately high due to the associated morbidity. Fractures are typically classified by the Garden classification (based on displacement and impaction) and Pauwels classification (based on the angle of the fracture line to the horizontal, reflecting shear forces). Garden I and II fractures are undisplaced or minimally displaced and impacted, while Garden III and IV are completely displaced. Pauwels classification (Type I <30°, Type II 30-50°, Type III >50°) correlates with increasing shear forces and instability, predictive of nonunion risk. Anatomic reduction and stable internal fixation remain the cornerstones of treatment to optimize outcomes and mitigate the risk of AVN and nonunion.
Surgical Anatomy & Biomechanics
Successful management of intracapsular hip fractures hinges on a thorough understanding of the femoral head's unique blood supply and the biomechanical forces at play.
Femoral Head Blood Supply
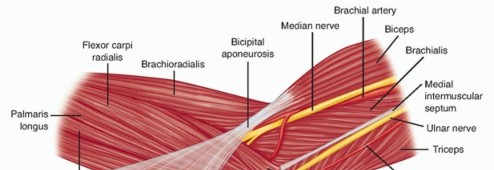
The arterial supply to the femoral head is predominantly derived from the medial femoral circumflex artery (MFCA) and, to a lesser extent, the lateral femoral circumflex artery (LFCA) and the artery of the ligamentum teres.
*
Medial Femoral Circumflex Artery (MFCA):
This is the dominant source. It typically arises from the profunda femoris artery and courses posteriorly, deep to the quadratus femoris muscle. It then gives off ascending branches that pierce the capsule to form the retinacular vessels (posterior superior, posterior inferior, anterior superior, anterior inferior), which ascend along the femoral neck within the synovium, ultimately forming an extracapsular arterial ring at the base of the femoral neck and an intracapsular arterial ring at the articular margin. The posterior superior retinacular vessels are often considered the most critical, supplying the majority of the superior and posterior femoral head.
*
Lateral Femoral Circumflex Artery (LFCA):
Contributes primarily to the extracapsular arterial ring but typically has less direct supply to the femoral head itself compared to the MFCA.
*
Artery of the Ligamentum Teres (Foveal Artery):
A branch of the obturator artery (or occasionally MFCA/LFCA), it travels within the ligamentum teres to supply a small, variable portion of the inferomedial femoral head. Its contribution is generally minor in adults but can be more significant in children and adolescents.
An intracapsular fracture, by definition, occurs within the synovial capsule, directly threatening these retinacular vessels. Displacement of the fracture fragments can tear or kink these vessels, leading to ischemia. Furthermore, an intracapsular hematoma can create a tamponade effect, elevating intracapsular pressure and further compromising blood flow to the femoral head. The integrity of the posterior retinacular vessels is particularly vulnerable and directly correlates with the risk of AVN.
Fracture Biomechanics and Stability
The stability of an intracapsular hip fracture is dictated by the fracture pattern and the direction of the forces applied.
*
Garden Classification:
Describes the degree of displacement and impaction.
*
Garden I (Incomplete, impacted valgus):
Relatively stable, impaction reduces shear.
*
Garden II (Complete, undisplaced):
Fracture line extends completely, but fragments remain aligned. Inherently less stable than Garden I and carries risk of secondary displacement.
*
Garden III (Complete, partially displaced):
Head is displaced relative to the neck, often varus angulation. Significant risk of AVN.
*
Garden IV (Complete, fully displaced):
No bony contact, head and neck are completely separated. Highest risk of AVN and nonunion.
*
Pauwels Classification:
Focuses on the angle of the fracture line relative to the horizontal plane. This angle reflects the shear forces acting on the fracture site.
*
Pauwels Type I (<30°):
Primarily compressive forces, relatively stable.
*
Pauwels Type II (30-50°):
Mixed compressive and shear forces, moderate instability.
*
Pauwels Type III (>50°):
Predominantly shear forces, highly unstable, and prone to nonunion without stable fixation.
The goal of surgical fixation is to counteract these shear and compressive forces, achieve stable compression across the fracture site, and provide rotational stability. Displaced fractures, especially those with high Pauwels angles, require robust fixation to resist collapse and maintain reduction until healing occurs.
Indications & Contraindications
The management of intracapsular hip fractures in young patients is predominantly surgical, with a strong emphasis on urgency. The goal is to preserve the native hip joint by achieving anatomic reduction and stable fixation, thereby minimizing the risk of avascular necrosis and nonunion.
Indications for Operative Management
- All displaced intracapsular femoral neck fractures (Garden III & IV) in young patients: This is a near-absolute indication. Prompt, anatomic reduction and stable internal fixation are critical to optimize femoral head viability and prevent nonunion.
- Undisplaced or minimally displaced intracapsular femoral neck fractures (Garden I & II) in young patients: While some Garden I fractures in elderly, low-demand patients might be managed non-operatively, in young, active patients, operative fixation is generally recommended. This is due to the significant risk of secondary displacement (up to 25%) and the potentially devastating consequences (AVN, nonunion) that would lead to premature hip arthroplasty. The operative fixation offers enhanced stability and reduces the risk of further vascular compromise.
- Urgency: The "time to surgery" is a critical factor. Operative fixation within 6-12 hours of injury (some literature extends to 24 hours) is strongly advocated to maximize the chances of femoral head survival by decompressing the intracapsular hematoma and restoring stability, potentially improving blood flow.
Relative Contraindications for Operative Management
- Unstable Medical Comorbidities: Patients with severe, uncompensated medical conditions that preclude safe anesthesia and surgery. However, even in these cases, stabilization and optimization are prioritized given the long-term implications.
- Moribund Patient: In situations where the patient's prognosis is extremely poor due to other life-threatening injuries, surgery for the hip fracture may be deferred or palliative measures considered.
- Severe Pre-existing Hip Pathology: Rarely, in a young patient with advanced, symptomatic pre-existing hip osteoarthritis or established, severe avascular necrosis prior to the acute fracture, a primary total hip arthroplasty might be considered. However, the default in young patients is always preservation of the native joint.
Operative vs. Non-Operative Indications
| Indication Type | Scenario | Rationale |
|---|---|---|
| Operative | Displaced Intracapsular Fracture (Garden III, IV) | Urgent anatomic reduction & stable fixation to prevent AVN & nonunion, preserve native joint. |
| Undisplaced/Minimally Displaced Intracapsular Fracture (Garden I, II) | Prophylactic fixation to prevent secondary displacement, reduce AVN/nonunion risk, and expedite recovery. | |
| Patients awaiting other critical life-saving procedures | Fixation within optimal time window (6-12 hours) if medically stable; otherwise, temporary stabilization. | |
| Non-Operative | Medically Unstable/Moribund Patient | High surgical risk outweighs potential benefits; often palliative care or temporary splinting. |
| Very rare, highly comminuted fractures with impossible fixation | (Controversial) May proceed directly to primary arthroplasty if no viable option for fixation. | |
| Elderly, low-demand, impacted valgus fractures (Garden I) | (Not applicable for "young patients" focus of this guide, but mentioned for completeness.) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are crucial for successful reduction and fixation of intracapsular hip fractures in young patients.
Pre-Operative Assessment & Planning
- Resuscitation and Stabilization: Adhere to ATLS (Advanced Trauma Life Support) protocols. These are often high-energy injuries, so assess for other life-threatening injuries (head, chest, abdominal, pelvic) and ensure hemodynamic stability.
-
Imaging:
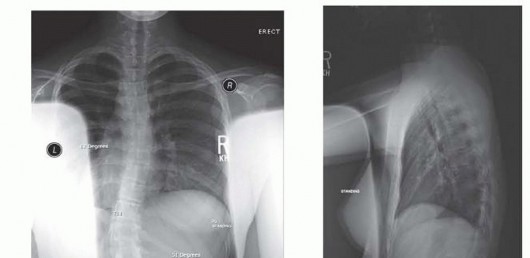
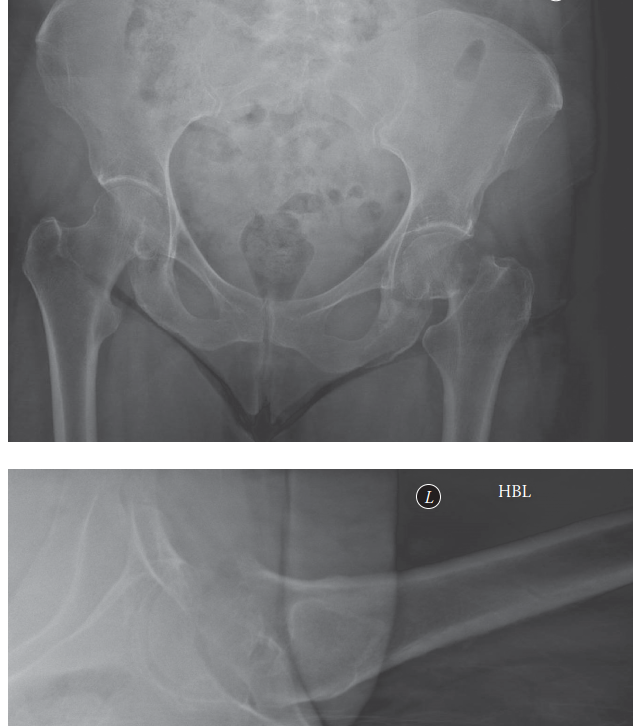
- AP Pelvis and Cross-Table Lateral Hip X-rays: Standard initial imaging to confirm diagnosis, classify fracture (Garden, Pauwels), and assess displacement.
- Computed Tomography (CT) Scan: Essential for detailed fracture morphology, especially for comminution, impaction patterns, and articular involvement. It aids in surgical planning for reduction maneuvers and screw placement. It can also rule out occult fractures.
- Magnetic Resonance Imaging (MRI): Not typically used in the acute setting for fracture diagnosis but can be valuable post-operatively for early detection of AVN or in cases of persistent pain with normal X-rays to assess for occult nonunion or early chondral damage.
- Timing of Surgery: "Time is bone." The consensus strongly supports urgent surgical intervention, ideally within 6-12 hours from injury, to decompress the intracapsular hematoma and restore mechanical stability, thereby minimizing the risk of vascular compromise and AVN. Delays beyond 24 hours are associated with increased rates of AVN and nonunion.
- Medical Optimization: Coordinate with anesthesia for pre-operative medical clearance and optimization. Address any co-morbidities.
- Implant Selection: Cannulated screws (CS) are the gold standard for internal fixation. Typically, three parallel screws are used in an inverted triangle configuration. Consider screw length, diameter, and partial vs. fully threaded options.
- Surgical Approach: Plan for potential need for open reduction if closed reduction attempts fail. The anterior approach (Smith-Petersen or modified Watson-Jones) is generally preferred for open reduction of femoral neck fractures, offering direct visualization and preservation of the blood supply.
Patient Positioning
-
Fracture Table vs. Radiolucent Operating Table:
- Fracture Table: Commonly used. Allows for controlled longitudinal traction and internal/external rotation of the leg, which aids in closed reduction. The contralateral leg is typically flexed and abducted to facilitate C-arm access.
- Radiolucent Operating Table: Offers more flexibility for open reduction and can be preferred if an open approach is anticipated or if complex reduction maneuvers are required that are difficult on a fracture table. Requires manual traction and positioning for fluoroscopy.
- Supine Position: The patient is placed supine.
- Traction: If using a fracture table, apply longitudinal traction to the injured leg. This helps to disimpact and align the fracture fragments.
- C-Arm Access: Ensure unrestricted C-arm access for both AP and lateral fluoroscopic views of the hip. The contralateral leg must be positioned out of the way (flexed and abducted on a well-padded leg holder) to permit adequate lateral imaging.
- Padding and Pressure Point Protection: Meticulously pad all bony prominences (heels, sacrum, ulnar nerves, peroneal nerves) to prevent pressure injuries.
- Sterile Preparation: Prepare and drape the entire hip, thigh, and pelvis, ensuring ample sterile field for potential open reduction and implant placement.
Reduction Maneuvers
Prior to skin incision, gentle closed reduction attempts are performed under fluoroscopic guidance.
*
Classic Leadbetter Maneuver:
While applying longitudinal traction, gently internally rotate the leg, abduct slightly, and then flex the hip. This sequence aims to disimpact the fracture, align the fragments, and correct varus and external rotation deformities common in displaced fractures.
*
Fluoroscopic Assessment:
Crucially, assess reduction quality using AP and lateral views.
*
AP View:
Look for restoration of the Shenton's line, equality of femoral head height, and correction of varus/valgus deformity.
*
Lateral View:
Assess for anterior or posterior displacement and correction of apex anterior/posterior angulation. Anatomic reduction is defined as less than 2mm of displacement and restoration of appropriate neck-shaft angle and anteversion.
*
Acceptable Reduction:
Anatomic reduction is paramount. If closed reduction is unsuccessful or deemed inadequate (e.g., >2mm displacement or significant angulation), an open reduction should be performed without delay. Repeated, forceful attempts at closed reduction should be avoided as they can further compromise the blood supply.
Detailed Surgical Approach / Technique
The goal of surgical technique for intracapsular hip fractures in young patients is urgent, anatomic reduction and stable fixation to maximize the chances of femoral head viability and prevent nonunion.
General Principles
- Urgency: As discussed, surgery ideally within 6-12 hours.
- Anatomic Reduction: This is the single most critical factor influencing the risk of AVN and nonunion. Any residual displacement or angulation significantly increases shear forces and vascular compromise.
- Stable Fixation: The chosen implant must provide sufficient stability to allow for early mobilization and fracture healing.
- Minimizing Soft Tissue Disruption: Efforts should be made to preserve the remaining blood supply to the femoral head, particularly the retinacular vessels.
Reduction Technique
-
Closed Reduction (Initial Attempt):
- With the patient on a fracture table, longitudinal traction is applied.
- The classic Leadbetter maneuver involves gentle hip flexion to 30-45 degrees, maximal internal rotation (often to 45 degrees), and then gentle abduction. This maneuver aims to disimpact the fracture, correct external rotation, and restore the neck-shaft angle.
-
Fluoroscopic Assessment:
Evaluate reduction on AP and lateral views.
- AP View: Restoration of Shenton's line, symmetrical femoral head height, and appropriate neck-shaft angle (125-135 degrees).
- Lateral View: Ensure no anterior or posterior displacement or angulation. The posterior cortex of the femoral neck should align with the posterior aspect of the femoral head.
- Acceptable Reduction: Less than 2mm displacement in any plane. If an anatomic or near-anatomic reduction is achieved, proceed with percutaneous fixation.
-
Open Reduction (if closed reduction fails):
- If closed reduction is inadequate after 2-3 gentle attempts, an open approach is indicated. Repeated forceful manipulations are detrimental to vascularity.
-
Approach Selection:
-
Anterior (Smith-Petersen or Modified Watson-Jones):
This is the preferred approach for open reduction of femoral neck fractures. It allows direct visualization of the fracture site, debridement of hematoma, and precise manipulation of fragments. It protects the posterior superior retinacular vessels, which are the primary blood supply.
- Incision: A straight or slightly curved incision is made from the ASIS distally along the sartorius muscle.
- Internervous Plane: Between the sartorius (femoral nerve) and tensor fascia lata (superior gluteal nerve). Deeper dissection proceeds between the rectus femoris (femoral nerve) and gluteus medius/minimus (superior gluteal nerve).
- Capsulotomy: A T-shaped or inverted-T capsulotomy allows for decompression of the intracapsular hematoma (critical for vascularity) and direct visualization of the fracture.
- Reduction: Direct manipulation with bone hooks or reduction clamps under direct vision. Ensure precise alignment of all fragments.
- Anterolateral (Modified Hardinge): Can also be used, splitting the gluteus medius.
- Posterolateral (Kocher-Langenbeck): Generally avoided for acute femoral neck fractures due to the risk of further damaging the posterior superior retinacular vessels and the greater muscle stripping required.
-
Anterior (Smith-Petersen or Modified Watson-Jones):
This is the preferred approach for open reduction of femoral neck fractures. It allows direct visualization of the fracture site, debridement of hematoma, and precise manipulation of fragments. It protects the posterior superior retinacular vessels, which are the primary blood supply.
Fixation Technique
The most common and effective method for internal fixation of intracapsular hip fractures in young patients is the use of multiple cannulated screws.
-
Fluoroscopic Guidance: All steps are performed under meticulous C-arm control, with frequent AP and lateral views.
-
Cannulated Screws (CS):
-
Number and Configuration:
Typically three 6.5mm or 7.3mm cannulated cancellous screws are used.
- Inverted Triangle Configuration: This provides optimal biomechanical stability against shear and rotational forces. One screw is placed centrally-inferiorly, and two screws are placed superiorly.
- Parallel Placement: The screws should be placed parallel to each other and parallel to the axis of the femoral neck, ending in the subchondral bone of the femoral head. This maximizes purchase and stability.
-
Entry Points:
The screws are typically inserted percutaneously through small stab incisions on the lateral femoral cortex, distal to the greater trochanter. The entry points are usually staggered to allow for proper spacing of the screw trajectories.
- Inferior Screw: Placed along the calcar femorale, often considered the primary weight-bearing screw. It should have good purchase in the dense bone of the calcar and subchondral bone.
- Superior Screws: Placed more anteriorly and posteriorly on the femoral neck, providing rotational stability.
-
Technique:
- Guide Wire Insertion: A K-wire is drilled from the lateral cortex into the femoral head, aiming for the desired trajectory. Confirm position with AP and lateral fluoroscopy. Crucial: The guide wire should be centrally placed in the femoral neck on both views and approximately 5-10mm from the articular surface in the femoral head.
- Repeat for all Wires: Insert all three guide wires. Ensure they are parallel and optimally positioned.
- Measurement: Measure the length of each guide wire to determine the appropriate screw length.
- Drilling/Tapping: Drill over the guide wires, and tap if using non-self-tapping screws, particularly in dense cortical bone.
- Screw Insertion: Insert the cannulated cancellous screws over the guide wires. The screws should be partially threaded, allowing for interfragmentary compression, or fully threaded if no compression is desired (e.g., if there is already good impaction). The threads should engage the femoral head without breaching the articular cartilage.
- Compression: Apply gentle compression by tightening the screws. Excessive compression can lead to collapse or loss of reduction, especially in comminuted fractures.
-
Final Fluoroscopic Check:
Confirm anatomic reduction and optimal screw placement on AP and lateral views, ensuring screws are not intra-articular and are of appropriate length.
- Image Interpretation: The image depicts an ideal inverted triangle configuration of three cannulated screws for internal fixation of a femoral neck fracture. Note the parallel placement, optimal engagement with the subchondral bone of the femoral head, and clear separation from the articular surface, ensuring maximum stability without iatrogenic joint damage.
-
Number and Configuration:
Typically three 6.5mm or 7.3mm cannulated cancellous screws are used.
-
Sliding Hip Screw (SHS) / Dynamic Hip Screw (DHS):
- Less commonly used for true intracapsular fractures in young patients due to the larger metalwork, potential for hardware prominence, and less ideal biomechanics for pure femoral neck fractures.
- May be considered in specific Pauwels Type III fractures with significant shear or comminution where greater stability is desired, or in fractures extending slightly into the trochanteric region. Requires careful surgical technique to avoid cutting out of the femoral head.
Capsular Management
After open reduction and fixation, the decision to close the capsule is debated.
*
Capsular Closure:
May help prevent adhesions and maintain a more physiological joint environment.
*
Leaving Capsule Open:
Some advocate leaving the capsule open to facilitate decompression and drainage of hematoma, which theoretically could reduce intracapsular pressure and improve blood flow. Current evidence does not definitively support one approach over the other for preventing AVN.
Complications & Management
Intracapsular hip fractures in young patients are associated with significant and often devastating complications, primarily due to the vulnerability of the femoral head's blood supply.
Common Complications
-
Avascular Necrosis (AVN) of the Femoral Head:
- Incidence: Highly variable, ranging from 10% to 80%. Influenced by initial displacement (Garden IV highest risk), time to surgery, quality of reduction, and surgical technique.
- Pathophysiology: Disruption of retinacular vessels (especially posterior superior branches), intracapsular hematoma leading to tamponade effect, and direct iatrogenic injury.
- Diagnosis: Early signs may be subtle. MRI is the gold standard for early detection (e.g., bone marrow edema, crescent sign). Radiographs show later stages (sclerosis, cystic changes, subchondral collapse, flattening of the femoral head).
-
Management:
- Non-operative: Protected weight-bearing, bisphosphonates (controversial, limited evidence).
- Early, Pre-collapse (Ficat Stage I/II): Core decompression (with or without bone grafting), vascularized fibula grafting (specialized technique, limited indications), osteotomies (e.g., valgus osteotomy, limited role).
- Late, Post-collapse (Ficat Stage III/IV): Total Hip Arthroplasty (THA) is the definitive treatment for symptomatic femoral head collapse, though challenging in young, active patients.
-
Nonunion:
- Incidence: 10-30%. Higher in displaced fractures, high Pauwels angles (Type III), inadequate reduction, poor fixation, and delayed surgery.
- Diagnosis: Persistent pain, limb shortening, inability to bear weight, progressive implant failure, and lack of radiographic healing >6 months post-op.
-
Management:
- Revision Internal Fixation: If the femoral head is still viable and there is potential for healing, revision with improved fixation (e.g., more stable construct, valgus osteotomy to convert shear to compression) and bone grafting (autograft or allograft) can be attempted.
- Total Hip Arthroplasty (THA): For established nonunion with femoral head collapse or when revision internal fixation is deemed unlikely to succeed, especially in the presence of AVN.
-
Malunion:
- Incidence: Variable, depends on reduction quality and stability of fixation.
- Diagnosis: Persistent pain, limp, leg length discrepancy, restricted range of motion, and radiographic evidence of residual angulation (e.g., varus or valgus deformity, excessive retroversion/anteversion).
-
Management:
- Conservative: Symptomatic management with physical therapy and activity modification.
- Corrective Osteotomy: For symptomatic malunion with significant deformity, an intertrochanteric osteotomy (e.g., valgus osteotomy for varus malunion) can restore biomechanics and offload damaged articular cartilage.
- Total Hip Arthroplasty (THA): For severe, symptomatic malunion with irreversible degenerative changes or failed osteotomy.
-
Infection:
- Incidence: Low (1-3%) with modern surgical techniques and prophylactic antibiotics.
- Diagnosis: Fever, wound erythema, purulent drainage, elevated inflammatory markers (ESR, CRP).
-
Management:
- Acute Infection (<4-6 weeks): Irrigation and debridement, retention of implants if stable, targeted antibiotics.
- Chronic Infection (>4-6 weeks): Usually requires implant removal, extensive debridement, and a staged approach (antibiotic spacer, delayed revision THA if indicated).
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: Varies, but hip fractures carry a high risk.
- Diagnosis: Swelling, pain in calf (DVT); dyspnea, chest pain, hypoxemia (PE).
- Management: Prophylactic anticoagulation (LMWH, fondaparinux, DOACs) for 4-6 weeks post-operatively. Early mobilization. Treatment with therapeutic anticoagulation for confirmed DVT/PE.
-
Hardware-Related Complications:
- Incidence: Variable.
- Examples: Screw prominence causing pain, articular penetration (iatrogenic AVN, cartilage damage), screw migration, breakage, or loosening.
- Management: Hardware removal if symptomatic, revision fixation, or arthroplasty depending on the underlying fracture status.
Complications & Salvage Strategies
| Complication | Incidence (Approx.) | Diagnosis | Salvage / Management Strategies ## Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following intracapsular hip fracture fixation in young patients is critical for promoting fracture union, recovering function, minimizing complications, and ultimately returning to pre-injury activity levels. The protocol is typically phased and adapted to individual patient progress and fracture stability.
Phase 1: Early Mobilization and Protected Weight-Bearing (Weeks 0-6/8)
- Goals: Protect fixation, control pain and swelling, initiate early range of motion (ROM), prevent deep vein thrombosis (DVT) and pneumonia.
-
Weight-Bearing (WB):
- Toe-Touch Weight-Bearing (TTWB) or Partial Weight-Bearing (PWB) (10-20% body weight): This is the standard for 6-8 weeks. The rationale is to provide micromotion believed to enhance osteogenesis while minimizing excessive shear or compressive forces that could displace the fracture or cause hardware failure.
- Assistive Devices: Walker or crutches are mandatory.
- Exceptions: In highly stable, impacted Garden I fractures with robust fixation, some surgeons may allow earlier, more aggressive PWB or even WBAT (Weight-Bearing As Tolerated), but this is less common for young patients where optimizing union and avoiding AVN is paramount.
-
Range of Motion (ROM):
- Early Gentle Active and Passive ROM: Begin within the first few days post-op. Focus on flexion, extension, abduction, and adduction within pain-free limits.
- Precautions: Avoid extreme hip flexion (>90 degrees), forced internal rotation (especially if an anterior approach was used), and excessive external rotation. The goal is to prevent stiffness without stressing the fracture site.
-
Strengthening:
- Isometric Exercises: Quadriceps sets, gluteal sets, ankle pumps. These help maintain muscle tone and promote circulation.
- Non-WB Exercises: Straight leg raises (SLR) in supine (if cleared by surgeon), hip abduction/adduction in side-lying (without resistance).
- Functional Mobility: Gait training with TTWB/PWB, transfer training (bed to chair), ascending/descending stairs (initially with supervision, step-to pattern).
- Pain Management: Multimodal approach including analgesics, nerve blocks, and cryotherapy.
- DVT Prophylaxis: Continue chemical prophylaxis and encourage ankle pumps.
Phase 2: Progressive Weight-Bearing and Strengthening (Weeks 6/8 - 12)
- Goals: Progress weight-bearing, improve hip strength and ROM, normalize gait pattern.
-
Weight-Bearing:
- Radiographic Assessment: Before advancing WB, obtain repeat AP/lateral radiographs to assess for early signs of fracture healing (e.g., callus formation, blurring of fracture line) and absence of implant failure or early AVN.
- Progressive Weight-Bearing (PWB to WBAT): Gradually increase weight-bearing to 50-75% of body weight, then transition to WBAT as pain allows and radiographic healing progresses.
- Assistive Devices: Wean from two crutches to one, then to a cane, as gait improves and strength allows.
- Range of Motion: Continue active and passive ROM exercises. Introduce gentle stretches to address any residual stiffness.
-
Strengthening:
- Resisted Exercises: Progress with resistance bands or light weights for hip flexion, extension, abduction, and adduction. Focus on gluteal strengthening (gluteus medius/maximus).
- Core Stability: Initiate core strengthening exercises to improve trunk stability, which is vital for hip function.
- Closed Chain Exercises: Mini-squats, leg presses (initially with minimal weight) to engage multiple muscle groups.
- Functional Training: Advance gait training to improve stride length and symmetry. Practice balance and proprioception exercises.
Phase 3: Advanced Strengthening and Return to Activity (Weeks 12+)
- Goals: Achieve full functional strength, restore full ROM, prepare for return to recreational and occupational activities, prevent re-injury.
- Weight-Bearing: Full weight-bearing without assistive devices.
-
Strengthening:
- High-Intensity Strengthening: Progress to advanced resistance exercises, incorporating functional movements.
- Plyometrics/Agility: If appropriate for the patient's pre-injury activity level and fracture healing, introduce light plyometric exercises and agility drills.
- Sport-Specific Training: For athletes, incorporate sport-specific drills and training activities under supervision.
- Impact Activities: Gradual reintroduction of higher impact activities (e.g., running, jumping) is typically deferred until 6-9 months post-op, assuming complete radiographic healing and no signs of AVN.
- Monitoring: Continued clinical and radiographic surveillance for signs of AVN, nonunion, or implant-related issues. MRI may be used to detect early AVN if clinically suspected.
General Considerations Throughout Rehabilitation:
- Pain Management: Continue to manage pain effectively to allow participation in therapy.
- Patient Education: Educate the patient on proper body mechanics, activity modification, and the importance of adherence to the protocol.
- Regular Clinical and Radiographic Follow-up: Essential to monitor fracture healing, detect complications early, and guide progression of rehabilitation. The risk of AVN is lifelong.
- Hardware Removal: Considered only if hardware is symptomatic (e.g., bursitis over screws) after fracture union is complete, typically 12-18 months post-op. It is not routinely performed.
Summary of Key Literature / Guidelines
The management of intracapsular hip fractures in young patients has been a subject of extensive research and evolving guidelines, primarily focused on mitigating the high rates of AVN and nonunion. Key themes include the urgency of intervention, the critical importance of anatomic reduction, and the role of stable fixation.
-
Time to Surgery:
- Numerous studies, including meta-analyses, consistently demonstrate a direct correlation between delayed surgical intervention and increased rates of AVN and nonunion.
- Kallio et al. (2009) and Karanth et al. (2010) , among others, highlighted that surgery performed within 6 hours significantly reduces the risk of AVN compared to delays beyond 24 hours. The consensus in the literature strongly advocates for surgery within 6-12 hours, with some extending to 24 hours, but earlier is always preferred when medically feasible. This window is believed to allow for decompression of the intracapsular hematoma and restoration of blood flow before irreversible ischemic damage occurs.
-
Quality of Reduction:
- Alho (1995) and subsequent authors emphasize that anatomic reduction (defined as less than 2mm displacement and restoration of proper neck-shaft angle) is paramount. Poor reduction is a significant independent predictor of both AVN and nonunion.
- Open reduction via an anterior approach (Smith-Petersen or modified Watson-Jones) is increasingly advocated when closed reduction is inadequate, as it allows for direct visualization, precise reduction, and decompression of the joint without further compromising the crucial posterior retinacular vessels.
-
Fixation Construct:
- Multiple Cannulated Screws (CS): Three parallel cannulated cancellous screws in an inverted triangle configuration are the gold standard for young patients. Biomechanical studies (e.g., Parker et al., 2004 ) have consistently shown this configuration to provide superior rotational and shear stability compared to two screws or a single sliding hip screw (DHS) for true intracapsular fractures. The screws should engage the subchondral bone of the femoral head and be placed along the calcar.
- Sliding Hip Screw (SHS/DHS): While effective for intertrochanteric fractures, DHS is less commonly preferred for true intracapsular fractures in young patients due to its bulk, larger osteotomy, and potential for excessive collapse and femoral head necrosis. It may be considered in specific Pauwels Type III fractures or for very proximal basilar neck fractures where increased stability against shear is desired.
- Fixed Angle Devices (e.g., angulated blade plates): Historically used, but largely supplanted by cannulated screws due to less invasive application and similar or superior biomechanical performance.
-
Role of Capsulotomy:
- The practice of capsulotomy to decompress the intracapsular hematoma and potentially improve femoral head perfusion has been debated. While some studies suggest a benefit, current evidence is not conclusive that it independently reduces the rate of AVN. However, in open reduction, capsulotomy is essential for direct visualization and precise reduction.
-
Pauwels Classification:
- The angle of the fracture line (Pauwels classification) remains a strong predictor of nonunion risk. High-angle (Type III) fractures are subject to greater shear forces and require robust fixation to resist collapse and promote healing. Some surgeons advocate for a valgus intertrochanteric osteotomy in conjunction with internal fixation for very high Pauwels angles to convert shear forces into compressive forces, though this is a more complex procedure.
-
Prevention of AVN:
- Beyond timely, anatomic reduction and stable fixation, other strategies, such as core decompression, vascularized fibula grafting, or bisphosphonate therapy, are primarily salvage procedures for early AVN, rather than primary prevention. Their prophylactic role in the acute setting is not established.
-
Rehabilitation:
- Most guidelines advocate for a period of protected weight-bearing (TTWB/PWB) for 6-12 weeks, followed by progressive weight-bearing based on radiographic evidence of healing. Premature unrestricted weight-bearing can lead to fracture collapse, nonunion, or loss of reduction.
In conclusion, key literature and clinical guidelines consistently reinforce that the optimal management for intracapsular hip fractures in young patients involves: expeditious surgical intervention, achievement of an anatomic reduction (ideally closed, but open if necessary), and stable internal fixation with multiple cannulated screws. Vigilant post-operative monitoring for AVN and nonunion, coupled with a structured rehabilitation program, is essential to maximize the chances of native hip preservation and optimize long-term functional outcomes in this challenging patient population.
You Might Also Like