Optimal Approaches to Treating Fractures: Faster Healing, Better Results

Key Takeaway
Looking for accurate information on Optimal Approaches to Treating Fractures: Faster Healing, Better Results? Approaches to treating fractures encompass traditional methods like immobilization via casts or surgery, alongside rehabilitation. Innovative options include Low-Intensity Pulsed Ultrasound (LIPUS) therapy, custom 3D-printed casts and implants, and Platelet-Rich Plasma (PRP) therapy. These advanced approaches aim to accelerate healing, minimize pain, and optimize patient outcomes by combining established and cutting-edge techniques.
Introduction & Epidemiology
Fractures represent a significant orthopedic burden, characterized by a structural discontinuity in bone integrity resulting from trauma, repetitive stress, or pathological processes. While historically defined by macroscopic bone disruption, a more granular understanding encompasses various classifications including open versus closed, simple versus comminuted, stable versus unstable, and intra-articular versus extra-articular injuries. The etiology is diverse, ranging from high-energy mechanisms (e.g., motor vehicle collisions, falls from height), low-energy trauma prevalent in osteoporotic populations, to stress fractures in athletes, and pathological fractures secondary to underlying disease processes.
Globally, fractures contribute substantially to morbidity, disability, and healthcare expenditure. The incidence of fractures varies significantly with age, sex, and geographical location. Pediatric fractures are common, often presenting unique challenges related to growth plate involvement and remodeling potential. In the adult population, long bone and periarticular fractures often result from high-energy trauma, leading to complex injury patterns. A substantial and increasing public health concern is the rising prevalence of fragility fractures, particularly in the aging demographic, largely driven by osteoporosis. Hip fractures, for instance, are associated with high mortality and significant long-term disability, underscoring the necessity for optimal management strategies. The evolving understanding of fracture biology and biomechanics, coupled with technological advancements, has propelled a paradigm shift from traditional methods of simple immobilization towards more sophisticated, biologically sensitive, and functionally oriented approaches aimed at achieving faster healing times and superior long-term functional outcomes.
Surgical Anatomy & Biomechanics
A comprehensive understanding of surgical anatomy and biomechanics is fundamental to optimal fracture management. Bone, as a complex composite material, exhibits distinct properties depending on its cortical and cancellous components. Cortical bone provides structural rigidity and strength, while cancellous bone offers excellent energy absorption and serves as a major site for metabolic activity and hematopoiesis. The vascular supply to bone, critical for healing, originates from both periosteal and medullary sources. The periosteal blood supply is particularly vital for cortical bone and is often compromised in high-energy trauma or extensive surgical dissection, necessitating approaches that minimize soft tissue stripping. The endosteal blood supply, derived from the medullary artery, is crucial for intramedullary bone healing.
The biomechanics of fracture healing dictates the choice of fixation strategy. Healing occurs through primary (direct) or secondary (indirect) bone healing. Primary healing, characterized by direct bone remodeling without callus formation, requires absolute stability and interfragmentary compression, typically achieved with lag screws or dynamic compression plates for simple fracture patterns. Secondary healing, involving external callus formation, occurs under conditions of relative stability and micro-motion, characteristic of intramedullary nailing or bridging plate osteosynthesis for comminuted fractures. Wolff's Law underscores the dynamic nature of bone remodeling, wherein bone adapts its structure in response to mechanical stresses, highlighting the importance of controlled loading during rehabilitation.
Specific anatomical considerations are paramount. For long bone diaphyseal fractures, rotational control and maintenance of length are critical. Periarticular fractures demand anatomical reduction of the articular surface to prevent post-traumatic arthritis, often requiring meticulous dissection and direct visualization. The concept of internervous planes is integral to modern surgical approaches, minimizing muscle and nerve damage, thereby facilitating early rehabilitation and preserving vascularity. Understanding these anatomical and biomechanical principles guides the selection of implants, dictates surgical approaches, and informs post-operative rehabilitation protocols, all contributing to optimized healing and functional restoration.
Indications & Contraindications
The decision-making process for fracture management, particularly regarding operative versus non-operative treatment, is multifaceted, influenced by fracture characteristics, patient factors, and available resources. The primary goal is to restore anatomical alignment, ensure stability, promote timely healing, and facilitate a rapid return to function while minimizing complications.
Non-Operative Indications
Non-operative management, typically involving closed reduction and external immobilization (casts, splints, braces), traction, or functional bracing, is generally reserved for:
*
Stable, minimally displaced fractures:
Where inherent stability of the fracture pattern is present, or stable reduction can be achieved and maintained.
*
Fractures in patients with prohibitive surgical risk:
Severe comorbidities, active infection at the surgical site (if not addressed), or general frailty where the risks of surgery outweigh the potential benefits.
*
Certain pediatric fractures:
Leveraging the significant remodeling potential of growing bones.
*
Stress fractures:
Often managed with rest and activity modification.
*
Select fractures in non-ambulatory patients:
Where restoration of full function is not a primary goal.
*
Patient preference:
After thorough discussion of risks, benefits, and alternatives, if a non-operative approach is deemed appropriate.
Operative Indications
Surgical intervention aims to achieve stable fixation, facilitate early mobilization, and optimize conditions for bone healing. Key indications include:
*
Unstable fractures:
Fractures that cannot be maintained in an acceptable reduction by non-operative means.
*
Displaced intra-articular fractures:
Requiring anatomical reduction to restore joint congruity and prevent post-traumatic arthritis.
*
Open fractures:
All open fractures are surgical emergencies requiring debridement and often internal or external fixation.
*
Fractures with neurovascular compromise:
Requiring urgent reduction and stabilization, sometimes necessitating exploration and repair of damaged structures.
*
Polytrauma patients:
Early definitive stabilization of long bone fractures (damage control orthopedics) to reduce systemic inflammatory response and improve outcomes.
*
Pathological fractures:
Often require robust fixation and sometimes adjuvant therapy (e.g., cement augmentation, oncological resection).
*
Impending skin compromise:
Severely displaced fractures threatening skin viability.
*
Failure of non-operative treatment:
Progressive displacement, intractable pain, or inability to achieve union.
*
Multiple fractures (floating joints):
To enable mobility and care.
*
Certain upper extremity fractures:
Where early functional return is paramount.
Contraindications
Absolute contraindications to surgery are rare and typically temporary:
*
Active infection at the surgical site:
Unless the surgery is specifically for infection control (e.g., debridement of an open fracture).
*
Extremely poor general health:
Uncontrolled sepsis, severe cardiac or respiratory instability, where the patient cannot physiologically tolerate anesthesia and surgery.
*
Prohibitive soft tissue injury:
Insufficient healthy soft tissue envelope for closure, severe crush injuries, or extensive degloving where delayed fixation is safer after soft tissue recovery.
Relative contraindications include severe underlying medical conditions that increase surgical risk, extreme osteoporosis precluding stable implant fixation, or patient non-compliance, which may jeopardize the success of surgical treatment. These are often managed on a case-by-case basis, weighing risks and benefits with the patient and multidisciplinary team.
| Operative Indications | Non-Operative Indications |
|---|---|
| Displaced intra-articular fractures | Stable, minimally displaced fractures |
| Open fractures (all grades) | Select pediatric fractures (high remodeling potential) |
| Unstable fractures (cannot be held by casting) | Fractures in patients with prohibitive surgical risk |
| Neurovascular compromise due to fracture | Stress fractures |
| Polytrauma with long bone or unstable pelvic fractures | Certain fractures in non-ambulatory patients |
| Pathological fractures requiring stabilization | Patient preference for non-operative management (if appropriate) |
| Impending skin necrosis due to fracture displacement | |
| Failure of adequate closed reduction or non-operative treatment | |
| Floating joints (e.g., ipsilateral femoral and tibial shaft fractures) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is a cornerstone of successful fracture surgery, minimizing intra-operative challenges and optimizing outcomes. This phase begins with a thorough patient assessment, including a detailed history, physical examination (neurovascular status, soft tissue integrity), and review of comorbidities and current medications (especially anticoagulants).
Imaging:
Standard orthogonal radiographs (AP and lateral views) are essential. Additional views (e.g., oblique, traction, stress views) may be required. For complex fractures, especially periarticular injuries, pelvic fractures, or those with significant comminution, a computed tomography (CT) scan is indispensable. CT with 3D reconstruction aids in understanding fracture morphology, articular involvement, and fragment orientation, facilitating precise surgical planning. Magnetic resonance imaging (MRI) may be indicated for suspected ligamentous injuries, occult fractures, or assessment of soft tissue pathology.
Surgical Plan Development:
1.
Fracture Classification:
Accurate classification (e.g., AO/OTA, Gustilo-Anderson) informs prognosis and treatment strategy.
2.
Reduction Technique:
Determine whether an open (direct visualization) or closed (indirect reduction using traction, ligamentotaxis, external fixators as reduction tools, or percutaneous clamps) technique will be employed.
3.
Implant Choice:
Select the appropriate implant type (e.g., intramedullary nail, dynamic compression plate, locking plate, external fixator, tension band wiring) based on fracture biomechanics, bone quality, and desired stability (absolute vs. relative). Plan for implant size, length, and screw trajectory.
4.
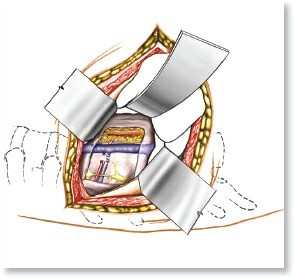
Surgical Approach:
Identify the optimal surgical approach, considering internervous planes, soft tissue preservation, and accessibility to the fracture site.
5.
Contingency Planning:
Anticipate potential intra-operative challenges such as difficult reduction, poor bone quality, or neurovascular injury, and plan alternative strategies.
6.
Templating:
Utilize digital or physical templates to pre-bend plates, determine implant length, and visualize screw placement, especially for complex or multi-fragmentary patterns.
Patient Positioning:
Correct patient positioning is crucial for surgical access, image intensifier (fluoroscopy) utilization, and patient safety.
*
Supine:
Common for lower extremity fractures (e.g., femur, tibia, ankle) and upper extremity fractures. Consideration for fracture tables for traction or specific maneuvers.
*
Prone:
Often used for posterior approaches to the spine, calcaneus, or proximal tibia.
*
Lateral Decubitus:
For hip fractures, shoulder fractures (beach chair position), or specific approaches to the tibia or fibula.
*
Beach Chair:
For shoulder and proximal humerus fractures.
Regardless of position, meticulous padding of pressure points, nerve protection, and careful draping to allow for necessary fluoroscopy arcs are paramount. Tourniquet application, if indicated, should be carefully planned for duration and pressure settings. The operating room setup must ensure all necessary instruments, implants, and fluoroscopy are readily available and in optimal positions.
Detailed Surgical Approach / Technique
Optimal fracture fixation techniques balance anatomical reduction, stable internal fixation, and preservation of the biological environment for healing.
General Principles of Open Reduction Internal Fixation (ORIF):
1.
Asepsis:
Strict adherence to sterile technique throughout the procedure is non-negotiable to minimize infection risk.
2.
Surgical Approach Selection:
* Approaches are chosen to provide adequate exposure while minimizing damage to neurovascular structures and soft tissues.
* Utilizing
internervous planes
(e.g., Deltopectoral for proximal humerus, anterolateral for distal tibia) allows for muscle retraction rather than transection, reducing bleeding, pain, and facilitating earlier recovery.
*
Minimally Invasive Plate Osteosynthesis (MIPO)
techniques are increasingly utilized, particularly for long bone fractures. These involve small incisions away from the fracture site, allowing for plate insertion submuscularly. This preserves periosteal blood supply, minimizes soft tissue stripping, and reduces surgical morbidity, aligning with biological osteosynthesis principles.
3.
Dissection:
Layer-by-layer dissection, with careful hemostasis and protection of vital structures, is performed. Blunt dissection is preferred over sharp where possible to minimize vascular and neural injury.
4.
Reduction Techniques:
*
Indirect Reduction:
Emphasized in MIPO and biological fixation strategies for comminuted fractures. Techniques include:
*
Ligamentotaxis:
Using continuous traction across intact soft tissues to approximate fragments, particularly useful for periarticular fractures.
*
Distraction/Compression:
Using external fixators or specific reduction clamps as temporary aids to restore length and alignment.
*
Joysticks:
K-wires inserted into main fragments for manipulation.
*
Image Intensifier Guidance:
Critical for closed reduction and percutaneous screw placement.
*
Direct Reduction:
For simple patterns or articular fractures requiring anatomical restoration. This involves direct visualization of fragments and their manipulation using pointed reduction clamps, bone hooks, or elevators. Interfragmentary compression is achieved with lag screws or dynamic compression plates.
5.
Fixation Principles:
*
Absolute Stability:
Achieved through interfragmentary compression (lag screws, DCPs) for simple, articular, or two-part fractures. This eliminates micro-motion at the fracture site, promoting primary bone healing.
*
Relative Stability:
Achieved with bridging plates, intramedullary nails, or external fixators for comminuted fractures. This allows for controlled micro-motion, which stimulates secondary bone healing and callus formation.
*
Intramedullary Nailing:
The preferred method for many diaphyseal long bone fractures (femur, tibia, humerus). Nails are load-sharing devices, providing relative stability and preserving periosteal blood supply, leading to faster healing and earlier weight-bearing. Reaming the canal can introduce autograft material, enhancing healing.
*
Locking Plate Technology:
Offers fixed-angle constructs, providing stability even in osteoporotic bone or comminuted fractures where conventional screw purchase is poor. Screws lock into the plate, creating a stable construct independent of plate-to-bone compression, acting as an internal fixator (biological plating).
*
External Fixation:
Primarily used for temporary stabilization in open fractures, highly contaminated wounds, severe soft tissue injuries (damage control orthopedics), or complex pelvic fractures. It can also be definitive in some situations.
6.
Bone Grafting:
* Indicated for large bone defects, segmental bone loss, or high-risk non-unions.
*
Autograft (iliac crest, proximal tibia):
Gold standard, providing osteoconductive, osteoinductive, and osteogenic properties.
*
Allograft (demineralized bone matrix, cancellous chips):
Osteoconductive and osteoinductive, but lacking osteogenic cells.
*
Bone graft substitutes (synthetic ceramics, polymers):
Primarily osteoconductive.
7.
Advanced Techniques & Adjuncts:
*
Computer-Assisted Navigation/Robotics:
For highly complex fractures (e.g., pelvic, acetabular, spinal), improving accuracy of screw placement and reduction.
*
3D Printing:
Used for creating patient-specific anatomical models for pre-operative planning, practicing complex reductions, or even fabricating custom surgical guides or implants for unique defects.
*
Low-Intensity Pulsed Ultrasound (LIPUS) and Pulsed Electromagnetic Fields (PEMF):
Non-invasive modalities demonstrated to accelerate fracture healing in some high-risk scenarios or established non-unions, primarily through modulation of cellular activity and signaling pathways involved in bone repair. These are typically applied post-operatively, as part of an integrated treatment strategy.
*
Biologics (BMPs, PRP):
Bone morphogenetic proteins (BMPs) have strong evidence for non-union treatment and fusion procedures. Platelet-rich plasma (PRP) has variable evidence but is being explored for its growth factor content in enhancing healing.
Wound Closure:
Meticulous layered wound closure is essential to prevent dead space, minimize hematoma formation, and achieve a healthy soft tissue envelope. Drains are used selectively. A sterile dressing is applied.
Complications & Management
Despite meticulous surgical technique and comprehensive pre-operative planning, complications can arise in fracture management, significantly impacting patient outcomes. Recognition, prevention, and timely management are critical.
| Complication | Incidence (General) | Salvage Strategy |
Post-Operative Rehabilitation Protocols
Optimal recovery from fracture often relies on effective post-operative rehabilitation protocols designed to accelerate bone healing, restore joint mobility, and regain functional strength. These protocols are individualized, evolving dynamically based on fracture characteristics, surgical stability, patient comorbidities, and individual progress.
Phase 1: Early Healing & Protection (Typically Weeks 0-6)
*
Goals:
Control pain and swelling, protect the surgical site and fixation, prevent complications (e.g., DVT, stiffness in adjacent joints).
*
Pain Management:
Multimodal approach including analgesics, ice, elevation.
*
Edema Control:
Elevation, gentle active range of motion (AROM) of uninvolved joints, compression dressings.
*
Weight-Bearing (WB) Status:
Strictly dictated by fracture type and fixation stability.
*
Non-Weight Bearing (NWB):
For unstable fixation, comminuted fractures, or early stages of some lower extremity fractures. Assistive devices (crutches, walker) are prescribed.
*
Touch-Down Weight Bearing (TDWB) or Partial Weight Bearing (PWB):
Gradual introduction of weight, guided by radiographic signs of healing and pain tolerance.
*
Weight-Bearing As Tolerated (WBAT):
For stable fixation (e.g., certain intramedullary nails) or upper extremity fractures where full WB is not applicable.
*
Range of Motion (ROM):
*
Protected or Passive ROM (PROM):
Initiated early for periarticular fractures to prevent arthrofibrosis, adhering to surgeon-defined arcs to protect fixation.
*
AROM:
For adjacent, uninvolved joints to prevent stiffness.
*
Muscle Activation:
Isometric exercises for muscles around the fracture site, without stressing the fixation. Gentle core stability exercises.
*
DVT Prophylaxis:
Continued as per institutional guidelines and patient risk factors.
Phase 2: Progressive Loading & Strengthening (Typically Weeks 6-12)
*
Goals:
Increase fracture stability, restore full ROM (or functional ROM), improve muscle strength, begin proprioceptive training.
*
Weight-Bearing Progression:
Gradually advance WB status as radiographic signs of healing progress and pain subsides. This is a critical stage for stimulating bone remodeling.
*
ROM Progression:
Advance from PROM to AROM and then to active-assisted ROM (AAROM) and resistive exercises within pain limits. Focus on restoring mobility to the affected joint(s).
*
Strengthening:
Introduce progressive resistance exercises for major muscle groups, initially with low resistance and high repetitions, gradually increasing intensity.
*
Proprioception & Balance:
Initiate exercises (e.g., single-leg stance, wobble board) to restore neuromuscular control, especially for lower extremity injuries.
*
Adjunctive Therapies:
For non-unions or high-risk cases,
Low-Intensity Pulsed Ultrasound (LIPUS)
or
Pulsed Electromagnetic Fields (PEMF)
may be continued or initiated to stimulate bone healing.
Phase 3: Functional Restoration & Return to Activity (Typically Weeks 12+ or after Union)
*
Goals:
Maximize strength, endurance, power, agility; return to pre-injury functional activities, work, or sport.
*
Advanced Strengthening:
High-resistance, high-intensity exercises, plyometrics (if appropriate).
*
Functional Training:
Sport-specific drills, job-specific tasks, agility training.
*
Endurance Training:
Cardiovascular conditioning.
*
Psychological Support:
Address fear of re-injury, provide encouragement.
*
Nutritional Support:
Optimize protein and micronutrient intake to support ongoing healing and muscle recovery.
*
Radiographic Monitoring:
Continue until clinical and radiographic union is confirmed.
*
Implant Removal:
Considered selectively, typically 12-24 months post-operatively, based on patient symptoms (pain, irritation), fracture location, patient age, and activity level.
Throughout all phases, close collaboration between the surgeon, physical therapist, occupational therapist, and the patient is paramount. Regular clinical and radiographic assessments guide progression, ensuring a safe and effective pathway to optimal recovery and preventing complications like malunion, non-union, or arthrofibrosis.
Summary of Key Literature / Guidelines
The field of fracture management is continuously evolving, driven by evidence-based medicine and technological innovation. Key literature and professional guidelines are critical for defining optimal approaches and ensuring consistent, high-quality patient care.
Core Principles & Foundational Literature:
1.
AO Foundation Principles:
The Arbeitsgemeinschaft für Osteosynthesefragen (AO) has been foundational in establishing principles of fracture management, emphasizing anatomical reduction of articular surfaces, stable internal fixation, preservation of blood supply, and early active mobilization. The AO comprehensive classification system provides a universal language for describing fractures.
2.
Biological Osteosynthesis:
A paradigm shift, championed by pioneers like Mast and Ganz, advocating for indirect reduction techniques and minimally invasive approaches (e.g., MIPO) to preserve the delicate soft tissue envelope and blood supply, thereby promoting secondary bone healing.
3.
Intramedullary Nailing:
Landmark studies have consistently demonstrated the superiority of intramedullary nailing for diaphyseal fractures of the femur and tibia over plating in terms of healing rates, complication profiles, and early weight-bearing. This technique is considered the gold standard for many long bone shaft fractures (e.g., Femoral and Tibial nailing).
4.
Locking Plate Technology:
Introduced in the late 1990s, locking plates (e.g., LCPs) have significantly expanded the indications for internal fixation, particularly in osteoporotic bone, metaphyseal and periarticular fractures, and highly comminuted patterns, offering stable, fixed-angle constructs independent of bone quality.
5.
Damage Control Orthopedics (DCO):
For multiply injured patients (polytrauma), early temporary stabilization with external fixators, followed by definitive fixation once the patient is physiologically stable, has been shown to reduce systemic inflammatory response and improve outcomes compared to immediate definitive fixation.
Professional Guidelines & Resources:
*
American Academy of Orthopaedic Surgeons (AAOS):
Publishes clinical practice guidelines (CPGs) for various fracture types, offering evidence-based recommendations for diagnosis, treatment, and rehabilitation (e.g., Management of Distal Radius Fractures, Hip Fractures).
*
Orthopaedic Trauma Association (OTA):
Focuses specifically on trauma care, providing educational resources, research, and expert consensus on complex fracture management.
*
Cochrane Reviews:
Systematic reviews that synthesize evidence from clinical trials, offering high-level evidence for the effectiveness of different interventions.
*
National Institutes of Health (NIH) Consensus Statements:
Provide expert opinion on challenging areas, such as the management of osteoporosis to prevent fragility fractures.
Emerging Technologies and Future Directions:
*
Advanced Biologics:
Research continues into the optimal use of bone morphogenetic proteins (BMPs), platelet-rich plasma (PRP), mesenchymal stem cells (MSCs), and gene therapy to augment bone healing, particularly in challenging non-unions or critical-sized defects. While BMP-2 has demonstrated efficacy in specific contexts (e.g., open tibial fractures), their routine use is still debated due to cost and potential side effects.
*
Personalized Medicine:
Leveraging genetic profiling and patient-specific factors to tailor treatment strategies and predict healing responses.
*
Robotics and Artificial Intelligence (AI):
AI-powered surgical planning, 3D printing of patient-specific guides and implants, and robotic-assisted navigation hold promise for enhancing precision, reducing surgical time, and improving outcomes for complex fractures.
*
Novel Imaging Techniques:
Advanced modalities for real-time intra-operative assessment of reduction and fixation quality.
*
Non-invasive Adjuvants:
Ongoing research aims to further elucidate the mechanisms and optimize the application of modalities like Low-Intensity Pulsed Ultrasound (LIPUS) and Pulsed Electromagnetic Fields (PEMF) to accelerate healing, especially in high-risk patients (e.g., smokers, diabetics, osteoporotics) or for recalcitrant non-unions. The current evidence supports their use primarily as adjuncts in these specific scenarios, rather than routine application across all fractures.
In conclusion, optimal fracture management is a dynamic interplay of sound anatomical knowledge, biomechanical principles, meticulous surgical technique, evidence-based decision-making, and individualized post-operative rehabilitation, continually refined by advancements in research and technology.
You Might Also Like