Developmental Dysplasia of the Hip (DDH): History, Epidemiology & Surgical Anatomy
Key Takeaway
Developmental Dysplasia of the Hip (DDH) encompasses a spectrum of hip abnormalities, from subtle dysplasia to full dislocation. Its comprehension spans ancient recognition to modern understanding, integrating epidemiology, key risk factors like breech presentation, and a detailed surgical anatomy of bony structures, ligaments, and muscles crucial for effective management.
Introduction & Epidemiology
The understanding and management of hip dysplasia, particularly Developmental Dysplasia of the Hip (DDH), have evolved from ancient observations of a disabling condition to a sophisticated discipline integrating advanced diagnostics, surgical techniques, and rehabilitative protocols. Historically, the manifestations of a dislocated hip were recognized for millennia. Hippocrates (460–357 BC) documented the severe disability associated with hip dislocation, demonstrating early clinical recognition without a comprehensive etiological understanding. Archaeological evidence, such as a dysplastic hip specimen from Neolithic times housed in the British Museum and Hellenistic bronze figurines depicting congenital dislocation, further attests to the long-standing presence of this condition in human populations.
For centuries, hip dislocations were broadly categorized as either accidental (traumatic) or spontaneous (symptomatic of other underlying pathologies). It was Guillaume Dupuytren (1777–1835) who introduced the pivotal concept of "original or congenital dislocation," recognizing a primary failure of fetal hip development as a distinct entity, though he considered it incurable. This landmark classification paved the way for distinguishing congenital developmental issues from acquired dislocations. The term "congenital dislocation of the hip" was later broadened to "Developmental Dysplasia of the Hip" (DDH) to encompass a spectrum ranging from subtle acetabular dysplasia to irreducible dislocation, acknowledging the potential for postnatal development or worsening of the condition.
DDH represents a spectrum of abnormalities affecting the developing hip, encompassing acetabular dysplasia, subluxation, and frank dislocation. The common pathological denominator is an inadequate coverage of the femoral head by the acetabulum, leading to abnormal joint mechanics and, if untreated, progressive degeneration culminating in premature osteoarthritis.
Epidemiology:
The incidence of DDH varies globally, with reported rates ranging from 1 to 3 cases per 1,000 live births for dislocation, and up to 10-15 per 1,000 for milder forms of dysplasia. Significant risk factors include:
*
Female sex:
Approximately 80% of affected individuals are female, potentially due to hormonal influences (e.g., maternal relaxin).
*
Firstborn status:
Attributed to tighter uterine constraints.
*
Breech presentation:
Especially frank breech, increasing the risk 8-10 fold due to sustained hip flexion and knee extension.
*
Positive family history:
A strong genetic predisposition is recognized, with a 10-fold increased risk if a first-degree relative was affected.
*
Oligohydramnios:
Limited amniotic fluid can contribute to compressive forces on the developing fetus.
*
Swaddling practices:
Improper swaddling that restricts hip abduction and extension has been implicated in increasing DDH incidence in some populations.
Left hip involvement is slightly more common than the right, and bilateral involvement occurs in approximately 20-30% of cases. Early detection through universal screening (clinical examination: Ortolani and Barlow maneuvers in neonates) and selective imaging (ultrasonography in infants, radiography in older children) is critical to optimize treatment outcomes and minimize the need for complex surgical interventions.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the hip joint is paramount for the effective management of DDH. The hip is a diarthrodial ball-and-socket joint, designed for stability and mobility.
Bony Anatomy:
*
Acetabulum:
Formed by the fusion of the ilium, ischium, and pubis. In DDH, the acetabulum is typically shallow, anteverted, and/or poorly developed (dysplastic), leading to insufficient femoral head coverage. Key radiographic parameters include the acetabular index, center-edge (CE) angle of Wiberg, and anterior/posterior coverage.
*
Femoral Head and Neck:
The femoral head should be spherical and centered within the acetabulum. In DDH, the femoral head may be hypoplastic, flattened, or develop a false acetabulum. The femoral neck often exhibits increased anteversion (normal 10-15 degrees) and valgus deformity.
*
Pelvis:
The overall pelvic morphology influences acetabular orientation.
Capsuloligamentous Structures:
*
Joint Capsule:
In DDH, particularly with dislocation, the capsule becomes elongated, thickened, and constricted, forming an hourglass constriction that can impede reduction. The hypertrophied ligamentum teres is also a barrier to reduction.
*
Iliofemoral Ligament (Y-ligament of Bigelow):
The strongest ligament, preventing hyperextension.
*
Pubofemoral and Ischiofemoral Ligaments:
Contribute to overall joint stability.
Musculature:
*
Abductors (Gluteus Medius, Minimus, Tensor Fascia Lata):
Crucial for gait stability and pelvic control. Their function is compromised in dysplastic hips due to altered biomechanics and potentially atrophy.
*
Adductors (Pectineus, Adductor Longus, Brevis, Magnus, Gracilis):
Often spastic and contracted in DDH, hindering hip abduction and reduction. An adductor tenotomy is frequently performed to facilitate reduction.
*
Iliopsoas:
The primary hip flexor. Its tendon can be hypertrophied and act as a mechanical block to reduction, necessitating tenotomy or lengthening.
Neurovascular Structures:
*
Femoral Nerve:
Lies anterior to the hip joint, susceptible to injury during anterior approaches or excessive traction.
*
Sciatic Nerve:
Lies posterior to the hip joint, at risk during posterior approaches or during reduction maneuvers.
*
Lateral Femoral Cutaneous Nerve:
Superficial, often encountered and at risk during anterior-lateral approaches (e.g., Smith-Petersen, Ganz PAO).
*
Femoral Artery and Vein:
Medial to the femoral nerve, vital structures.
Biomechanics of Dysplasia:
The primary biomechanical deficit in DDH is insufficient femoral head coverage, leading to:
*
Increased Contact Stress:
The reduced contact area between the femoral head and acetabulum concentrates stress on a smaller cartilage surface, accelerating wear and degeneration.
*
Joint Instability:
Poor bony containment allows for abnormal translation and subluxation, especially during weight-bearing.
*
Abnormal Muscle Function:
Altered lever arms and muscle lengths result in compensatory muscle activity, leading to fatigue, pain, and abnormal gait (e.g., Trendelenburg gait).
*
Progression to Osteoarthritis:
Chronic abnormal loading and instability inevitably lead to progressive articular cartilage damage and premature osteoarthritis, often decades earlier than in healthy hips.
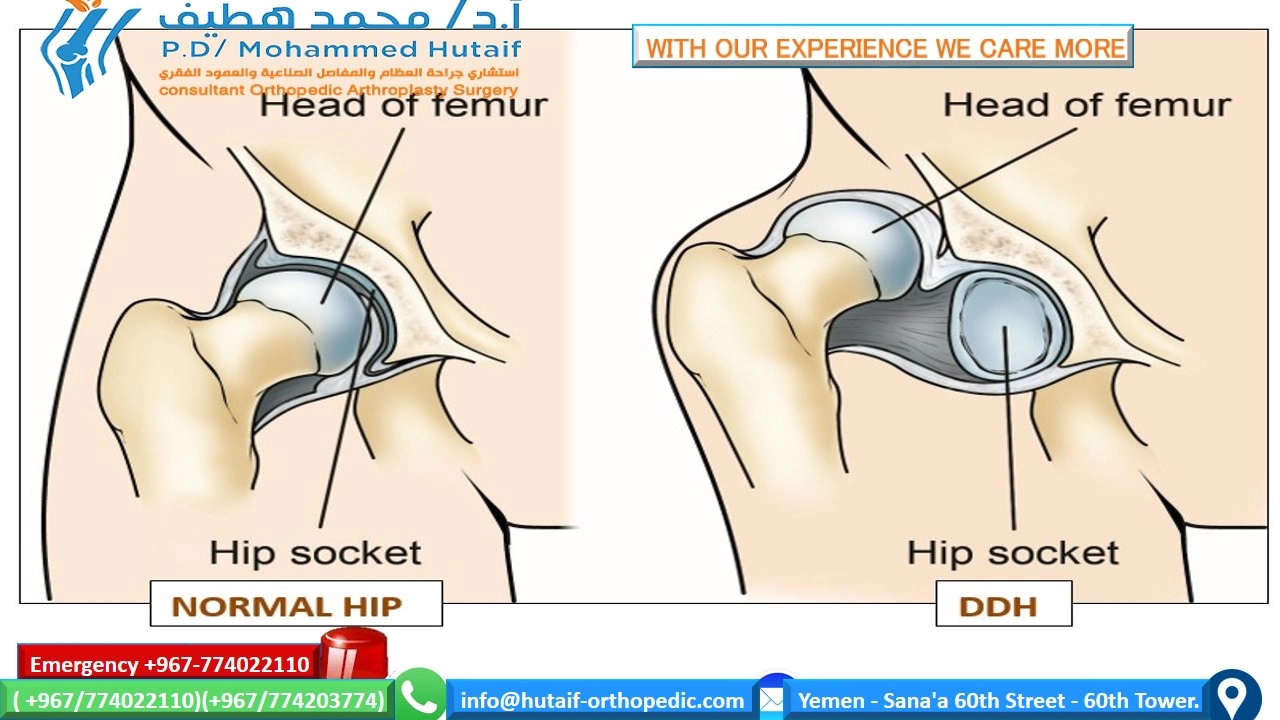
Illustrative image of a normal hip joint versus a dysplastic or dislocated hip joint, highlighting key anatomical differences and altered biomechanics.
Indications & Contraindications
The decision-making process for the treatment of DDH is complex, guided by the patient's age, severity of dysplasia, reducibility of the hip, and the presence of associated deformities. Treatment options range from observation to extensive surgical reconstruction.
Non-Operative Indications
Non-operative management is primarily indicated for infants and young children, relying on external orthoses to maintain hip reduction and facilitate proper acetabular development.
-
Pavlik Harness:
- Indications: Infants from birth to approximately 6 months of age with reducible hip subluxation or dislocation (Ortolani positive, Barlow positive). It is most effective when initiated early.
- Mechanism: Maintains the hips in flexion (90-110 degrees) and abduction (40-60 degrees) while allowing hip motion, thereby promoting acetabular molding.
-
Abduction Orthoses (e.g., Tübingen, Frejka Pillow, various custom braces):
- Indications: Often used for infants between 6-18 months of age, or as a step-down from the Pavlik harness for milder dysplasia. Also suitable for older infants where the Pavlik harness fails or is contraindicated.
- Mechanism: Provides rigid immobilization in abduction and flexion, aiming to centralize the femoral head.
-
Closed Reduction and Spica Cast Immobilization:
- Indications: Unreducible or unstable hips in infants generally between 6-18 months, or older infants (up to 2 years) who fail Pavlik harness treatment. Performed under general anesthesia.
- Mechanism: Manual reduction of the femoral head into the acetabulum, followed by immobilization in a spica cast (usually in a "human position" of 90 degrees flexion, 45 degrees abduction, and neutral rotation) to maintain reduction. Arthrography is often used to confirm concentric reduction.
Operative Indications
Surgical intervention becomes necessary when non-operative methods fail, or for older children, adolescents, and young adults where the underlying pathology requires bony realignment or reconstruction.
-
Open Reduction:
- Indications: Failure of closed reduction, irreducibility due to soft tissue interposition (e.g., hypertrophied ligamentum teres, inverted labrum, constricted capsule, iliopsoas tendon), patients older than 18-24 months at presentation, or significant residual dysplasia after closed reduction.
-
Pelvic Osteotomies:
Aim to reorient the acetabulum to improve femoral head coverage.
- Redirectional Osteotomies (e.g., Salter Innominate Osteotomy): For children typically 18 months to 8 years old with mild-moderate residual acetabular dysplasia. It involves a single cut through the ilium, moving the entire acetabulum anteriorly, laterally, and inferiorly.
- Reshaping Osteotomies (e.g., Dega, Pemberton Osteotomy): For children between 1.5 and 8-10 years with significant acetabular deficiency, often with an open triradiate cartilage. They reshape the acetabulum by creating an osteotomy that hinges on the triradiate cartilage.
- Triple Innominate Osteotomy (Sutherland/Steel): For older children (8-12 years) with residual dysplasia, allowing for more substantial acetabular repositioning compared to Salter. Involves osteotomies of the ilium, ischium, and pubis.
- Periacetabular Osteotomy (PAO) of Ganz: The gold standard for symptomatic acetabular dysplasia in adolescents and young adults with open or recently closed triradiate cartilage, and no significant osteoarthritis. It allows multiplanar correction of the acetabulum while preserving the posterior column and blood supply to the acetabular fragment.
-
Femoral Osteotomies:
Address femoral deformities often co-existent with DDH.
- Proximal Femoral Varus Derotation Osteotomy (VDRO): Indicated for excessive femoral anteversion, coxa valga, or to improve stability after reduction in younger children.
- Femoral Shortening Osteotomy: Often performed concurrently with open reduction in older children (e.g., >2 years) to reduce tension on neurovascular structures, facilitate reduction, and decrease the risk of AVN by reducing intra-articular pressure.
Contraindications
-
Absolute Contraindications to Surgery:
- Severe medical comorbidities precluding safe anesthesia.
- Established severe osteoarthritis or avascular necrosis precluding salvage (may instead indicate Total Hip Arthroplasty (THA)).
- Non-ambulatory patients with cerebral palsy or other neuromuscular disorders without pain, where the dislocation is not causing functional limitations or skin breakdown (conservative management may be preferred).
-
Relative Contraindications:
- Active infection.
- Skeletal immaturity (for certain osteotomies, though many are designed for growing skeletons).
- Patient non-compliance with post-operative protocols.
Operative vs. Non-Operative Indications Summary Table
| Intervention | Primary Indication | Patient Age Range (Typical) | Key Considerations |
|---|---|---|---|
| Non-Operative | |||
| Pavlik Harness | Reducible hip subluxation/dislocation (Ortolani/Barlow positive) | 0-6 months | Early initiation, parent compliance, skin care, frequent follow-up. |
| Abduction Orthosis | Mild dysplasia, residual instability post-Pavlik, failure of Pavlik or contraindication for it | 6-18 months | More rigid than Pavlik, less motion allowed. |
| Closed Reduction + Spica Cast | Unreducible/unstable hip in older infants, failure of Pavlik, 1st line for late presentations | 6-24 months | General anesthesia, arthrography for confirmation, meticulous casting, AVN risk, strict follow-up. |
| Operative | |||
| Open Reduction | Failure of closed reduction, irreducibility due to soft tissue block, older children | > 18-24 months | Often combined with femoral shortening, capsulorrhaphy. |
| Salter Osteotomy | Mild-moderate residual acetabular dysplasia, stable reduction | 1.5-8 years | Single iliac cut, relatively less invasive, good for anterior/lateral coverage. |
| Dega/Pemberton Osteotomy | Significant acetabular deficiency, especially anterior/lateral, open triradiate cartilage | 1.5-10 years | Targets anterior/lateral acetabular rim, hinges on triradiate. |
| Triple Innominate Osteotomy | Residual dysplasia in older children, more severe deficiencies, closed triradiate | 8-12 years | More complex, provides greater reorientation than Salter. |
| Periacetabular Osteotomy (PAO) | Symptomatic acetabular dysplasia, preserved joint space, absence of significant osteoarthritis | Adolescents-Young Adults | Multiplanar correction, preserves posterior column, technically demanding. |
| Proximal Femoral Osteotomy | Excessive femoral anteversion, coxa valga, concomitant with open reduction for stability/AVN risk | Variable (often with open reduction or PAO) | Corrects femoral geometry, reduces intra-articular pressure. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and careful patient positioning are essential for successful outcomes in DDH surgery, minimizing complications and optimizing surgical efficiency.
Pre-Operative Planning
-
Clinical Assessment:
- Comprehensive physical examination, including assessment of range of motion, limb length discrepancy, gait, and neurovascular status.
- Detailed patient history, including previous treatments and associated medical conditions.
-
Imaging Studies:
- Plain Radiographs: Anteroposterior (AP) pelvis with hips in neutral rotation is standard. False profile and Dunn views may be helpful for assessing anterior and posterior coverage. Parameters like CE angle, Tönnis angle, acetabular index, and femoral head coverage are measured.
- CT Scan with 3D Reconstruction: Indispensable for complex cases, especially for PAO. Provides detailed information on acetabular morphology, femoral anteversion, true joint space, and osteotomy trajectories. Crucial for templating screw placement and osteotomy cuts.
- MRI/MR Arthrography: Useful for evaluating soft tissue constraints (labrum, ligamentum teres, capsule, psoas), assessing articular cartilage health, and detecting early avascular necrosis (AVN).
- Ultrasound: Primarily for infants for dynamic assessment of hip stability and acetabular morphology (Graf classification).
-
Surgical Templating:
- Using radiographs and CT scans, the desired degree of acetabular correction (e.g., increasing CE angle, decreasing Tönnis angle) is templated.
- For PAO, the target orientation of the acetabular fragment and planned screw trajectories are marked.
- For femoral osteotomies, the degree of varus, valgus, or derotation is determined.
-
Equipment and Instrumentation:
- Ensure availability of specialized instruments for osteotomies (e.g., specific osteotomes, oscillating saws, retractors for deep pelvic dissection, specific screw sets).
- Fluoroscopy unit (C-arm) and image intensifier are mandatory for intraoperative confirmation of reduction and osteotomy placement.
- Blood products should be cross-matched and available, especially for extensive procedures like PAO or open reduction in older children.
- Spica casting material should be prepared if a spica cast is part of the post-operative protocol.
-
Anesthesia Consultation:
- Pre-operative evaluation of the patient's suitability for prolonged anesthesia and potential blood loss.
- Epidural or regional nerve blocks may be considered for post-operative pain management.
Patient Positioning
Patient positioning depends heavily on the chosen surgical approach.
-
Supine Position:
- Common for: Anterior approaches (e.g., Smith-Petersen for open reduction), Ganz PAO, Salter osteotomy.
- Setup: Patient supine on a radiolucent operating table. Ensure adequate padding at pressure points.
-
Key Considerations:
- Traction: A traction table may be used, particularly for PAO, to facilitate distraction of the hip joint, aid in osteotomy performance, and protect neurovascular structures. The unoperated leg is often suspended in a well-padded boot, while the operated leg is draped free or placed in traction.
- Fluoroscopy Access: The C-arm must have unrestricted access for AP, lateral, and oblique views of the hip and pelvis. This often requires placing a bump under the contralateral hip or ensuring the table is sufficiently narrow.
- Neurovascular Protection: Careful positioning to avoid compression of the brachial plexus, ulnar nerve, and common peroneal nerve. The lateral femoral cutaneous nerve (LFCN) is particularly vulnerable during anterior-lateral approaches to the hip/pelvis.
- Draping: Standard sterile preparation and draping, allowing access to the entire hip and lateral thigh.
-
Lateral Decubitus Position:
- Less common for DDH: May be used for specific posterior approaches or combination approaches, but generally not preferred for the primary corrective osteotomies for dysplasia.
- Setup: Patient on their side, with the affected hip superior. Pillows or blankets for stabilization.
- Key Considerations: Careful attention to protecting the contralateral limb and neurovascular structures.
For PAO, the supine position is standard. The patient is placed close to the edge of the operating table to allow for maximum fluoroscopy access. A sacral bump may be used. The anterior superior iliac spine (ASIS) is typically the most prominent bony landmark.
Detailed Surgical Approach / Technique
Given the breadth of DDH surgeries, we will detail a representative modern approach for residual acetabular dysplasia in adolescents/young adults: the Periacetabular Osteotomy (PAO) of Ganz , often considered the treatment of choice for symptomatic acetabular dysplasia with preserved joint space. This procedure is technically demanding and requires meticulous execution.
Periacetabular Osteotomy (PAO) of Ganz
Principle: The PAO involves creating osteotomies around the acetabulum, detaching the acetabular fragment from the rest of the pelvis, and then rotating it to achieve better femoral head coverage. Crucially, the posterior column and the blood supply to the acetabulum are preserved.
1. Incision and Initial Dissection:
*
Anterior-Lateral Approach:
A modified Smith-Petersen or bikini incision is typically used, extending from the iliac crest towards the ASIS, and then curving distally and posteriorly along the tensor fascia lata. This allows for excellent exposure while minimizing soft tissue damage.
*
Layered Dissection:
* Incision through skin and subcutaneous tissue.
* Careful identification and protection of the
lateral femoral cutaneous nerve (LFCN)
, which typically exits beneath the inguinal ligament, medial to the ASIS. It can be found passing over or through the sartorius muscle.
* The fascia of the sartorius muscle is incised, and the muscle is mobilized medially.
* The interval between the
sartorius muscle (medially)
and the
tensor fascia lata (laterally)
is developed. This is the superficial part of the internervous plane (femoral nerve to sartorius, superior gluteal nerve to TFL).
* Deep to the sartorius, the
rectus femoris muscle
is identified. Its direct and reflected heads are detached from the ASIS and supra-acetabular region, respectively, and retracted medially. This exposes the anterior capsule and the ilium.
* The
iliopsoas muscle
(supplied by the femoral nerve) is identified and retracted medially. The neurovascular bundle (femoral nerve, artery, vein) lies posteromedial to the iliopsoas and must be meticulously protected.
2. Identification of Osteotomy Sites and Initial Cuts:
* The primary osteotomies are performed in the ilium, ischium, and pubis.
*
Iliac Osteotomy:
* The outer table of the ilium is exposed above the hip joint. A curved osteotomy is initiated from just above the ASIS, directed posteriorly towards the anterior superior iliac spine. The trajectory then curves distally and posteriorly, parallel to the superior acetabular rim, aiming towards the posterior inferior iliac spine, but staying anterior to the sacroiliac joint. This cut is critical and defines the superior border of the acetabular fragment. It should be deep enough to enter the cancellous bone but
not
penetrate the inner cortical table at this stage.
* The cut should be curvilinear, passing through the outer cortex and spongiosa, avoiding the sacroiliac joint.
*
Ischial Osteotomy:
* The patient's hip is flexed to 90 degrees and internally rotated, and the adductors are retracted to expose the inferior aspect of the acetabulum.
* The ischium is approached via the interval between the adductor longus and pectineus muscles.
* The ischial osteotomy is typically performed just distal to the acetabulum, aiming for the greater sciatic notch. This cut is usually blind and requires careful tactile guidance and fluoroscopy to ensure it does not injure the sciatic nerve. An osteotome is advanced along the inferior pubic ramus toward the ischial tuberosity, and then curved superiorly towards the lesser sciatic notch.
*
Pubic Osteotomy:
* The superior pubic ramus is exposed by retracting the iliopsoas and neurovascular bundle medially.
* The pubic osteotomy is performed horizontally through the superior pubic ramus, approximately 2-3 cm medial to the acetabulum, using an oscillating saw or osteotome.
3. Completion of Osteotomies and Mobilization:
*
Completion of Iliac Osteotomy:
The inner table of the ilium is carefully osteotomized from within the lesser pelvis using curved osteotomes, under direct visualization or with tactile feedback to ensure complete detachment. This is the most technically challenging and critical step. The surgeon must hug the bone to protect the contents of the lesser pelvis (iliac vessels, femoral nerve). The cut propagates posteriorly, connecting with the ischial osteotomy, and superiorly, completing the circumference of the acetabular fragment.
*
Mobilization:
Once all osteotomies are complete, the acetabular fragment, along with its attached femoral head (if reduced), is carefully mobilized using a bone hook or laminar spreader. The aim is to free it completely, allowing multiplanar repositioning.
*
Capsulotomy/Labral Repair (if indicated):
If there are intra-articular pathologies such as a hypertrophied labrum or ligamentum teres that are preventing optimal reduction or repositioning, these may be addressed at this stage. Labral tears are often repaired.
4. Repositioning and Fixation:
* The acetabular fragment is now rotated to achieve optimal femoral head coverage. This typically involves:
*
Lateralization:
Moving the acetabulum laterally to increase coverage.
*
Anteriorization:
Moving the acetabulum anteriorly to cover anterior deficiency.
*
Distalization:
Lowering the acetabular rim.
*
Intraoperative Fluoroscopy:
Critical to confirm the desired correction in AP, false profile, and lateral views. The CE angle should be improved to acceptable values (e.g., >25-30 degrees).
*
Fixation:
Once the optimal position is achieved, the acetabular fragment is secured to the stable posterior column and ilium with 2-4 cortical screws. The screws should be bicortical, carefully placed to avoid joint penetration or neurovascular injury.
5. Wound Closure:
* Thorough irrigation of the surgical site.
* Reattachment of the rectus femoris muscle.
* Closure of the tensor fascia lata and sartorius fascia.
* Subcutaneous and skin closure.
* A drain may be placed temporarily.
Adjunct Procedures:
*
Adductor Tenotomy:
Often performed prior to open reduction or PAO if adductor spasticity is significant, to facilitate hip abduction and reduce tension.
*
Femoral Shortening/Derotation Osteotomy:
May be performed simultaneously, particularly in older children with irreducible hips, to reduce tension on the joint and neurovascular structures, or to correct excessive femoral anteversion or coxa valga.
Complications & Management
Surgical interventions for DDH carry potential risks. Awareness of these complications, their incidence, and appropriate management strategies is crucial for all orthopedic surgeons.
Common Complications in DDH Surgery
| Complication | Incidence (Approximate) | Salvage Strategies / Management ## Hip Dysplasia Disease History: From Mystery to Modern Understanding
The journey of understanding Developmental Dysplasia of the Hip (DDH) reflects a progressive shift from ancient, generalized observations of disability to contemporary, sophisticated insights into its etiology, biomechanics, and comprehensive management. This evolution has been marked by pivotal clinical descriptions, anatomical discoveries, and technological advancements, culminating in a multidisciplinary approach that seeks to prevent long-term morbidity.
Early Recognition and Conceptualization (Pre-18th Century)
For millennia, the conspicuous disability arising from a dislocated hip was acknowledged across various civilizations. Hippocrates (460–357 BC), widely regarded as the "Father of Medicine," provided remarkably accurate clinical descriptions of hip dislocations in his treatise "On Joints." He meticulously detailed the clinical presentation and attempts at reduction, underscoring the ancient world's awareness of the condition's debilitating effects. His writings, though lacking an understanding of congenital origins, represent an early form of clinical documentation that persisted for centuries.
Archaeological and artistic evidence further corroborates the historical presence of hip dysplasia. A specimen of a dysplastic hip from the Neolithic period, now housed in the British Museum, indicates its prehistoric prevalence. Similarly, bronze figurines from the Hellenistic era depicting individuals with congenital dislocations suggest that the condition was not merely observed clinically but also artistically represented. Despite this widespread recognition of the "infantile dislocated hip" in the Mediterranean world by the end of the first millennium BC, its etiology remained largely a mystery, often attributed to trauma, disease, or even supernatural causes rather than a developmental abnormality.
Emergence of a Distinct Pathological Entity (18th - 19th Century)
The transition from a generalized understanding of "dislocation" to the specific identification of a "congenital" form began in the Age of Enlightenment. Prior to this, hip dislocations were broadly categorized as accidental (traumatic) or spontaneous (secondary to infectious, inflammatory, or neoplastic processes).
In France, Nicolas Andry (1658–1742), a pioneer in orthopedics, mentioned hip conditions in his influential work, "Orthopaedia, or the Art of Correcting and Preventing Deformities in Children," though without fully distinguishing the congenital variant.
The pivotal breakthrough came with Guillaume Dupuytren (1777–1835), a renowned French surgeon and anatomist. Dupuytren, through meticulous anatomical dissections and clinical observations, described a unique category of hip dislocation that he termed "original or congenital dislocation." He correctly attributed this to a failure of fetal hip development, distinguishing it clearly from traumatic or acquired forms. This represented a profound conceptual shift, moving away from an etiological vacuum towards a primary developmental defect. While Dupuytren recognized its congenital nature, he considered the condition incurable, reflecting the limited therapeutic options of his time. His work laid the fundamental groundwork for future investigations into the pathogenesis and management of what would later be termed Developmental Dysplasia of the Hip.
The Era of Anatomical and Pathological Understanding (Late 19th - Early 20th Century)
Following Dupuytren, subsequent clinicians and anatomists delved deeper into the specific pathological changes associated with congenital hip dislocation. Important figures like Adolf Lorenz (1854–1946) championed non-operative treatments, including manual reduction and plaster casting, pushing the boundaries of what Dupuytren considered incurable. Lorenz’s "bloodless reduction" techniques, though not always successful and often associated with complications like avascular necrosis, represented a significant therapeutic endeavor.
The early 20th century saw increased recognition of the spectrum of conditions, from mild acetabular dysplasia to complete dislocation. Imaging, initially with simple radiographs, allowed for a clearer visualization of the bony abnormalities, providing objective criteria for diagnosis and assessment of treatment outcomes. However, the exact mechanisms of development and the interplay of genetic and environmental factors remained largely obscure.
Modern Understanding: Etiology, Screening, and Management (Mid-20th Century to Present)
The latter half of the 20th century witnessed an explosion in the understanding and management of DDH, driven by advancements in imaging, surgical techniques, and a more nuanced appreciation of joint biology.
- Etiological Factors: The concept of DDH shifted from "congenital" (implying present at birth) to "developmental" to encompass the potential for the hip to be normal at birth and subsequently develop dysplasia, or for existing dysplasia to improve or worsen. Genetic predisposition, hormonal influences (e.g., maternal relaxin), mechanical factors (e.g., breech presentation, oligohydramnios, uterine constraint), and postnatal swaddling practices were identified as key contributors.
- Screening and Early Diagnosis: The importance of universal clinical screening using the Ortolani and Barlow maneuvers in neonates became standard practice. The advent of ultrasonography by Graf in the 1980s revolutionized early diagnosis, allowing dynamic, radiation-free assessment of acetabular morphology and femoral head coverage in infants before ossification of the femoral head and acetabulum obscured cartilaginous structures on radiographs.
- Refined Non-Operative Treatment: The Pavlik harness , introduced by Arnold Pavlik in 1944, became the gold standard for treating reducible DDH in infants up to 6 months of age. Its success lies in maintaining gentle flexion and abduction, promoting concentric reduction and stimulating acetabular development, while allowing for some hip motion.
-
Evolution of Surgical Techniques:
- Open Reduction: Techniques improved with better understanding of soft tissue blocks (hypertrophied ligamentum teres, inverted labrum, constricted capsule, iliopsoas tendon) and safer approaches.
- Pelvic Osteotomies: A range of osteotomies were developed to address residual acetabular dysplasia at various ages. The Salter innominate osteotomy (1961) provided redirection of the acetabulum in younger children. The Dega and Pemberton osteotomies offered reshaping options. For adolescents and young adults, the multi-planar Ganz Periacetabular Osteotomy (PAO) (1988) emerged as a groundbreaking procedure, allowing precise correction of acetabular orientation while preserving the posterior column and the blood supply to the acetabular fragment, thereby avoiding complications associated with previous triple osteotomies.
- Femoral Osteotomies: Proximal femoral varus derotation osteotomies (VDRO) became standard for addressing excessive femoral anteversion or coxa valga, often performed concurrently with open reduction in older children to reduce joint pressure and tension on neurovascular structures.
- Focus on Long-Term Outcomes: The ultimate goal shifted from merely achieving reduction to preventing premature osteoarthritis, a common sequela of untreated or inadequately treated DDH. Research into risk factors for avascular necrosis (AVN) of the femoral head and techniques to mitigate this devastating complication became paramount.
Today, DDH management is highly specialized, emphasizing early diagnosis, tailored interventions based on age and severity, and a multidisciplinary team approach. While the mystery of its precise etiology continues to be explored at genetic and molecular levels, the evolution of understanding and treatment has dramatically improved the lives of countless individuals affected by this condition.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy and the intricate biomechanics of the hip joint is not merely academic but directly impacts the planning, execution, and outcomes of DDH surgery. The dysplastic hip deviates significantly from normal anatomy, presenting unique challenges.
Normal Hip Anatomy and Biomechanics
The hip is a triaxial diarthrodial ball-and-socket joint, engineered for both stability and a wide range of motion.
1. Bony Anatomy:
*
Acetabulum:
A cup-shaped socket formed by the fusion of the ilium (superior), ischium (posterior-inferior), and pubis (anterior-inferior). The weight-bearing dome (sourcil) of the acetabulum provides superior coverage for the femoral head. The acetabular fossa houses the pulvinar (fat pad) and ligamentum teres. The lunate surface, covered by articular cartilage, is the primary weight-bearing area.
*
Femoral Head:
A spherical structure, typically covered by articular cartilage, articulating with the lunate surface.
*
Femoral Neck:
Connects the head to the shaft, characterized by:
*
Angle of Inclination:
(Cervical-diaphyseal angle) Normally 125-135 degrees in adults; higher in infants, decreasing with age. Coxa valga (increased angle) or coxa vara (decreased angle) are common deformities in DDH.
*
Angle of Anteversion:
(Femoral neck anteversion) The angle between the axis of the femoral neck and the transcondylar axis of the knee. Normally 10-15 degrees in adults; higher in infants (up to 40 degrees). Excessive anteversion in DDH often contributes to instability.
2. Capsuloligamentous Structures:
*
Joint Capsule:
A strong fibrous capsule enclosing the joint. It is reinforced by three strong ligaments anteriorly:
*
Iliofemoral Ligament (Y-ligament of Bigelow):
The strongest, limiting hyperextension.
*
Pubofemoral Ligament:
Limits abduction and external rotation.
*
Ischiofemoral Ligament:
Limits internal rotation and extension.
*
Ligamentum Teres:
An intra-articular ligament originating from the acetabular fossa and inserting into the fovea of the femoral head. It carries a small artery (foveal artery, branch of obturator artery) to the femoral head, particularly important in children. In DDH, it can be hypertrophied and act as a block to reduction.
*
Labrum:
A fibrocartilaginous rim that deepens the acetabulum, increases congruity, and provides a suction seal. In DDH, it can be everted, hypertrophied, or inverted into the joint, acting as a mechanical obstruction.
3. Musculature:
*
Abductors (Gluteus Medius, Minimus, Tensor Fascia Lata):
Primarily responsible for stabilizing the pelvis during gait (preventing Trendelenburg sign) and hip abduction. Innervated by the superior gluteal nerve.
*
Adductors (Pectineus, Adductor Longus, Brevis, Magnus, Gracilis):
Primarily responsible for hip adduction. Innervated by the obturator nerve. Often contracted and tight in DDH, limiting abduction and preventing reduction.
*
Flexors (Iliopsoas, Rectus Femoris, Sartorius):
Iliopsoas (ilioacus and psoas major, innervated by femoral nerve and lumbar plexus) is the strongest hip flexor. Its tendon can be a significant block to reduction in DDH, often requiring lengthening or tenotomy.
*
Extensors (Gluteus Maximus, Hamstrings):
Primarily responsible for hip extension.
4. Neurovascular Structures:
*
Femoral Nerve:
Lies lateral to the femoral artery and vein, beneath the inguinal ligament, providing motor innervation to quadriceps and sensory innervation to anteromedial thigh. Vulnerable during anterior approaches.
*
Sciatic Nerve:
Exits the pelvis via the greater sciatic notch, posterior to the hip joint, providing motor and sensory innervation to the posterior thigh and leg. At risk during posterior approaches, ischial osteotomies, and excessive traction.
*
Lateral Femoral Cutaneous Nerve (LFCN):
Sensory nerve, pierces the fascia or courses deep to the inguinal ligament, medial to the ASIS. Highly variable course and very vulnerable during anterior-lateral approaches (e.g., Smith-Petersen, PAO).
Biomechanics of the Dysplastic Hip
DDH disrupts the normal biomechanical relationship, leading to instability, abnormal stress distribution, and ultimately, degenerative changes.
-
Acetabular Dysplasia:
Characterized by a shallow, vertically oriented, and/or excessively anteverted acetabulum. This results in:
- Reduced Femoral Head Coverage: Quantified by parameters like the Acetabular Index (AI) in children (angle between Hilgenreiner's line and a line from the medial to lateral acetabular roof) or the Lateral Center-Edge (CE) angle of Wiberg in adolescents/adults (angle between a vertical line through the femoral head center and a line from the femoral head center to the lateral acetabular rim). Normal CE angle >25 degrees.
- Concentrated Stress: Reduced contact area between the femoral head and lunate surface leads to abnormally high peak pressures on the articular cartilage. This is the primary driver of premature osteoarthritis.
-
Femoral Deformities:
- Excessive Femoral Anteversion: Often seen with DDH, contributing to anterior instability and impingement. Compensatory "in-toeing" gait may develop.
- Coxa Valga: Increased femoral neck-shaft angle, further decreasing femoral head containment in a shallow acetabulum and altering abductor mechanics.
-
Soft Tissue Adaptations:
- Capsular Laxity/Thickening: The joint capsule becomes elongated and redundant with chronic dislocation, but can also become thickened and constricted (e.g., hourglass constriction) preventing reduction.
- Muscle Imbalance: Adductor muscles (e.g., adductor longus, pectineus) and iliopsoas often become contracted due to the displaced hip, limiting abduction and extension. The abductor muscles (gluteus medius/minimus) may become ineffective due to altered lever arm mechanics.
-
Consequences:
- Instability and Subluxation: The poorly contained femoral head can repeatedly subluxate or dislocate, leading to cartilage wear and labral damage.
- Femoroacetabular Impingement (FAI): Overcoverage after corrective osteotomy, or conversely, a dysplastic femoral head can cause impingement (e.g., pincer or cam-like morphology), leading to labral tears and cartilage delamination.
- Limb Length Discrepancy (LLD): Often present with unilateral dislocation, potentially leading to compensatory scoliosis and gait abnormalities.
- Progressive Osteoarthritis: The inevitable long-term consequence of abnormal joint loading and instability, typically manifesting in early adulthood.
Surgical interventions aim to restore normal anatomy and biomechanics by:
* Achieving concentric reduction of the femoral head.
* Improving femoral head coverage by redirecting or reshaping the acetabulum.
* Correcting femoral deformities (anteversion, valgus).
* Releasing soft tissue contractures (adductor tenotomy, iliopsoas release, capsulotomy).
* Restoring muscle balance and function.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical phase following DDH surgery, aiming to protect the surgical repair, restore hip function, and facilitate optimal long-term outcomes. Protocols are highly individualized, dependent on the patient's age, the specific surgical procedure performed, and the surgeon's preferences.
General Principles
- Protection of Surgical Repair: The primary goal is to maintain the achieved reduction and fixation while allowing for tissue healing. This often involves periods of immobilization and restricted weight-bearing.
- Pain Management: Effective analgesia is crucial for patient comfort and participation in early rehabilitation.
- Prevention of Complications: Vigilance for complications such as infection, DVT, nerve palsy, and stiffness.
- Gradual Restoration of Motion and Strength: Progressing from passive to active range of motion (ROM) and then to strengthening exercises.
- Functional Progression: Re-establishing weight-bearing, gait, and eventually sport-specific activities.
Typical Protocols Based on Procedure
1. Closed Reduction with Spica Cast (Infants 6-24 months):
*
Immobilization:
Hip spica cast applied immediately post-reduction, typically in a "human position" (90° flexion, 45° abduction, neutral rotation).
*
Duration:
6-12 weeks, with cast changes (often 3-6 weeks) to monitor skin integrity, growth, and maintain reduction. Radiographs are taken during cast changes.
*
Rehabilitation:
*
Cast Care:
Parent education on skin care, diapering, and positioning to prevent pressure sores.
*
After Cast Removal:
Gradual weaning from abduction bracing (e.g., custom brace or Pavlik harness for several months).
*
ROM:
Gentle, passive ROM exercises are initiated once the cast is removed. Avoid forced abduction or hyperextension initially to prevent stress on the healing capsule.
*
Weight-Bearing:
Gradual return to weight-bearing and crawling/walking as tolerated, under close supervision.
*
Monitoring:
Regular radiographic follow-up is essential to monitor acetabular development and screen for AVN.
2. Open Reduction (Older Children >18-24 months):
*
Immobilization:
Spica cast often applied for 6-12 weeks post-operatively to protect reduction.
*
Rehabilitation (post-cast removal):
*
Phase 1 (Initial Protection - first 6-12 weeks post-cast):
*
Weight-Bearing:
Non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) with crutches/walker.
*
ROM:
Gentle passive ROM, particularly focusing on flexion and rotation. Limit abduction initially to protect capsular repair.
*
Therapy:
Pain management, edema control, isometric exercises for hip and core musculature.
*
Phase 2 (Intermediate - 3-6 months post-op):
*
Weight-Bearing:
Progressive weight-bearing (PWB) as tolerated, guided by imaging and clinical assessment.
*
ROM:
Active-assisted and active ROM exercises.
*
Strengthening:
Gradual introduction of isotonic strengthening (e.g., hip flexion, extension, light abduction/adduction) with minimal resistance. Core stability exercises.
*
Gait Training:
Focus on normal gait mechanics with assistive devices.
*
Phase 3 (Advanced - 6-12 months post-op):
*
Weight-Bearing:
Full weight-bearing (FWB) and discontinuation of assistive devices.
*
Strengthening:
Progressive resistance exercises for all hip muscle groups. Proprioceptive training.
*
Functional Training:
Agility drills, stair climbing, return to age-appropriate activities.
*
Long-Term Monitoring:
Continued follow-up for joint development and potential complications like AVN or residual dysplasia.
3. Pelvic Osteotomies (Salter, Dega, Pemberton - Children):
*
Immobilization:
Often a hip spica cast for 4-8 weeks to allow osteotomy healing and protect internal fixation.
*
Rehabilitation (post-cast removal):
Similar to open reduction protocols, emphasizing gradual weight-bearing progression as per osteotomy healing.
*
Weight-Bearing:
NWB or TDWB for 6-12 weeks, progressing to PWB and FWB based on radiographic evidence of bone healing.
*
ROM:
Initiated gently after cast removal, avoiding extreme ranges that could stress the osteotomy site.
*
Strengthening:
Gradual strengthening of hip abductors, flexors, and extensors.
*
Activity:
Return to light activities after 3-6 months, and full activity after 6-12 months, depending on bone healing.
4. Periacetabular Osteotomy (PAO) of Ganz (Adolescents/Young Adults):
*
Immediate Post-Operative (Day 0-7):
*
Weight-Bearing:
Strict NWB on the operated leg. Crutches or walker.
*
ROM:
Passive and active-assisted ROM exercises within a protected range (e.g., flexion 0-90°, abduction up to 30°, no forced adduction, neutral rotation). Avoid external rotation past neutral and combined flexion-adduction-internal rotation (anterior impingement precautions). Continuous passive motion (CPM) may be used.
*
Therapy:
Pain management, edema control, gentle quad and gluteal sets, ankle pumps. Hip precautions are essential.
*
Early Phase (Weeks 1-6):
*
Weight-Bearing:
NWB continues.
*
ROM:
Progressing passive/active-assisted ROM within protected ranges.
*
Strengthening:
Isometric hip flexion, extension, abduction, and adduction. Core strengthening. Upper body conditioning for crutch ambulation.
*
Mid-Phase (Weeks 6-12):
*
Weight-Bearing:
Transition to TDWB or PWB (25-50% body weight) with crutches, as per surgeon preference and radiographic evidence of osteotomy healing.
*
ROM:
Progressing to active ROM. Full flexion to 100-110° and abduction to 40° aimed for.
*
Strengthening:
Light resistance exercises (theraband). Introduction of stationary cycling with high seat.
*
Gait Training:
Focus on proper gait mechanics, minimizing Trendelenburg.
*
Late Phase (Months 3-6):
*
Weight-Bearing:
Progress to FWB, gradually weaning from crutches.
*
Strengthening:
Progressive resistive exercises for all hip musculature. Proprioception and balance training.
*
Functional Training:
Stepper, elliptical, swimming. Return to light daily activities.
*
Return to Activity/Sport (Months 6-12+):
*
Advanced Strengthening:
Plyometrics, sport-specific drills.
*
Gradual Return:
Phased return to impact activities and sports, typically not before 9-12 months post-operatively, once full strength and stability are achieved and radiographs show robust osteotomy healing.
*
Screw Removal:
Screws may be removed after 1-2 years if symptomatic or as a routine.
5. Proximal Femoral Osteotomies:
*
Immobilization:
Often a hip spica cast or abduction brace for 6-8 weeks for younger children. In adolescents, internal fixation with plates/screws typically allows earlier controlled motion.
*
Rehabilitation:
Similar principles to pelvic osteotomies. Weight-bearing progression is guided by radiological evidence of osteotomy healing, usually NWB or TDWB for 6-12 weeks, followed by PWB. ROM initiated once stable, with precautions specific to the osteotomy (e.g., protecting rotation after a derotation osteotomy).
Key Considerations Across All Protocols
- Individualization: Protocols must be adapted to each patient's pain tolerance, progress, and specific surgical findings.
- Patient Compliance: Education and motivation are critical for adherence to restrictions and exercise programs.
- Radiographic Monitoring: Regular X-rays are crucial to assess osteotomy healing, reduction maintenance, and identify potential complications like AVN.
- Addressing Secondary Issues: Management of muscle contractures, limb length discrepancy, and gait abnormalities should be integrated.
- Psychological Support: Especially for adolescents undergoing major hip surgery, psychological support can aid in adherence and recovery.
Summary of Key Literature / Guidelines
The understanding and management of DDH are continuously refined through rigorous research and the development of evidence-based guidelines. Several key publications and societal recommendations guide clinical practice.
1. Historical and Foundational Texts:
*
Hippocrates, "On Joints":
Provides the earliest documented clinical descriptions of hip dislocations.
*
Dupuytren, "Leçons Orales de Clinique Chirurgicale":
Landmark work distinguishing congenital dislocation from other forms, though limited by contemporary therapeutic capabilities.
*
Lorenz, A.:
Pioneering work on non-operative "bloodless reduction" techniques, which, despite complications, set the stage for modern closed reduction methods.
*
Pavlik, A.:
Described the harness that bears his name in 1944, revolutionizing early non-operative management for infantile DDH.
2. Diagnostic and Classification Systems:
*
Graf, R. (1980s):
Developed the standardized ultrasonic examination and classification of infantile hip dysplasia, which remains the cornerstone of early diagnosis. His work allowed for the detection of subtle acetabular morphology long before radiological changes were apparent.
*
Tönnis, D.:
Contributed significantly to the radiological classification of DDH severity and prognostic indicators, particularly for older children and adults. His criteria for osteoarthritis progression are widely cited.
*
Wiberg, G.:
Described the Lateral Center-Edge (CE) angle, a fundamental radiographic measurement for assessing acetabular coverage in adolescents and adults.
3. Surgical Technique Development:
*
Salter, R.B. (1961):
Published the description of the innominate osteotomy, a pivotal redirectional pelvic osteotomy for correcting acetabular dysplasia in younger children.
*
Ganz, R., Klaue, K., et al. (1988):
Introduced the Periacetabular Osteotomy (PAO), a paradigm shift in the surgical treatment of symptomatic acetabular dysplasia in adolescents and young adults. This osteotomy's ability to provide multiplanar correction while preserving the posterior column and vascularity was a major advancement. Multiple long-term follow-up studies have since confirmed its efficacy in delaying or preventing total hip arthroplasty.
4. Contemporary Guidelines and Consensus Statements:
*
American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines:
The AAOS regularly updates evidence-based guidelines for various orthopedic conditions, including DDH. These guidelines typically cover screening recommendations, diagnostic algorithms, and treatment pathways for different age groups, often stratifying recommendations based on the strength of evidence. Key areas include:
*
Screening:
Recommendations for universal clinical screening and selective ultrasound screening based on risk factors (e.g., breech presentation, family history).
*
Pavlik Harness Management:
Guidance on appropriate indications, fitting, and monitoring to optimize outcomes and minimize complications (e.g., femoral nerve palsy, AVN).
*
Surgical Indications:
Criteria for when closed reduction, open reduction, or osteotomies are indicated, often based on age, reducibility, and severity.
*
Pediatric Orthopaedic Society of North America (POSNA):
POSNA provides specific recommendations and educational resources focused on pediatric orthopedic conditions, including DDH. Their consensus statements and webinars often detail best practices for the full spectrum of DDH care, from neonatal screening to complex reconstructive surgeries.
*
International Hip Dysplasia Institute (IHDI):
A collaborative effort dedicated to improving the health and lives of individuals with hip dysplasia. The IHDI provides accessible information for both clinicians and patients, promoting early diagnosis and optimal treatment strategies, particularly emphasizing safe infant positioning practices.
5. Key Literature Themes and Current Trends:
*
Long-Term Outcomes of PAO:
Numerous long-term studies demonstrate the success of PAO in improving hip function, alleviating pain, and significantly delaying or preventing the need for total hip arthroplasty in well-selected patients with acetabular dysplasia.
*
Risk Factors for Avascular Necrosis (AVN):
Continued research focuses on identifying modifiable risk factors for AVN following reduction (especially closed reduction in older infants) and developing strategies to mitigate this devastating complication, including cautious reduction maneuvers, femoral shortening osteotomies, and careful monitoring.
*
Role of Arthroscopy in DDH:
Increasing use of hip arthroscopy in conjunction with PAO or for isolated labral repair/chondroplasty in mild dysplasia, particularly for addressing femoroacetabular impingement lesions that may co-exist or develop after osteotomy.
*
Transition of Care:
Greater emphasis on the transition of care from pediatric to adult orthopedic specialists for long-term follow-up and management of residual problems or early osteoarthritis in young adults treated for DDH.
*
Genetics and Biomarkers:
Ongoing research into the genetic basis and potential biomarkers for DDH to enable earlier identification of at-risk infants and potentially personalize treatment strategies.
The literature consistently supports early detection and appropriate intervention as paramount to achieving favorable long-term outcomes in DDH. The evolving landscape of diagnostic tools and surgical techniques continues to improve the prognosis for individuals affected by this complex developmental condition.
