Femoral Head Fractures: Epidemiology, Anatomy, Biomechanics, and Clinical Significance
Key Takeaway
Femoral head fractures are severe injuries, often linked to high-energy trauma and hip dislocations. They pose significant risk for post-traumatic arthritis (PTA) and osteonecrosis (ONFH) due to potential vascular supply disruption. Comprehensive understanding of their epidemiology, surgical anatomy, biomechanics, and Pipkin classification is essential for effective orthopedic management.
Introduction & Epidemiology
Femoral head fractures represent a relatively uncommon yet highly morbid injury pattern, frequently encountered in the context of high-energy trauma. While the true incidence is challenging to ascertain due to their strong association with hip dislocations, these fractures are critical to recognize and manage meticulously due to their profound potential for long-term functional impairment, primarily through the development of post-traumatic arthritis (PTA) and osteonecrosis of the femoral head (ONFH).
The epidemiology is inherently linked to hip dislocation patterns. Approximately 10% of posterior hip dislocations are complicated by an associated femoral head fracture. In contrast, anterior hip dislocations, while less common overall, are associated with femoral head fractures in a significantly higher proportion, ranging from 25% to 75% of cases. The disparity in incidence between posterior and anterior dislocation mechanisms reflects differing biomechanical forces at play.
Historically, most femoral head fractures were described as shear or cleavage types, often visualized on plain radiographs. However, with the widespread adoption and increased use of advanced cross-sectional imaging, specifically computed tomography (CT), there has been a notable increase in the recognition of indentation-type or crush-type fractures. These subtle impaction injuries, often occurring anteriorly, were previously underestimated or missed. Impaction fractures are particularly common in association with anterior hip dislocations.
The typical demographic affected by femoral head fractures includes young, active individuals involved in motor vehicle collisions, falls from height, or industrial accidents. This underscores the critical need for optimal management to restore joint congruity and function, thereby preserving a high quality of life. The injury is rarely isolated; a formal trauma evaluation is imperative given that most femoral head fractures are a sequela of high-energy mechanisms. Comprehensive assessment often reveals polytrauma, with up to 95% of patients presenting with concomitant injuries requiring inpatient management independent of the femoral head fracture itself. Common associated injuries include acetabular fractures, ipsilateral lower extremity injuries such as knee ligament disruptions, and other pelvic or abdominal trauma.
The classification system most widely utilized for femoral head fractures is the Pipkin classification, introduced in 1957, which categorizes these injuries based on the location of the fracture line relative to the fovea capitis and the presence of associated injuries. This classification system directly guides management strategies and offers prognostic insights regarding potential complications.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the hip joint is paramount for the successful management of femoral head fractures. The femoral head, a highly spherical structure, articulates with the acetabulum to form a ball-and-socket joint, providing both mobility and stability.
Gross Anatomy
The femoral head is largely covered by articular cartilage, excluding the fovea capitis, a non-articular depression that serves as the attachment point for the ligamentum teres. The ligamentum teres, while having a limited role in static hip stability, does contain a small artery (a branch of the obturator artery) which contributes minimally to femoral head vascularity, particularly in adults. The main load-bearing surface of the femoral head encompasses approximately 70% of its articular surface. Any disruption to this critical articular cartilage or the underlying subchondral bone has significant implications for future joint health and is a primary driver for the development of post-traumatic arthritis.
Vascular Anatomy
The vascular supply to the femoral head is predominantly derived from the medial femoral circumflex artery (MFCA), a branch of the deep femoral artery. The MFCA gives rise to several retinacular vessels (superior, inferior, anterior, and posterior) that ascend along the femoral neck within the capsular reflections. The superior and posterior retinacular vessels, traversing beneath the piriformis and obturator internus tendons respectively, are the most critical contributors to the vascularity of the weight-bearing superior and posterior aspects of the femoral head. A smaller contribution arises from the lateral femoral circumflex artery (LFCA) anteriorly, and the aforementioned branch from the obturator artery within the ligamentum teres.
Femoral head fractures, particularly those associated with hip dislocations, place these critical retinacular vessels at high risk of stretch, compression, or direct transection. Disruption of this blood supply, especially the MFCA branches, significantly increases the risk of ONFH. The timing of hip reduction after dislocation is a strong predictor of ONFH risk, highlighting the urgency of emergent, gentle reduction maneuvers.
Biomechanics of Injury
The mechanism of femoral head fracture is inherently linked to the mechanism of hip dislocation. The injury typically involves significant axial loading applied to the femur while the hip is in a specific position.
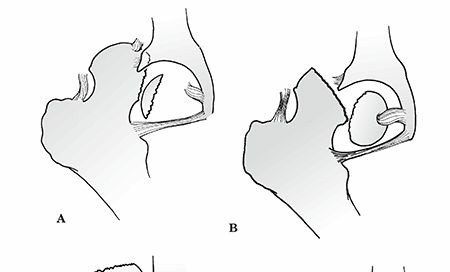
- Posterior Hip Dislocation with Femoral Head Fracture: This is the most common scenario. When the hip is flexed, adducted, and internally rotated (e.g., dashboard injury in a motor vehicle collision), a posterior force on the flexed knee drives the femoral head posteriorly. If the force is applied when the hip is partially flexed and adducted, the femoral head impacts the posterior rim of the acetabulum. The force can either cause an isolated posterior dislocation, a posterior acetabular wall fracture, or a femoral head fracture. Shear or cleavage fractures (Pipkin I and II) typically occur as the femoral head is levered out of the acetabulum, impinging against the posterior acetabular rim.
- Anterior Hip Dislocation with Femoral Head Fracture: Less common but often more complex. This occurs when the hip is in abduction and external rotation, and an axial load drives the femoral head anteriorly, typically impacting the anterior-inferior acetabular rim. This mechanism is frequently associated with impaction-type or crush fractures of the anterior-superior femoral head, often near the fovea, corresponding to the classic Pipkin I or II injury with an anterior dislocation.
The forces involved are often extremely high, explaining the frequently encountered associated injuries and the need for comprehensive trauma management.
Indications & Contraindications
Management decisions for femoral head fractures are primarily guided by the Pipkin classification, which stratifies the injury based on the fragment's relationship to the fovea and the presence of concomitant fractures. The overarching goal of treatment, whether operative or non-operative, is to achieve a stable, congruent hip joint with an anatomically reduced articular surface to minimize the risk of post-traumatic arthritis and osteonecrosis.
Pipkin Classification
- Pipkin Type I: Fracture of the femoral head inferior to the fovea capitis. These typically involve non-weight-bearing portions of the head.
- Pipkin Type II: Fracture of the femoral head superior to the fovea capitis, involving the weight-bearing articular surface. These are inherently more critical due to the potential for significant post-traumatic arthritis if not anatomically reduced.
- Pipkin Type III: A Pipkin Type I or II fracture with an associated femoral neck fracture. This significantly complicates management due to heightened risk of ONFH and nonunion.
- Pipkin Type IV: A Pipkin Type I or II fracture with an associated acetabular fracture. This typically represents a more severe, complex injury pattern.
Non-Operative Indications
Non-operative management is reserved for a select subset of femoral head fractures where surgical intervention carries greater risks or offers no significant advantage over conservative care.
- Small, Nondisplaced Pipkin Type I Fractures: Fragments that are inferior to the fovea, do not involve the weight-bearing surface, and are stable and anatomically reduced after closed reduction of the hip dislocation.
- Extremely Comminuted Fragments: In rare instances, if the femoral head fragment is extremely small and comminuted, surgical fixation may be impractical or detrimental to the remaining cartilage. In these cases, excision of the fragment may be considered, but only if it does not significantly compromise joint stability or load-bearing.
- Medical Contraindications to Surgery: Patients with severe comorbidities that significantly increase surgical risk and whose functional demands are low may be candidates for non-operative management, provided the hip remains stable after reduction.
Non-operative management typically involves a period of restricted weight-bearing (often non-weight-bearing for 6-12 weeks) and controlled range of motion, with close radiographic follow-up to monitor for fragment displacement, heterotopic ossification, or early signs of ONFH or arthritis.
Operative Indications
Operative intervention is the standard of care for most femoral head fractures, particularly those involving the weight-bearing surface or causing mechanical instability.
- Displaced Articular Fragments (Pipkin Type II, III, IV, and displaced I): Any displacement of the articular surface that results in incongruity of the hip joint is a strong indication for open reduction and internal fixation (ORIF). The threshold for displacement requiring surgery is often considered to be 1-2 mm, though even smaller steps or gaps can predispose to post-traumatic arthritis.
- Incarcerated Fragments: Fragments that remain within the joint space after attempted closed reduction of the hip dislocation, preventing concentric reduction. These must be surgically removed or reduced and fixed.
- Unstable Hip After Closed Reduction: If the hip joint remains unstable after reduction of the dislocation, often due to a large or dislodged femoral head fragment, ORIF is indicated to restore stability.
- Associated Femoral Neck Fracture (Pipkin Type III): These injuries are highly unstable and carry a very high risk of ONFH. ORIF of both the femoral neck and head is typically required, sometimes combined with primary arthroplasty in elderly patients or those with pre-existing arthritis.
- Associated Acetabular Fracture (Pipkin Type IV): These complex injuries often require a combined approach to address both the femoral head and acetabular components. The specific surgical strategy depends on the morphology of both fractures.
- Large Fragment Size: Even a Pipkin Type I fracture, if the fragment is substantial, may warrant fixation to prevent displacement and ensure joint congruity.
- Recurrent Dislocation: If the femoral head fragment contributes to recurrent instability following reduction, surgical intervention is necessary.
Contraindications
Absolute contraindications to surgical management are rare and typically relate to the patient's overall medical status rather than the fracture itself (e.g., active systemic infection, uncontrolled life-threatening comorbidities that preclude anesthesia). Relative contraindications may include severely comminuted non-reconstructable fragments (in which case fragment excision or arthroplasty might be considered), or a patient with extremely low functional demands who is non-ambulatory and stable with non-operative management.
Table: Operative vs. Non-Operative Indications for Femoral Head Fractures
| Indication | Operative Management | Non-Operative Management |
|---|---|---|
| Pipkin Type I |
- Displaced fragments (>1-2mm)
- Fragment preventing concentric reduction - Large fragment size |
- Small, nondisplaced fragment
- Concentric, stable reduction achieved - Fragment inferior to fovea |
| Pipkin Type II |
-
All displaced fractures involving weight-bearing surface
- Fragment preventing concentric reduction |
- (Rarely) Undisplaced, stable, very small fragment in low-demand patient.
- Medical contraindications. |
| Pipkin Type III |
-
All cases typically require ORIF of both neck and head
- (Consider arthroplasty in elderly/low-demand patients) |
- N/A (high instability, high ONFH risk) |
| Pipkin Type IV | - All cases typically require ORIF of both head and acetabulum | - N/A (complex, unstable injury) |
| Associated Pathology |
- Incarcerated fragment
- Hip instability after reduction - Recurrent dislocation |
- N/A |
| Patient Factors |
- Young, active patient
- High functional demands |
- Severe medical comorbidities
- Non-ambulatory - Very low functional demands |
| Goals | - Anatomic reduction, stable fixation, prevent PTA/ONFH | - Prevent fragment displacement, maintain stability, manage symptoms |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes in femoral head fractures. Given the high-energy nature of these injuries, initial resuscitation and stabilization according to ATLS protocols are paramount.
Initial Assessment and Imaging
- Emergent Hip Reduction: The single most critical initial step after a posterior hip dislocation, especially if associated with a femoral head fracture, is emergent closed reduction. This must be performed as rapidly as possible (ideally within 6 hours) to mitigate the risk of femoral head osteonecrosis. All reductions should be performed under adequate sedation and muscle relaxation.
- Post-Reduction Imaging: Following successful closed reduction, immediate radiographs (AP pelvis and lateral hip) are essential to confirm concentric reduction and assess for any incarcerated fragments.
- Computed Tomography (CT): A comprehensive CT scan of the pelvis and hip is indispensable for definitive diagnosis and pre-operative planning. It precisely characterizes the femoral head fracture morphology (size, location, displacement, comminution), identifies incarcerated fragments (bone or cartilage), and evaluates for associated acetabular or femoral neck fractures, which may be subtle on plain radiographs. CT also aids in planning surgical approach and fixation strategy.
- Magnetic Resonance Imaging (MRI): While not routine acutely, MRI may be considered in equivocal cases or later to assess for cartilage damage, labral tears, or early signs of osteonecrosis.
Pre-Operative Planning Considerations
- Fracture Classification: Reconfirm Pipkin classification and identify associated injuries (acetabular, femoral neck).
- Fragment Location and Size: Anterior fragments may necessitate an anterior approach, while posterior fragments typically require a posterior approach. The size and geometry of the fragment will dictate potential fixation methods (headless screws, small plates, suture anchors).
- Associated Injuries: If an acetabular fracture (Pipkin Type IV) or femoral neck fracture (Pipkin Type III) is present, the surgical approach and fixation strategy must address both components. This may involve staged procedures or a combined approach.
-
Surgical Approach Selection:
The choice of surgical approach is dictated by:
- Fragment location: Posterior fragments are typically accessed via the Kocher-Langenbeck approach. Anterior fragments are accessed via Smith-Petersen, Watson-Jones, or Ganz surgical hip dislocation.
- Associated injuries: Acetabular fractures may influence the choice of approach (e.g., ilioinguinal for anterior column/wall, Kocher-Langenbeck for posterior column/wall).
- Surgeon preference and experience.
- Need for 360-degree visualization: The surgical hip dislocation technique (Ganz approach) allows for complete visualization of the femoral head and may be preferred for complex or intra-articular fractures.
- Fixation Strategy: Select appropriate implants (e.g., 2.7 mm or 3.5 mm headless compression screws, small fragment plates, bioabsorbable pins) based on fragment size, bone quality, and desired stability. Plan screw trajectories to maximize purchase and avoid intra-articular placement.
- Timing of Surgery: After emergent reduction of the hip dislocation, definitive ORIF of the femoral head fracture is typically performed within a few days, once the patient is medically stable and thorough pre-operative planning is complete. While emergent reduction is key for ONFH prevention, delaying definitive fixation slightly does not appear to negatively impact outcomes as long as the joint is concentrically reduced and stable.
Patient Positioning
The patient's position on the operating table depends entirely on the chosen surgical approach.
-
Lateral Decubitus Position:
- Common for the Kocher-Langenbeck approach (posterior).
- Allows access to the posterior aspect of the hip.
- Careful padding of bony prominences and axilla.
- Often involves a beanbag or sacral support.
-
Supine Position:
- Common for anterior approaches (Smith-Petersen, Watson-Jones) and surgical hip dislocation.
- May be utilized on a standard OR table or a fracture table.
- A fracture table can provide controlled traction, which may be advantageous for visualization or reduction.
- Consideration for leg positioning, allowing for hip flexion, extension, abduction, adduction, and rotation during the procedure.
- Intraoperative Fluoroscopy: Essential regardless of position to confirm fragment reduction, screw placement, and joint congruity. The C-arm must have unrestricted access around the hip.
Detailed Surgical Approach / Technique
The primary goals of operative management are anatomical reduction of the femoral head fragment, stable internal fixation, restoration of joint congruity, and preservation of femoral head vascularity. The choice of surgical approach depends on the fracture location (anterior vs. posterior) and associated injuries.
General Principles of Fixation
- Open Reduction: Direct visualization of the articular surface is crucial. Incarcerated fragments (bony or cartilaginous) must be identified and removed or reduced.
- Anatomic Reduction: The articular fragment must be reduced anatomically to restore joint congruity. Even small steps or gaps can significantly increase the risk of post-traumatic arthritis.
- Stable Internal Fixation: Implants should provide rigid fixation, allowing for early mobilization while minimizing hardware prominence that could irritate the articular cartilage. Headless compression screws (e.g., 2.7mm or 3.5mm cannulated) are frequently used, placed from a non-articular portion of the femoral head into the main bone stock, or vice versa, ensuring the screw heads are fully countersunk.
- Vascular Preservation: Meticulous dissection and careful retraction are essential to protect the retinacular vessels, particularly during posterior approaches.
- Capsular Repair: Whenever possible, the hip capsule should be repaired to enhance joint stability.
Common Surgical Approaches
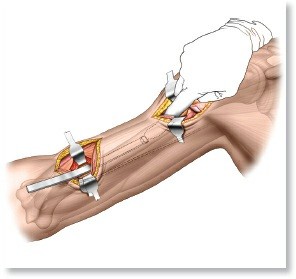
1. Kocher-Langenbeck Approach (Posterior)
- Indications: Most commonly used for posterior femoral head fractures (e.g., Pipkin Type I or II fragments presenting posteriorly), posterior acetabular fractures, or associated posterior hip dislocations.
- Patient Positioning: Lateral decubitus position with the affected limb draped free to allow for full range of motion.
- Incision: A curvilinear incision centered over the greater trochanter, extending proximally along the iliac crest and distally along the posterior aspect of the femur.
-
Dissection:
- The gluteus maximus fascia is incised, and the muscle is split in line with its fibers.
- The short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) are identified. The piriformis is typically tagged and tenotomized near its insertion on the greater trochanter. The obturator internus and gemelli can also be released. Care is taken to protect the sciatic nerve, which lies anterior to the piriformis in about 85% of cases. The superior gluteal neurovascular bundle is superior to piriformis and must also be protected.
- The ascending branch of the medial femoral circumflex artery, running along the superior border of the quadratus femoris, is a critical blood supply to the femoral head and must be protected.
- The posterior hip capsule is exposed.
-
Arthrotomy and Fragment Management:
- A T-shaped or H-shaped capsulotomy is performed to fully visualize the femoral head and any fragments.
- The femoral head fracture fragment is identified. Gently manipulate the hip (flexion, adduction, internal rotation) to facilitate visualization and reduction.
- Fragment reduction can be achieved with fine reduction clamps, dental picks, or a joystick K-wire. Once anatomically reduced, provisional K-wires are used to maintain reduction.
- Definitive fixation is typically achieved with two or more headless compression screws, placed to compress the fracture and buried beneath the cartilage surface. Screw trajectories should avoid the fovea if possible.
- Closure: The capsule is meticulously repaired. The short external rotators are reattached through drill holes in the greater trochanter or with suture anchors. The gluteus maximus is reapproximated, and standard wound closure follows.
2. Anterior Approaches (Smith-Petersen, Watson-Jones)
- Indications: Primarily for anterior femoral head fractures (e.g., impaction fractures associated with anterior dislocations), anterior acetabular fractures, or anterior surgical hip dislocation.
- Patient Positioning: Supine position.
-
Smith-Petersen (Anteromedial) Approach:
- Incision: Longitudinal incision from the ASIS distally.
- Dissection: Between the sartorius (medially) and the tensor fascia lata and rectus femoris (laterally). The lateral femoral cutaneous nerve should be identified and protected.
- The anterior hip capsule is exposed.
-
Watson-Jones (Anterolateral) Approach:
- Incision: Longitudinal incision extending from the ASIS distally, slightly lateral to the Smith-Petersen.
- Dissection: Between the tensor fascia lata (medially) and the gluteus medius/vastus lateralis (laterally).
- The interval between the gluteus medius and rectus femoris is utilized, or the rectus femoris is retracted medially. The anterior hip capsule is exposed.
-
Arthrotomy and Fragment Management:
- Similar principles to the posterior approach. The capsule is incised.
- Fragments are visualized, reduced, and fixed, often with headless screws.
- Closure: Capsular repair and standard wound closure.
3. Surgical Hip Dislocation (Ganz Trochanteric Flip Osteotomy)
- Indications: Complex femoral head fractures (Pipkin Type II, III, IV), fractures requiring 360-degree visualization of the femoral head or acetabulum, associated femoral neck fractures, or challenging intra-articular pathologies.
- Patient Positioning: Lateral decubitus position is common, though supine is also used.
- Incision: Posterolateral incision, similar to the Kocher-Langenbeck, but extending further distally to allow for trochanteric osteotomy.
-
Trochanteric Flip Osteotomy:
- The gluteus maximus is split, and the trochanteric bursa is excised.
- The interval between the gluteus medius and piriformis is identified.
- An osteotomy of the greater trochanter, including the insertion of gluteus medius and minimus, is performed. The osteotomy is planned carefully to preserve the vascularity of the trochanteric fragment and the retinacular vessels arising from the MFCA. The "safe surgical dislocation" technique emphasizes preserving the posterior superior retinacular vessels, which are crucial for femoral head blood supply. This means avoiding disruption to the gluteus medius, minimus, and vastus lateralis insertions where the MFCA branches ascend.
- The trochanteric fragment is then "flipped" anteriorly, preserving its muscle attachments.
-
Surgical Dislocation:
- The hip is dislocated anteriorly by controlled external rotation and extension after capsulotomy. This provides complete visualization of the femoral head and acetabulum.
-

-
Fragment Management:
- The femoral head fracture fragment(s) are anatomically reduced under direct vision.
-
 - Fixation is performed, typically with headless compression screws. The wide exposure allows for optimal screw trajectory and confirmation of seating below the articular surface.
- Any associated acetabular fracture or intra-articular debris is addressed.
-

-
Reduction and Closure:
- The hip is carefully reduced.
- The trochanteric osteotomy is reattached with two or three large fragment cancellous screws (e.g., 3.5mm or 4.5mm) or tension band wiring. This must be a stable fixation to allow for early mobilization.
- The capsule is repaired, and the wound is closed in layers.
Special Considerations
- Impaction Fractures: For indentation or crush fractures, the depressed segment of cartilage and subchondral bone may need to be elevated from below (e.g., through a cortical window in the femoral neck or a small arthrotomy) and supported with bone graft (autograft or allograft) to restore the spherical contour of the femoral head.
- Fragment Excision: Very small, non-articular, or highly comminuted fragments that cannot be fixed and are not essential for joint stability may be considered for excision, but this is generally avoided for weight-bearing fragments.
- Arthroscopy: Hip arthroscopy can be used as an adjunct, either diagnostically to assess fragment reduction and articular congruity or therapeutically to remove small incarcerated fragments or perform limited débridement.
Complications & Management
Femoral head fractures, despite optimal management, are associated with a significant rate of complications, which underscores the complexity and severity of these injuries. Vigilant post-operative monitoring and a clear management strategy for potential complications are crucial.
Common Complications
-
Post-Traumatic Arthritis (PTA):
- Incidence: The most common and debilitating long-term complication, occurring in 20% to 50% of cases, even after seemingly successful ORIF. Factors contributing to PTA include residual articular incongruity (>1-2mm step-off or gap), associated cartilage damage, and the initial energy of the trauma.
-
Management:
- Early: Symptomatic management, physical therapy, activity modification.
- Moderate: Arthroscopy for débridement, osteochondral grafting (limited utility), periacetabular osteotomy (PAO) for selected cases of residual dysplasia or malorientation in young patients.
- Severe: Total Hip Arthroplasty (THA). This is often the definitive salvage procedure for debilitating PTA, especially in older patients or those with extensive cartilage loss.
-
Osteonecrosis of the Femoral Head (ONFH) / Avascular Necrosis (AVN):
- Incidence: Highly variable (5% to 40%), directly correlated with the initial energy of injury, the extent of vascular disruption, and most importantly, the time to hip reduction. Delayed reduction beyond 6-12 hours significantly increases the risk. Associated femoral neck fractures (Pipkin Type III) also dramatically elevate this risk.
-
Management:
- Early (pre-collapse): Core decompression, vascularized or non-vascularized fibular grafting, osteotomy (e.g., rotational osteotomy) in select cases.
- Late (post-collapse): Total Hip Arthroplasty (THA). Hemiarthroplasty may be considered in low-demand, elderly patients, but THA is generally preferred for functional outcomes.
-
Heterotopic Ossification (HO):
- Incidence: Common after high-energy hip trauma and surgical approaches that disrupt muscle planes (e.g., Kocher-Langenbeck), occurring in 10-20% of cases, potentially limiting range of motion.
-
Management:
- Prophylaxis: Indomethacin (NSAID) for 3-6 weeks post-operatively or single-dose localized radiation therapy (700-800 cGy within 72 hours pre- or post-op) are effective.
- Established HO: Observation for mild cases. Surgical excision of mature HO (typically >1 year post-injury, once bone scan shows quiescence) for functional impairment.
-
Infection:
- Incidence: Relatively low (1-5%) but devastating, especially in a joint replacement.
-
Management:
- Superficial: Oral antibiotics, wound care.
- Deep: Surgical irrigation and débridement, intravenous antibiotics. May require implant removal and staged revision arthroplasty if THA is indicated.
-
Iatrogenic Nerve Injury:
- Incidence: Variable depending on approach. Sciatic nerve palsy is a known risk with posterior dislocations and posterior approaches (Kocher-Langenbeck), occurring in up to 10-20% of dislocations. Femoral nerve injury is less common with anterior approaches.
- Management: Observation for neuropraxia. Surgical exploration for complete transection or persistent compression (e.g., from hematoma or hardware). Nerve repair or grafting if indicated for severe deficits.
-
Nonunion/Malunion of the Femoral Head Fragment:
- Incidence: Rare with stable fixation but can occur. More common with Pipkin Type III fractures (femoral neck component).
-
Management:
- Nonunion: Revision ORIF with bone grafting. In the presence of significant pain or early arthritis, THA may be considered.
- Malunion: May lead to persistent joint incongruity and accelerated PTA, often requiring eventual THA.
-
Re-dislocation/Instability:
- Incidence: Rare after stable fixation and capsular repair. More likely with inadequate initial reduction, large unrepaired capsular defects, or significant associated acetabular bone loss.
- Management: Closed reduction if possible. If recurrent, consider revision surgery to address underlying instability (e.g., repair capsule, address acetabular rim, reconsider fragment fixation).
-
Hardware-Related Complications:
- Incidence: Screw migration, prominence, or breakage can occur, irritating the articular cartilage or soft tissues.
- Management: Hardware removal if symptomatic or if intra-articular.
Table: Common Complications of Femoral Head Fractures
| Complication | Incidence | Salvage Strategies / Management | Post-traumatic arthritis (PTA) | 20-50% | Initial: Activity modification, NSAIDs. Advanced: Arthroscopy, osteotomy (rarely), Total Hip Arthroplasty (THA). |
|
Post-Traumatic Arthritis
| 20-50% (often higher) |
Conservative:
Activity modification, NSAIDs, intra-articular injections.
Surgical:
Arthroscopic débridement, microfracture, osteochondral allograft (limited), peri-acetabular osteotomy (PAO) for selected younger patients.
Salvage:
Total Hip Arthroplasty (THA). |
|
Osteonecrosis (AVN)
| 5-40% |
Early (Pre-collapse):
Core decompression, vascularized or non-vascularized fibular grafting, osteotomy.
Late (Post-collapse):
Total Hip Arthroplasty (THA). |
|
Heterotopic Ossification (HO)
| 10-20% |
Prophylaxis:
NSAIDs (e.g., Indomethacin) for 3-6 weeks, or single-dose radiation therapy (within 72 hours pre/post-op).
Treatment:
Observation for mild/asymptomatic. Surgical excision of mature HO (once quiescent) for functional impairment. |
|
Infection
| 1-5% |
Superficial:
Oral antibiotics, local wound care.
Deep:
Surgical irrigation and débridement, targeted IV antibiotics. If hardware involved, may require staged removal and revision. |
|
Iatrogenic Nerve Injury
| Sciatic: 10-20% |
Conservative:
Observation for neuropraxia.
Surgical:
Exploration for persistent compression, hematoma, or suspected transection; nerve repair/grafting if indicated. |
|
Nonunion/Malunion
| Rare |
Nonunion:
Revision ORIF with bone grafting. If symptomatic or leading to arthritis, consider THA.
Malunion:
Often leads to accelerated PTA, requiring eventual THA. |
|
Re-dislocation/Instability
| Rare (<5%) |
Acute:
Closed reduction.
Recurrent:
Revision surgery to address underlying cause (capsular repair, fragment fixation, acetabular rim pathology). |
|
Hardware-Related
| Variable | Removal of symptomatic or intra-articular hardware. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical to optimize functional recovery, restore range of motion, and mitigate the risk of complications following femoral head fracture fixation. The protocol must be tailored to the specific fracture pattern, quality of fixation, patient's bone quality, and any associated injuries. Close communication between the surgeon and physical therapist is paramount.
Phase I: Immediate Post-Operative (Weeks 0-6)
Goals:
* Pain and edema control.
* Protection of surgical repair and fixation.
* Prevention of joint stiffness.
* Initiation of gentle muscle activation.
Weight-Bearing:
*
Non-Weight Bearing (NWB) or Touch-Weight Bearing (TTWB):
Typically prescribed for 6-12 weeks, depending on fixation stability, fracture comminution, and risk of osteonecrosis. This is critical to allow for initial fracture healing and integration of the repaired articular surface. Crutches or a walker are used.
Range of Motion (ROM):
*
Passive Range of Motion (PROM) and Gentle Active-Assisted Range of Motion (AAROM):
Initiated early, within pain limits.
*
Precautions:
Avoid extreme hip flexion (>90 degrees), adduction past midline, and internal rotation for posterior approaches (to prevent posterior dislocation). Avoid extreme abduction and external rotation for anterior approaches (to prevent anterior dislocation). Specific limitations will be dictated by the surgeon based on capsular repair and stability assessment intraoperatively.
* Continuous Passive Motion (CPM) machine may be used in some centers, but evidence for improved long-term outcomes is mixed.
Muscle Strengthening:
*
Gentle Isometrics:
Gluteal sets, quadriceps sets, hamstring sets.
* Ankle pumps and foot circles to prevent deep vein thrombosis (DVT).
* Core stability exercises (gentle abdominal bracing).
Functional Activities:
* Bed mobility training.
* Transfers (bed to chair) with NWB precautions.
* Education on assistive device use and home safety.
Phase II: Early Progressive (Weeks 6-12)
Goals:
* Gradual progression of weight-bearing.
* Increase hip ROM within tolerance.
* Initiate active strengthening.
* Improve neuromuscular control.
Weight-Bearing:
*
Progressive Weight Bearing (PWB):
Transition from NWB/TTWB to PWB with crutches or walker, typically beginning around 6 weeks post-op, assuming radiographic signs of healing and no pain with initial loading. Progression is often based on clinical tolerance and surgeon guidance (e.g., 25% PWB for 2 weeks, then 50% for 2 weeks, etc.).
Range of Motion (ROM):
*
Active Range of Motion (AROM):
Gradually increase flexion, abduction, extension, and rotation as tolerated, respecting surgical precautions.
* Stretching for tight musculature (e.g., hip flexors, hamstrings).
Muscle Strengthening:
*
Light Resistance Exercises:
Hip abduction/adduction, flexion/extension (e.g., with resistance bands, light weights).
* Gluteus medius and minimus strengthening (clamshells, side-lying abduction).
* Core strengthening (planks, pelvic tilts).
* Initiate stationary cycling (low resistance, high seat) to promote ROM and non-impact conditioning.
Proprioception and Balance:
* Single-leg balance activities (initially with support).
* Weight-shifting exercises.
Phase III: Advanced Strengthening & Functional Return (Weeks 12-24 and Beyond)
Goals:
* Achieve full, pain-free ROM.
* Normalize gait pattern.
* Maximize strength, power, and endurance.
* Prepare for return to pre-injury activities.
Weight-Bearing:
*
Full Weight Bearing (FWB):
Progress from PWB to FWB without assistive devices, typically by 12-16 weeks, once radiographic healing is confirmed and pain is well-controlled.
Muscle Strengthening:
*
Progressive Resistance Training:
Advanced hip and core strengthening.
* Functional exercises: Lunges, squats, step-ups.
* Agility drills and sport-specific training for athletes.
* Isokinetic strengthening.
Cardiovascular Conditioning:
* Continue cycling, progress to elliptical, swimming, or treadmill walking/jogging as appropriate.
Return to Activity:
* Gradual return to recreational activities and sports, guided by pain, strength, ROM, and functional assessment. High-impact activities should be introduced cautiously and often with a prolonged delay to protect the healing joint and articular cartilage.
* Close monitoring for any signs of early arthritis or osteonecrosis.
Long-Term Monitoring
- Radiographic Follow-up: Regular X-rays (AP pelvis, lateral hip) at 3, 6, 12 months, and annually for several years to monitor for fracture healing, hardware issues, heterotopic ossification, and, critically, early signs of osteonecrosis or post-traumatic arthritis.
- Clinical Assessment: Persistent pain, limping, or decreased ROM should prompt further investigation (e.g., MRI for ONFH).
- Patient Education: Counsel patients on the long-term risk of post-traumatic arthritis and the potential need for future intervention, such as total hip arthroplasty, particularly for Pipkin Type II and IV injuries.
Summary of Key Literature / Guidelines
The literature on femoral head fractures, while not as extensive as for more common hip and pelvic injuries, consistently emphasizes several critical principles and offers insights into optimal management.
-
Emergent Reduction: The most consistently cited factor influencing the outcome of hip dislocations, particularly regarding the risk of osteonecrosis of the femoral head (ONFH), is the time to reduction. Studies have repeatedly shown that reduction within 6 hours significantly lowers the incidence of ONFH. This principle applies equally to hip dislocations with associated femoral head fractures. Delayed reduction beyond 12 hours is associated with a markedly increased incidence of ONFH, potentially up to 40% or more.
- Reference: Upadhyay et al., JBJS Am 2009. This meta-analysis underscored the prognostic importance of timing of reduction for hip dislocations.
-
Anatomic Reduction and Stable Fixation: For articular femoral head fractures, achieving and maintaining an anatomic reduction with stable internal fixation is paramount to minimize the risk of post-traumatic arthritis (PTA). Even minor residual articular step-offs or gaps (>1-2mm) are strongly correlated with accelerated degenerative changes.
- Reference: Brumback and Kenzora, J Orthop Trauma 1991. Early work emphasized the need for precise reduction in joint fractures.
- Reference: Giannoudis et al., J Bone Joint Surg Br 2009. A review highlighting critical factors in the management of complex hip injuries.
-
Pipkin Classification as a Guide: The Pipkin classification remains the most widely accepted system for guiding management and prognostication.
- Pipkin Type I: Non-weight-bearing fragments inferior to the fovea. If small and non-displaced after concentric reduction, non-operative management with protected weight-bearing is an option. If displaced or large, ORIF is preferred.
- Pipkin Type II: Weight-bearing fragments superior to the fovea. Almost universally require ORIF to restore articular congruity.
- Pipkin Type III: Pipkin I or II with an associated femoral neck fracture. These are highly unstable with a very high risk of ONFH. ORIF of both fracture components is typically recommended in young patients. In older patients or those with severe comminution, primary arthroplasty (hemiarthroplasty or THA) may be considered, although this is controversial in younger, active individuals.
- Pipkin Type IV: Pipkin I or II with an associated acetabular fracture. These complex injuries demand comprehensive management addressing both components, often via combined or extended approaches.
-
Role of Advanced Imaging (CT): The advent of routine pre- and post-reduction CT scanning has revolutionized the diagnosis and management of femoral head fractures. CT accurately characterizes fracture morphology, identifies incarcerated fragments, and reveals associated acetabular or femoral neck fractures that may be missed on plain radiographs. This detailed information is critical for pre-operative planning and surgical approach selection.
-
Surgical Approach Selection: The choice of surgical approach (e.g., Kocher-Langenbeck for posterior fragments, anterior approaches for anterior fragments, surgical hip dislocation for complex patterns) should be tailored to the fracture characteristics and surgeon experience. The Ganz surgical hip dislocation (trochanteric flip osteotomy) provides unparalleled visualization of the femoral head and acetabulum, making it advantageous for complex injuries where precise anatomical reduction is paramount and vascular preservation can be meticulously managed.
- Reference: Ganz et al., Clin Orthop Relat Res 2001. Seminal paper describing the surgical hip dislocation technique and its indications.
-
Vascular Preservation: During surgical intervention, meticulous soft tissue handling and careful identification of the retinacular vessels, particularly the ascending branches of the medial femoral circumflex artery, are essential to minimize iatrogenic injury and reduce the risk of ONFH.
-
Complication Rates: Despite optimal treatment, the rates of long-term complications, particularly PTA and ONFH, remain significant. This underscores the severity of the initial injury. Patients must be counselled about these risks and the potential need for future salvage procedures, such as total hip arthroplasty. Studies show that a high percentage of patients will require subsequent THA for debilitating arthritis or ONFH in the long term.
-
Rehabilitation: Post-operative rehabilitation protocols must be carefully designed, balancing protection of fixation with early, controlled range of motion to prevent stiffness. Protected weight-bearing is crucial for several weeks to months, depending on fracture stability.
In conclusion, the management of femoral head fractures demands an immediate, systematic approach, starting with emergent hip reduction. Definitive treatment, typically open reduction and internal fixation, requires a thorough understanding of hip anatomy, biomechanics, and precise surgical technique to restore joint congruity and minimize the devastating long-term complications of post-traumatic arthritis and osteonecrosis. Continued research focuses on improving fixation techniques, understanding cartilage healing, and refining joint preservation strategies.
Clinical & Radiographic Imaging

You Might Also Like