Comprehensive Guide to Preventing Dislocation After Total Hip Replacement
Key Takeaway
Preventing total hip replacement (THR) dislocation involves meticulous surgical technique, precise component positioning (acetabular anteversion/inclination, femoral anteversion), optimizing combined anteversion, utilizing larger femoral heads, and restoring proper hip biomechanics like offset and leg length. Crucially, maintaining appropriate soft tissue tension through meticulous capsule and rotator repair is paramount to ensuring long-term prosthetic stability.
Introduction & Epidemiology
Total hip replacement (THR) remains one of the most successful and impactful orthopedic procedures for alleviating pain and restoring function in patients with end-stage hip pathology. While advancements in implant design, surgical techniques, and perioperative care have significantly improved outcomes, prosthetic dislocation remains a leading cause of revision surgery and a significant source of patient morbidity.
Epidemiologically, the incidence of dislocation following primary THR ranges from 0.5% to 5%, with higher rates observed in revision THR, often reaching 10-20%. Early dislocations typically occur within the first three months post-operatively and are frequently attributed to surgical technique, component malposition, or early non-compliance with precautions. Late dislocations, occurring beyond three months, are more often associated with factors such as soft tissue laxity, component wear, neuromuscular dysfunction, or trauma. Each dislocation event not only imposes substantial healthcare costs through emergency department visits, closed reductions, potential hospitalizations, and subsequent revision surgeries, but also significantly impacts a patient's quality of life, often leading to anxiety, reduced activity levels, and fear of recurrence. Understanding and mitigating the multifactorial risk factors contributing to dislocation is paramount for optimizing long-term outcomes in THR.
Surgical Anatomy & Biomechanics
A thorough understanding of the hip's intricate anatomy and its biomechanical function is fundamental to preventing dislocation after THR.
Acetabular Anatomy
The acetabulum, a concave articular surface of the pelvis, dictates initial component placement. Its native orientation involves an average of 40-50° of inclination and 15-20° of anteversion in relation to the anterior pelvic plane. However, significant inter-individual variability exists, influenced by pelvic tilt, sagittal plane alignment, and potential spinal pathology. Dysplastic acetabula or those with previous trauma present unique challenges.
Femoral Anatomy
The proximal femur, comprising the head, neck, and trochanters, must be accurately replicated or restored by the femoral implant. Femoral neck-shaft angle, femoral offset, and femoral anteversion are critical parameters. Native femoral anteversion typically ranges from 10-20°, and restoration is vital to prevent impingement and ensure stability.
Soft Tissue Structures
- Capsule and Ligaments: The hip capsule, reinforced by the iliofemoral, pubofemoral, and ischiofemoral ligaments, plays a crucial role in intrinsic stability. While the capsule is often violated during THR, its integrity and repair, particularly the posterior capsule, are important for stability, especially with posterior approaches.
-
Musculature:
- Abductors: Gluteus medius and minimus are the primary abductors, inserting onto the greater trochanter. Their integrity and tension are critical for stability, preventing Trendelenburg gait, and resisting superior dislocation. Superior gluteal nerve injury can compromise their function.
- External Rotators: Piriformis, gemelli (superior and inferior), obturator internus, obturator externus, and quadratus femoris. These muscles are often divided or reflected in posterior approaches, making their meticulous repair vital.
- Adductors: Adductor magnus, longus, brevis, pectineus, and gracilis. While less directly involved in primary stability, their spasticity can contribute to adduction-impingement in certain neurological conditions.
- Flexors: Iliopsoas, rectus femoris. Iliopsoas impingement on an anteriorly proud acetabular component can cause pain but is rarely a direct cause of dislocation.
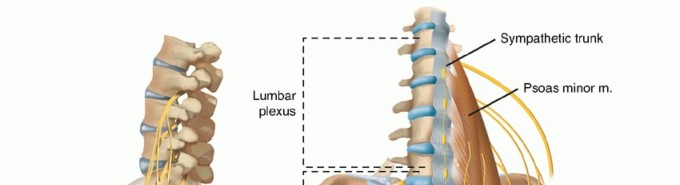
Neurovascular Structures
Proximity of the sciatic nerve (posterior), femoral nerve (anterior), and superior gluteal nerve (superolateral) necessitates careful retraction and protection during all approaches. Sciatic nerve palsy, a severe complication, can impair muscle function and predispose to dislocation. The superior gluteal neurovascular bundle is vulnerable during acetabular reaming or screw placement, potentially leading to abductor weakness.
Biomechanics of Prosthetic Stability
Dislocation typically occurs when the femoral head egresses the acetabular liner. The "jump distance" – the linear excursion the femoral head must travel before dislocating – is a key concept.
*
Component Positioning:
*
Acetabular Anteversion and Inclination:
Lewinnek's "safe zone" (40° inclination ± 10°, 15° anteversion ± 10°) remains a widely cited guideline. Deviations, particularly excessive anteversion or retroversion, and high inclination, increase dislocation risk.
*
Femoral Anteversion:
Proper restoration of femoral anteversion, combined with the acetabular component's version, defines the "combined anteversion." Optimizing combined anteversion minimizes impingement and maximizes range of motion without dislocating.
*
Femoral Head Size:
Larger femoral heads increase the jump distance, significantly enhancing prosthetic stability across a greater range of motion before impingement. Current practice favors larger heads (typically >32mm, often 36mm or greater) in standard bearings.
*
Offset and Leg Length:
Restoration of hip biomechanics, including femoral offset and leg length, is critical. Inadequate offset or leg shortening reduces abductor tension, leading to abductor weakness and increased dislocation risk. Excessive lengthening can also lead to instability or nerve stretch.
*
Soft Tissue Tension:
Appropriate soft tissue tension, achieved through meticulous repair of the capsule and external rotators (posterior approach), or preservation of the abductors (lateral approaches), is paramount. Laxity, either from inadequate repair or pre-existing abductor insufficiency, directly contributes to instability.
*
Impingement:
Bony or prosthetic impingement limits the hip's range of motion, creating lever-out forces that can lead to dislocation. This can result from malpositioned components, inadequate osteophyte removal, or excessive soft tissue bulk.
Indications & Contraindications
Indications for Total Hip Replacement (THR)
The primary indications for THR are intractable hip pain and functional limitation despite non-operative management, typically due to end-stage arthritic conditions.
*
Osteoarthritis (Primary or Secondary):
Most common indication.
*
Avascular Necrosis (AVN):
Collapse of the femoral head.
*
Inflammatory Arthritis:
Rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis.
*
Post-Traumatic Arthritis:
Following acetabular or femoral head fractures.
*
Developmental Dysplasia of the Hip (DDH):
With degenerative changes.
*
Certain Hip Fractures:
Femoral neck fractures in active, healthy individuals where internal fixation has failed or is contraindicated.
*
Benign and Malignant Tumors:
Resection and reconstruction (less common).
Indications for Revision THR for Recurrent Dislocation
When dislocation occurs repeatedly, revision surgery is often indicated after failed non-operative measures (bracing, activity modification).
*
Component Malposition:
Acetabular component malalignment (excessive anteversion/retroversion, inclination), or femoral component malversion.
*
Impingement:
Bony (e.g., osteophytes, posterior wall deficiency) or prosthetic (e.g., liner/skirt impingement).
*
Soft Tissue Laxity/Abductor Insufficiency:
Inadequate abductor tension, abductor tear, or damage to the posterior capsule/external rotators.
*
Liner Wear or Damage:
Leading to reduced jump distance.
*
Head-Neck Ratio Issues:
Insufficient head-neck offset or use of small femoral heads in situations requiring more stability.
Contraindications for THR
-
Absolute Contraindications:
- Active local or systemic infection.
- Rapidly progressive neurological disease or uncontrolled neuromuscular disorder affecting the hip musculature (e.g., severe Parkinson's, evolving stroke) making post-operative rehabilitation impractical or increasing dislocation risk significantly.
- Skeletal immaturity (relative, but generally true).
-
Relative Contraindications:
- Morbid obesity (increased complication rates, including dislocation).
- Significant medical comorbidities precluding safe anesthesia or recovery.
- Non-ambulatory status pre-operatively (benefits may not outweigh risks).
- Severe generalized osteoporosis (compromises implant fixation).
- Extensor mechanism insufficiency (e.g., quadriceps paralysis).
- Severe vascular disease in the limb.
| Indication Type | Primary THR | Revision THR for Recurrent Dislocation |
|---|---|---|
| Operative | - End-stage OA, AVN, inflammatory arthritis | - Component malposition (acetabular/femoral) |
| - Post-traumatic arthritis, DDH | - Impingement (bony/prosthetic) | |
| - Certain femoral neck fractures (in active patients) | - Soft tissue laxity / Abductor insufficiency | |
| - Failed non-operative management for pain/dysfunction | - Liner wear/damage | |
| - Repeated dislocations despite non-operative management | ||
| Non-Operative | - Early stage arthritis responsive to conservative care | - First-time dislocation (consider closed reduction) |
| - Mild/moderate symptoms | - Dislocation in moribund or non-ambulatory patients | |
| - Significant medical comorbidities precluding surgery | - Patient refusal or contraindication to surgery |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical steps in minimizing dislocation risk.
Pre-Operative Planning
-
Patient Optimization:
- Medical Clearance: Comprehensive assessment of cardiac, pulmonary, renal, and endocrine status. Optimization of chronic conditions (e.g., diabetes, hypertension).
- Nutritional Status: Address malnutrition, which can impair wound healing and increase infection risk, potentially compromising soft tissue integrity.
- Smoking Cessation: Advise at least 4-6 weeks pre-operatively to improve bone healing, reduce infection, and enhance soft tissue viability.
- DVT Prophylaxis: Standardized protocol based on patient risk factors.
- Physical Therapy Assessment: Identify pre-existing muscle weakness, range of motion limitations, and educate on post-operative precautions (if indicated by planned approach or patient risk factors).
- Spinal-Pelvic Relationship: In patients with spinal pathology (e.g., fusion, severe kyphosis), altered pelvic tilt dynamics can significantly impact functional acetabular orientation, necessitating customized component placement strategies. A lateral standing and seated radiograph may be helpful.
-
Radiographic Templating:
- Standard X-rays: AP pelvis with both hips, true lateral of the affected hip.
- Computed Tomography (CT) Scan: Indicated for complex primary cases (dysplasia, severe deformity), revision THR, or when precise component version measurement is required. CT allows for accurate assessment of true acetabular version, bony defects, and provides a 3D model for templating.
-
Templating Goals:
- Accurate sizing of both acetabular and femoral components.
- Restoration of hip center of rotation.
- Restoration of femoral offset and leg length equality.
- Prediction of acetabular inclination and anteversion.
- Pre-operative identification of potential bone loss or difficult anatomy.
- Selection of appropriate implant type (e.g., cemented vs. uncemented, specific head-neck geometry).
- Surgeon-Specific Education: While not patient education, the surgeon must effectively communicate the procedural details, expected recovery, and specifically address dislocation risks and prevention strategies with the patient. This involves explaining the reasoning behind activity restrictions (if employed) and the importance of compliance.
Patient Positioning
Proper positioning ensures adequate surgical exposure, prevents iatrogenic injury, and allows for accurate component placement.
1.
Lateral Decubitus Position (for Posterior and Direct Lateral Approaches):
*
Setup:
Patient placed on their unaffected side. Securely positioned using beanbag or specific hip positioners. Ensure the pelvis is perpendicular to the floor, avoiding rotation, which can lead to misjudged acetabular orientation.
*
Padding:
Meticulous padding of all pressure points (axilla, contralateral knee, ankle, peroneal nerve region) to prevent nerve compression or skin breakdown.
*
Stability:
Ensure the patient is firmly secured to prevent movement during reaming or impaction, which can compromise component placement.
2.
Supine Position (for Direct Anterior and Anterolateral Approaches):
*
Setup:
Patient supine on a radiolucent table or a specialized fracture table (traction table).
*
Pelvic Tilt:
Crucial to maintain a neutral pelvic tilt during surgery. Some surgeons use external fixation devices or specific blocks to control pelvic rotation.
*
Imaging:
Allows for intraoperative fluoroscopy to verify component position (especially with DAA).
*
Padding:
All pressure points, particularly the heels, sacrum, and ulnar nerves, must be padded.
Regardless of the approach, the surgical team must confirm the patient's position is stable, allows for full range of motion of the operative hip, and enables unimpeded access for instrumentation.
Detailed Surgical Approach / Technique
The choice of surgical approach and meticulous intraoperative technique are paramount in minimizing the risk of dislocation after THR. While no single approach is universally superior, specific steps within each technique are crucial for optimizing stability. Here, we focus on principles applicable to dislocation prevention, often exemplified by the posterior approach due to its historical association with higher dislocation rates and the subsequent evolution of specific preventative techniques.
Choice of Surgical Approach and its Impact on Dislocation Risk
-
Posterior Approach (PA):
- Dissection: Incision centered over the greater trochanter, extending proximally and distally. The gluteus maximus is split bluntly in line with its fibers. The short external rotators (piriformis, gemelli, obturator internus, quadratus femoris) and the posterior capsule are divided or tagged for later repair.
- Advantages: Excellent exposure of both acetabulum and femur, familiar to many surgeons, reproducible.
- Disadvantages: Traditionally associated with higher rates of posterior dislocation due to disruption of the posterior capsule and external rotators.
- Dislocation Mitigation: Crucial steps include meticulous repair of the posterior capsule and external rotators. Repairing these structures, often with strong non-absorbable sutures, restores a critical soft tissue barrier and limits posterior hyperextension and internal rotation.
-
Direct Anterior Approach (DAA):
- Dissection: An interval between the tensor fascia lata (superior gluteal nerve) and the sartorius/rectus femoris (femoral nerve) is utilized. The hip capsule is typically anteriorly incised or preserved.
- Advantages: Muscle-sparing, potentially lower posterior dislocation risk due to preservation of posterior structures. Allows for intraoperative fluoroscopy to aid component positioning.
- Disadvantages: Steep learning curve, potential for lateral femoral cutaneous nerve (LFCN) injury, limited exposure in obese or muscular patients, potential for femoral fracture during preparation, challenges in complex revisions. Higher risk for early anterior dislocation in some studies.
- Dislocation Mitigation: Careful femoral preparation to avoid fractures, precise acetabular positioning verified with fluoroscopy, and meticulous closure of the anterior capsule if incised.
-
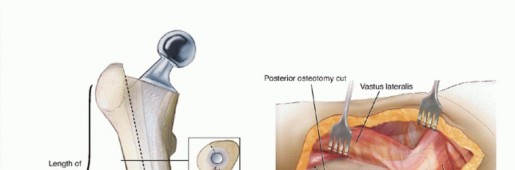
Direct Lateral/Anterolateral Approaches (Hardinge/Modified Hardinge):
- Dissection: Involves detaching or splitting the abductor muscles (gluteus medius and minimus) from the greater trochanter. The interval between the gluteus medius and tensor fascia lata (for anterolateral) is utilized.
- Advantages: Good anterior and superior stability due to preserved posterior capsule.
- Disadvantages: Risk of abductor weakness or detachment, leading to Trendelenburg gait.
- Dislocation Mitigation: Meticulous repair of the abductor mechanism to the greater trochanter is critical to prevent post-operative abductor insufficiency and superior dislocation.
Key Intraoperative Steps for Dislocation Prevention
Regardless of the approach, several universal principles significantly influence hip stability:
-
Acetabular Component Positioning:
This is perhaps the most critical factor.
- Target Zone: Aim for 40° ± 10° of inclination and 15° ± 10° of anteversion relative to the anterior pelvic plane (Lewinnek safe zone). While these zones are guidelines, patient-specific factors (e.g., spinal fusion, pelvic tilt) may necessitate adjustments. Newer concepts emphasize functional safe zones based on individual spinopelvic kinematics.
- Combined Anteversion: The sum of acetabular anteversion and femoral anteversion. Optimal combined anteversion (typically 35-45°) provides stability across a functional range of motion, minimizing both anterior and posterior impingement.
- Coverage: Ensure adequate bony coverage of the acetabular component. Avoid eccentric reaming or placing the cup too medial or too superior.
- Osteophyte Removal: Thoroughly remove all peripheral osteophytes, especially posterior and inferior, as these can cause impingement and lever-out the femoral head.
-
Femoral Component Positioning:
- Version: The femoral component should be implanted with appropriate anteversion, typically matching the native femoral version (10-20°). Excessive retroversion significantly increases posterior dislocation risk.
-
Offset and Leg Length Restoration:
- Femoral Offset: Restoration of the native femoral offset is crucial for optimizing abductor lever arm and tension. Inadequate offset leads to abductor laxity and weakness.
- Leg Length: Aim for equal leg lengths to avoid biomechanical compromise and patient dissatisfaction. Intraoperative methods include measuring distances from fixed points (e.g., greater trochanter to pelvis), contralateral limb comparison, or using specific leg length calipers.
-
Femoral Head Size:
- Jump Distance: Larger femoral heads dramatically increase the "jump distance" required for the head to dislocate, thereby enhancing stability. The use of femoral heads ≥ 32mm, and often 36mm or greater, has become standard practice and is strongly supported by literature to reduce dislocation rates.
- Bearing Surface Considerations: While larger heads improve stability, the choice of bearing surface (metal-on-polyethylene, ceramic-on-polyethylene, ceramic-on-ceramic) influences wear characteristics and overall longevity.
-
Liner Options:
- Standard Liner: Most common.
- Lipped Liner: A posterior-lipped liner can be used in posterior approaches to augment posterior stability by increasing the posterior jump distance, especially if soft tissue repair is compromised or the patient is at higher risk. The lip must be oriented correctly (posteriorly).
- Constrained Liner: Reserved for specific indications, such as recurrent dislocations due to severe abductor insufficiency, neuromuscular disorders, or in revision settings where other measures have failed. Constrained liners physically lock the head within the liner but have higher mechanical failure rates (liner dissociation, fracture, wear) and transfer stresses to the bone-implant interface.
-
Soft Tissue Tension and Repair:
- Capsular Repair: For the posterior approach, meticulous repair of the posterior capsule and external rotators is critical. This recreates a soft tissue barrier and limits internal rotation and adduction in flexion, significantly reducing posterior dislocation risk. This typically involves placing multiple sutures through the capsule/rotators and reattaching them to the posterior aspect of the acetabular rim or greater trochanter.
- Abductor Repair: In lateral approaches, careful reattachment of the gluteus medius/minimus to the greater trochanter is essential for preventing abductor insufficiency and superior dislocation.
- Iliopsoas Release: Rarely, if severe impingement from the anterior capsule or iliopsoas is encountered, a limited release may be considered, but this should be approached cautiously to avoid destabilizing the hip.
-
Trial Reduction and Stability Assessment:
- Dynamic Assessment: Before final component impaction, a trial reduction with trial components is performed. The hip is tested through a full range of motion, including extreme flexion, extension, internal/external rotation, and adduction, to assess for impingement and stability.
- Shuck Test: Gentle traction applied to the limb. If the femoral head can easily be distracted from the acetabulum (excessive shuck), it suggests inadequate soft tissue tension.
- Impaction Assessment: Visually inspect for any bony or prosthetic impingement during maneuvers.
- Stability in "At-Risk" Positions: Specifically test stability in the positions that are most prone to dislocation for the chosen approach (e.g., flexion-adduction-internal rotation for posterior approach; hyperextension-external rotation for anterior approach).
By meticulously adhering to these principles, surgeons can significantly reduce the incidence of post-operative dislocation in THR.
Complications & Management
While dislocation is the primary focus, other complications can indirectly increase dislocation risk or necessitate complex salvage strategies.
Dislocation
- Incidence: 0.5-5% for primary THR; 10-20% for revision THR.
-
Timing:
- Early (<3 months): Often multifactorial, commonly related to component malposition, inadequate soft tissue tension/repair, or early patient non-compliance.
- Late (>3 months): Often associated with patient-related factors (neuromuscular conditions, cognitive impairment), progressive soft tissue laxity, trauma, or implant wear.
-
Management:
- Closed Reduction: First-line treatment for acute dislocation. Performed under sedation or general anesthesia. Post-reduction radiographs (AP and lateral) are mandatory to confirm reduction and rule out periprosthetic fracture.
- Post-Reduction Protocol: After closed reduction, assess for underlying cause. Brace for 6-12 weeks, activity modification, and physical therapy.
-
Recurrent Dislocation:
If dislocation recurs despite closed reduction and conservative measures, or if an underlying mechanical cause is evident, surgical revision is indicated.
- Diagnostic Workup: Comprehensive workup includes standard radiographs (AP pelvis, true laterals) to assess component position, leg length, and signs of loosening. CT scan is invaluable for precise measurement of acetabular and femoral component version, assessment of bony impingement, and identification of component loosening. MRI or arthrography may be used to assess abductor integrity.
-
Salvage Strategies (Revision Surgery):
- Component Re-orientation: Revision of acetabular and/or femoral components if malposition is identified. This is often the most definitive solution.
-
Liner Exchange:
- Lipped Liner: To increase jump distance in a specific direction (e.g., posterior lip for posterior dislocation).
- Constrained Liner: For severe instability due to irreversible soft tissue laxity or neuromuscular dysfunction. Higher risk of wear, liner dissociation, or transfer of stress to the implant-bone interface.
- Larger Femoral Head: Increasing head size (e.g., 28mm to 36mm or 40mm) significantly increases jump distance and improves stability.
- Modular Neck Exchange: To adjust femoral anteversion, offset, or leg length if a modular stem is in place.
- Abductor Repair/Reconstruction: For abductor tears or insufficiency (e.g., using allograft or synthetic mesh).
- Augmentation: Use of a posterior acetabular cage or allograft for severe posterior wall defects.
- Girdlestone Resection Arthroplasty: A rare salvage for recalcitrant infection and instability in medically infirm patients.
- Arthrodesis: Extremely rare, primarily for young, active patients with persistent pain and instability where other options are exhausted.
Other Relevant Complications
-
Periprosthetic Fracture:
- Incidence: 0.1-1.0% in primary THR; higher in revision.
- Management: Varies greatly by fracture location (acetabulum, femur), type (Vancouver classification for femoral), and stability of components. May require ORIF, component revision, or both. Can compromise stability directly if associated with component loosening or indirect effects on soft tissue envelope.
-
Infection (Periprosthetic Joint Infection - PJI):
- Incidence: 0.5-2.0% in primary THR.
- Management: Two-stage exchange (most common), debridement and implant retention (DAIR) in acute cases, one-stage exchange, or salvage procedures (arthrodesis, Girdlestone). PJI compromises soft tissue integrity, can lead to component loosening, and subsequent instability if components are poorly fixed or if multiple debridements lead to significant tissue loss.
-
Neurovascular Injury:
- Incidence: Sciatic nerve 0.5-1.5%; Femoral nerve <0.5%.
- Management: Conservative management for stretch injuries. Surgical exploration for direct transection, hematoma compression. Can lead to motor deficits (e.g., foot drop from sciatic nerve injury) or muscle weakness (e.g., quadriceps from femoral nerve injury) which can compromise gait and contribute to instability.
-
Leg Length Discrepancy (LLD):
- Incidence: Perceived LLD is high; functionally significant LLD >1cm approx. 5-10%.
- Management: Non-operative (shoe lift) for minor discrepancies. Revision for major discrepancies causing pain, limp, or instability due to excessive lengthening or shortening. Excessive lengthening can cause nerve stretch, while shortening reduces abductor tension, both increasing dislocation risk.
-
Abductor Insufficiency (Tears/Weakness):
- Incidence: Up to 20% symptomatic after lateral approach, often less after PA or DAA. Acute tears less common, but chronic tears can be disabling.
- Management: Physical therapy, anti-inflammatory medication. Surgical repair for symptomatic, chronic tears (often with augmentation). Leads to Trendelenburg gait and can directly contribute to superior or superolateral dislocation due to lack of stabilization.
| Complication | Incidence (Primary THR) | Salvage Strategies (Focus on Dislocation Link) |
|---|---|---|
| Dislocation | 0.5-5% | - Closed reduction (first-line) |
| (Early & Late) | - Revision for component malposition (acetabular/femoral) | |
| - Liner exchange (lipped, constrained) | ||
| - Larger femoral head | ||
| - Modular neck exchange (for offset/version adjustment) | ||
| - Abductor repair/reconstruction | ||
| Periprosthetic Fracture | 0.1-1.0% | - ORIF (Open Reduction Internal Fixation) |
| (Intra-op & Post-op) | - Component revision/exchange (if fracture compromises fixation or requires stem removal) - Can directly affect soft tissue tension and component stability. | |
| Periprosthetic Infection | 0.5-2.0% | - Two-stage exchange arthroplasty (most common) |
| (PJI) | - Debridement and implant retention (DAIR) | |
| - Single-stage exchange (selected cases) - Compromised soft tissue envelope from PJI increases dislocation risk. | ||
| Neurovascular Injury | 0.5-2.0% | - Observation (stretch injury) |
| - Surgical exploration/decompression (direct injury, hematoma) - Motor deficits can compromise stability via muscle weakness (e.g., foot drop). | ||
| Leg Length Discrepancy | 5-10% (>1cm) | - Non-operative (shoe lift) for minor. |
| - Revision for significant functional impairment or pain. - Excessive shortening decreases abductor tension; excessive lengthening can lead to nerve palsy or impingement. | ||
| Abductor Insufficiency/Tear | Varies by approach | - Physical therapy, activity modification. |
| - Surgical repair (often augmented) for chronic symptomatic tears. - Leads to Trendelenburg gait and contributes to superior/superolateral dislocation. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation plays a crucial role in the functional recovery of THR patients and, importantly, in mitigating the risk of dislocation. Protocols are tailored, taking into account the surgical approach, intraoperative stability, patient risk factors, and surgeon preference.
General Principles
- Early Mobilization: Commencement of out-of-bed activities and weight-bearing (typically full weight-bearing as tolerated for uncemented components) on the day of surgery or post-op day one, as tolerated. This minimizes complications such as DVT, pulmonary embolism, and deconditioning.
- Pain Management: Multimodal analgesia to facilitate early participation in therapy.
- DVT Prophylaxis: Continued pharmacological and mechanical prophylaxis as per institutional guidelines.
- Wound Care: Meticulous wound care to prevent infection.
Dislocation Precautions (Approach-Specific)
While the trend in modern THR is towards fewer or no formal precautions for stable hips with larger head sizes and robust soft tissue repair, specific precautions remain vital for certain patients or surgical scenarios. The necessity and duration of these precautions are determined by intraoperative stability testing and individual patient risk.
-
Posterior Approach Precautions:
- Avoid Hip Flexion > 90°: Prevents posterior impingement and lever-out.
- Avoid Adduction Past Midline: Especially in combination with flexion and internal rotation.
- Avoid Internal Rotation: Particularly when the hip is flexed.
- Activities to Avoid: Crossing legs, sleeping on the side without a pillow between knees, low chairs, bending at the waist to pick things up.
- Duration: Typically 6-12 weeks, or longer based on surgeon's assessment of stability.
-
Anterior/Anterolateral Approach Precautions (if any):
-
Historically, anterior dislocations are less common. However, some surgeons may advise caution with:
- Avoid Hip Hyperextension and Extreme External Rotation: To prevent anterior impingement or dislocation, especially in the early post-operative period.
- Avoid Excessive Adduction: To protect the abductor repair in lateral approaches.
- Duration: Often shorter or less restrictive than posterior approach precautions, or none at all if stability is excellent.
-
Historically, anterior dislocations are less common. However, some surgeons may advise caution with:
Physical Therapy Phases
-
Phase 1: Acute Phase (Weeks 0-6)
- Goals: Pain and edema control, protection of the healing tissues, initiation of gentle range of motion (within precautions), early strengthening, independent functional mobility.
-
Interventions:
- Range of Motion: Gentle active and passive range of motion within prescribed limits. Continuous passive motion (CPM) is generally not indicated.
- Strengthening: Isometric exercises for gluteals, quadriceps, and hamstrings. Gentle hip abduction, flexion, and extension within limits.
- Gait Training: Full weight-bearing as tolerated with appropriate assistive devices (walker, crutches) progressing to a single cane. Focus on normal gait mechanics.
- Functional Mobility: Instruction in bed mobility, transfers (sit-to-stand), ascending/descending stairs (if applicable).
- Patient Education: Reinforce dislocation precautions, activity modification, use of assistive devices, pain management strategies.
-
Phase 2: Subacute Phase (Weeks 6-12)
- Goals: Progressive strengthening, improved balance and proprioception, restoration of full functional range of motion, normalization of gait, independent performance of ADLs.
-
Interventions:
- Strengthening: Progressive resistance exercises for all hip muscle groups, particularly abductors and extensors. Exercises may include side-lying abduction, glute bridges, mini-squats, step-ups.
- Balance and Proprioception: Single-leg standing, wobble board exercises (advanced).
- Gait: Weaning off assistive devices, focus on endurance and efficiency.
- Functional Training: Initiating light household chores, driving (when safe and off narcotics).
-
Phase 3: Return to Function / Advanced Activity Phase (Weeks 12+)
- Goals: Advanced strengthening, return to recreational activities, sports (low-impact), and work.
-
Interventions:
- Advanced Strengthening: Higher-level resistance training, plyometrics (for appropriate patients).
- Sport-Specific Training: For patients returning to specific sports (e.g., golf, cycling). Emphasize low-impact activities. Avoid high-impact sports, running, and contact sports.
- Activity Modification: Ongoing education about avoiding activities that place the hip at extreme risk for dislocation (e.g., deep squats, certain yoga poses, extreme internal rotation with flexion).
- Maintenance Program: Encourage continuation of home exercise program for long-term strength and flexibility.
Critical Considerations
- Patient Compliance: Adherence to precautions and exercise programs is critical. Non-compliance is a significant risk factor for early dislocation.
- Neuromuscular Status: Patients with pre-existing neuromuscular disorders (e.g., Parkinson's, stroke, cerebral palsy) require highly individualized protocols due to increased dislocation risk and slower motor recovery.
- Abductor Integrity: For cases with abductor compromise, rehabilitation needs to be slower and more protective to allow for healing and strengthening.
- Pain Management: Effective pain control is essential to allow active participation in therapy.
While strict dislocation precautions may be reduced or eliminated for optimally placed, stable hips with larger heads, the principles of strengthening and restoring normal biomechanics through structured rehabilitation remain universally critical for preventing late instability and optimizing functional outcomes.
Summary of Key Literature / Guidelines
The literature on preventing dislocation after THR is extensive, highlighting several key factors and evolving guidelines.
Component Positioning: The "Safe Zone" and Beyond
- Lewinnek's Safe Zone (1978): Classically defined as 40° ± 10° of acetabular inclination and 15° ± 10° of anteversion. This landmark study established a radiographic target associated with lower dislocation rates.
- Callaghan's Zone (1994): Suggested a slightly broader zone of 30-50° inclination and 5-25° anteversion.
- Limitations of Static Safe Zones: Modern literature acknowledges that strict adherence to a static "safe zone" may be insufficient due to inter-individual variability in spinopelvic kinematics. Patients with spinal pathology (e.g., lumbar fusion, severe kyphosis) demonstrate altered pelvic tilt during sitting and standing, which dynamically changes the functional orientation of the acetabular component. This has led to concepts like the "functional safe zone" or "patient-specific positioning," often utilizing pre-operative CT imaging and intraoperative navigation/robotics to optimize component placement for individual kinematic profiles.
- Combined Anteversion: The concept, integrating both acetabular and femoral component version, is increasingly recognized. An optimal combined anteversion (typically 35-45°) minimizes impingement and maximizes the arc of motion before dislocation.
Femoral Head Size
- Evidence: A vast body of literature unequivocally supports the use of larger femoral heads (>32mm, preferably 36mm or greater) in reducing dislocation rates. Larger heads increase the "jump distance" – the linear distance the center of the femoral head must travel before dislocating – effectively enhancing intrinsic stability.
- Trade-offs: While larger heads are beneficial for stability, concerns regarding increased volumetric wear in metal-on-polyethylene bearings led to a period of using smaller heads. However, advancements in polyethylene technology (e.g., highly cross-linked polyethylene) have mitigated these wear concerns, making larger heads the standard for most bearing surfaces.
Surgical Approach
-
Comparative Studies:
Meta-analyses and large registry studies have compared dislocation rates across different approaches.
- Posterior Approach (PA): Historically, PA was associated with higher dislocation rates than other approaches due to disruption of the posterior capsule and external rotators. However, with modern techniques, including meticulous capsular and short external rotator repair, the dislocation rate has significantly decreased and is comparable to other approaches in experienced hands.
- Direct Anterior Approach (DAA): Often touted for lower dislocation rates due to preservation of the posterior soft tissues. However, some studies suggest a learning curve and potentially a higher risk of early anterior dislocation in certain contexts, or no significant difference compared to a well-executed PA.
- Lateral/Anterolateral Approaches: Generally show low dislocation rates, but can be associated with higher rates of abductor weakness or limp if not meticulously repaired.
- Surgeon Experience: Regardless of the approach, surgeon experience and volume are consistently shown to be critical factors in minimizing complications, including dislocation.
Soft Tissue Repair
- Capsular and Short External Rotator Repair (PA): Numerous studies confirm that meticulous repair of the posterior capsule and short external rotators significantly reduces the risk of posterior dislocation following the posterior approach. This technique is now considered standard of care for this approach.
- Abductor Repair (Lateral Approaches): Careful reattachment of the abductor mechanism is crucial to prevent abductor tears and subsequent superior dislocation or Trendelenburg gait.
Constrained Liners
- Indications: Constrained liners are effective in preventing recurrent dislocations in high-risk patients (e.g., severe abductor deficiency, neuromuscular disorders, cognitive impairment) or in revision settings where other strategies have failed.
- Limitations: They have higher rates of mechanical complications (liner dissociation, breakage, accelerated wear, increased stress at the implant-bone interface) compared to standard liners. Their use is reserved for specific, carefully selected cases.
Role of Technology
- Navigation and Robotics: Computer navigation and robotic assistance systems are increasingly used to improve the accuracy and reproducibility of acetabular and femoral component positioning, potentially leading to a further reduction in dislocation rates by achieving more precise adherence to pre-operative plans and desired safe zones (including patient-specific functional zones).
Key Guidelines / Societies
- AAOS (American Academy of Orthopaedic Surgeons) and AAHKS (American Association of Hip and Knee Surgeons): These professional organizations consistently emphasize the importance of appropriate component positioning, adequate soft tissue tension, and patient-specific risk factor assessment in their clinical guidelines and educational materials regarding THR. They advocate for the use of larger femoral heads and meticulous surgical technique, with an acknowledgment of evolving evidence regarding surgical approaches and patient-specific biomechanics.
In conclusion, preventing dislocation after THR involves a multifactorial strategy encompassing meticulous pre-operative planning, precise intraoperative execution of component positioning and soft tissue management, selection of appropriate implant geometries (especially femoral head size), and a tailored post-operative rehabilitation protocol. Contemporary practice moves beyond rigid adherence to static parameters, embracing patient-specific biomechanics and leveraging technological advancements to optimize implant stability.
You Might Also Like